
Abstract
Faciogenital dysplasia 5 (FGD5) amplification drives tumor cell proliferation, and is present in 9.5% of breast cancers. We describe FGD5 expression, assess associations between FGD5 amplification and FGD5 expression, and assess FGD5 expression in relation to proliferation and prognosis. FGD5 immunohistochemistry was done on primary tumors (n=829) and lymph node metastases (n=231) from a cohort of Norwegian patients. We explored associations between FGD5 amplification, FGD5 expression, and proliferation, and analyzed the prognostic value of FGD5 expression by estimating cumulative risks of death and hazard ratios (HRs). We identified nuclear and cytoplasmic expression in 64% and 73% of primary tumors, respectively, and found an association between gene amplification and nuclear expression (p=0.02). The proportion of cases with FGD5 expression was higher in lymph node metastases, compared with primary tumors (p=0.004 for nuclear and p=0.001 for cytoplasmic staining). Neither proliferation nor prognosis was associated with FGD5 expression (age-adjusted HR 1.12 [95% confidence interval = 0.89–1.41] for nuclear expression; and 0.88 [95% CI = 0.70–1.12] for cytoplasmic expression). FGD5 is expressed in a high proportion of breast cancers and lymph node metastases. There was a correlation between FGD5 amplification and nuclear expression, but no association between FGD5 expression and proliferation or prognosis.
Introduction
Sustained proliferation is one of the hallmarks of cancer, 1 and identification of genes that are essential for tumor cell proliferation could be important for prognostication and development of targeted treatment of cancer patients. A combined genomic approach has identified FGD5 (Faciogenital dysplasia 5) amplification as a driver of proliferation in breast cancer. 2 Using fluorescence in situ hybridization (FISH), we previously identified FGD5 amplification in 9.5% of breast cancers, and found that FGD5 amplification was associated with higher tumor proliferation and a poorer prognosis. 3 FGD5 is located on the short arm of chromosome 3, 4 and in our study of FGD5, we defined amplification as FGD5/chromosome enumeration probe 3 (CEP3) ratio ≥2 and/or mean FGD5 copy number/tumor cell ≥4. 3
FGD5 is a Rho guanine nucleotide exchange factor (Rho GEF). Rho GEFs activate Rho GTPases through replacement of guanosine diphosphate (GDP) by guanosine triphosphate (GTP). 5 Rho GTPases regulate the cytoskeleton6,7 and are involved in cellular processes such as cell cycle progression, 8 gene expression,9,10 and cell movement. 7 Furthermore, their activity has been linked to tumorigenesis, 11 and overexpression has been demonstrated in breast cancer, 12 with higher levels in high grade and highly proliferative tumors.13,14 Some genes encoding Rho GEFs are classified as oncogenes,15,16 and although rare, mutations in Rho GEF encoding genes have been identified in cancer.17–19 Upregulation of Rho GEFs may be present in a large proportion of breast cancers,20–22 and high expression is associated with poor differentiation 21 and poor outcome. 23 Due to their role in cancer progression, Rho GEFs and Rho GTPases may be targets for therapy.23,24
In the present study, we used tissue microarrays (TMA) from 829 primary breast cancers from a cohort of Norwegian breast cancer patients. 25 The aims of the study were to describe FGD5 expression by immunohistochemistry (IHC) in primary breast cancers and lymph node metastases; to assess a possible association between FGD5 amplification and FGD5 IHC expression; and to assess a possible association between FGD5 expression, and proliferation and prognosis.
Materials and Methods
Ethical Considerations
The study was approved by the Regional Committee for Medical and Health Sciences Research Ethics (REK, Midt-Norge, Norway, reference number 836/2009).
Study Population
Between 1956 and 1959, a population-based survey for the early detection of breast cancer was carried out in three counties in Norway. 26 We have studied breast cancers occurring among women from one county (Trøndelag), between 1961 and 2008. 25 The women were born between 1886 and 1928. The Cancer Registry of Norway 27 provided information on incident cancer, and the Norwegian Cause of Death Registry supplied information on date and cause of death. During follow-up, 1379 breast cancers were diagnosed, and 909 were previously reclassified into molecular subtypes by means of IHC and in situ hybridization (ISH). 25
The majority of subtyped tumors (867/909) were included in TMAs, and in the present study, these were stained with FGD5 antibody. A total of 38 cases were excluded, due to insufficient amount (n=32) or poor quality (n=6) of tumor tissue. Thus, 829 tumors remained.
Of the 829 cases, 293 had known lymph node metastases at diagnosis, and 233 of these were available in TMAs. Two cases were excluded due to insufficient amounts of tumor tissue. Thus, 231 cases were suitable for assessment of FGD5 expression in lymph node metastases.
Specimen Characteristics
All tumors were previously classified according to histopathological type and grade using current guidelines28,29 and molecular subtype. 25 Briefly, TMAs were constructed using the Tissue Arrayer Minicore 3 with TMA Designer2 software (Alphelys, 78370 Plaisir, France). Three 1 mm-in-diameter tissue cores from the periphery of the primary tumor and three cores from the lymph node metastases were assembled in recipient blocks. Immunohistochemical markers used for molecular subtyping included the following: estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (HER2), Ki67, cytokeratin 5 (CK5) and epidermal growth factor receptor (EGFR) (Table 1). 25 HER2 status was assessed using chromogenic in situ hybridization (CISH). A detailed description of marker assessment used in molecular subtyping is given in previous publications by our group.25,30 With regard to Ki67, assessment was done in hotspots, counting 500 tumor cells. Nuclear Ki67 staining was considered positive, regardless of staining intensity. 31
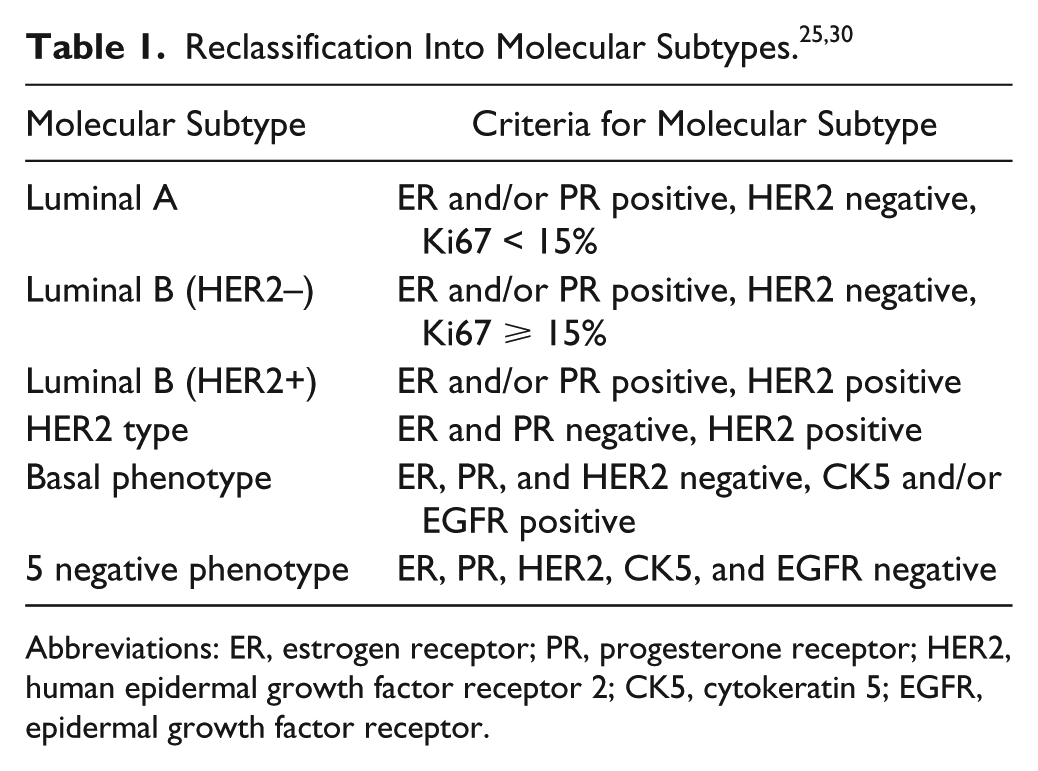
Abbreviations: ER, estrogen receptor; PR, progesterone receptor; HER2, human epidermal growth factor receptor 2; CK5, cytokeratin 5; EGFR, epidermal growth factor receptor.
From the TMAs, 4-μm thick sections were cut and mounted on Superfrost+ glass slides. Sections were dried at 37C overnight, and stored in the freezer at −20C until use. FGD5 IHC was performed according to the manufacturer’s guidelines: Slides were heated at 60C for 1.5 hr, and pretreated in a PT Link, Pre-Treatment Module for Tissue Specimens (Dako Denmark A/S, 2600 Glostrup, Denmark) with EnVision FLEX Target Retrieval Solution Low pH (DAKO DM829) at 97C for 20 min. IHC using rabbit polyclonal FGD5 antibody (Table 2) was done in a DakoCytomation Autostainer Plus (Dako). Dako REAL EnVision Detection System with Peroxidase/DAB+, Rabbit/Mouse, code K5007 was used for visualization.
Antibodies Used for Immunohistochemistry and Immunoblotting.
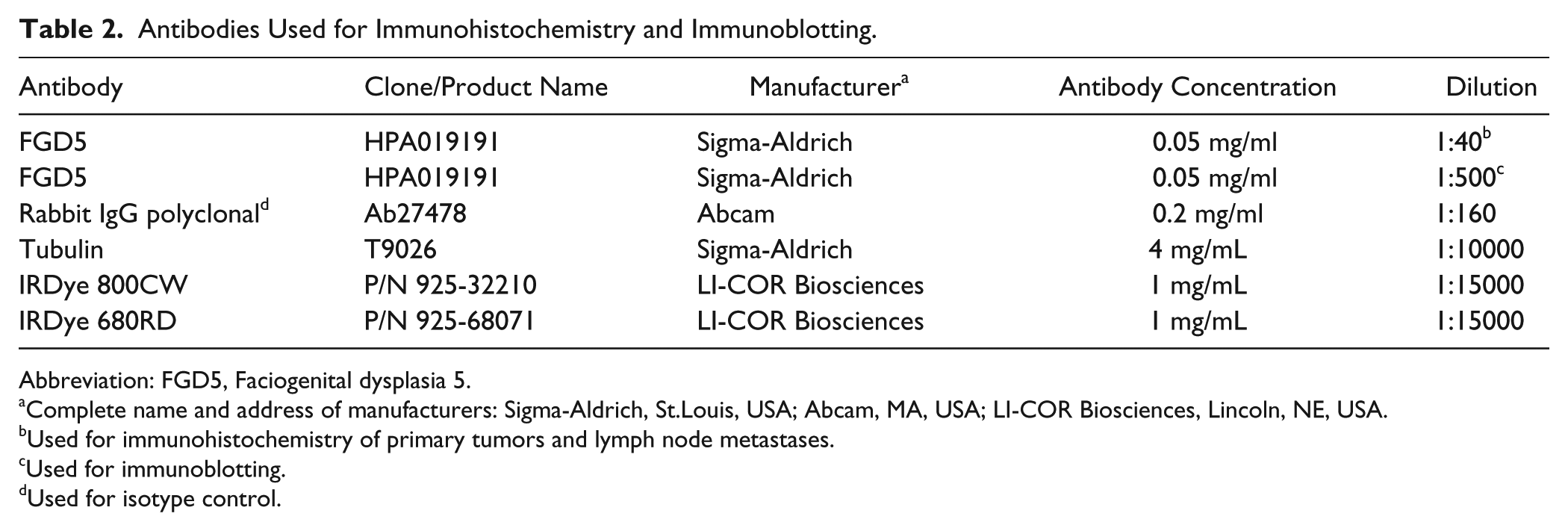
Abbreviation: FGD5, Faciogenital dysplasia 5.
Complete name and address of manufacturers: Sigma-Aldrich, St.Louis, USA; Abcam, MA, USA; LI-COR Biosciences, Lincoln, NE, USA.
Used for immunohistochemistry of primary tumors and lymph node metastases.
Used for immunoblotting.
Used for isotype control.
Immunohistochemical Controls
Negative and positive controls were included. Normal breast tissue was used as a positive tissue control (Supplemental Fig. 1). For negative controls, we omitted the primary antibody in a section from normal breast and in a TMA section containing breast cancer tissue from our study cohort (Supplemental Figs. 1 and 2). For isotype controls, we used a section from normal breast, and a TMA section containing breast cancer tissue from our study cohort (Supplemental Figs. 1 and 3). Isotype control sections were compared with the corresponding FGD5 stained sections. Cytoplasmic staining was not present in the isotype control sections, however some cases had sporadic cells with faint nuclear staining. The isotype control (rabbit IgG, polyclonal, Table 2) was diluted to obtain the same protein concentration as the primary FGD5 antibody. 32
Cell Culture
Michigan Cancer Foundation 7 (MCF-7), T47-D and HCC1806 (human breast carcinomas) cell lines obtained from ATCC (Manassas, VA) were grown in EMEM (Life Technologies, Carlsbad, CA) with 0.01 mg/mL insulin (Life Technologies), 10% FCS (Life Technologies) and 1% penicillin/streptomycin (Life Technologies), in 5% CO2 atmosphere at 37C.
Immunoblotting
For validation of FGD5 antibody specificity, we performed immunoblot analysis of MCF-7, T47-D and HCC1806 whole cell extracts (WCE) prepared according to a previously published protocol. 33 Over 20 μg of WCE was separated on NuPAGE 4% to 12% gradient Bis-Tris polyacrylamide gels (Invitrogen) and transferred to an Immobilon-FL membrane (Millipore) for subsequent immunoblotting. Upon blocking the membrane was incubated with primary antibodies targeting FGD5 and tubulin. Primary antibodies were detected using infrared (IR) Dye-conjugated secondary antibodies IRDye 800CW Goat antimouse IgG and IRDye 680RD Goat antirabbit IgG (Table 2). The signal was visualized using direct IR fluorescence via the Odyssey Scanner, LI-COR Biosciences.
Scoring, Reporting, and Classification of Tumors
Slides were assessed in a bright-field microscope, and for each case, the reported score was an average of all available TMA cylinders. Cytoplasmic FGD5 staining intensity (0 = no staining, 1 = weak, 2 = moderate, and 3 = strong staining) and the proportion of cells with cytoplasmic staining (0: no staining, 1: <10%, 2: 10–50%, and 3: >50%) were recorded. A staining index (SI) was calculated, multiplying intensity by proportion. SI 0 to 1 was considered negative, and SI ≥ 2 was considered positive. The proportion of tumor cells with positive nuclear staining was also recorded, irrespective of staining intensity. All IHC stains were assessed by two pathologists (MV and AMB or PGM) independently. Discrepant results were discussed, and consensus was reached. The REMARK criteria for tumor marker prognostic studies were followed. 34
Statistical Analyses
We used Pearson’s chi-square test to assess differences in clinical and tumor characteristics across categories of FGD5 IHC staining; to compare proportions of FGD5 IHC staining across categories of FGD5 copy number status; and to compare FGD5 IHC staining in primary tumors and lymph node metastases. We also performed multivariate logistic regression to adjust for other tumor characteristics. Cumulative incidence of death from breast cancer was estimated according to categories of FGD5 staining. In these analyses, death from other causes was considered a competing event, and Gray’s test was used to test for equality between cumulative incidence curves. We used Cox proportional hazards models to estimate hazard ratios (HRs) of death from breast cancer (with 95% confidence intervals [CIs]) according to FGD5 staining, censoring at time of death from other causes. Negative staining was used as the reference. Adjustments were made for other prognostic factors at baseline: age (≤49, 50–59, 60–64, 65–69, 70–74, ≥75 years), histological grade,1–3 and stage (I-IV). Adjustments were made for each factor separately, and all combined. No clear violations of proportionality were observed in log-minus-log plots. Stata version 13.1 (Stata Corp., College Station, TX) was used for statistical analyses.
Results
FGD5 Expression and FGD5 Copy Number Status in Primary Tumors
Cytoplasmic FGD5 staining was present in a large proportion of tumors, and a SI ≥ 2 was identified in 73% of cases (Table 3, Fig. 1B). We found no clear associations between FGD5 copy number status and cytoplasmic staining in the primary tumors (Table 4). With cut-offs of 1% and 10%, we identified positive nuclear FGD5 staining in 64% and 26% of cases, respectively (Table 3, Fig. 1A). There was an association between FGD5 copy number status and nuclear staining (1% cut-off), with a higher proportion of positive nuclei among amplified, compared with non-amplified cases (85% vs. 67%, p=0.02). With a cut-off of 10%, however, there was no association between FGD5 copy number status and nuclear staining. Positive cytoplasmic and nuclear staining of FGD5 was found in a high proportion of cases within all molecular subtypes (Table 3). For cytoplasmic staining, SI > 2 was found in 74% of Luminal A, 75% of Luminal B (HER2–), 70% of Luminal B (HER2+), 61% of HER2 type, 50% of 5NP (negative phenotype), and 81% of basal phenotype (BP) tumors, respectively. After adjustment for other characteristics, the odds of positive cytoplasmic staining (SI > 2) was highest for BP, and lowest for 5NP. For nuclear staining, the odds of FGD5 expression (≥1% or ≥10%) was highest in Luminal A tumors. Positive FGD5 staining in endothelial cells was observed (Fig. 1C).
Characteristics of the Study Population According to FGD5 Staining.
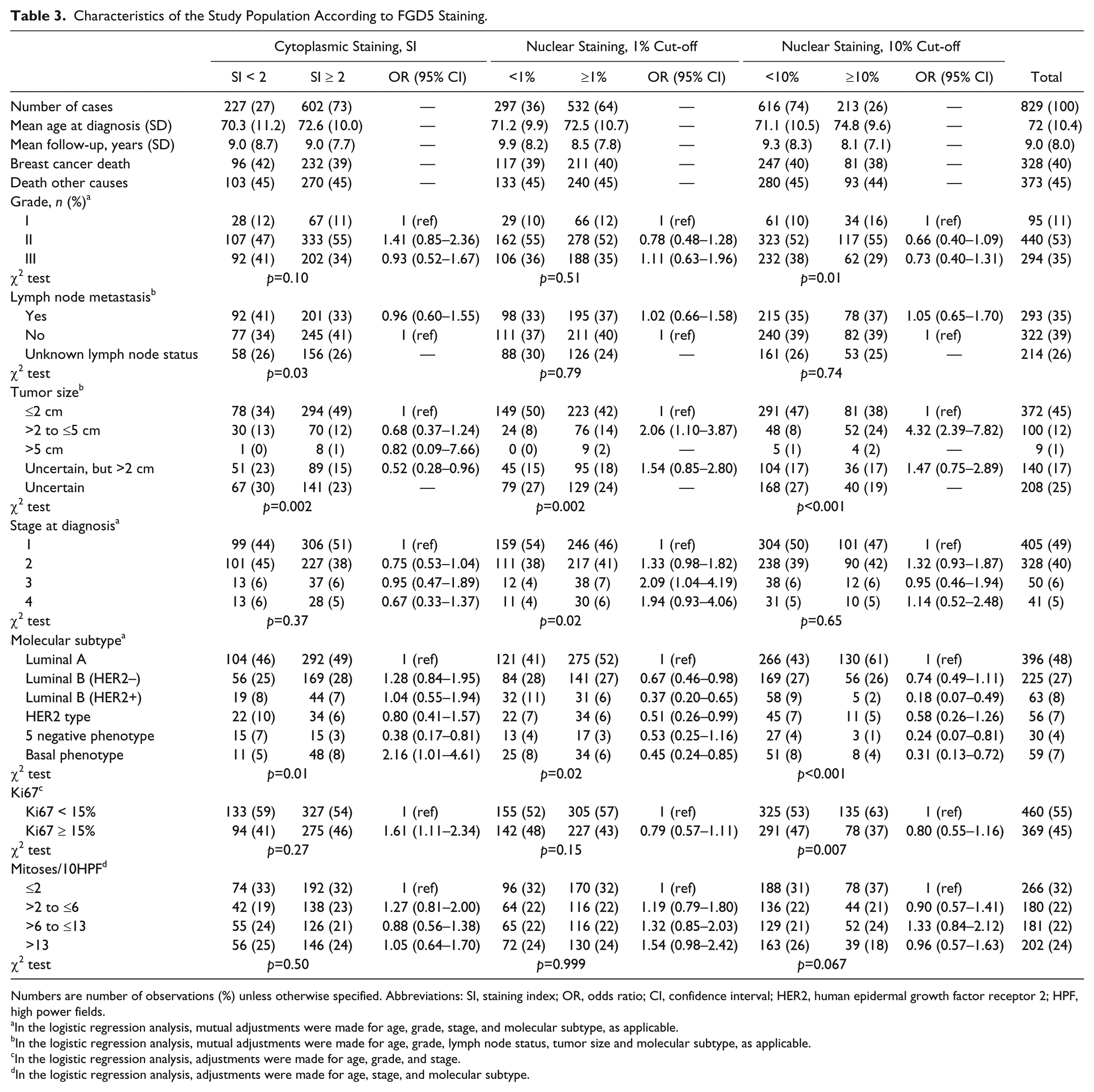
Numbers are number of observations (%) unless otherwise specified. Abbreviations: SI, staining index; OR, odds ratio; CI, confidence interval; HER2, human epidermal growth factor receptor 2; HPF, high power fields.
In the logistic regression analysis, mutual adjustments were made for age, grade, stage, and molecular subtype, as applicable.
In the logistic regression analysis, mutual adjustments were made for age, grade, lymph node status, tumor size and molecular subtype, as applicable.
In the logistic regression analysis, adjustments were made for age, grade, and stage.
In the logistic regression analysis, adjustments were made for age, stage, and molecular subtype.
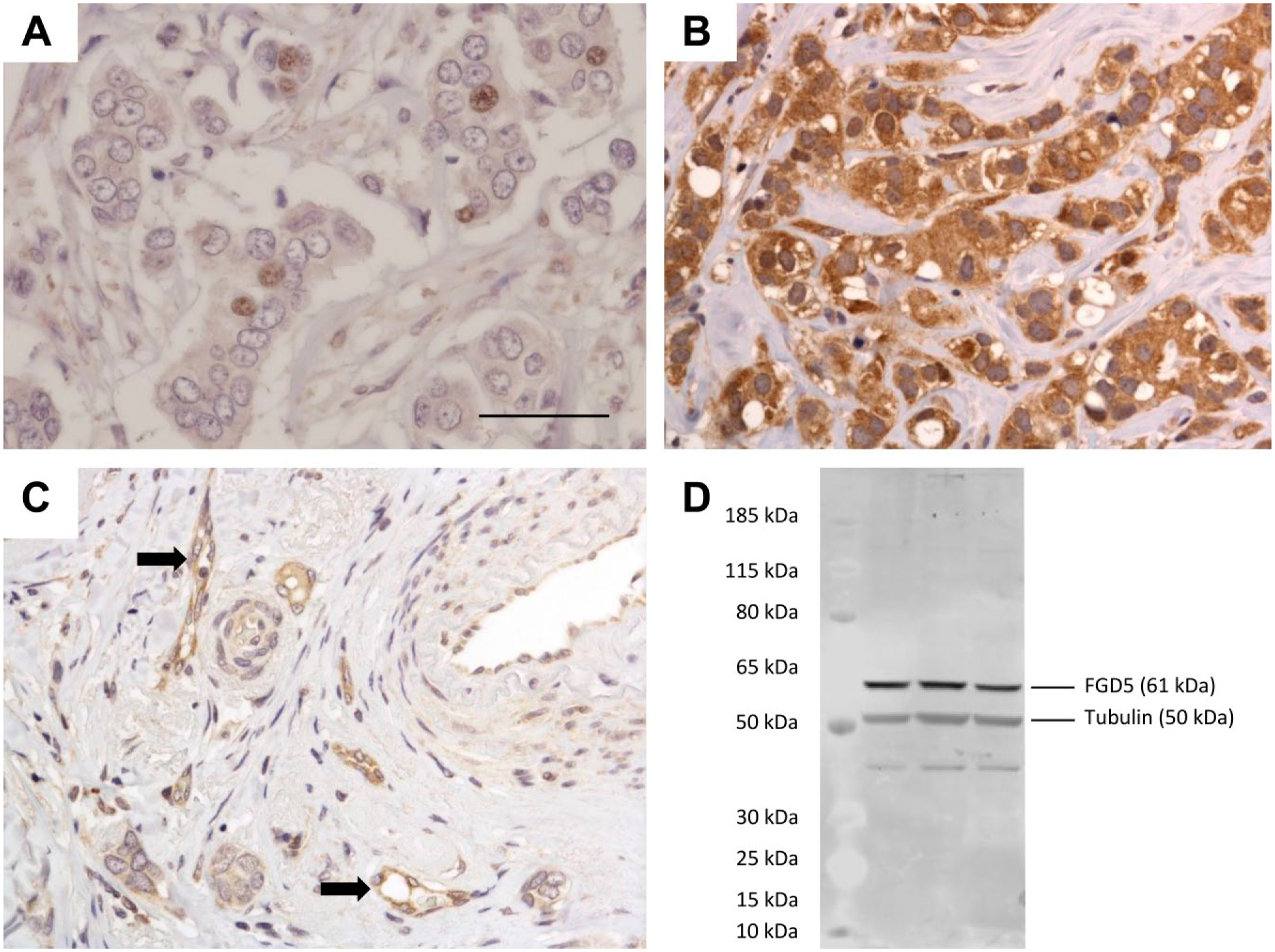
FGD5 immunohistochemical staining in the nuclei (A) and cytoplasm (B) of tumor cells, and in blood vessels (arrows) (C). Scale bar = 50 µm. (D) Immunoblot analysis using anti-FGD5 rabbit polyclonal antibody (HPA019191, Sigma-Aldrich) on breast cancer cell lines (from the left; MCF-7, T47-D, and HCC1806) showing a prominent band consistent with isotype 2 (61 kDa). Abbreviation: FGD5, faciogenital dysplasia 5; MCF-7, Michigan Cancer Foundation 7.
FGD5 Copy Number Status and FGD5 Immunohistochemical Expression in Primary Tumors.
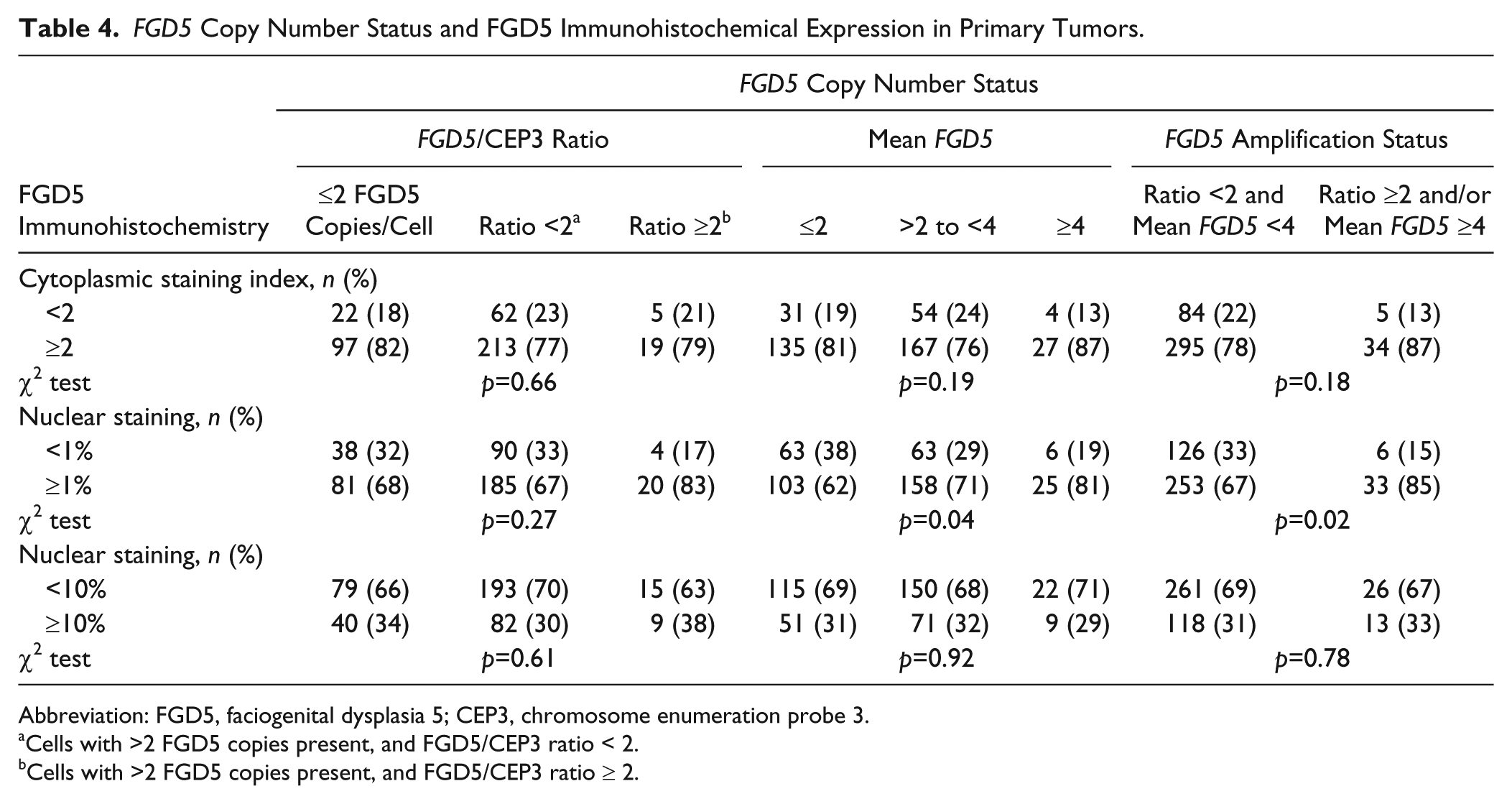
Abbreviation: FGD5, faciogenital dysplasia 5; CEP3, chromosome enumeration probe 3.
Cells with >2 FGD5 copies present, and FGD5/CEP3 ratio < 2.
Cells with >2 FGD5 copies present, and FGD5/CEP3 ratio ≥ 2.
FGD5 Expression in Lymph Node Metastases
A SI ≥ 2 was identified in 80% of lymph node metastases (Table 5). Of all cases with SI < 2 in the primary tumor, 68% had SI ≥ 2 in the corresponding lymph node metastases (p=0.001). Nuclear FGD5 staining was present in 92% (1% cut-off) and 45% (10% cut-off) of lymph node metastases. Among cases with negative nuclear staining (1% cut-off) in the primary tumors, 85% had positive nuclear staining in the corresponding lymph node metastases (p=0.004). Correspondingly, with a 10% cut-off, 38% of cases with negative nuclear staining in the primary tumors, had positive staining in the lymph node metastases (p<0.001).
FGD5 Cytoplasmic and Nuclear Staining in Primary Tumors and Lymph Node Metastases.
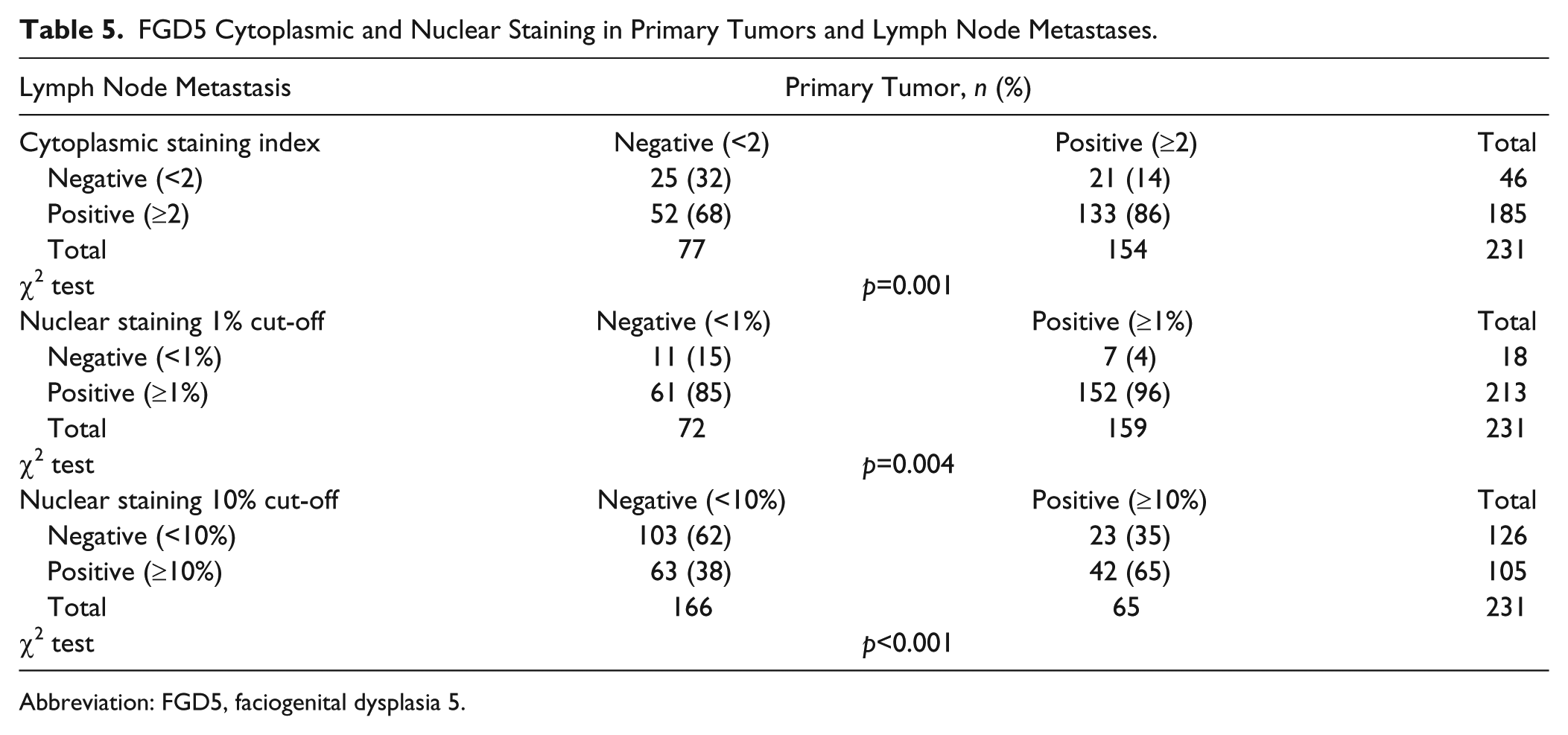
Abbreviation: FGD5, faciogenital dysplasia 5.
Immunoblotting
Antibody specificity was validated by immunoblot analysis of three human breast cancer cell lines (MCF-7, T47-D and HCC1806), in which the most prominent band (61 kDa, Fig. 1D) corresponded to isoform 2 of FGD5 (Fig. 1D).35,36
FGD5 and Proliferation
The distribution of Ki67 low/high (<15% vs. ≤15%) tumors was similar when FGD5 staining of primary tumors was categorized based on SI, or based on nuclear staining with a 1% cut-off (p=0.27 and p=0.15, respectively, Table 3). The proportion of Ki67-high tumors was lower among cases with ≥10% FGD5-positive nuclei, compared with cases with <10% positive nuclei (37% vs. 47%, p=0.007). We found no clear differences in the number of mitoses in the primary tumors across categories of cytoplasmic or nuclear FGD5 staining.
FGD5 IHC and Prognosis
We found similar cumulative risks of death from breast cancer when cases were subdivided based on SI status (SI < 2 vs. ≥ 2, Gray’s test: p=0.36) and nuclear staining (1% cut-off, Gray’s test: p=0.62; 10% cut-off, Gray’s test: p=0.83) (Table 6). Cox regression analyses using negative staining as a reference confirmed this finding, and showed age-adjusted HR of 0.88 (95% CI = 0.70–1.12) for SI, 1.12 (95% CI = 0.89–1.41) for nuclear staining at 1% cut-off, and 0.96 (95% CI = 0.74–1.24) for nuclear staining at 10% cut-off. Adjustments for stage and histological grade at diagnosis did not significantly change these estimates. We also performed separate analyses for each molecular subtype and found no clear differences in prognosis across categories of cytoplasmic and nuclear staining (data not shown).
Absolute and Relative Risks of Death From Breast Cancer According to Cytoplasmic and Nuclear Immunohistochemical FGD5 Staining.
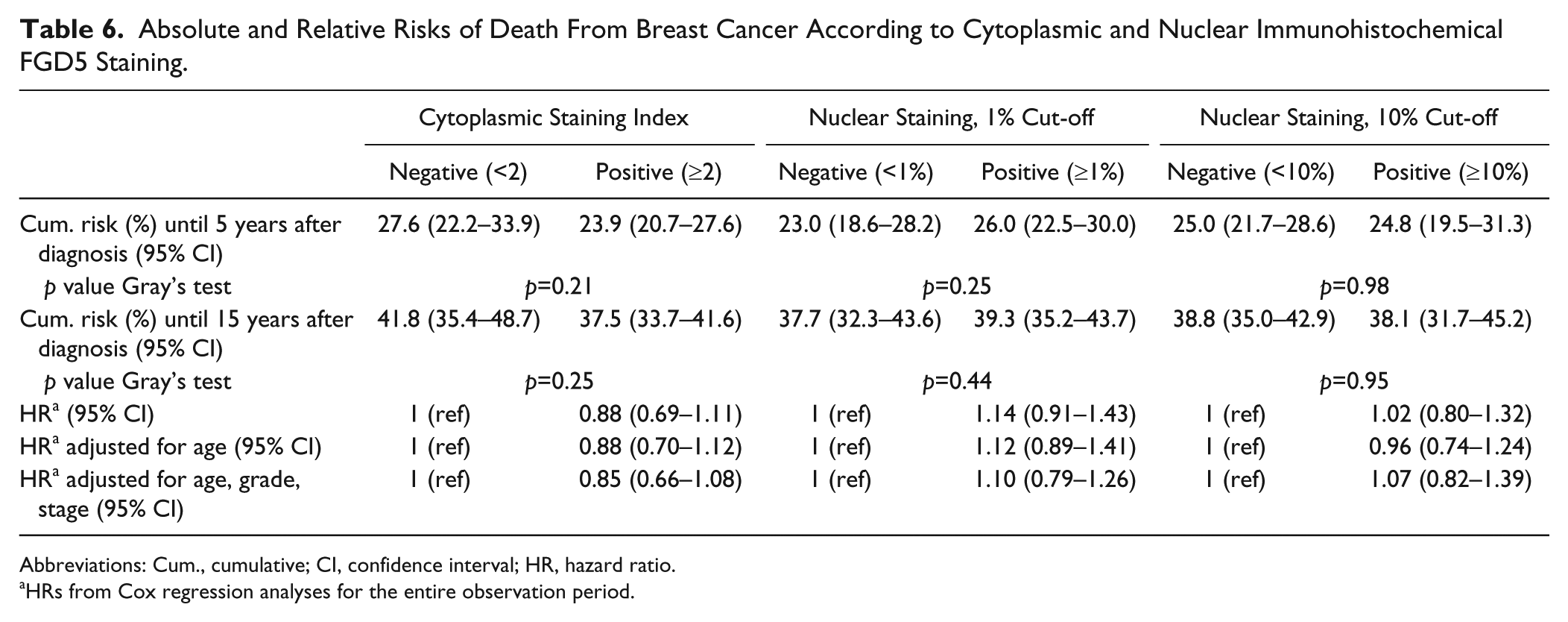
Abbreviations: Cum., cumulative; CI, confidence interval; HR, hazard ratio.
HRs from Cox regression analyses for the entire observation period.
Discussion
We identified FGD5 staining in the cytoplasm and nuclei in a large proportion of primary breast cancers and lymph node metastases. The proportion of cases with positive FGD5 staining in lymph node metastases was markedly higher compared with the corresponding primary tumors. There was a positive association between FGD5 amplification status and nuclear staining at 1% cut-off in the primary tumors. However, neither proliferation nor prognosis was found to be associated with FGD5 expression.
A strength of our study is the large number of cases with long-term follow-up data acquired from high quality national registries. 27 Assessment of IHC was done by two pathologists independently, using predetermined criteria for evaluation. Discrepant results were discussed, and consensus was reached.
Breast cancers included in this study were diagnosed between 1961 and 2008, and it is likely that preanalytical conditions have varied during the inclusion period, possibly influencing our results. 37 However it has been shown in other studies that valuable results can be obtained using archival material.37,38
According to the Human Protein Atlas, a cytoplasmic staining pattern was expected. 39 FGD5 is a new marker with no available guidelines for assessment, and for cytoplasmic staining, we used a SI, where the intensity of staining was multiplied with the proportion of stained cells. This approach has been used for other markers.40–42 We regarded SI ≥ 2 as positive, similar to previous studies of other markers.25,30,40,43 In addition, we observed nuclear staining in a large proportion of cases, and the proportion of stained nuclei, irrespective of staining intensity was recorded. Not including staining intensity in the assessment of nuclear markers is routine both for hormone receptors and Ki67 in breast cancer.31,44 For nuclear staining, two different cut-off levels were used in the analyses.
Gatza et al. found that FGD5 was amplified uniquely in highly proliferative luminal tumors, and that amplification of the gene was prognostic in luminal tumors. 2 Their molecular subtyping was done by gene expression analysis, and luminal tumors were defined as all tumors that were not basal. We reclassified breast cancer tumors into six different molecular subtypes using surrogate IHC and ISH markers.25,30 It has been shown that molecular subtyping by gene expression analysis is similar, but not identical to subtyping using surrogate markers.45–48 In our previous study, FGD5 copy number increase was identified within all molecular subtypes, and amplifications were found in all molecular subtypes except the 5NP. In the present study, we identified positive FGD5 staining in a high proportion of cases within all molecular subtypes, with the highest proportion observed in the BP. Despite some differences in cytoplasmic and nuclear staining, we found no clear differences in prognostic value of FGD5 across subtypes.
There was a positive association between FGD5 amplification and nuclear FGD5 staining. For most cases in which nuclear FGD5 staining was identified, the percentage of positive nuclei was low (median value 4%).
In breast cancer, amplification of the HER2 gene is strongly associated with overexpression of the HER2 protein. 49 Therefore, to select patients for targeted anti-HER2 treatment, both ISH and IHC can be used.50,51 However, studies of many other genes have demonstrated a poor correlation between gene copy number or mRNA expression, and protein level.14,49,52
In this study, lack of correlation between FGD5 copy number and cytoplasmic staining was observed. Although a correlation between gene copy number and mRNA levels has been indicated previously, 2 for the samples included in this study this correlation has not been demonstrated so far. Lack of correlation between FGD5 copy number and cytoplasmic staining suggests that the amplified gene copy is potentially silenced. The amplified gene copy could have been translocated to a new region in the genome, and potentially silenced through mechanisms such as methylation. Furthermore, since within FGD5 is encoded noncoding RNA (LOC105376963), the copy number increase does not only affect FGD5 expression, but could also result in altered expression of the noncoding RNA, potentially influencing other genes and/or other pathways.
The lack of correlation between copy number and protein levels could reflect underlying biology, and our findings suggest that FGD5 affects proliferation in other ways than through its protein product. FGD5 protein has been described to exist in two isoforms, the longer 160 kDa isoform 1 and shorter 61 kDa isoform 2. Interestingly, the immunoblot analysis indicated presence of only shorter isoform 2 in the tested breast cancer cell lines (Fig. 1D). It is however not possible to exclude that another isoform not detected by the antibody is present and potentially play a role in breast cancer cells. As this is the first study of FGD5 expression in a cohort of breast cancer patients, our findings need to be validated in other cohorts. Further studies using other FGD5 antibodies or a proteomic approach would be of added value.
The antibody used in the present study was a polyclonal Protein Epitope Signature Tag antibody (PrEST) 53 selected from the Human Protein Atlas.54,55 PrESTs have similar specificity to monoclonal antibodies. 53
We found no clear association between FGD5 expression and prognosis in this study. However, we previously found strong associations between FGD5 amplification status and prognosis in the same cohort of breast cancer patients. Evidently, the role of FGD5 in breast cancer proliferation and prognosis is not yet clarified. FGD5 is classified as a Rho GEF, and these molecules are known to activate Rho GTPases, whose activity has been linked to cancer progression.8,11–14 FGD5 is expressed in endothelial cells,56–60 and studies have demonstrated its presence in the plasma membrane58,60 and in the perinuclear region 58 of human umbilical vein endothelial cells (HUVECs). FGD5 can affect endothelial cell barriers through interactions with the Rho GTPase Cdc42, 60 and the latter has been identified as the selective binding partner for FGD5. 57 In a recent study, Cdc42 protein expression was identified in a large proportion of breast cancers, and cytoplasmic expression was associated with higher grade and higher Ki67 levels. 61 A possible link between FGD5 and angiogenesis has been suggested,57–59 and Rho GTPases such as Cdc42 are involved in angiogenesis through regulation of the cytoskeleton and organization of endothelial cells.62,63 Interestingly, positive FGD5 staining in blood vessels was identified in our study, and thus, assessing whether FGD5 copy number status or FGD5 expression may be associated with tumor angiogenesis could provide valuable information on the role of FGD5 in breast cancer development.
In conclusion, we have demonstrated cytoplasmic and nuclear FGD5 staining in a large proportion of primary breast cancers and lymph node metastases. The proportion of FGD5-positive lymph nodes was higher compared with the corresponding primary tumors. There was an association between FGD5 amplification status and nuclear FGD5 staining; however, neither proliferation nor prognosis was found to be associated with FGD5 expression.
Supplemental Material
DS_10.1369_0022155418792032 – Supplemental material for Characterization of FGD5 Expression in Primary Breast Cancers and Lymph Node Metastases
Supplemental material, DS_10.1369_0022155418792032 for Characterization of FGD5 Expression in Primary Breast Cancers and Lymph Node Metastases by Marit Valla, Patricia G. Mjønes, Monica J. Engstrøm, Borgny Ytterhus, Diana L. Bordin, Barbara van Loon, Lars A. Akslen, Lars J. Vatten, Signe Opdahl and Anna M. Bofin in Journal of Histochemistry & Cytochemistry
Footnotes
Acknowledgements
The authors thank the Department of Pathology at St. Olavs Hospital, Trondheim University Hospital, Norway for making the archives available for the study, the Cancer Registry of Norway, and the Norwegian Cause of Death Registry for providing the patient data, and Tonje S. Steigedal and Jimita P. Toraskar for supplying two of the breast cancer cell lines.
Competing Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors have contributed to this article. More specifically, MV: study design and writing the article, annotation of FGD5 IHC, statistical analyses, and interpretation of results; PGM: writing the article and annotation of FGD5 IHC; MJE: writing the article and molecular subtyping of the patient cohort; BY: writing the article and laboratory work during molecular subtyping and FGD5 IHC; DLB: writing the article, immunoblot, interpretation of results; BVL: writing the article, immunoblot, and interpretation of results; LAA: writing the article and interpretation of results; LJV: writing the article and interpretation of results; SO: writing the article and interpretation of results; AMB: study design and writing the article, annotation of FGD5 IHC, interpretation of results, and molecular subtyping of the patient cohort.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research Council of Norway (project number 231297) and the Liaison Committee between the Central Norway Regional Health Authority and the Norwegian University of Science and Technology (project number 46030001 and 46056705).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.