
Abstract
Aberrant regulation of the receptor tyrosine kinase platelet-derived growth factor alpha (PDGFRα) is implicated in several types of cancer. Inhibition of the PDGFRα pathway may be a beneficial therapy, and detection of PDGFRα in tumor biopsies may lead to insights about which patients respond to therapy. Exploratory or clinical biomarker use of PDGFRα IHC has been frequently reported, often with polyclonal antibody sc-338. An sc-338-based assay was systematically compared with anti-PDGFRα rabbit monoclonal antibody D13C6 using immunoblot profiling and IHC in formalin-fixed and paraffin-embedded human tumor cell lines. Application of sc-338 to blots of whole cell lysates showed multiple bands including some of unknown origin, whereas application of D13C6 resulted in a prominent band at the expected molecular mass of PDGFRα. The IHC assay using D13C6 showed appropriate staining in cell lines, whereas the assay using sc-338 suggested nonspecific detection of proteins. An optimized IHC assay using D13C6 showed a range of staining in the tumor stromal compartment in lung and ovarian carcinomas. These observations suggest that use of clone sc-338 produced unreliable results and should not be used for an IHC research grade assay. In addition, this precludes its use as a potential antibody for a clinical diagnostic tool.
Introduction
Platelet-derived growth factor receptor alpha (PDGFRα) is a cell surface receptor tyrosine kinase that functions in the regulation of normal cell growth and differentiation, and it is important for mesenchymal cell development.1,2 Upon binding of its cognate ligands in the PDGF family, PDGFRα recruits Src homology 2 (SH2) domain-containing effector molecules and initiates one or multiple signaling cascades, including the Ras/MAPK (ERK), PI3K, and PLC-γ pathways.1,3,4 Pathway activation may alter cellular processes implicated in the development of cancer, 5 including angiogenesis, stromal expansion, increased rates of mitosis, stimulation of cellular motility, or prevention of apoptosis. 6 Aberrations in PDGFRα activation caused by overexpression, 7 amplification,8–10 translocation, 11 or point mutations of the PDGFRA gene 12 have been implicated in cellular transformation and the pathogenesis of solid tumors. Overexpression of PDGFRα protein is reported in a variety of human tumors, including gliomas, gastrointestinal stromal tumor (GIST), and malignancies of the ovary, prostate, breast, colon, lung, skin, and bone.13–16 In addition to direct effects on tumor cells, PDGF/PDGFRα signaling mediates paracrine effects by PDGFRα expressed on tumor-adjacent stromal fibroblasts and affects regulation of tumor angiogenesis. 1
As the biological underpinnings of PDGFRα in tumor progression are more thoroughly elucidated, targeted therapeutics are being developed to treat discrete subtypes of cancer. Targeting PDGFRα with specific therapeutic antibodies or small molecule inhibitors may interrupt signaling and suppress tumor growth by direct tumor inhibition and/or disrupting supporting stroma and blood vessels. 17 Antitumor activity of therapeutic antibodies that target PDGFRα has been shown in preclinical xenograft studies which include growth inhibition of glioblastoma, leiomyosarcoma,15,18 and lung cancers. 17 Also, models of metastasis with human prostate carcinoma show delay of progression of early metastatic foci and reduction of established lesions. 19
There is a growing interest in developing laboratory assays for routine clinical use to refine diagnoses, such as defining epidermal growth factor receptor (EGFR) mutation status in lung cancer20–22 or identifying patients with human epidermal growth factor receptor 2 (HER2)–positive breast cancer.23,24 Ultimately, the goal is that these tests will help clinicians identify the most appropriate therapeutic approach for their patients. IHC is a well-established platform in diagnostic pathology, providing surgical pathologists with a powerful tool to explore molecular proteomics. 25 Differences in analytic sensitivity and specificity between diagnostic antibody clones may severely impact the clinical utility of an IHC assay if it leads to unacceptably high false-positive or false-negative clinical results. Therefore, for certain high-use, predictive IHC assays, the College of American Pathologists’ cancer synoptic templates require listing which diagnostic IHC antibody clone was used. 26 With a focus on PDGFRα, we investigated two IHC assays: (1) an assay using a rabbit polyclonal antibody, based on the antibody used in several published reports;12,27–30 and (2) an assay employing a rabbit monoclonal antibody that was developed following a comprehensive IHC assay development paradigm. Here, we provide data that compare the performance of the assays, and we make recommendations for future studies that aim to detect PDGFRα in tumor tissues.
Materials and Methods
Ethics Statement
Asterand Bioscience (Detroit, MI) confirms that the following activities were completed by their collaborators in the process of obtaining human tissues: approval from institutional and independent review board, authorization from the privacy officer, and obtaining government licenses and industry accreditations. All informed consent forms used by Asterand Bioscience are subject to review and approval by appropriate regulatory and ethics authorities. In circumstances where a consent form is unavailable, Asterand Bioscience obtained a waiver of informed consent from an institutional review board to enable the use of the tissues and clinical information for research. Additional ethical considerations in practice by Asterand Bioscience are available at http://www.asterandbio.com/company/ethics/.
Control Cell Lines, Cell Culture, and Histotechnological Preparation of Cell Lines
Control cell lines for IHC were identified by a strategic process, including (1) screening cell line microarrays comprising approximately 40 tumor cell lines using PDGFRα IHC (D13C6) as described in the methods below; (2) arbitrary selection of representative lines that exhibited relatively high, moderate, low, or negative cytoplasmic/membranous immunoreactivity; (3) cross-referencing selections with publicly available gene expression databases; and finally (4) subsequent confirmation of protein abundance and mRNA expression by Western blotting and ISH assays, respectively, as described below.
Gene expression values were obtained from Broad-Novartis Cancer Cell Line Encyclopedia (CCLE; http://www.broadinstitute.org/ccle). Briefly, CCLE generated data by mRNA hybridization on Affymetrix U133 Plus 2.0 arrays, and then applied the Robust Multi-array Average (RMA) algorithm, normalized using quantile normalization, and log2 transformed the data. Log2 values representing estimated expression levels were extracted from file CCLE_Expression_Entrez_2012-10-18.res and are included below.
All media were supplemented to include 10% FBS and 1% (v/v) penicillin/streptomycin. All cells were propagated at 37C and 5% CO2. OVCAR8 cells (human ovarian carcinoma, selected for negative PDGFRα immunoreactivity, RMA log2 3.4) were obtained from the Division of Cancer Treatment and Diagnosis at the National Cancer Institute (Frederick, MD), and A2780 cells (human ovarian carcinoma, selected for low PDGFRα immunoreactivity, RMA log2 10.3) were obtained from Eli Lilly and Company (Indianapolis, IN) internal stocks. A2780 was selected as a cell line of interest despite the inconsistency between the RMA log2 value and the immunoreactivity categorization as both mRNA and protein abundance were to be assessed in the current study. Both cell lines were expanded using RPMI-1640 (Thermo Fisher Scientific, Rockford, IL) supplemented with 1% sodium pyruvate. Other cell lines were obtained from the American Type Culture Collection (ATCC, Manassas, VA): M059K cells (human glioblastoma, selected for moderate PDGFRα immunoreactivity, RMA log2 8.5) were expanded using 1:1 mixture of DMEM and Ham’s F12 medium with 2.5-mM
Western Blots
Whole cell extracts were prepared by resuspending in protease inhibitor–supplemented RIPA buffer (Thermo Fisher Scientific). Samples were combined with loading buffer containing sodium dodecyl sulfate and dithiothreitol (DTT), placed in a 95C heat block for 3 min, and then separated on NuPAGE 4–12% bis-tris polyacrylamide gels (Life Technologies [Thermo Fisher Scientific], Grand Island, NY). Gels were transferred to nitrocellulose membranes and probed with a primary antibody (antibody sc-338, rabbit polyclonal IgG, Santa Cruz Biotechnology, Dallas, TX, RRID: AB_631064; or clone D13C6, rabbit monoclonal IgG, Cell Signaling Technology, Danvers, MA, RRID: AB_10692773) overnight at 4C with agitation. Blots were incubated with species-specific, horseradish peroxidase (HRP)–conjugated secondary antibodies for 1 hr and then visualized using enhanced chemiluminescence detection (Pierce, Thermo Fisher Scientific). The anti-glyceraldehyde 3-phosphate dehydrogenase (GAPDH) primary antibody (clone 14C10; Cell Signaling Technology) was used to verify equal protein loading on gels. All primary antibodies were applied at a working dilution of 1:1000.
Human Tissue Specimens
PDGFRα expression was evaluated using FFPE human tumor specimens obtained from commercial sources (Asterand Bioscience). Acquisition and processing of these tissues was confirmed to be in line with rigorous human tissue acquisition protocols that ensure collection and supply of high-quality human tissues for novel biomarker studies. Unpublished certificates of analysis for FFPE tissues can be obtained directly from Asterand Bioscience which include these quality control activities: (1) tissues were processed with less than 30-min cold ischemic time, (2) samples were fixed in 10% NBF, (3) hematoxylin and eosin slides were reviewed by a board-certified pathologist to ensure tissue of origin and diagnoses were consistent with clinical data, and (4) samples were checked for paraffin and processing quality. The submitted diagnoses of all tumors were independently confirmed and refined by an independent board-certified pathologist (G.J.O.).
Immunohistochemistry
FFPE sections of cell line microarrays and tumor blocks were cut (5 µm) and lifted onto Superfrost Plus adhesion slides (Thermo Fisher Scientific). Slides were allowed to dry and then baked at 60C for 0.5 to 1 hr before staining.
For the anti-PDGFRα antibody D13C6 (rabbit monoclonal IgG; Cell Signaling Technology), slides were loaded into the PT Link (Dako, Carpinteria, CA) for deparaffinization, rehydration, and epitope retrieval using Tris/EDTA buffer (pH 9) for 20 min at 97C. Slides were transferred to the Autostainer Link 48, and endogenous peroxidases were blocked with EnVision Flex Peroxidase Blocking Reagent (Dako) for 5 min, the primary antibody was applied at 1.5 µg/ml in antibody diluent (Dako) for 15 min, EnVision Flex+ rabbit linker (Dako) was applied for 15 min, EnVision FLEX/HRP (Dako) was applied for 20 min, Substrate Working Solution (one drop of 3,3′-diaminobenzidine substrate [DAB] per ml of substrate buffer) was applied for 10 min, and finally EnVision Flex Hematoxylin was applied for 5 min. Slides were removed from the stainer and dehydrated by sequential submersion in 95% ethanol, 100% ethanol, and xylene, and coverslipped using routine procedures.
We also produced a PDGFRα IHC assay based on antibody sc-338 (rabbit polyclonal; Santa Cruz Biotechnology) using similar autostaining technology to published methods. 29 Briefly, slides were loaded into the Discovery XT automated stainer (Ventana Medical Systems, Tucson, AZ), and deparaffinization, rehydration, and epitope retrieval using CC1 (Ventana Medical Systems Cell Conditioning Solution) for 36 min at 100C were completed. The Discovery DAB Map Detection Kit (Ventana Medical Systems) was used for visualization with some modifications. Briefly, slides were treated with Inhibitor D for 4 min to reduce endogenous peroxidase activity, treated with egg white avidin for 4 min, and then treated with free biotin for 4 min. Primary antibody was applied at 4.0 µg/ml for 1 hr, goat anti-rabbit secondary antibody (Dako) was applied for 32 min, Blocker D (Ventana Medical Systems) was applied for 4 min to reduce background staining, SA-HRP D was applied for 16 min, one drop of DAB D and one drop of DAB H2O2 D substrate were applied for 8 min, Copper D copper sulfate solution was applied for 4 min, Hematoxylin 2 was applied for 8 min, and finally bluing reagent was applied for 4 min. Slides were removed from the stainer; washed with a soap solution; dehydrated by sequential submersion in 95% ethanol, 100% ethanol, and xylene; and coverslipped using routine procedures.
For negative controls, IHC assays were run with primary antibody substituted with antibody diluent to ensure no chromogenic staining originated from the secondary antibody. Also, rabbit isotype IgG (Cell Signaling Technology) was used in place of primary antibody to help confirm that immunoreactivity was not due to nonspecific interaction with IgG.
Brightfield In Situ Hybridization
FFPE sections were cut and dried as for IHC and used for automated brightfield in situ hybridization (BRISH). Dry slides were loaded on the Bond RX (Leica Biosystems, Buffalo Grove, IL), and deparaffinization, rehydration, and pretreatment using EDTA buffer solution (ER2, pH9; Leica Biosystems) were performed at 100C for 10 or 15 min for FFPE cell lines and tumor tissues, respectively. Then, RNAscope LS reagent kit (Advanced Cell Diagnostics [ACD], Hayward, CA) was used for detection of mRNA. Briefly, protease was applied for 10 or 25 min for FFPE cell lines and tumor tissues, respectively; and then peroxide was applied for 10 min. PDGFRA or PDGFRB RNAscope LS 2.0 probe (ACD) was hybridized at 40C for 2 hr. The signal amplification steps were performed per manufacturer’s instructions for Amp 1-6, with the addition of a 2× saline sodium citrate (SSC; Thermo Fisher Scientific) stringency wash performed after Amp 1. DAB and hematoxylin were applied as part of the modified Bond Polymer Refine Detection kit (Leica Biosystems). Slides were dehydrated and coverslipped as described above.
For negative and positive controls, BRISH assays were run with a probe designed against the Bacillus subtilis gene dihydrodipicolinate reductase (dapB) to ensure no background chromogenic signal originated from the assay. Also, a probe designed to detect peptidylprolyl isomerase B (PPIB) was performed on each tissue and cell line to confirm that each FFPE block was fixed and processed appropriately and that mRNA was detectable.
Imaging and Image Analysis
Images were obtained as high-resolution digital scans (ScanScope XT; Aperio Technologies, Vista, CA) at ×200 or ×400 original magnification. HALO v2.0.909.5088 (Indica Labs, Albuquerque, NM) was used to analyze four technical replicate fields of view per line with an average of 250 cells per analysis. IHC on cell lines was assessed with the CytoNuclear algorithm (v1.4) with these parameter settings: image zoom, 1; positive signal stain, sampled from representative DAB-positive cell; and stain minimum optical density (OD) at 0.090, 0.156, 0.224 for weak, moderate, and strong cutoffs, respectively. PDGFRA BRISH on cell lines was assessed with the ISH algorithm (v1.2) with these parameter settings: image zoom, 1; positive signal stain, sampled from representative DAB-positive cell; detect cells, true; cell radius, 10; signal contrast threshold, 0.76; spot segmentation aggressiveness, 0.95; and signal size, 2.1. The output for the IHC signal was captured as average OD, whereas the BRISH signal was captured as average signal per cell. For BRISH, the signal appeared as discrete round dots typically less than 1 µm in diameter which were enumerated by the algorithm. Image analysis results were graphed using Prism v7.00 (GraphPad Software, Inc., La Jolla, CA), and average values were plotted along with standard deviations. For IHC comparisons, a paired t-test was performed for each control cell line using Prism. A p value of less than 0.05 was considered significant.
Results
Immunoblot Profiles and IHC Profiles Differed When Comparing Antibody sc-338 With Antibody D13C6
The most straightforward way to characterize and compare the two anti-PDGFRα antibodies of interest was to perform immunoblot analysis. A series of four human tumor cell lines were selected that were predicted to express PDGFRα at various levels based on a multistep process of screening gene expression and immunoreactivity information as described in the methods. OVCAR8 (ovarian carcinoma), A2780 (ovarian carcinoma), M059K (glioblastoma), and MG63 (osteosarcoma) lines were predicted to exhibit negative, low, moderate, and high PDGFRα, respectively. Also included were stably transfected overexpressers of either PDGFRα or PDGFRβ in PAE cells. The two anti-PDGFRα antibodies were compared on identical gels of whole cell lysates. The use of sc-338 resulted in a higher abundance of signal at the predicted molecular mass (190 kDa) in PDGFRα transfectants compared with the PDGFRβ transfectants; however, there were additional prominent bands in the immunoblot profile (Fig. 1A). The additional prominent bands were also present in the cell line lysates chosen to assess endogenous PDGFRα expression, although the expected range of expression levels was observed at the predicted molecular mass. These included the highest expression in MG63 cells followed by lower expressing M059K cells. The profile of the anti-PDGFRα antibody D13C6 also showed a prominent band at 190 kDa in the PDGFRα that was not present in the PDGFRβ transfectants (Fig. 1B). The MG63 cells and M059K cells exhibited a strong and moderate level of PDGFRα expression, respectively. A doublet was clearly visible in the MG63 cells near the predicted molecular mass, consistent with expected differences in PDGFRα glycosylation status. There was a band visible at approximately 45 kDa in the MG63 lysates. A band of similar size was present in the PDGFRα, but not the PDGFRβ transfection lysate, suggesting the band originated from PDGFRA sequences. Endogenous expression of PDGFRα in the other cell lines was not observed.
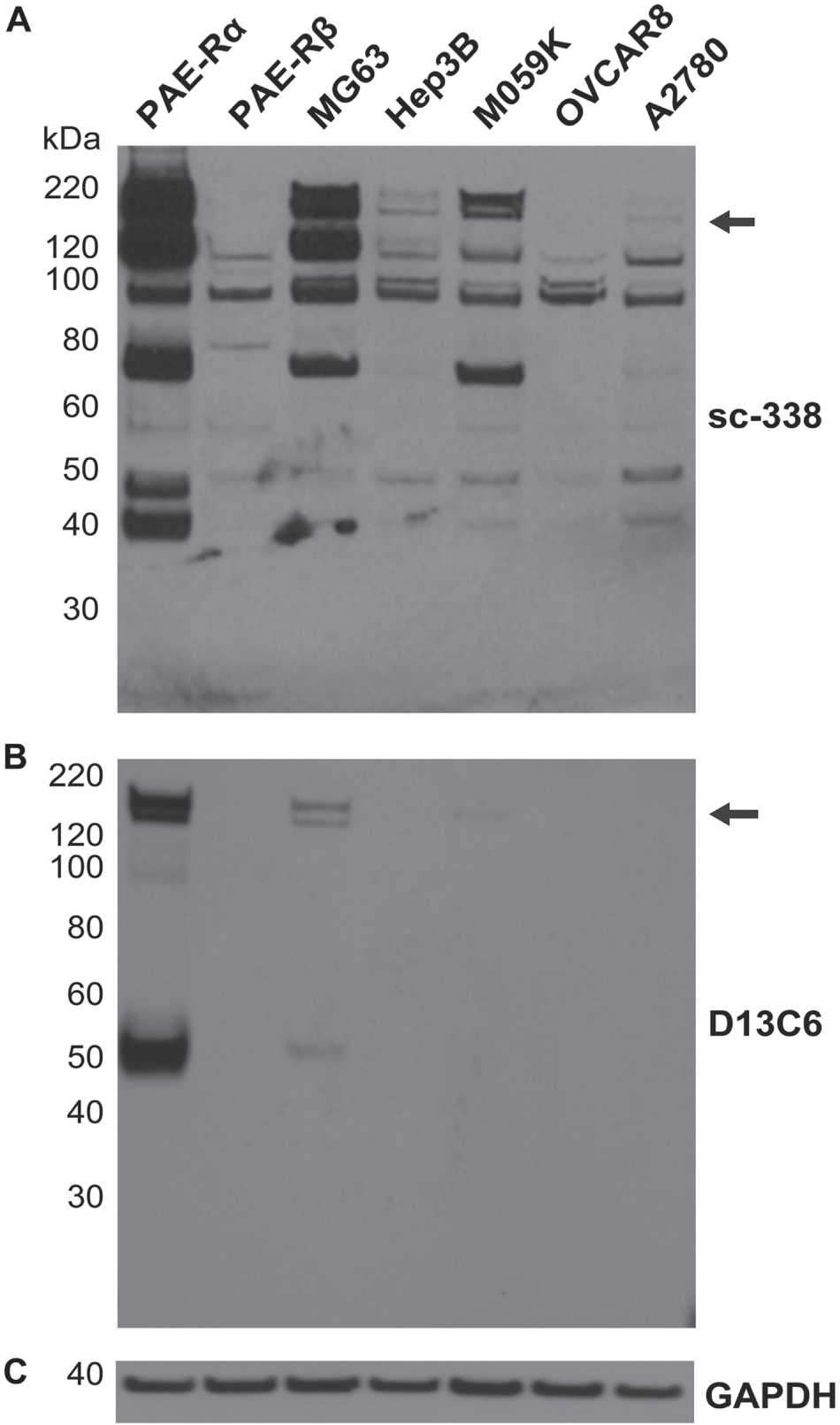
Immunoblot profiling of platelet-derived growth factor alpha (PDGFRα) on whole cell lysates using (A) anti-PDGFRα rabbit polyclonal antibody sc-338 or (B) anti-PDGFRα rabbit monoclonal antibody D13C6. Arrows show predicted size of PDGFRα at 190 kDa on each blot. (C) Glyceraldehyde 3-phosphate dehydrogenase was included to assess equal lysate loading, representative of both blots.
An aliquot of the control cell lines described above were formalin fixed and paraffin embedded (FFPE) and were intact after processing (Fig. 2A). An IHC assay based on the sc-338 antibody exhibited strong cytoplasmic immunoreactivity in all cell lines tested including non-PDGFRα expressing OVCAR8, and also had immunoreactivity present in nuclei (Fig. 2B). An independent IHC assay using the D13C6 antibody was developed following an assay development paradigm previously described. 33 This assay demonstrated a wider range of staining intensities from negative immunoreactivity (OVCAR8), through light cytoplasmic immunoreactivity (M059K), to more intense staining (MG63, Fig. 2C). The PDGFRα transfectants were the most intensely staining, whereas PDGFRβ-transfected cells were negative. Nuclei were essentially negative when the D13C6 antibody was applied. Positive M059K cells showed mainly cytoplasmic immunoreactivity and frequently exhibited a punctate pattern, whereas in MG63 cells, there was a higher frequency of positivity with cytoplasmic immunoreactivity and membranous accentuation (Fig. S1A). When directly comparing the immunoreactivity patterns between the two antibodies in MG63 cells, the heterogeneity and subcellular details observed when using D13C6 were lost when using sc-338 (Fig. 2B and C, insets; Fig. S1).
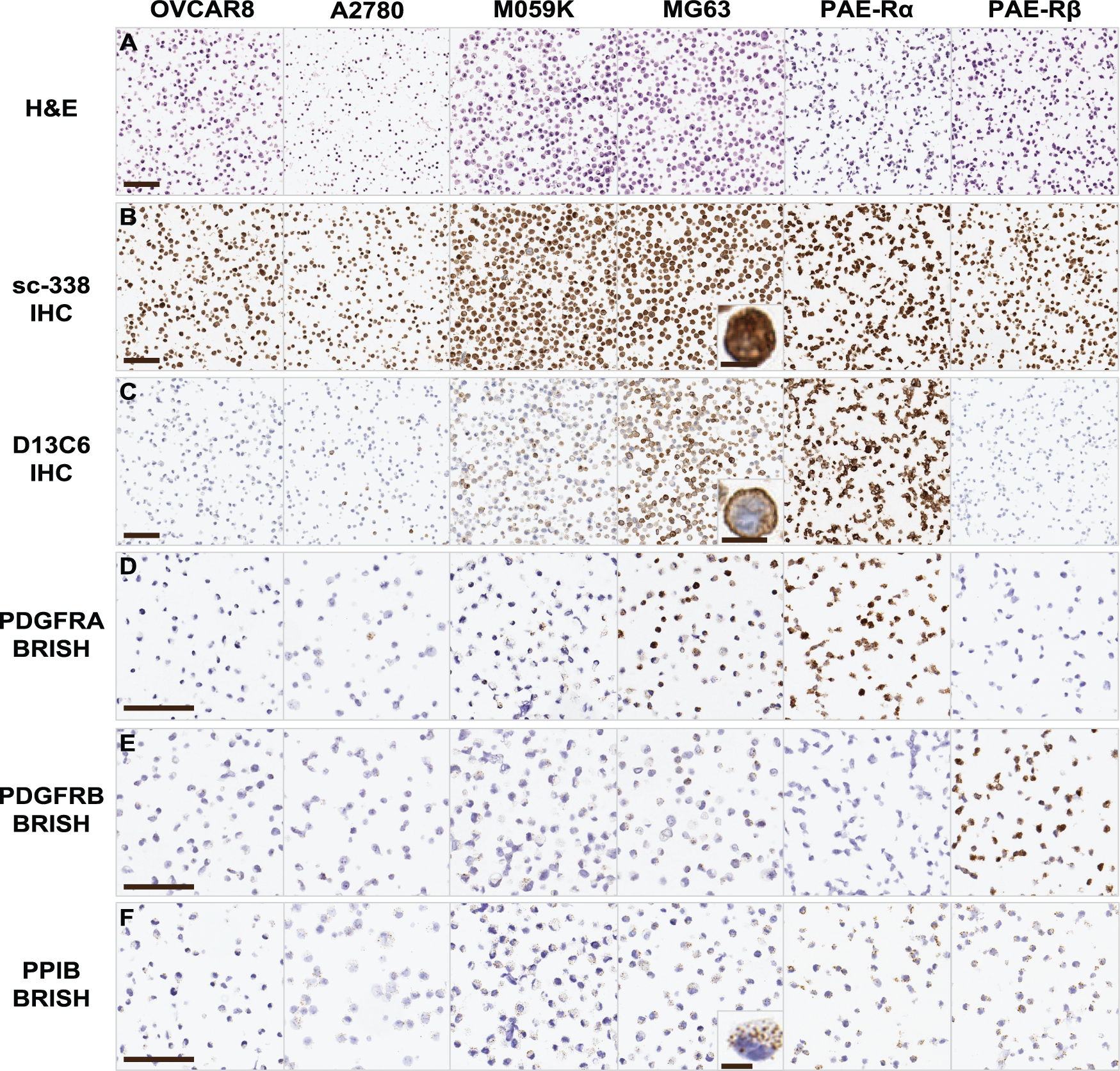
Representative high-resolution scans of formalin-fixed paraffin-embedded cell line preparations from select human tumor cell lines or transfectants: (A) H&E stain, (B) IHC (3,3′-diaminobenzidine) using anti-PDGFRα rabbit polyclonal antibody sc-338, or (C) anti-PDGFRα rabbit monoclonal antibody D13C6. ISH visualized by brightfield microscopy is shown using probes designed to detect (D) PDGFRA, (E) PDGFRB, or (F) quality control peptidylprolyl isomerase B (PPIB) mRNA. Porcine aortic endothelial (PAE) cells stably transfected with PDGFRA (Rα) or PDGFRB (Rβ). Slides used for IHC and BRISH were counterstained with hematoxylin (blue). Scale bars in OVCAR8 panels represent 100 µm and are applicable to subsequent panels. Scale bars in insets represent 10 µm. Abbreviations: H&E, hematoxylin and eosin; BRISH, brightfield in situ hybridization; PDGFRα, platelet-derived growth factor alpha.
To further qualify the selection of cell lines for PDGFRα comparisons, ISH for PDGFRA and PDGFRB mRNAs was performed and then visualized by brightfield microscopy (BRISH; Fig. 2D and E). BRISH was also performed using a probe designed against the gene PPIB, to ensure that mRNA was present and detectable in all cell lines (Fig. 2F). Chromogenic signal for BRISH appeared as discrete round dots approximately 1 µm in diameter (Fig. 2F, inset). Based on automated image analysis of high-resolution digital scans of the slides of OVCAR8, M059K, and MG63 cell lines, BRISH was consistent with predicted mRNA levels. However, in our hands, A2780 displayed the lowest expression by BRISH but exhibited consistency between BRISH and IHC signal. PDGFRA message was positively associated with IHC for the D13C6 antibody, exhibiting a range of ODs of 0.19 (arbitrary units, Fig. 3). IHC using sc-338 was also positively associated with PDGFRA message; however, it spanned a smaller dynamic range of 0.13 units. The difference between average ODs for each antibody for each independent cell line was statistically significant (p<0.0008, paired t-test), and across all cell lines, the median immunoreactivity of the sc-338 antibody was approximately fourfold higher than that of the D13C6 immunoreactivity.
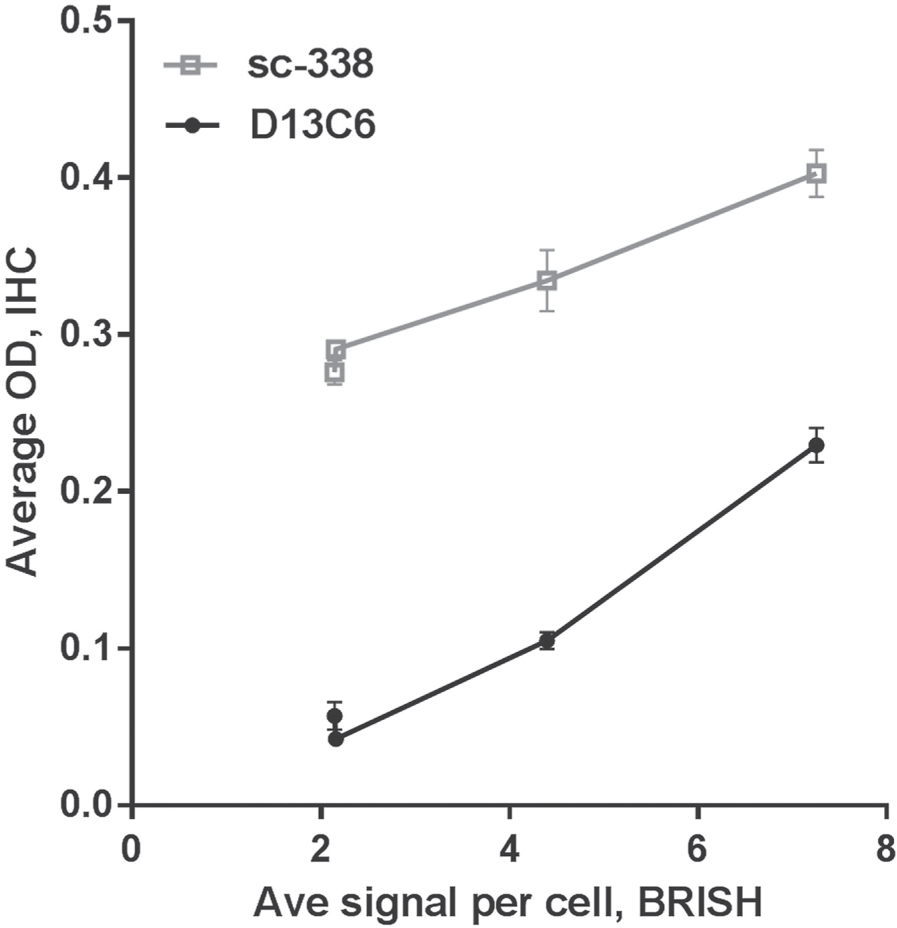
High-resolution digital images were assessed by automated image analysis to quantify. Average OD for immunoreactivity and average signal per cell were determined for replicate fields of view for IHC and BRISH signal, respectively. Error bars represent standard deviation. The difference between average ODs for each antibody for each independent cell line was statistically significant (p<0.0008, paired t-test). Abbreviations: OD, optical density; BRISH, brightfield in situ hybridization.
To distinguish between contributions from the antibody specificity and antibody concentration, sc-338 antibody was diluted until true negative signal was observed in cells known to be negative for PDGFRα by immunoblotting and BRISH (Fig. 4A). For cell lines including transfected cells, this dilution of antibody sc-338 remained positive in lines expected to be positive, with expected diminished signal strength due to dilution. However, at this concentration (0.10 µg/ml), no sc-338 immunoreactivity was observed on FFPE tumor specimens (Fig. 4B).
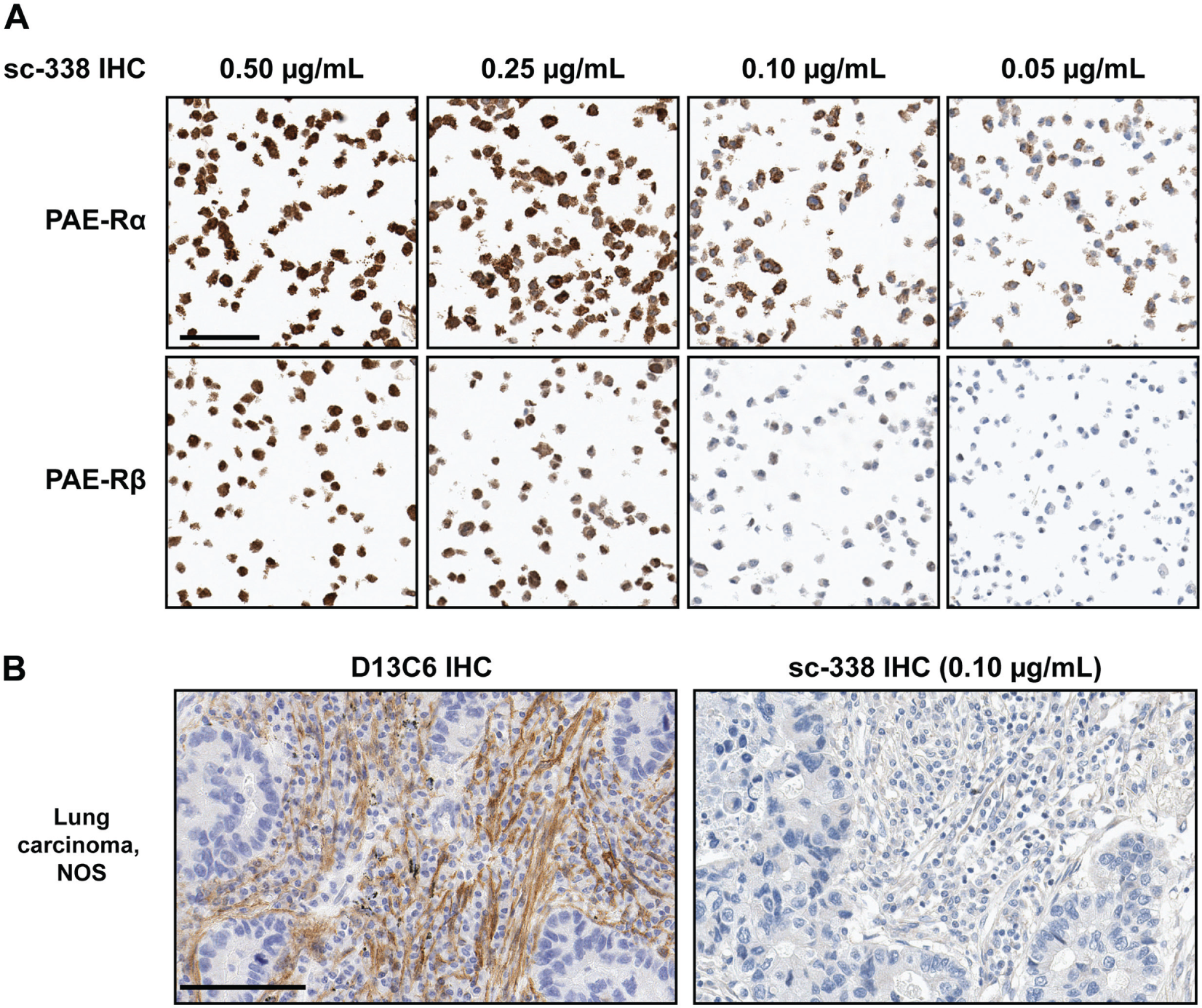
(A) IHC using sc-338-based assay at the indicated concentrations of primary antibody. (B) Comparison for the two IHC assays on a single case of lung carcinoma, not otherwise specified (NOS). The selection of the primary antibody concentration for sc-338 was based on the concentration that showed the maximum differences in immunoreactivity in panel A. All scale bars represent 100 µm and are applicable to subsequent panels. Slides were counterstained with hematoxylin (blue).
PDGFRα IHC Using Clone D13C6 Exhibits Immunoreactivity Patterns in Tumor Tissues Consistent With mRNA Detection
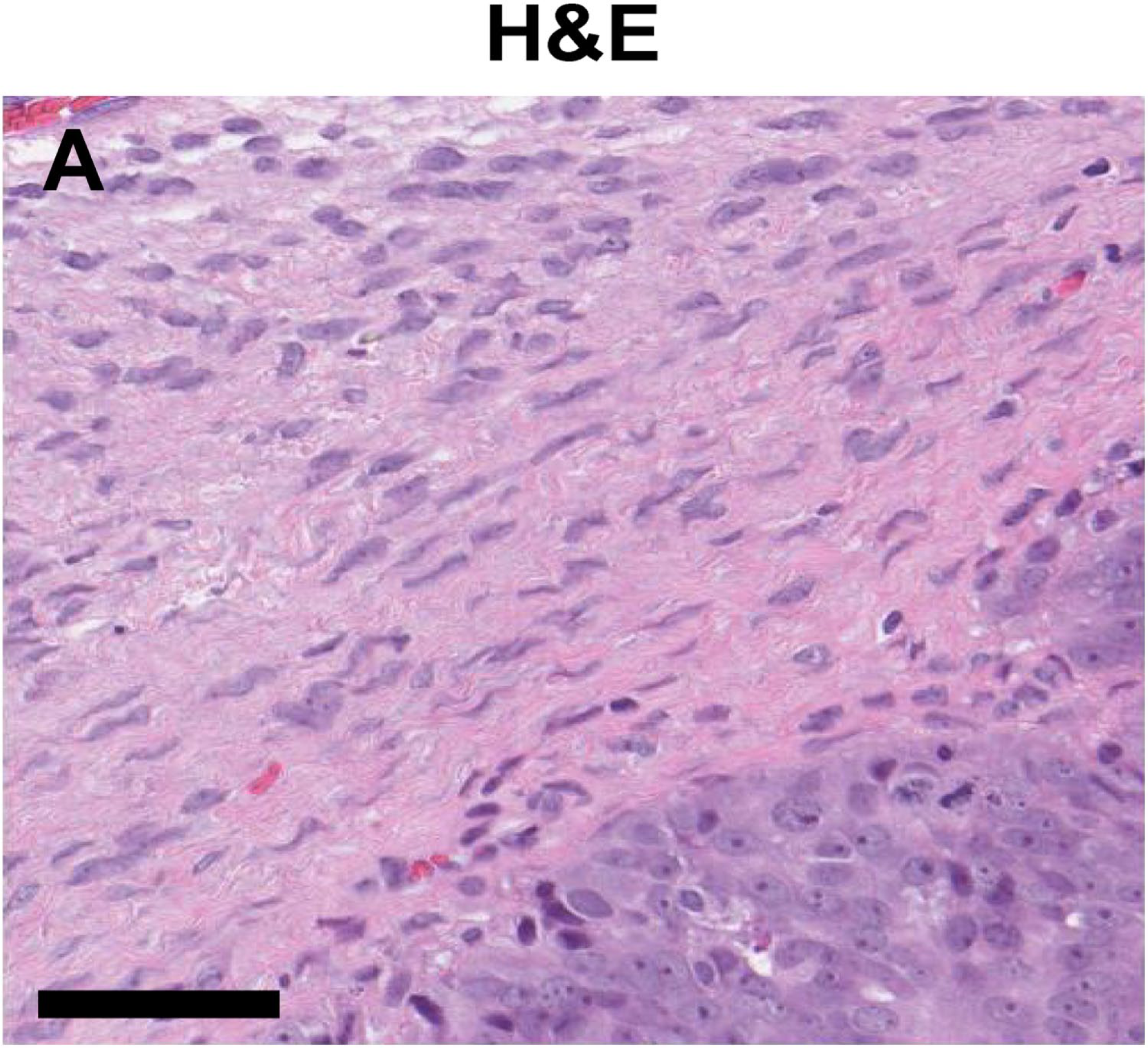
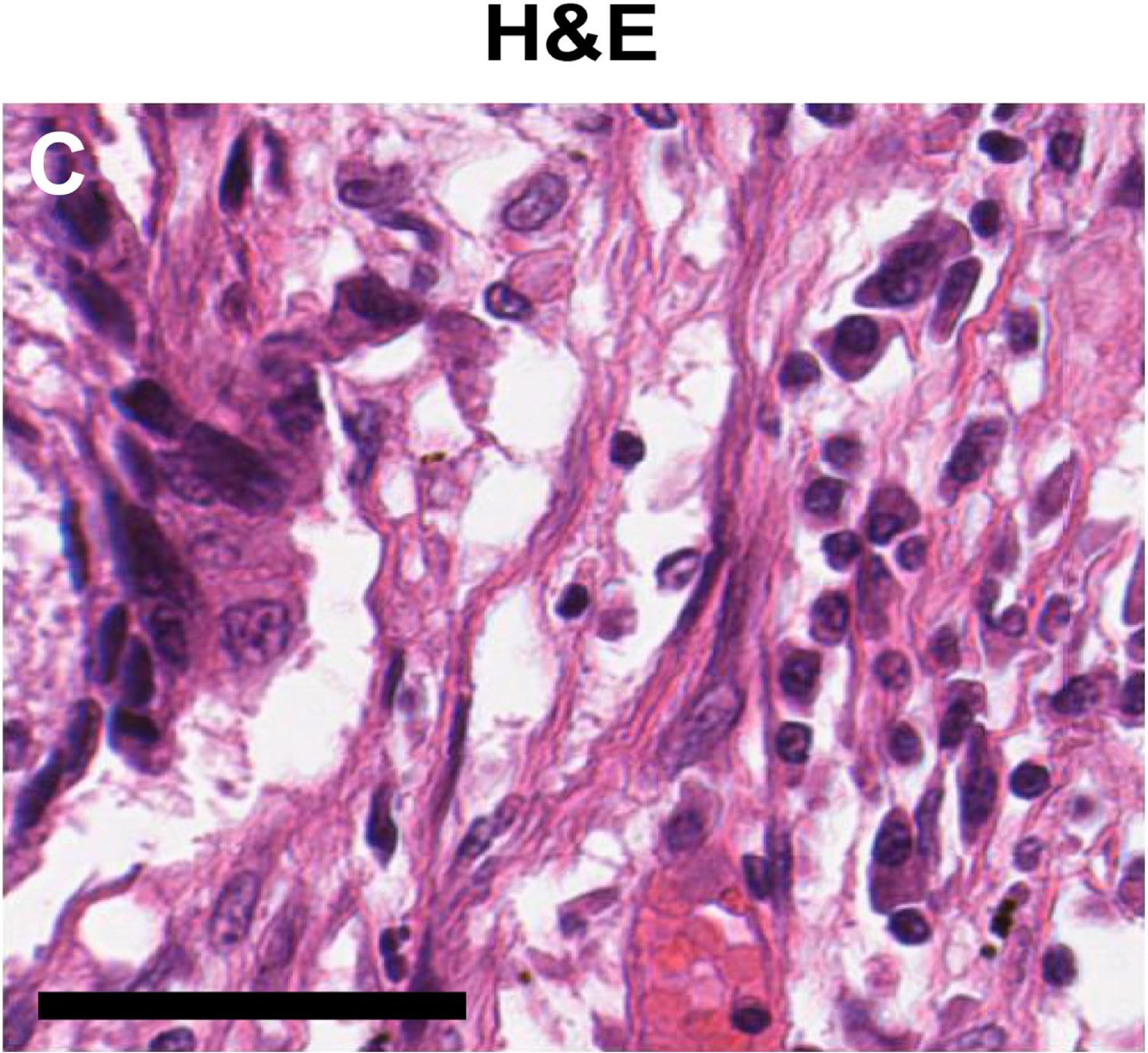
The D13C6-based IHC assay was optimized for detection of PDGFRα in a variety of FFPE tumor tissues, including tumors of the lung and ovary. Expression was largely present in fibroblast-derived cells of the tumor associated stroma, consistent with the known biology of the receptor. Representative results showed a range of expression: intense in a case of ovarian serous papillary carcinoma (Fig. 5A), moderate expression in two cases of squamous cell carcinomas of the lung (Fig. 5B and C), low in mucinous carcinoma of the ovary (Fig. 5D), and negative in a case ovarian endometrioid adenocarcinoma (Fig. 5E). A rabbit isotype IHC control was used in place of primary antibodies to ensure that no signal was produced from nonspecific interactions with rabbit IgG (Fig. S2).
Editor’s Highlight
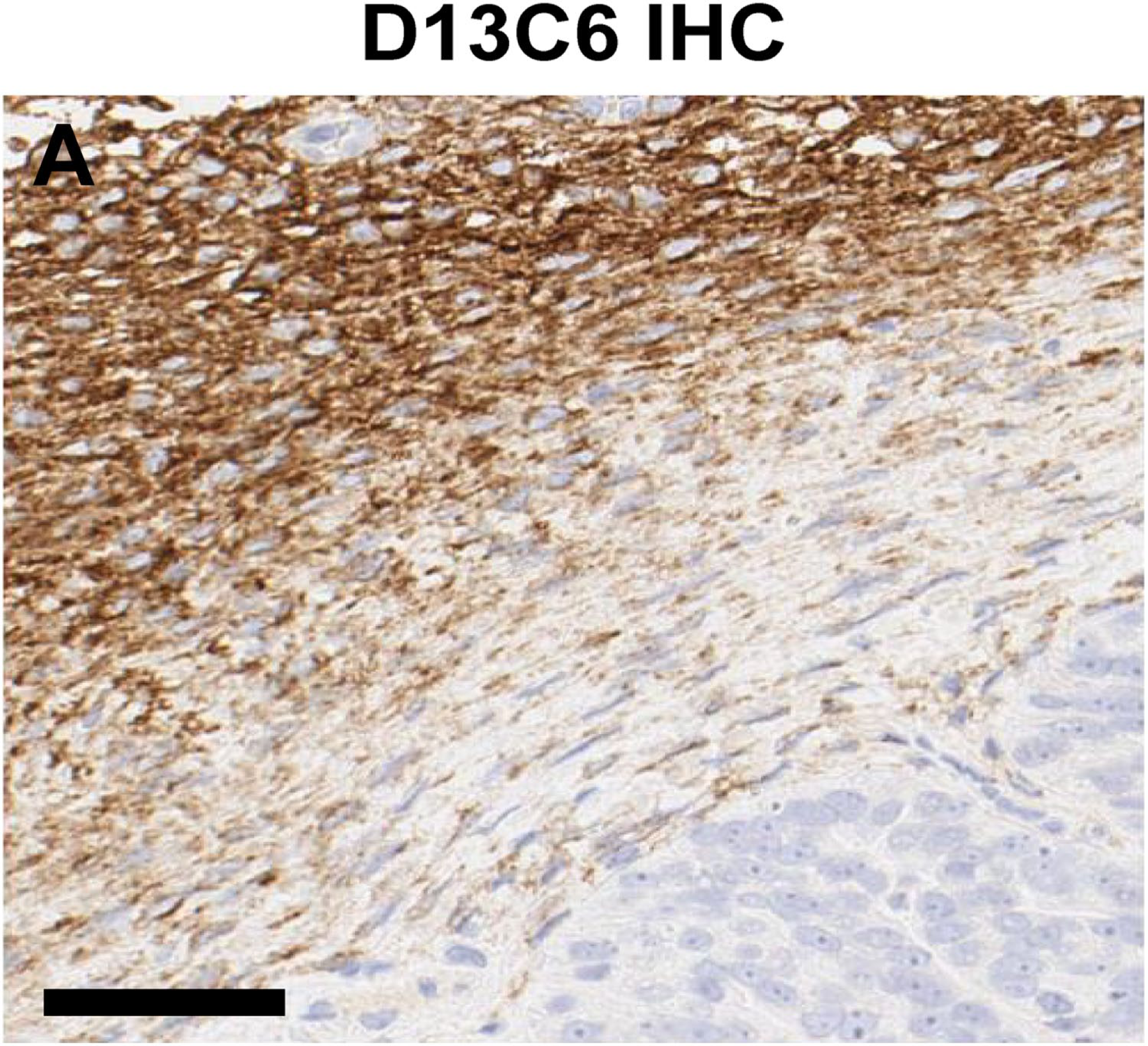
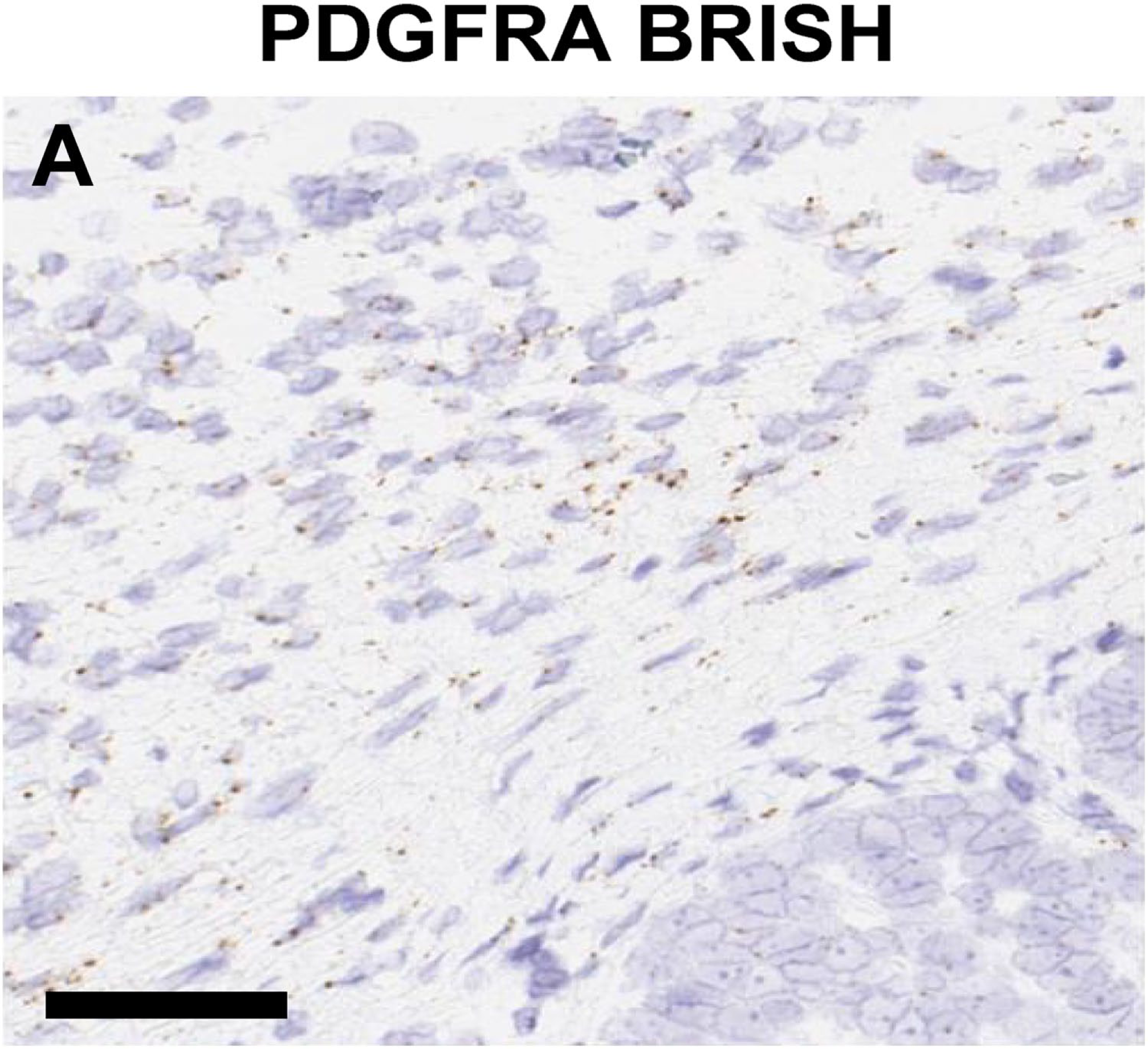
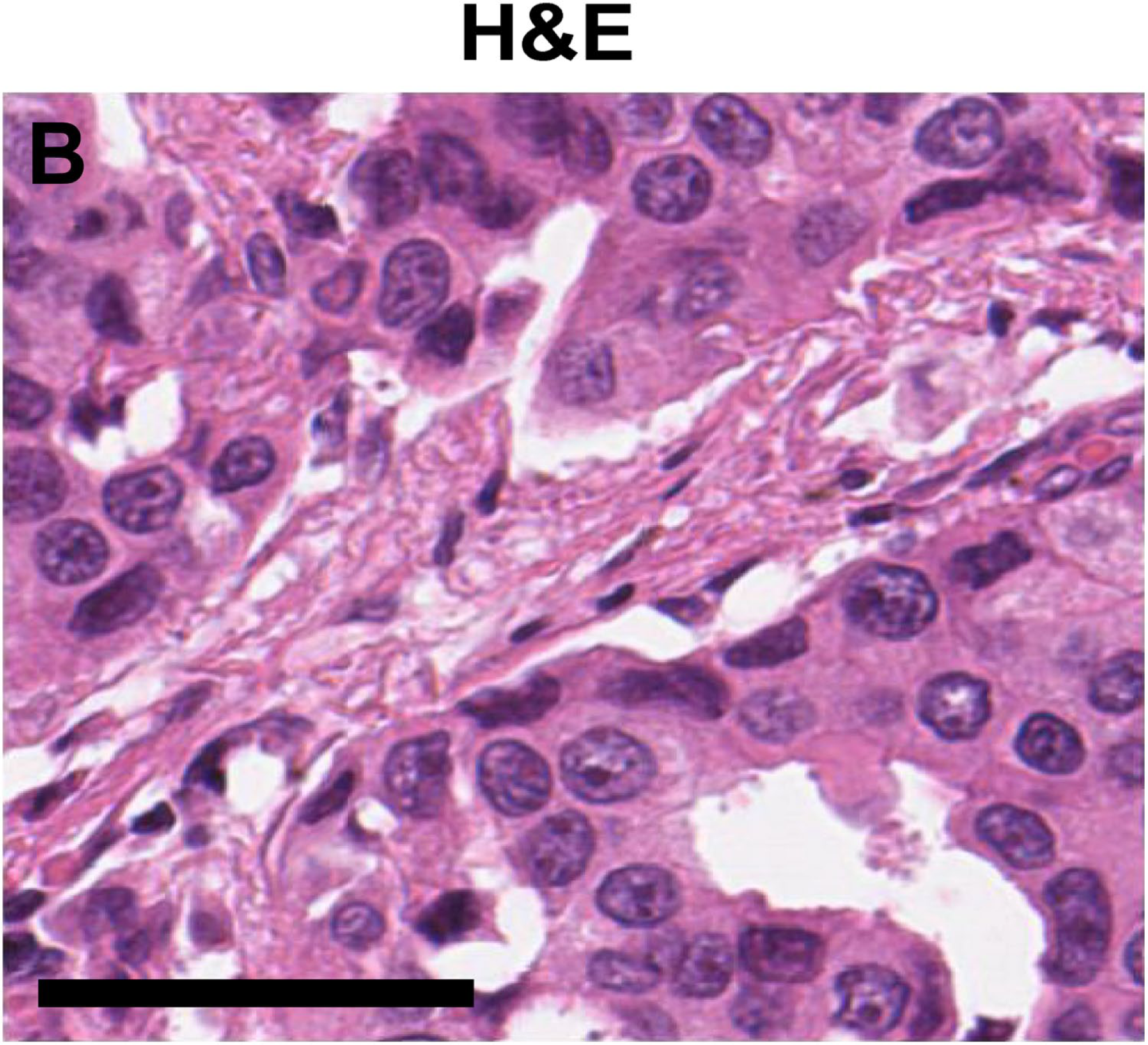
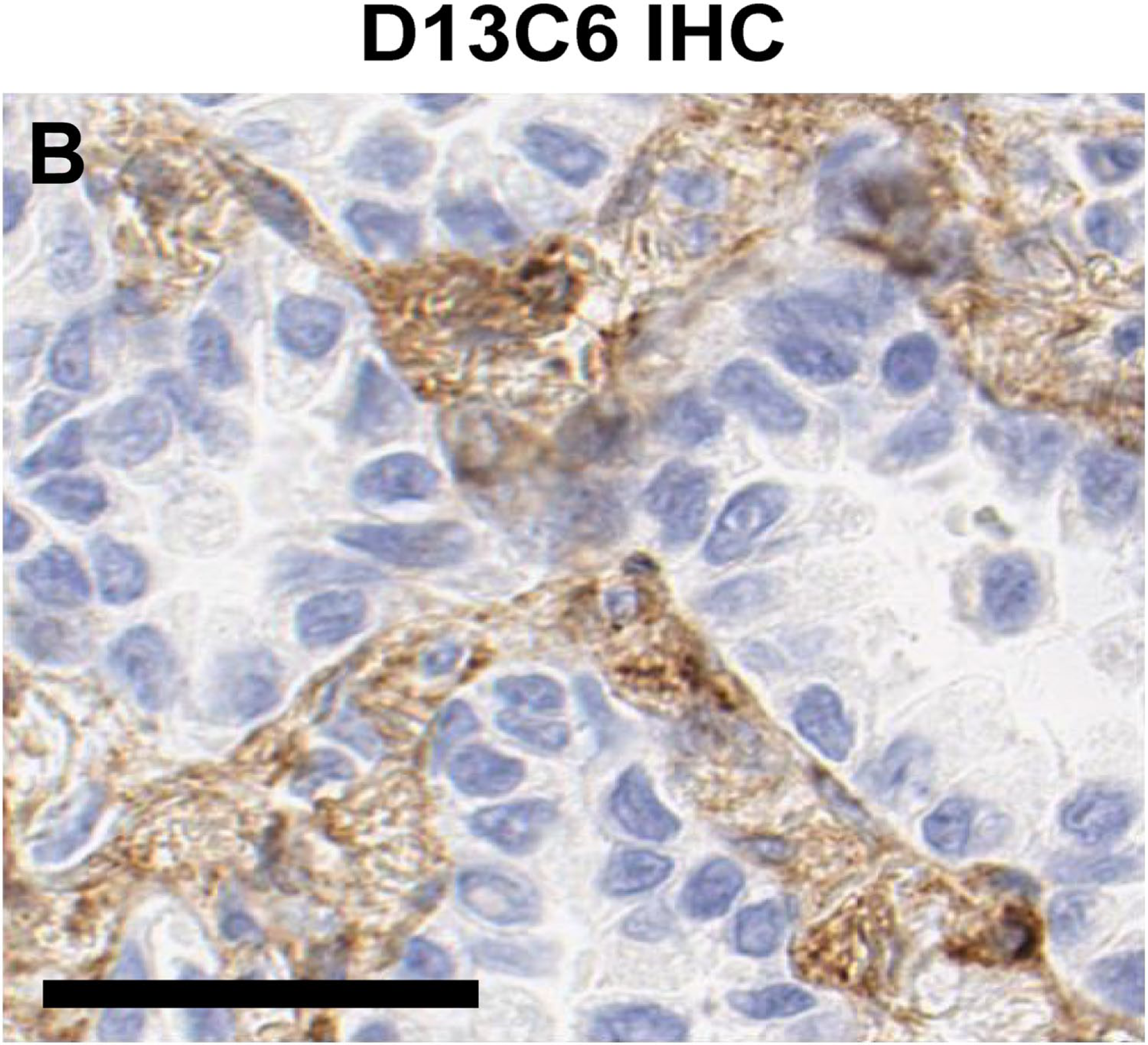
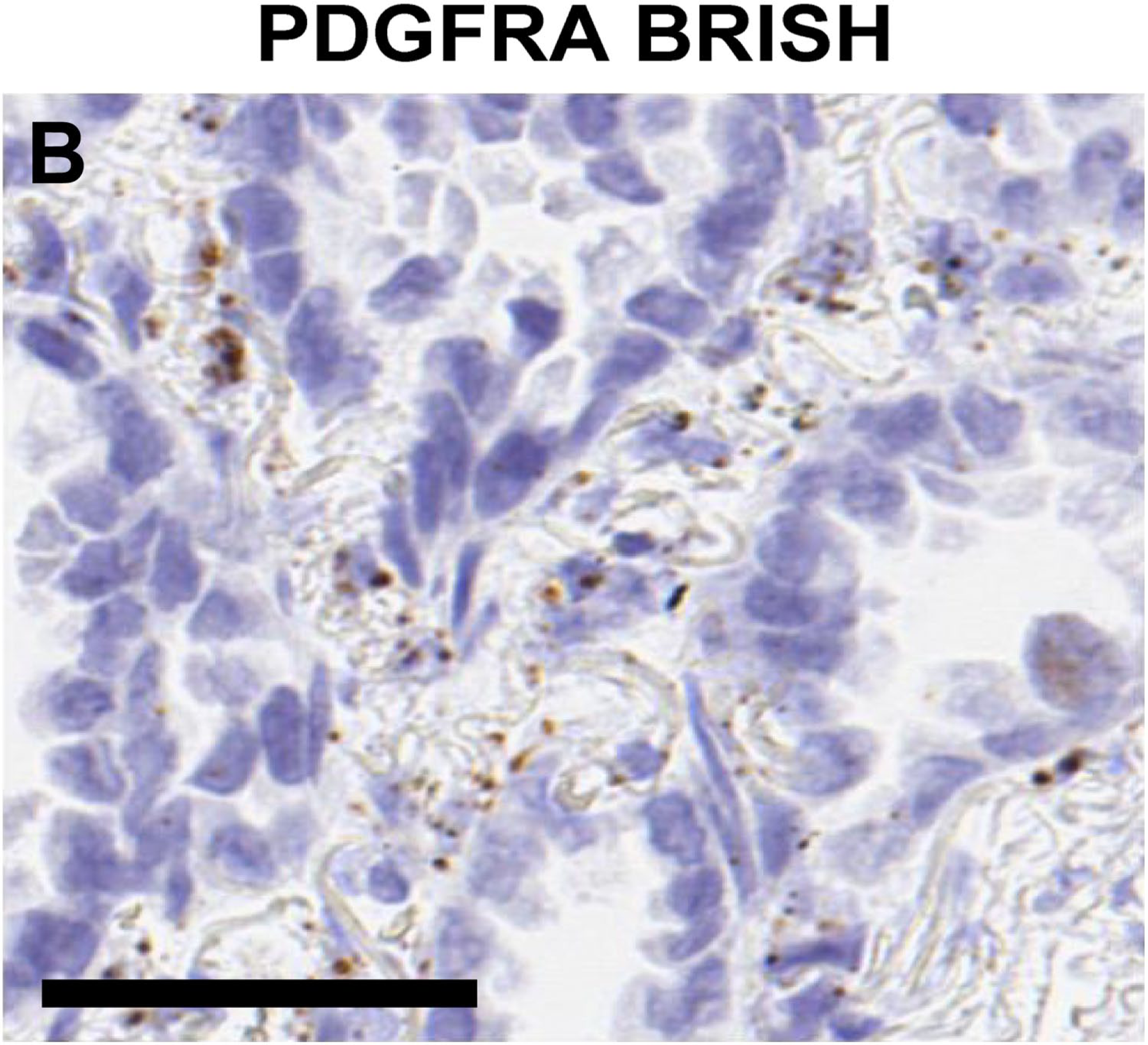
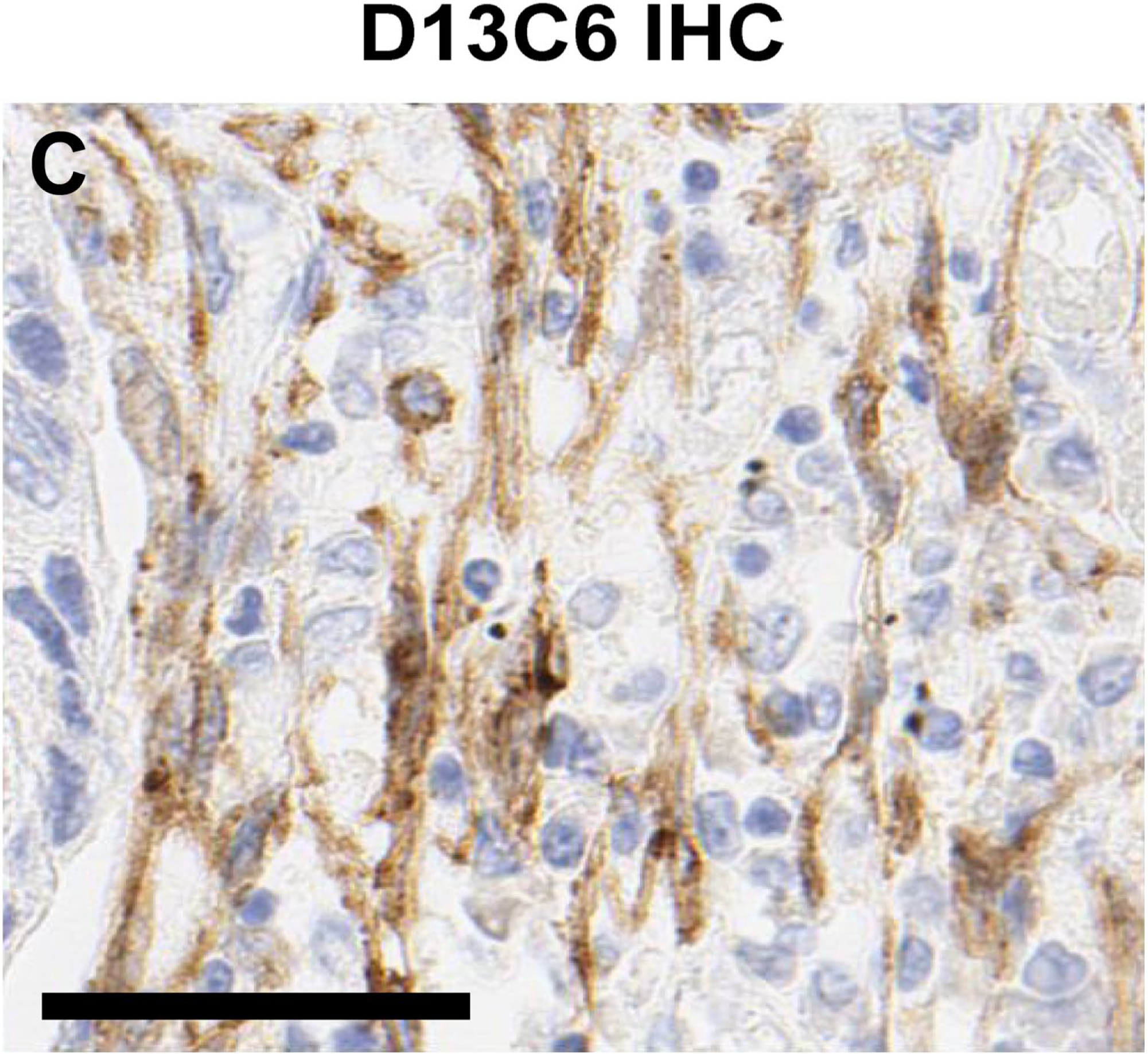
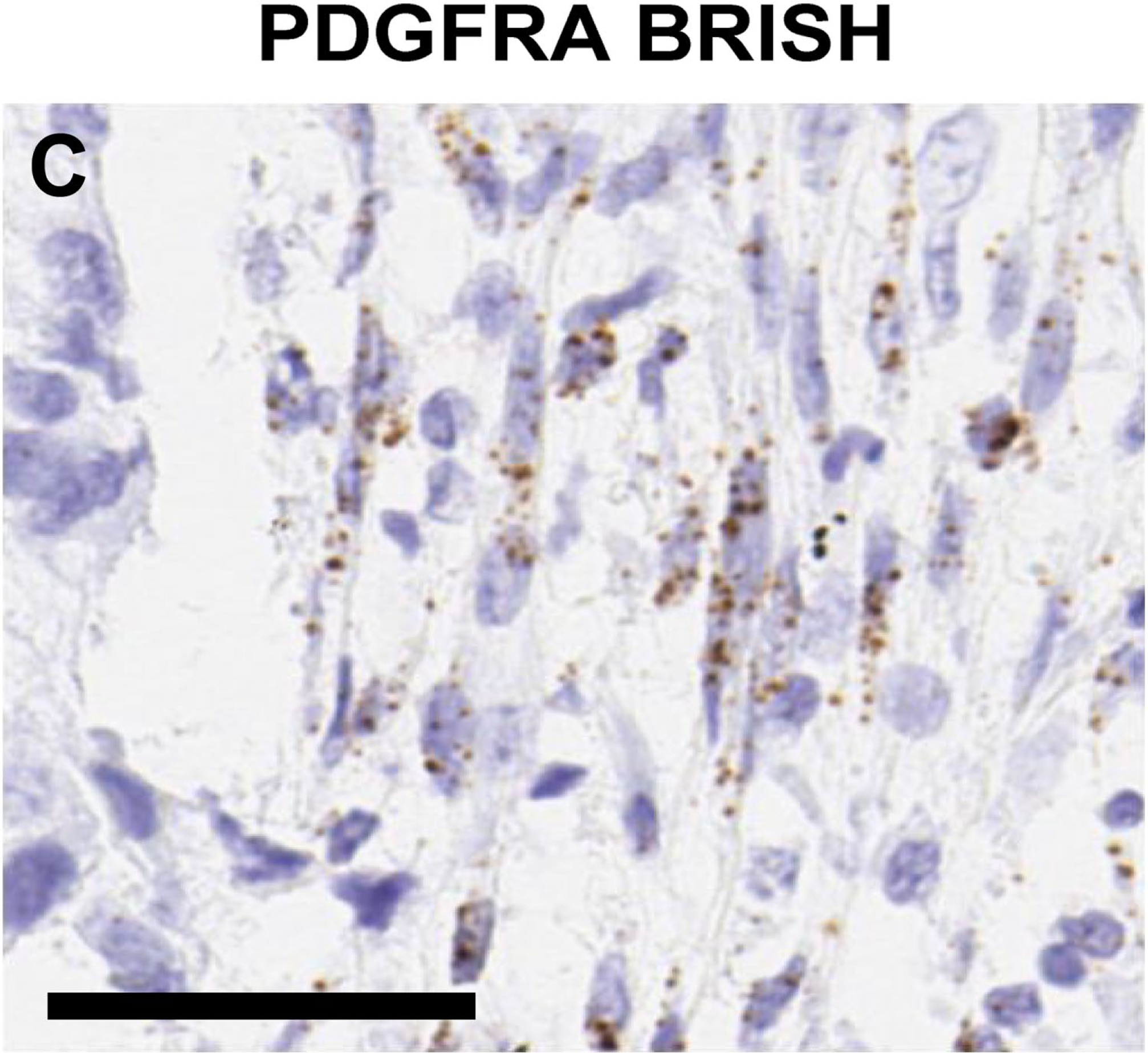
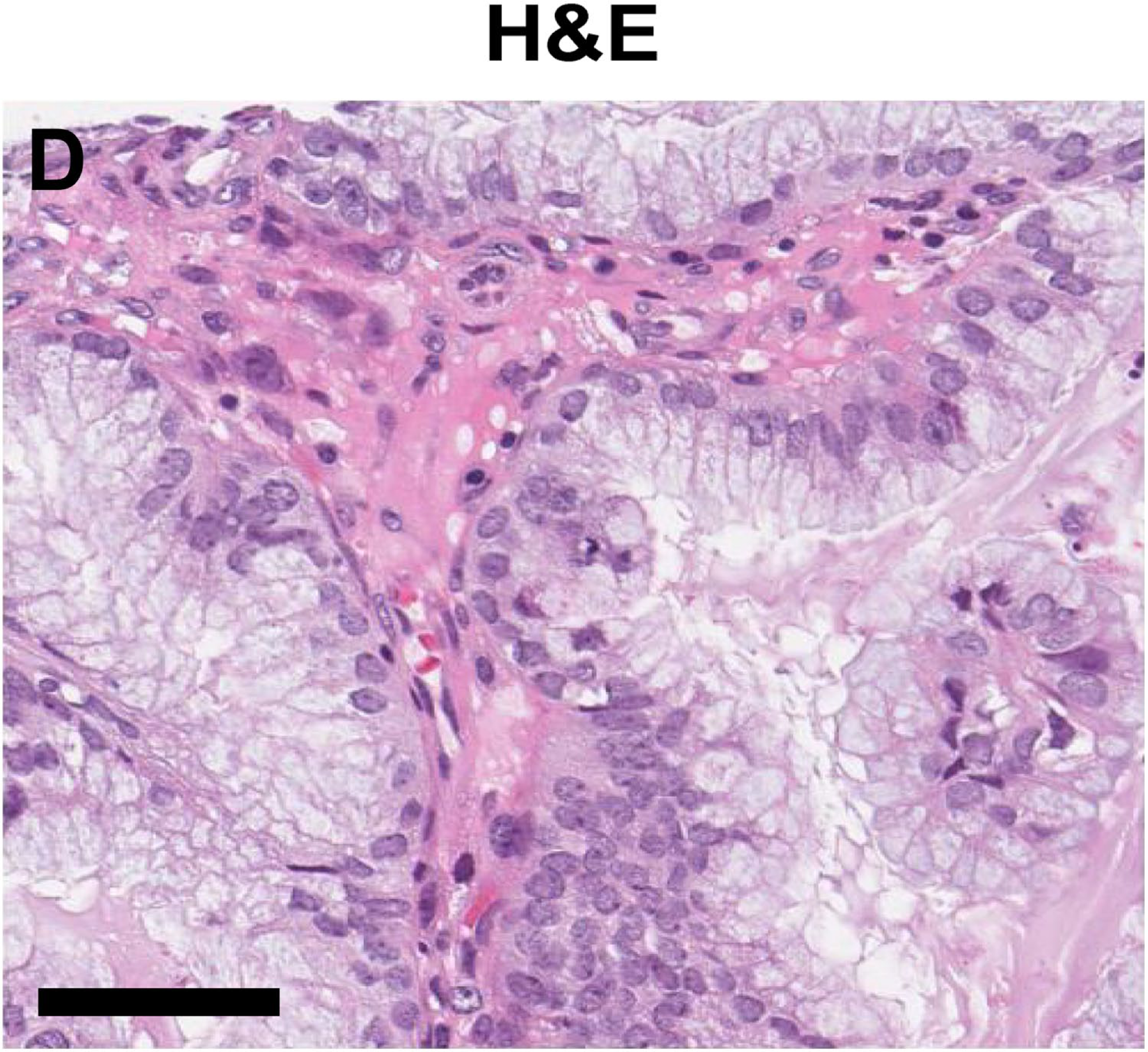
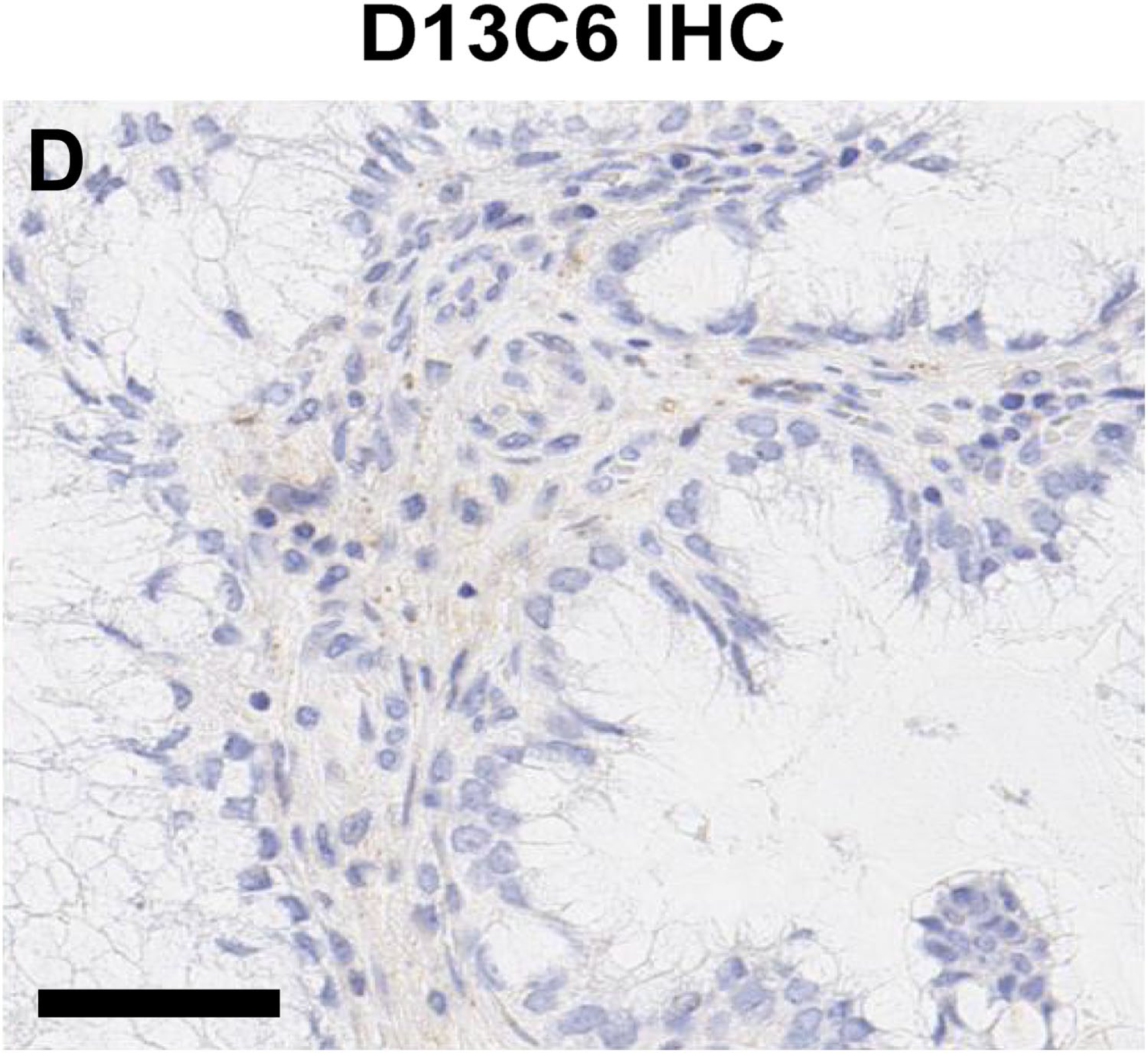
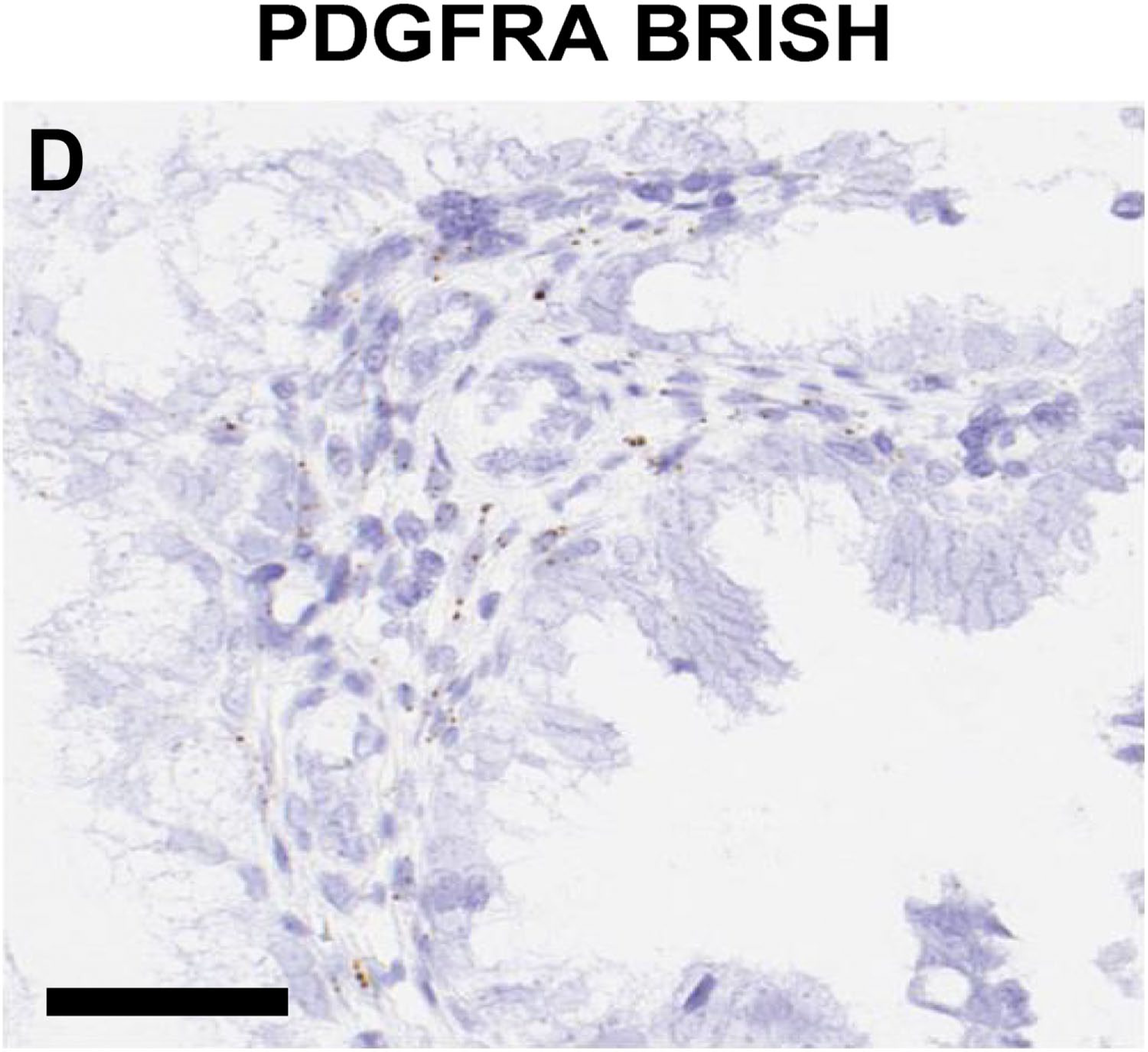
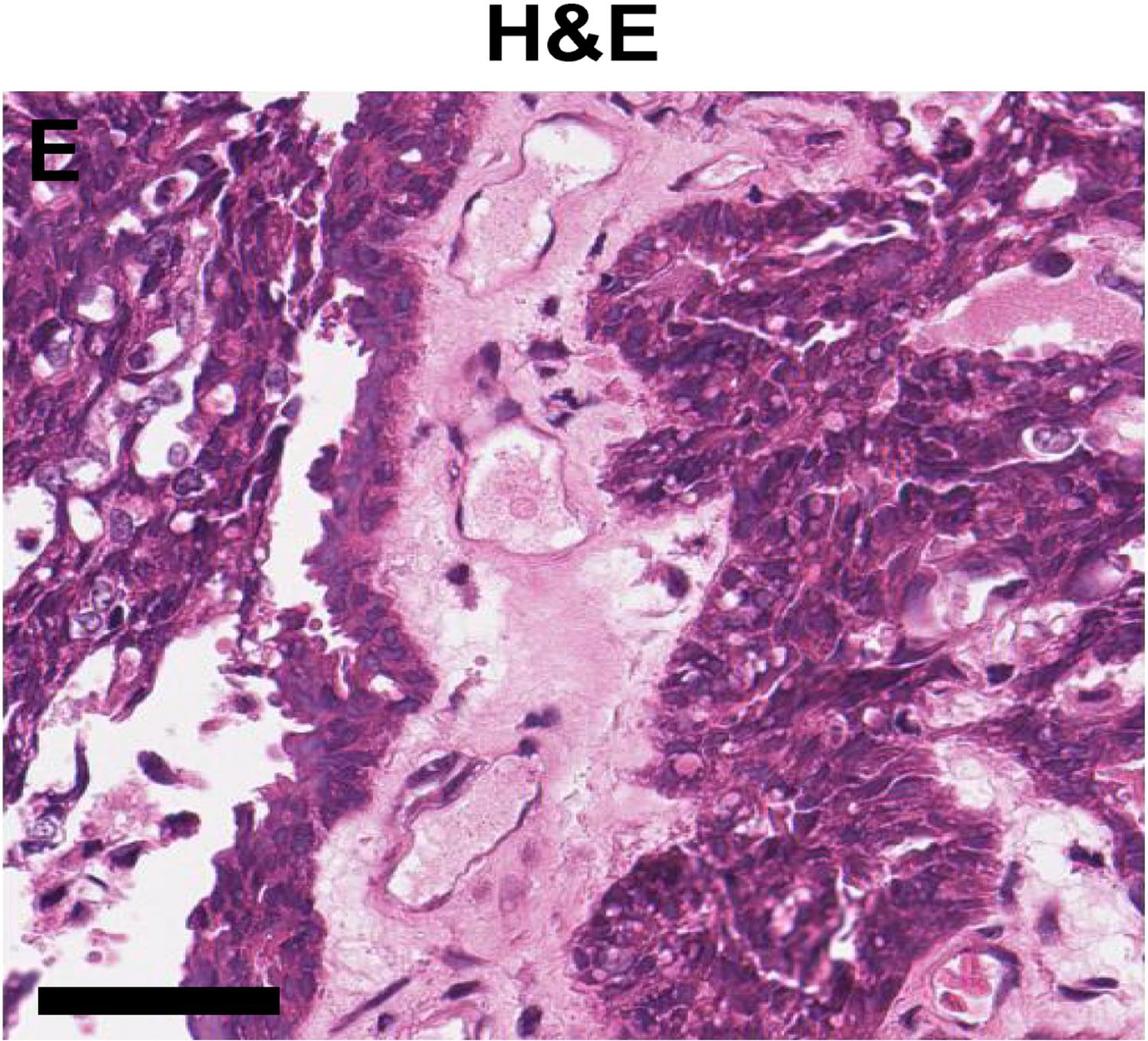
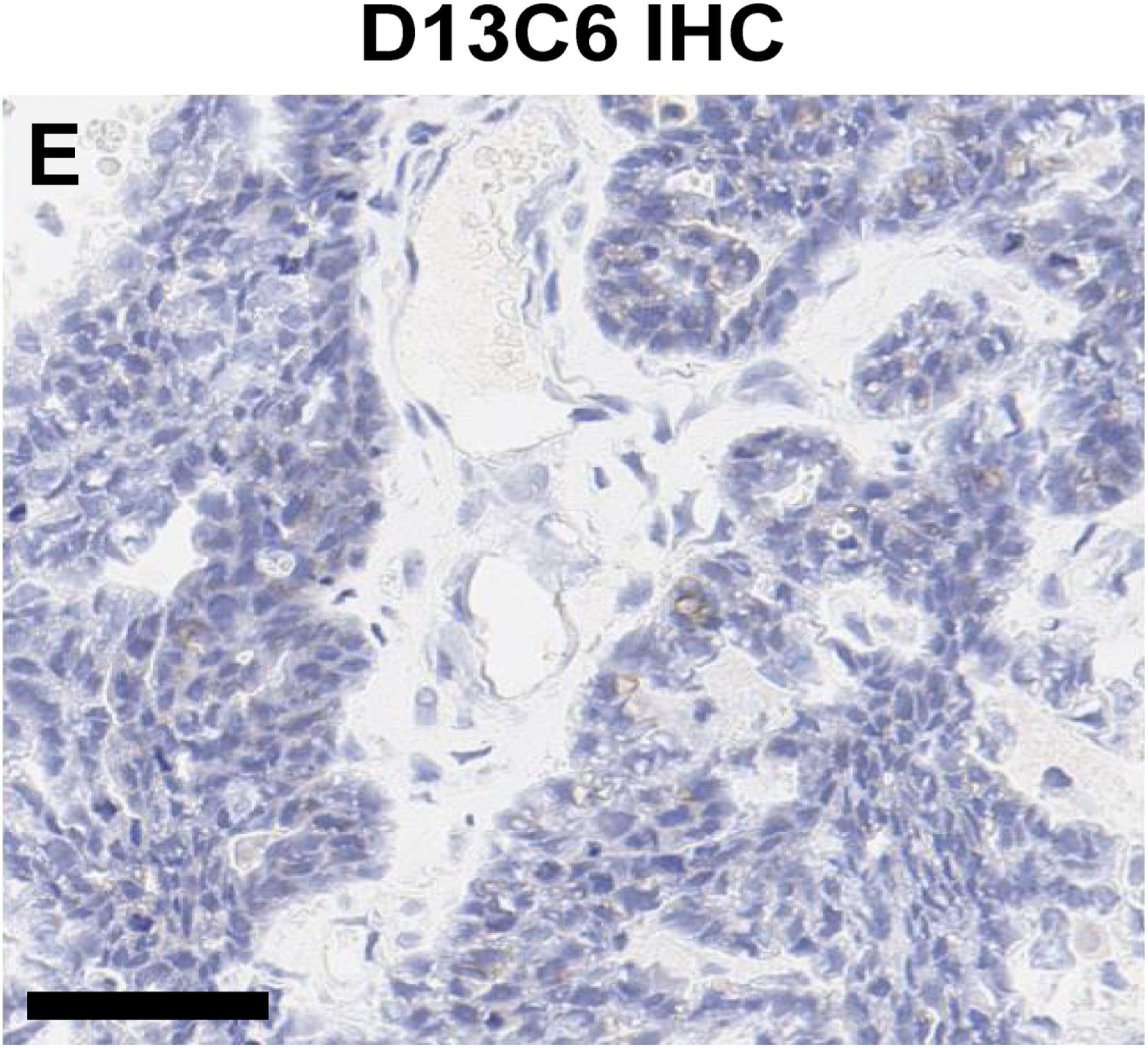
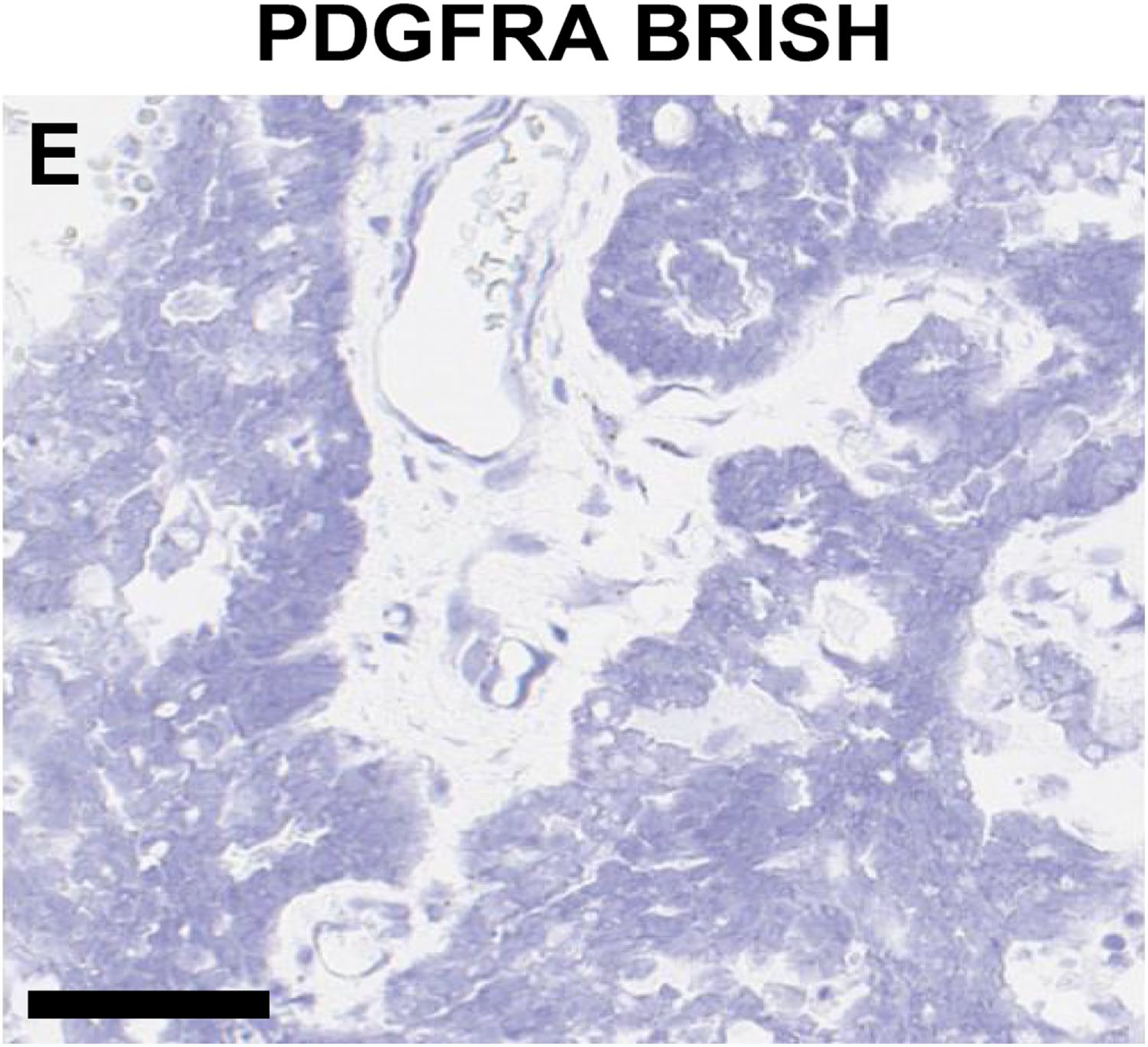
A series of BRISH assays were performed on the human lung and ovarian carcinoma tissues. First, PPIB BRISH was used to confirm each human tumor tissue block was fixed and processed appropriately and that mRNA was preserved. Next, a probe designed to detect the bacterial gene dapB was applied to ensure that there was no background signal (Fig. S3). Finally, PDGFRA BRISH was performed. Comparisons of PDGFRA mRNA localization with PDGFRα protein localization on each case were consistent with the immunoreactivity patterns observed when performing IHC with the D13C6 antibody (Fig. 5).
Discussion
We have described a considerable difference in analytic performance between two commercially available antibodies for PDGFRα. This difference was potentially attributable to the polyclonal versus monoclonal nature of the antibodies, the recognition of different epitopes on the receptor, or differences due to epitope retrieval in the IHC methods. However, the data suggested that sc-338-based IHC performed on an automated platform commonly used in pathology laboratories 34 had insurmountable technical issues regarding specificity. The monoclonal antibody D13C6, in our hands, appeared specific for the intended PDGFRα target.
Description of the antibody clone and detailed IHC procedures used in the methods sections of scientific publications is a recent and unevenly applied requirement across the many scientific journals. Use of anti-PDGFRα antibody sc-338 is described in studies in human small cell lung carcinomas, 30 GISTs,12,29 chondrosarcomas, 27 and renal cell carcinomas. 28 Dissimilar information about assay development is provided in these studies with only some describing sc-338 working dilutions (1:200–1:100) and which platforms and reagents were used for automated IHC. At this working concentration, the IHC results using sc-338 in this report showed nonspecific staining, including potential cross-reactivity. The observed homogeneous and diffuse immunoreactivity characteristics (Fig. S1) were consistent with other reports of immunoreactivity of sc-338, even when a different automated platform was used. 35 For ovarian carcinoma, a relationship between high PDGFRα assessed by IHC in tumor cells and lower overall survival has been reported.36,37 However, there is conflicting evidence of prognostic value for PDGFRα IHC using antibody sc-338 in which no association with overall survival was observed. 35 This highlights the potential impact of antibody selection and IHC optimization when used for clinical interpretation. Rigorous validation methods to evaluate IHCs for appropriate analytic variables are essential, and as such, IHC development paradigms have been proposed.38,39
We recognize the potential for reports of IHCs used in an exploratory or research setting to influence the selection of antibodies and assays for intended use in a clinical setting. If PDGFRα IHC should ever be required as a prognostic or therapeutically predictive biomarker, careful attention to the antibody clone used and interpretation criteria based on the analytic performance of that clone to maximize clinical utility is necessary. 26 Furthermore, given the discrepancy in analytic specificity for PDGFRα between the two antibodies in this study, different interpretation criteria can be easily envisioned as necessary if the antibodies are used for the same purpose. For example, the lack of PDGFRα specificity of the sc-338 antibody could produce a much higher rate of qualitatively “positive” results for this receptor. Interpretation criteria would need to be adjusted on an antibody versus antibody basis to reflect this propensity. As was demonstrated, dilution of the sc-338 antibody to correct analytic specificity compromised the ability of the antibody to detect the target on FFPE tumor tissues. The variable analytic sensitivity and specificity of antibodies, particularly among different clonal origins of the antibodies, and the desired objective nature of clinical IHC require appropriate analytical validation.40–42
Our data preclude the use of antibody sc-338 for IHC as research grade assay or for development of clinical biomarkers. We recommend the use of antibody D13C6 as an alternative.
Footnotes
Acknowledgements
The authors thank Drew Nedderman, Angie Fulford, Jim Alston, and Darryl Ballard (Eli Lilly and Company) for critical support on automated brightfield in situ hybridization development and numerous runs. They recognize Colleen Burns (Lilly) for IHC studies and antibody information. They also thank Brittany Schroer and Jason Bailey (Lilly) for summarizing recent reports pertinent to the current study.
Competing Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
TRH, LOR, KMC AES, and GJO conceived and designed the IHC development studies. TRH, LOR, and GJO collected and organized data. TRH, LOR, KMC, AES, and GJO analyzed and interpreted data. TRH, LOR, KMC, AES, and GJO wrote the manuscript. All authors have read and approved the final manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funder, Eli Lilly and Company, provided support in the form of salaries for all coauthors but did not have any additional role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.