
Abstract
BUBR1 (budding uninhibited by benzimidazole-related 1) represents the component of a controlling complex in mitosis. Defects in mitotic control complex result in chromosomal instability and, as a result, disturb the mitotic process. This study was aimed at examining the prognostic value linked to the expression of BUBR1 in a group of patients with breast cancer. We analyzed the expression of BUBR1 in 98 stage II breast cancer patients with a median follow-up of 15 years. Immunohistochemical reactions were performed using monoclonal antibodies against BUBR1. We also studied the prognostic value of BUBR1 mRNA expression using the Kaplan-Meier (KM) plotter, which assessed the effect of 22,277 genes on survival in 2422 breast cancer patients. A background database was established using gene expression data and survival information on 2422 patients downloaded from the Gene Expression Omnibus (GEO; Affymetrix HGU133A and HGU133+2 microarrays). The median relapse-free survival was 6.43 years. Univariate and multivariate analyses showed that higher expression of BUBR1 was typical for cases of shorter overall survival, disease-free time, and disease-specific survival. KM plotter analysis showed that elevated BUBR1 mRNA expression had a negative impact on patients’ relapse-free, distant metastases–free, and overall survival. Elevated BUBR1 expression was associated with poor survival in early stage breast cancer patients.
The incidence of breast cancer has been continuing to increase for many years and, currently, it represents the most frequent malignancy in females (Ferlay et al. 2010). Progress gained in the control of the disease reflects mainly the widespread use of mammography, an increased number of patients treated at early stages of the disease, and well-designed and effective therapy. Much less favorable results for treatment are obtained in patients with more advanced stages of the disease. Therefore, new ways are being investigated to improve efficacy of the applied therapy.
At present, indications for the application of individual methods involving systemic treatment are based on an analysis of prognostic factors. On the other hand, factors that define the probability of obtaining remission following the application of a specific therapeutic method are expressed by predictive indices (Goldhirsch et al. 2009). The knowledge of predictive factors is much more restricted than that related to prognostic factors. An urgent need is noted for studies aimed at identification of the former (Nasir et al. 2011). This study aimed to define patient groups with possibly the highest chance for remission following administration of a specific manner of treatment. This would help to avoid ineffective and thus needless treatment with toxic drugs (Goldhirsch et al. 2009).
One of the interesting areas in recently conducted studies involves the prognostic evaluation of markers linked to the function of control points in cell division. In a group of compounds, a mechanism can be distinguished that controls the process of chromosome segregation, also termed the spindle assembly checkpoint (SAC) (Du et al. 2011). When abnormalities occur in the function of the SAC, defects develop in the structure of descendant cells, most frequently leading to aneuploidy, which can be noted in several types of human neoplastic cells. Nevertheless, it still remains unclear whether the acquired aneuploidy in some way speeds up tumor progression in humans and, if so, how aneuploidy facilitates the progression of cancer (Weaver and Cleveland 2007). Several lines of evidence point to a significant effect of errors in the mitotic control system on the manifestation of chromosomal instability, which shows that analyses of the processes are justified (Nasir et al. 2011). The activity of a certain group of compounds involves the reestablishment of the normal course of mitosis as soon as abnormalities in chromosomal divisions are recognized. Detection of such abnormalities results in blocking of the process before the subsequent phase of anaphase. Occasionally, the division process is only periodically blocked before the time point in which all chromosomes are properly linked to the spindle (Weaver and Cleveland 2007; Bolanos-Garcia and Blundell 2011).
Among methods to follow these anomalies, an evaluation of BUBR1 (budding uninhibited by benzimidazole-related 1) activity seems particularly interesting as the protein represents the principal component in the complex that controls the mitotic process. The mitotic kinase, BUBR1, also called BUB1B by the Human Genome Organization, represents an important controlling component of the karyokinetic spindle (Nasir et al. 2011). In the course of a correct mitotic process, achievement of an appropriate segregation of sister chromatids requires that they are attached to opposite poles of the spindle (bipolar orientation) through two kinetochores. Only such a pattern can ensure that each of the two daughter cells will receive one chromosomal copy. The multidomain protein kinases BUB1 (budding uninhibited by benzimidazole 1) and the above-described BUBR1 (in yeasts, worms, and plants, termed also Mad3-mitotic-arrest deficient) represent the central part of the control point in the mitotic spindle ready for assembly. This evolutionarily preserved and indispensable system of self-control in the eukaryotic cell cycle warrants a high quality of chromosomal segregation by delaying the manifestation of anaphase in all chromosomes that are incorrectly bioriented to mitotic spindles; it takes part in the inhibition of anaphase-promoting complex/cyclosome (Shichiri et al. 2002; Greene et al. 2008; Lee et al. 2009; Frio et al. 2010; Bolanos-Garcia and Blundell 2011; Nasir et al. 2011).
A number of authors have described a high activity of BUBR1, which may be linked to the progression of the epithelial form of ovarian tumors. Similar correlations were observed in other carcinomas of breast, stomach, urinary bladder, thyroid, kidneys, and large intestine (Nobuyuki et al. 2008; Lee et al. 2009; Frio et al. 2010). Reports have appeared indicating that overall BUBR1 localization, revealed by immunostaining, differs between normal and neoplastic tissues of urinary bladder, large intestine, pancreas, and skin. The authors have suggested that BUBR1 may have a role as a prognostic factor, permitting the detection of oncologic anomalies at their early phase of cell division (Lee et al. 2009; Bolanos-Garcia and Blundell 2011).
Reports are available that document BUBR1 expression in breast cancer (Du et al. 2011) but, until now, its prognostic value has not been evaluated. Thus, this study aimed at evaluating BUBR1 expression in a group of breast cancer patients.
Methods
Patients
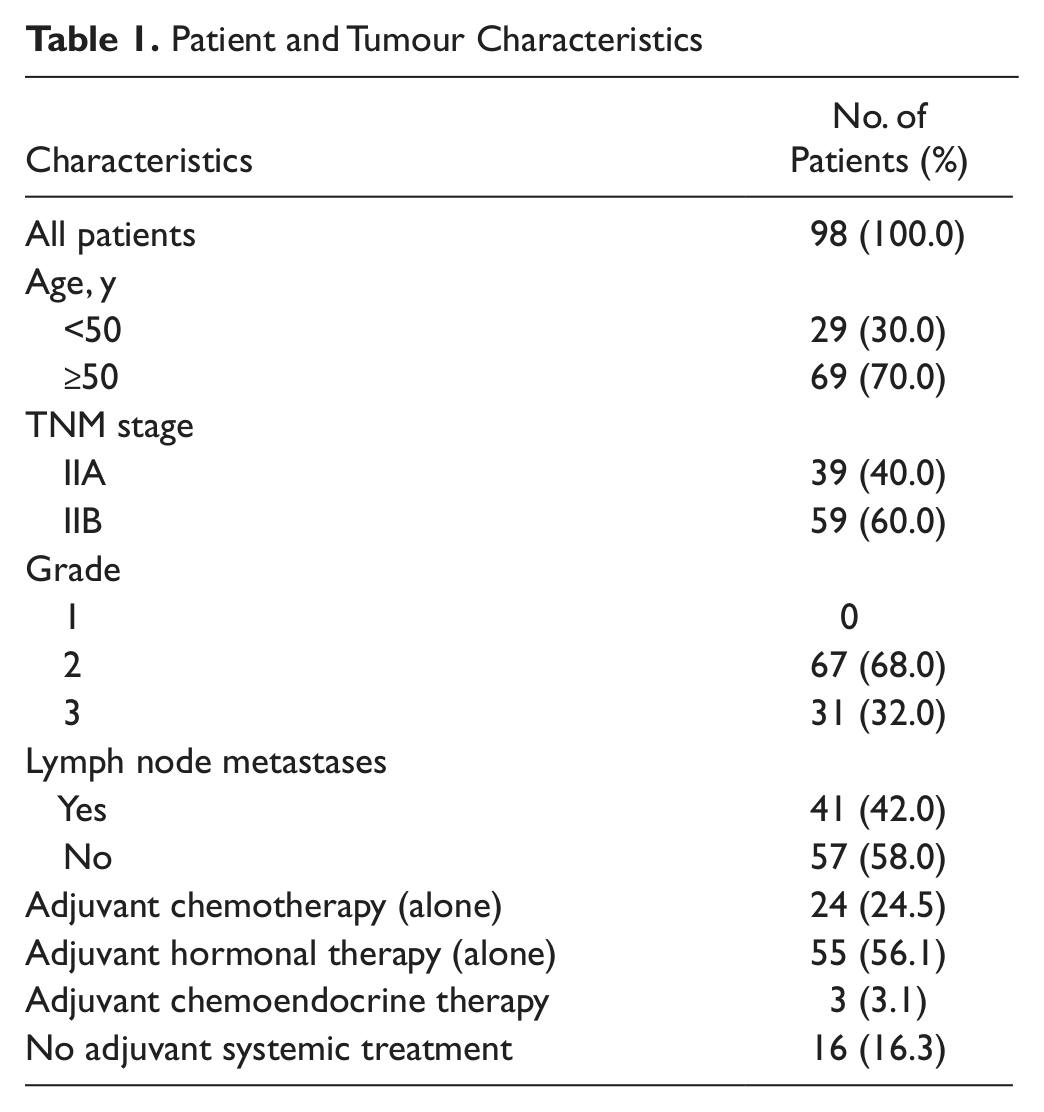
Material for the immunohistochemical (IHC) studies originated from 98 patients with breast cancer. All patients were diagnosed and treated at the Lower Silesia Oncology Centre in Wroclaw (Poland) between January 1993 and June 1994. Mean age of the patients was 56 years; the youngest was 29 years, and the eldest was 86 years. The diagnosed breast carcinoma was stage IIA in 39 patients and IIB stage in 59 patients, according to the TNM 1997 classification. Size of the tumor ranged between 1 and 7.5 cm, with a mean size of 3.2 cm. Metastases to lymph nodes were detected in 41 patients (Table 1). The study was approved by the Commission of Bioethics at the University Medical School in Wroclaw (Poland). The consent pertained to investigations funded by the Polish Ministry of Science and Higher Education under grant number 0638/B/P01/2008/35. Because the studies were carried out on archival material from 1993 to 1994, the Commission of Bioethics agreed to omit the procedures for obtaining informed consent of patients.
Patient and Tumour Characteristics
All patients were subjected to the modified radical mastectomy according to Madden (Madden 1965; Scanlon and Caprini 1975). Adjuvant treatment was applied in 82 patients, of whom 24 received chemotherapy alone, 55 received hormonal therapy alone, and 3 had chemotherapy followed by hormonal therapy. Chemotherapy was based on 6 cycles of CMF (cyclophosphamide, 5-fluorouracil, methotrexate). Hormonal therapy involved the administration of tamoxifen for 5 years. In a proportion of treated patients, postoperative radiotherapy was applied. The postoperative radiotherapy in the patients followed indications compatible with management standards in 1993–1994: irradiation was applied only in patients with a tumor diameter exceeding 3 cm and/or numerous metastases to the axillary lymph nodes. The way in which adjuvant radiotherapy and chemotherapy were combined with each other was not unequivocally specified. The grade was evaluated using the three-grade classification of Bloom and Richardson (1957), as modified by Elston and Ellis (1991). In the tumor specimens, exclusively ductal G2 or G3 carcinoma was demonstrated. Following the applied treatment, the patients were subjected to periodical control at the Lower Silesia Oncology Centre. The mean period of observation was 14.2 years (range, 9.1–16.5 years). Data related to relapse and death were accumulated using medical documentation available at the Lower Silesia Oncology Centre.
Immunohistochemistry
Formalin-fixed, paraffin-embedded tissue was freshly cut (4 µm). The sections were mounted on Superfrost Plus slides (Menzel Gläser; Göttingen, Germany), dewaxed in xylene, and gradually hydrated. Activity of endogenous peroxidase was blocked by 30-min exposure to 1% H2O2. All the studied sections were boiled for 20 min at 500 W in Antigen Retrieval Solution (DAKO; Glostrup, Denmark). Then, immunohistochemical reactions were conducted using monoclonal mouse anti-human BUBR1 antibody (Clone 9/BUBR1; BD Transduction Laboratories, San Diego, CA) diluted 1:300 in the Antibody Diluent, Background Reducing (DAKO) (Lee et al. 2009).
For detection of c-erbB-2 (HER2/neu) protein, the ready semiquantitative diagnostic immunocytochemical kit was used (HercepTest Kit, K5207; DAKO). For determination of hormone receptor expression, monoclonal mouse human estrogen receptor–specific (Clone 1D5, N1575; DAKO) and monoclonal mouse human progesterone receptor–specific (Clone PgR636, N1630; DAKO) antibodies were used. In each case, control reactions were included, in which the specific antibody was substituted by the Primary Mouse Negative Control (DAKO).
The specific antibodies were incubated with studied sections for 1 hr at room temperature. This was followed by incubations with biotinylated antibody (20 min at room temperature) and streptavidin-biotinylated peroxidase complex (20 min at room temperature) from the LSAB+ kit (DAKO). For visualization of the reaction, the DAB+ Liquid kit was used (DAKO) (7 min at room temperature). The sections were counterstained with Mayer’s hematoxylin for 30 sec.
Evaluation of Reaction Intensity
Intensity of immunohistochemical reactions was estimated independently by two pathologists. In doubtful cases, a reevaluation was performed using a double-headed microscope, and staining was discussed until a consensus was achieved. Intensity of BUBR1 expression was evaluated using the semi-quantitative immunoreactive score (IRS), which took into account the intensity of the color reaction and the percentage of positive cells (Remmele and Stegner 1987). The result, which represented the product of scores allocated for the evaluated traits, ranged between 0 and 12 (Table 2).
Evaluation Criteria of BUBR1 Expression Using Immunoreactive Score (IRS) Scale
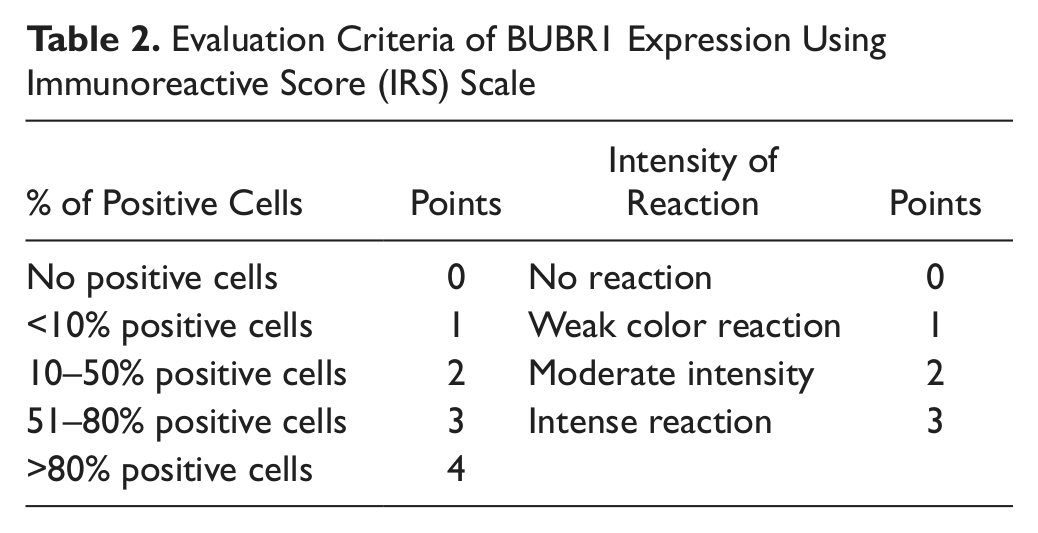
During subsequent statistical analyses, a two-grade scale system was applied, allocating 0 points for expression of BUBR1 ≤4 IRS and 1 for expression of BUBR1 ≥6 IRS.
An evaluation of estrogen and progesterone receptor expression was performed using standard methods. The staining intensity (0–3 scale) and proportion of positive cells (0–5 scale) were reported, and the Allred score (AS), which combines the two variables, was calculated. HER2 status was evaluated using the Food and Drug Administration–approved scoring system of 0, 1+, 2+, and 3+ (0 = no immunostaining; 1+ = weak immunostaining, less than 30% of tumor cells; 2+ = complete membranous staining, either uniform or weak in at least 10% of cells; 3+ = uniform intense membranous staining in at least 30% of cells).
Statistical Analysis
All statistical analyses were conducted using Statistica 9.0 PL software (Stanisz 2007). Disease-free survival (DFS) was defined as the time between the primary surgical treatment and date of relapse or death, whichever occurred first, and DFS was censored at the last follow-up for those who were alive without recurrence. Overall survival (OS) was defined as the time between the primary surgical treatment and death, and OS was censored at the last follow-up for those who were alive. Disease-specific survival (DSS) was defined as the time between the primary surgical treatment and death from cancer. Clinicopathological variables considered in the univariate analysis included age at the time of primary surgery, which was a surrogate for the date of diagnosis (continuous variable); lymph node status (pN positive vs pN negative); hormonal receptor (HR) status (by IHC; positive vs negative); HER2 expression; and grade of malignancy, according to the scale by Bloom and Richardson (1957). Correlations between these variables and BUBR1 status were analyzed using Spearman tests. To estimate survival, Kaplan-Meier (KM) statistics, log-rank tests, and Cox proportional hazard regression (Stanisz 2007) were used.
KM Plotter Online Survival Analysis
The KM plotter is capable of assessing the effect of 22,277 genes on survival in 2472 breast cancer patients (Györffy et al. 2010; http://kmplot.com/breast). A background database was established using gene expression data and survival information on 2422 patients downloaded from the Gene Expression Omnibus (GEO; Affymetrix [Santa Clara, CA] HGU133A and HGU133+2 microarrays). The median relapse-free survival was 6.43 years. After quality control and normalization, only probes present on both Affymetrix platforms were retained (n=22,277). The background database was handled by a MySQL server, which integrates gene expression and clinical data simultaneously. To analyze the prognostic value of a particular gene, the samples were split into two groups according to the median (or upper/lower quartile) expression of the gene. The two groups could be compared in terms of relapse-free survival, overall survival, and distant metastasis–free survival.
Results
Immunostaining
The performed immunohistochemical reactions with BUBR1-specific antibodies documented a cytoplasmic localization of the protein in breast cancer cells, with variable intensity in individual cases (Fig. 1).
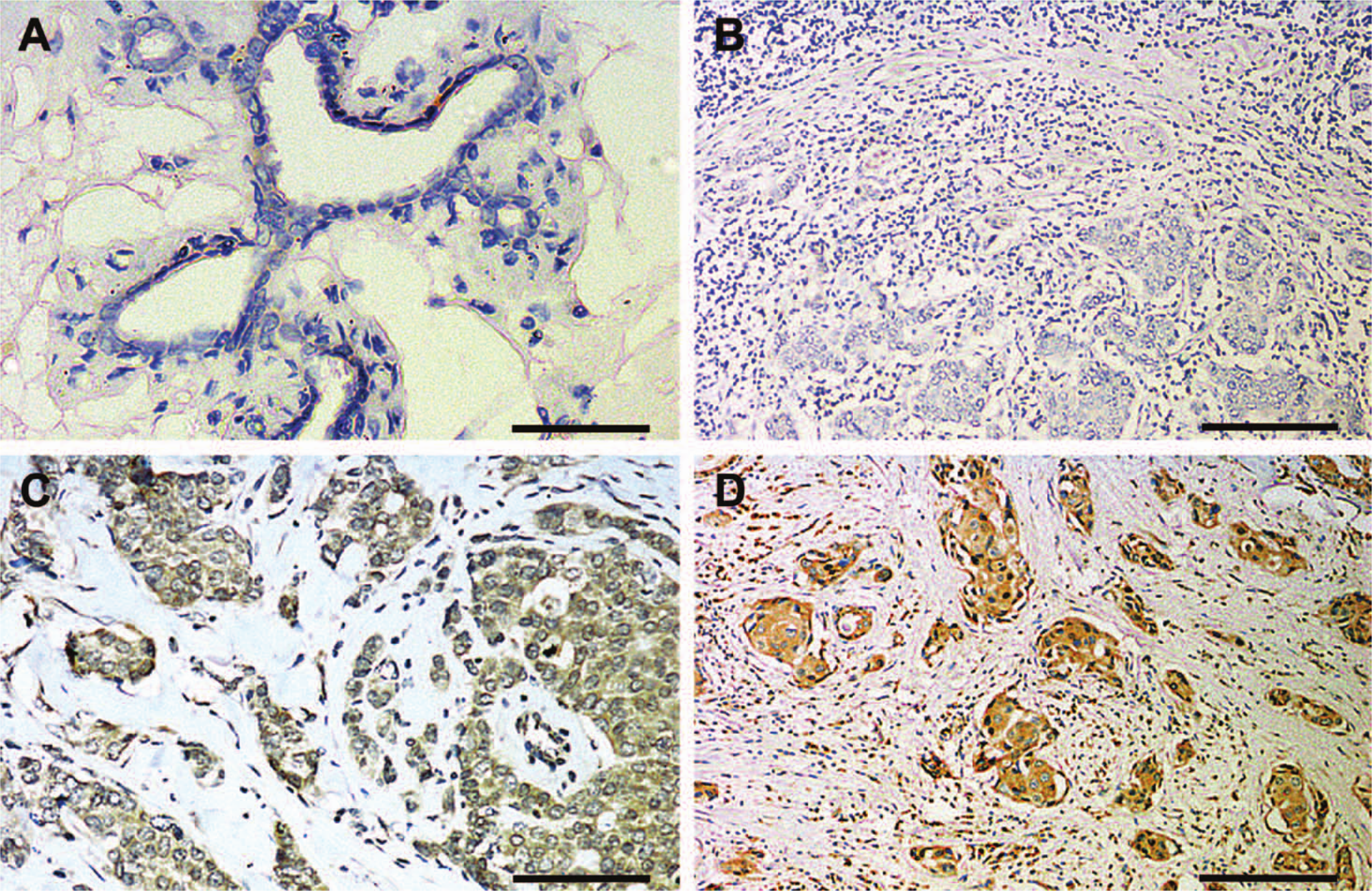
Immunohistochemical analysis of the BUBR1 (budding uninhibited by benzimidazole-related 1) expression: (A) in the healthy epithelium, only single cells show a weak reaction (hematoxylin); (B) no reaction in the cancer cells (immunoreactive score [IRS] = 0; hematoxylin); (C) weak reaction in the cancer cells (IRS = 4; hematoxylin); (D) strong reaction in the cancer cells (IRS = 12; hematoxylin). Bars: A = 50 µm; B, D = 200 µm; and C = 100 µm.
Of the 98 evaluated preparations, no color reaction was detected in 21 cases (21.5%), the reaction was evaluated as 1 according to the IRS in 12 cases (34%), and it was evaluated at 2, 3, 4, 6, 8, 9, and 12, respectively, in 19 (19%), 4 (4%), 7 (7%), 10 (10%), 11 (11%), and 4 (4%) cases (Table 3). For the purpose of subsequent analysis of survival, we divided the patients into two groups of high (≥6) and low (≤4) expression of BUBR1 protein according to the IRS scale.
Results of Univariate Analysis for 15 Years of DFS, DSS, and OS
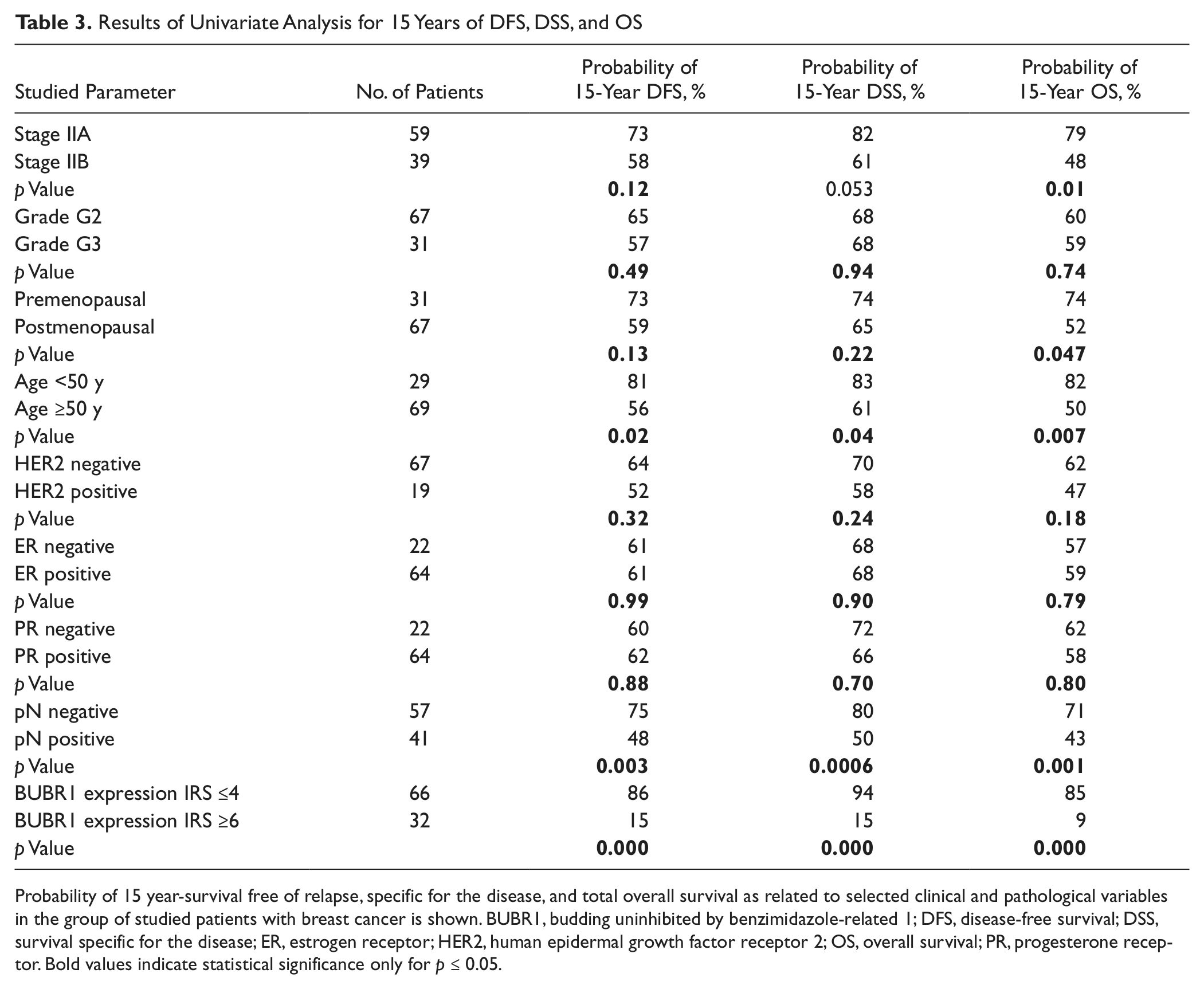
Probability of 15 year-survival free of relapse, specific for the disease, and total overall survival as related to selected clinical and pathological variables in the group of studied patients with breast cancer is shown. BUBR1, budding uninhibited by benzimidazole-related 1; DFS, disease-free survival; DSS, survival specific for the disease; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; OS, overall survival; PR, progesterone receptor. Bold values indicate statistical significance only for p ≤ 0.05.
BUBR1 Expression and Clinicopathological Data
Of the examined clinicopathological variables, the expression of BUBR1 protein in cancer cells was related exclusively to the presence of metastases to lymph nodes (N+) (p=0.0068, r = 0.27; Table 4).
Relationships Between the Analyzed Clinicopathological Parameters
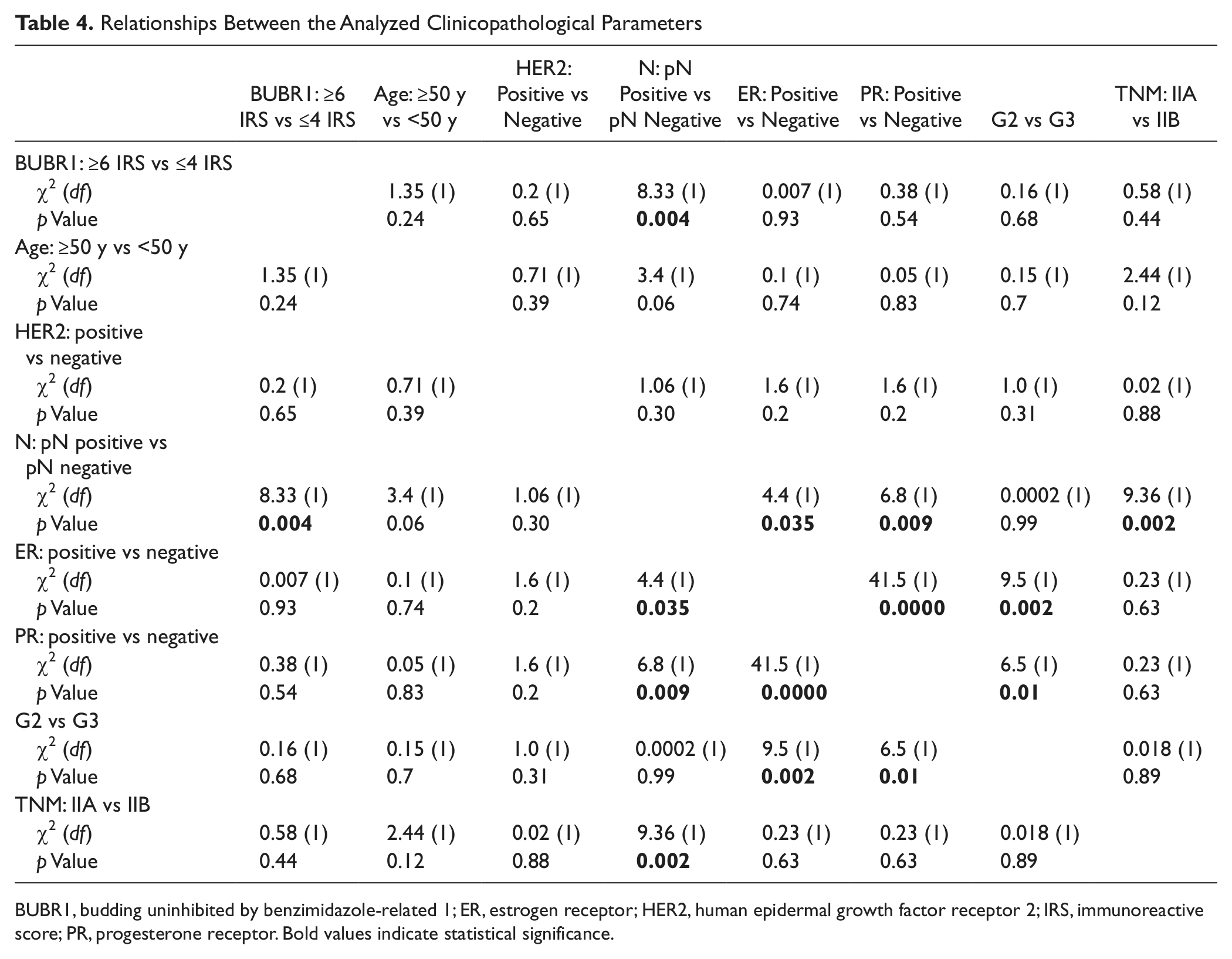
BUBR1, budding uninhibited by benzimidazole-related 1; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; IRS, immunoreactive score; PR, progesterone receptor. Bold values indicate statistical significance.
Moreover, the presence of lymph node metastases was related to the expressions of estrogen receptor (p=0.00054, r= 0.36), progesterone receptor (p=0.0165, r= 0.25), and stage of disease (TNM).
In addition, the studied group manifested a strong relationship between the expressions of progesterone receptor (p=0.0036, r= −0.31) and estrogen receptor (p=0.00012, r= −0.4) in cancer cells and G grade of tumor malignancy.
BUBR1 Expression and Survival Data
In the course of the observations, 37 (38%) patients died, including 8 with no indications of cancer progression. Sixty-one (62%) patients remained viable, including 5 patients with a documented relapse. In three of these patients, locoregional relapse in the scar was noted, which appeared in one of the patients 6 months after the operation, after 9 years in the second patient, and after 13 years in the third patient. Moreover, two patients remained viable with a documented metastasis to the lungs. In one patient, the spread to the lungs was detected after 7 years. Since that time, the patient has remained viable for over 6 years. In the other patient, pulmonary metastases manifested after 14 years, and since that time, the patient has remained viable for over 1 year.
Univariate analysis documented significant relationships between overall survival (OS) and IIB grade of advancement, menopausal status of the patients, age older than 50 years, presence of metastases to lymph nodes (N+), and high expression of BUBR1 (≥6 according to the IRS) in cancer cells (Table 3, Fig. 2A–C).
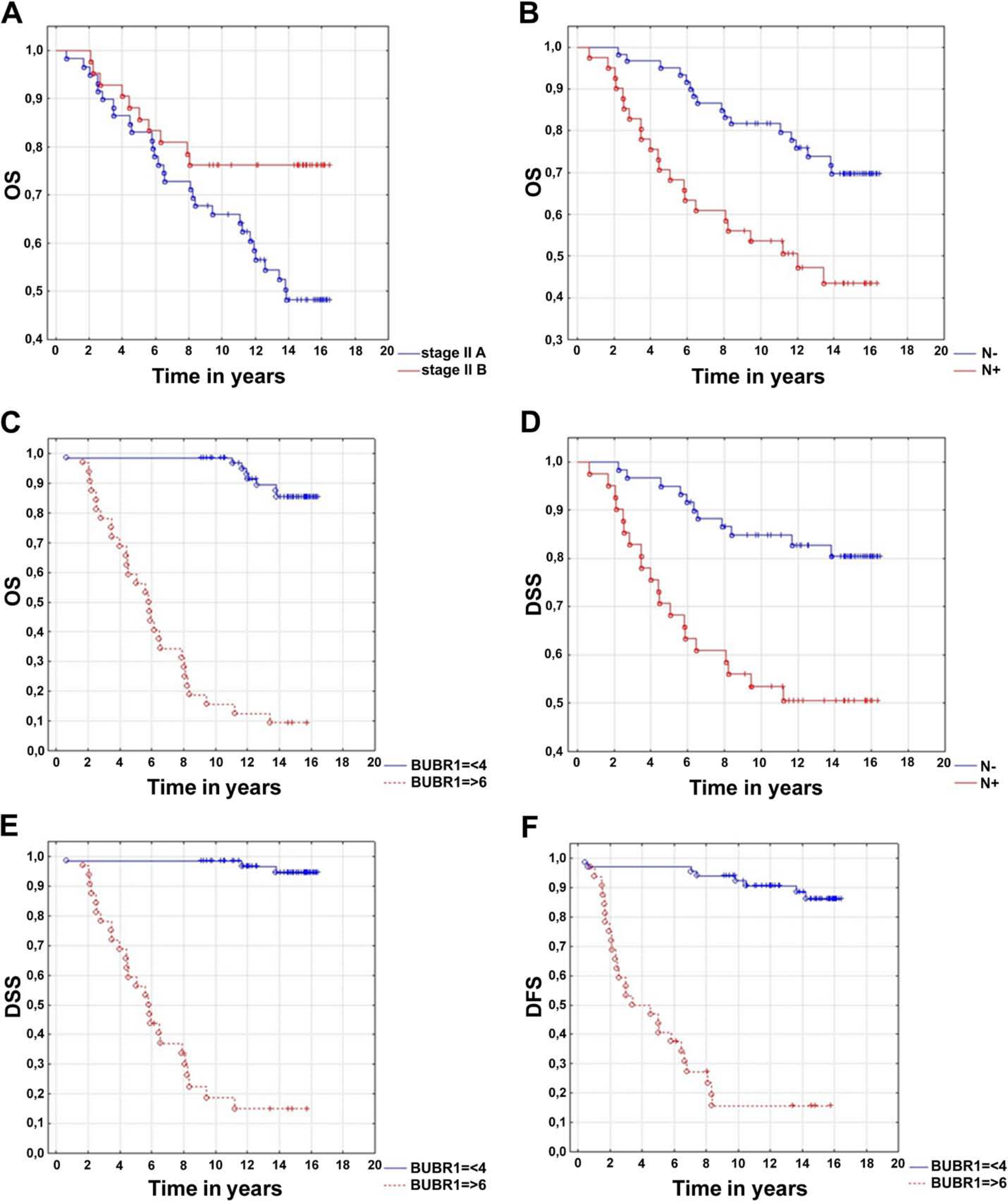
(A) Kaplan-Meier curves for overall survival (OS) and stage of disease in the studied group of breast cancer patients (p=0.01). (B) Kaplan-Meier curves for OS and stage of lymph nodes in the studied group of breast cancer patients (p=0.001). (C) Kaplan-Meier curves for OS and expression of BUBR1 in the studied group of breast cancer patients (p<0.0000). (D) Kaplan-Meier curves for disease-specific survival (DSS) and stage of lymph nodes in the studied group of breast cancer patients (p=0.0006). (E) Kaplan-Meier curves for DSS and expression of BUBR1 in the studied group of breast cancer patients (p<0.0000). (F) Kaplan-Meier curves for disease-free survival (DFS) and expression of BUBR1 in the studied group of breast cancer patients (p<0.0000).
On the other hand, less favorable DSS and DFS rates were demonstrated by patients older than 50 years, with the presence of metastases to the lymph nodes (N+) and with a high expression of BUBR1 (≥6) in the cell nuclei (Table 3; Fig. 2D, E).
In the multivariate analysis, the effect on DFS was manifested exclusively by a high level of BUBR1 expression. In the case of DSS, independent prognostic factors were found to include a high level of BUBR1 expression and an overexpression of HER2. In the case of OS, independent prognostic factors were found to include a high level of BUBR1 expression, overexpression of HER2, and clinical stage of disease (TNM stage) (Table 5, Fig. 2F).
Results of Multivariate Cox Analysis for DFS, DSS, and OS
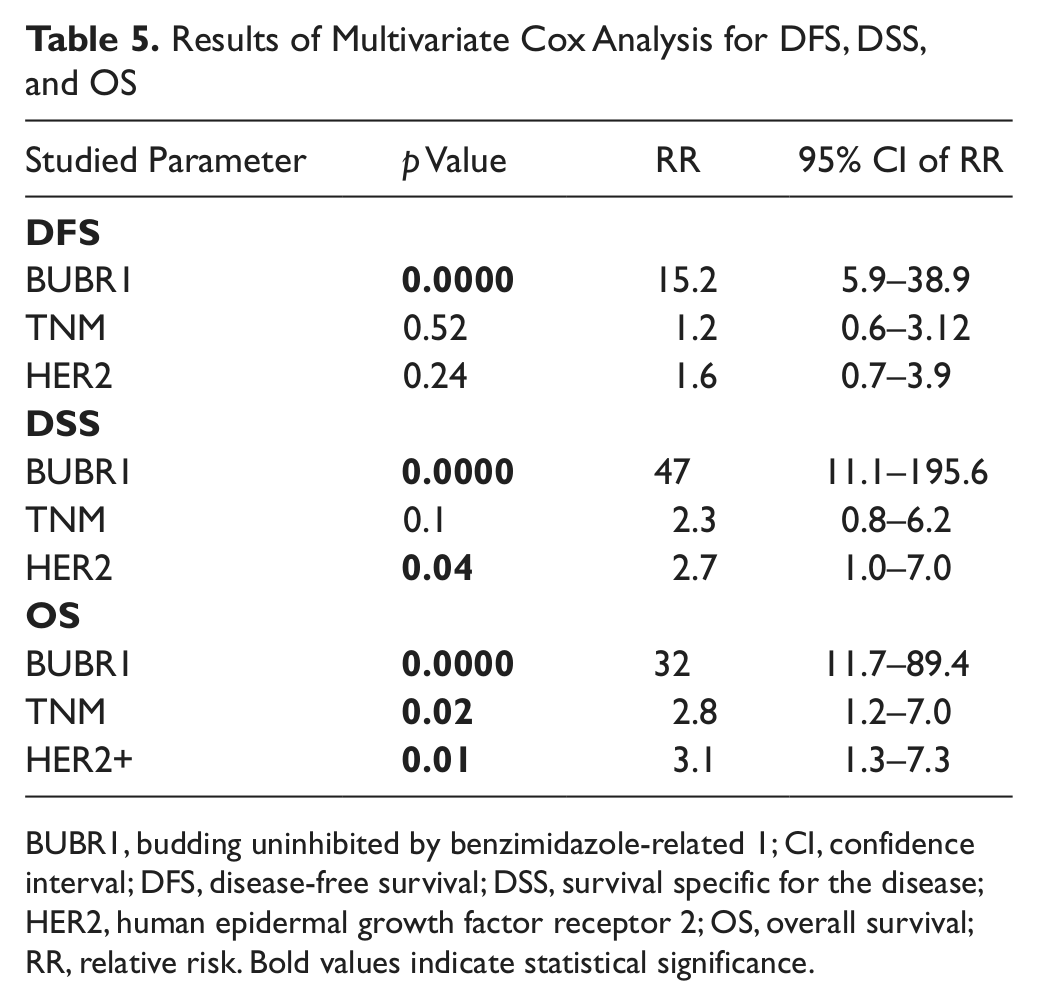
BUBR1, budding uninhibited by benzimidazole-related 1; CI, confidence interval; DFS, disease-free survival; DSS, survival specific for the disease; HER2, human epidermal growth factor receptor 2; OS, overall survival; RR, relative risk. Bold values indicate statistical significance.
KM Plotter Online Survival Analysis
In the KM plotter online survival analysis of the prognostic value manifested by BUBR1 mRNA (Affy id.: 206155_at), an elevated BUBR1 mRNA expression was found to exert a negative impact on the patients’ relapse-free, distant metastases–free, and overall survival. An increased expression of BUBR1 was found to carry an unfavorable prognostic value, independent of presence, in patients with regional lymph node metastases (Table 6) (Györffy et al. 2010; http://kmplot.com/breast).
Kaplan-Meier Plotter Analysis of Prognostic Significance of the BUBR1 mRNA Expression
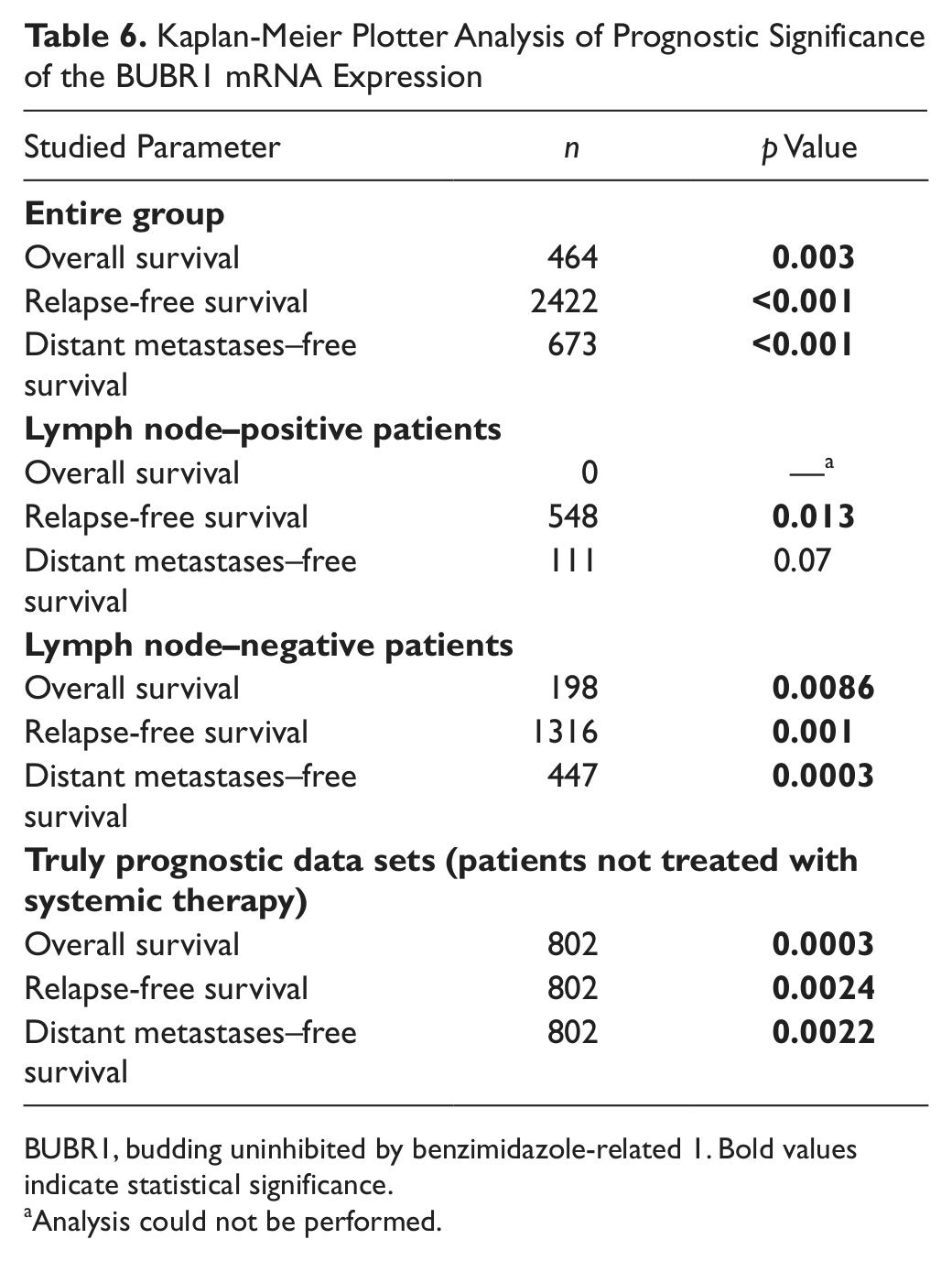
BUBR1, budding uninhibited by benzimidazole-related 1. Bold values indicate statistical significance.
Analysis could not be performed.
Discussion
The elevated level of BUBR1 is not thought to initiate tumor development, and mutations of tumor suppressor genes, such as BRCA1and BRCA2, are present long before there is any increase in the activity of BUBR1 (Lee et al. 2009). However, an accelerated proliferation rate makes the cells susceptible to a high mutation rate, accompanied by an accumulation of the mutations, which frequently leads to cell death. Nevertheless, a proportion of these abnormal cells survive, and the anomalies that they present also stimulate and intensify the neoplastic process. Just these surviving cells manifest higher levels of BUBR1, linked mainly to the high frequency of enforced, abnormal proliferation. In parallel, the cells manifest genetic instability, mainly due to accumulated mutations (e.g., aneuploidy). Aneuploidy, or the loss of a chromosome in cellular progeny, develops during mitosis due to erroneous aggregation of sister chromatids. Aneuploidy represents a common trait in several types of neoplastic cells; it is frequently linked to other mutations, primarily, deletions and insertions. Nevertheless, it still remains to be clarified if the acquired aneuploidy represents a specific accelerator of the progression of human tumors and, if so, how aneuploidy promotes cancer progression (Weaver and Cleveland 2007).
In a proportion of reports, however, authors have drawn readers’ attention to the fact that chromosomal instability and, as an effect, development of a tumor may be linked in some way to the modification of the activity manifested by the kinases operating at the mitotic spindle checkpoint. These authors have described the role of BUB1 in carcinogenesis, pointing to the linkage between the manifestation of BUB1 gene mutations and the expression of the protein in neoplastic tissues and in cell lines on one hand, and the development of spontaneous tumors on the other, in mice characterized by the presence of hypomorphic alleles. In the case of BUBR1, deletions and missense mutations were seen in families with mosaic-variegated aneuploidy, with the syndrome characterized by microcephaly and mental retardation. The biallelic mutations provided new indications related to the potential for developing cancer, pointing to the chance for manifestation of germinal mutations also in the gene of the mitotic spindle checkpoint (Logarinho and Bousbaa 2008; Privette et al. 2008; Chinthalapally et al. 2009; Bolanos-Garcia and Blundell 2011).
A particularly evident relationship was documented between the activity of BUBR1 and the risk of developing breast cancer. Studies by Nasir et al. (2011) confirmed the overexpression of the BUBR1 protein within a histologically normal-looking tissue of the mammary gland. Subsequently, the neoplastic process was verified using microarrays and real-time PCR studies. The result of Nasir et al. suggested that detection of BUBR1 overexpression might provide a new immunohistochemical biomarker for breast cancer; this marker offers particular sensitivity, as it was detectable already at the early stage of neoplasia when the histological pattern of the gland was still unaltered (Nasir et al. 2011). Du et al. (2011), in turn, described in patients with breast cancer a relationship between BUBR1 overexpression and known clinicopathological parameters, on one hand, and the expressions of estrogen receptor, progesterone receptor, Ki-67, and HER2 on the other (Du et al. 2011). Both in univariate and multivariate data analyses, Du et al. demonstrated that positive BUBR1 expression was associated with a high Ki-67 labeling index. In the univariate analysis, but not in the multivariate analysis, positive BUBR1 expression was also associated with a high histological tumor grade. Although the studies documented BUBR1 expression in breast cancer, they did not examine the prognostic value of BUBR1 overexpression.
Also in our study, we have observed a pronounced correlation between the high activity of BUBR1 and an unfavorable course of the disease: the unfavorable effect of overexpression was highly significant both for the local control of the neoplastic process and for the distant survival of the patients. It seems important to stress that our study has for the first time documented the unfavorable prognostic significance of BUBR1 overexpression in patients with breast cancer. The value of the results is accentuated by the long period of monitoring of the patients (mean duration: 14 years) and the relatively homogeneous group of patients with respect to their grade of advancement. Prognostic power of the index evidently exceeded the power of other classical prognostic factors, even the prognostic value of metastases to lymph nodes. Such a strict relationship between the overexpression of BUBR1 and the unfavorable results of the conducted treatment should be related, first of all, to the highly selective functionality of the kinase. Also, other results encountered in the database and involving results on RNA microarrays related to activities of various potential prognostic markers point to BUBR1 as one of the most active factors (Györffy et al. 2010).
It should be noted that functional BUBR1 is of key importance for dividing cells but not for resting cells. Thus, no activity of BUBR1 should be noted in non-dividing cells. Therefore, the augmented activity of BUBR1 also correlates mainly for patients with poor prognosis for patients with an aggressive form of the tumor. Its the high expression reflects the high proliferative ability of neoplastic cells, as proven also by the fact that elevated levels of BUBR1 coincide with high mitotic indices (Lee et al. 2009).
An interesting aspect of studies conducted on neoplastic cells that manifest aneuploidy involves taking therapeutic advantage of the anomaly in the course of cell division. It seems interesting to examine the role of BUBR1 as a potential therapeutic target of drugs belonging to microtubule inhibitors. This might open a new investigative pathway aimed at confirming the predictive value of the BUBR1 protein. Shifting the therapeutic target to the point of controlling of the division spindle might provide an interesting approach to cancer treatment. However, it should be kept in mind that accelerated proliferation is typical of not only neoplastic cells, and the key problem will be posed by sensitivity of hematopoietic cells to the suggested therapy. In this respect, it would seem interesting to evaluate the role of BUBR1 protein activity not only as a prognostic but also as a predictive biomarker to select a group of patients sensitive to the action of antineoplastic drugs, in whom anomalies were detected in the process of division in the karyokinetic spindle.
Conclusion
Elevated expression of the mitotic kinase, BUBR1, is associated with poor survival in early breast cancer patients. Modulating BUBR1 activity may be a promising future approach to tailored therapy of breast cancers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the grant No. 0638/B/P01/2008/35 from the Ministry of Science and Higher Education (Poland).