
Abstract
An 11-yr-old Dressage mare had abnormal gait, and an abscess of the left hoof was suspected but not observed. Radiographic and computerized tomographic evaluations showed a large cystic lesion near the apex of the pedal bone, and a smaller, similar lesion at the lateral wing. Sagittal sections through the affected member revealed two intraosseous cysts at the third phalanx. Histologic and histochemical results characterized the lesions as intraosseous epidermoid cysts of the third phalanx.
Keywords
Clinical History
During the summer of 2007, an 11-year-old, warm-blooded Dressage mare had unbalanced gait and suddenly became lame on the left hind limb; a hoof abscess was suspected but none was detected. Initial clinical examination (H. Saarinen) and radiographic evaluations revealed a large cystic lesion near the apex of the pedal bone, and a smaller, similar lesion at the lateral wing. Treatment with metronidazole for 2 weeks and the utilization of bar shoes alleviated the problem temporarily. At the end of March 2008, a second evaluation (A. Tupamäki) by lameness examination revealed abnormal gait of the left hind limb, worsened lameness during the left circle, and a positive flexion test of the distal limb. At this time, differential diagnoses included a tumor (such as osteosarcoma) of the pedal bone or a bone cyst. Due to the progressive nature of the lesions, a guarded prognosis was given, and the horse was humanely euthanized at the University Animal Hospital, University of Helsinki, Finland, after which the distal part of the left hind limb was submitted for radiographic and computerized tomographic (CT) evaluations.
After imaging, the excised limb and the animal were submitted to the Section of Veterinary Pathology for routine necropsy. Sagittal sections were made through the distal extremity of the left hind limb. Tissue sections from the affected area were decalcified and routinely processed for histopathologic evaluation (Hematoxylin and Eosin; HE), and selected sections were stained with Masson's trichrome.
Radiographic and CT Observations
The radiographic and CT images of the left hind pedal bone revealed a large cystic lesion close to the apex that had a sclerotic external lining and was filled with a radio-dense homogeneous mass. The dorsal wall of this cyst was very thin and expanded against the dorsal cortical bone. In addition, there was a smaller cystic lesion at the plantar side of the lateral wing of the pedal bone (Figs. 1, 2).
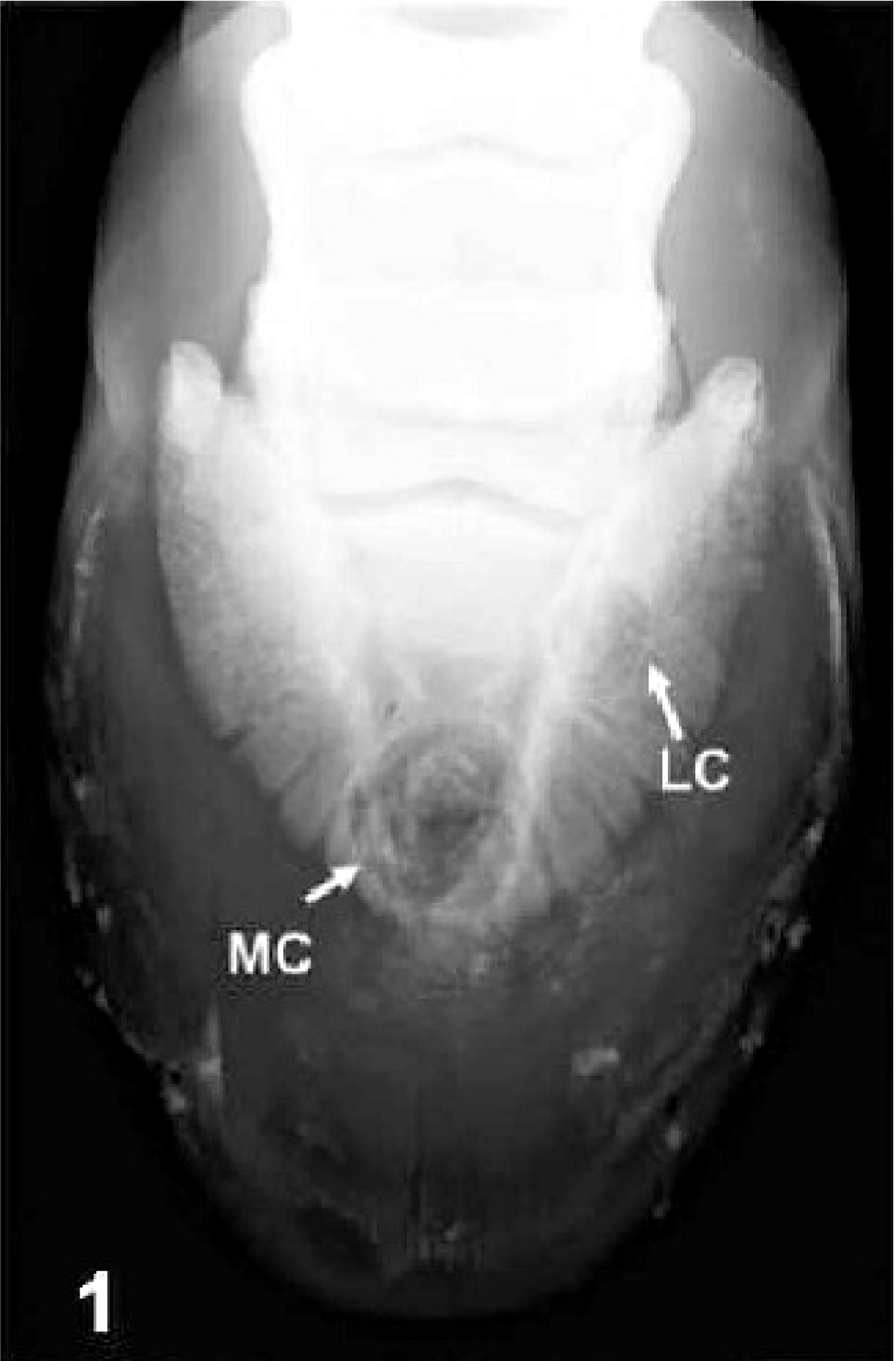
Radiographic image, frontal view. Third phalanx; horse. There are 2 radio-dense homogenous cystic masses located at the medial (MC) and lateral (LC) areas of the pedal bone.
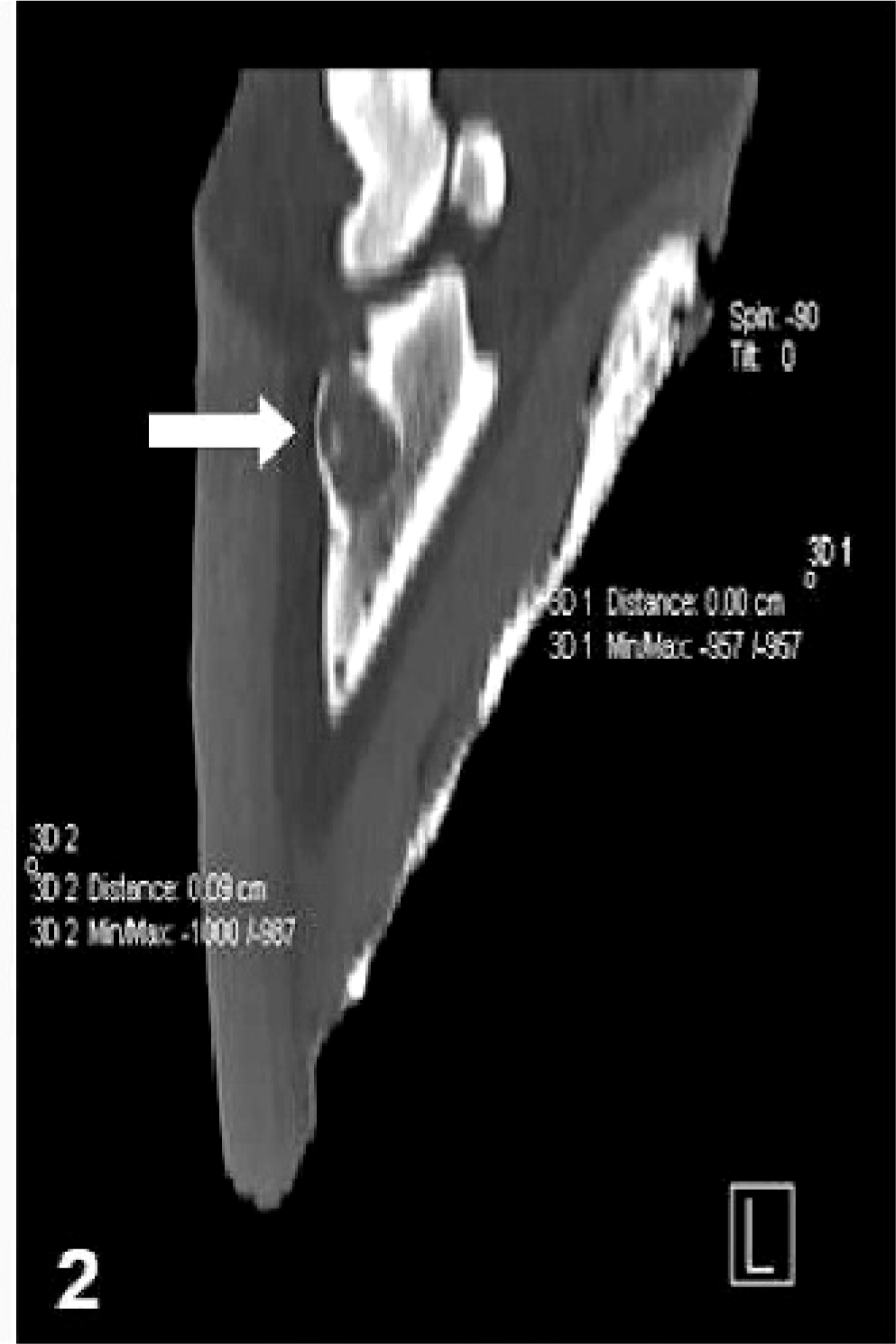
CT image, lateral view. Third phalanx; horse. There is a radiolucent homogenous cystic structure (arrow) at the dorsal aspect of the pedal bone.
Gross findings
Significant gross findings were restricted to the distal extremity of the left hind member; all other tissues and organs were normal. A sagittal section through the limb revealed a centrally located 1.8 × 2.5 cm cystic area at the third phalanx behind and below the hoof wall (Fig. 3); and a similar area (0.5 × 1.2 cm) at the lateral border of the third phalanx. These space-occupying lesions contained a cream-colored, tightly compacted, odorless and nonsuppurative material that was partially surrounded by concentric laminated formations (Fig. 4).
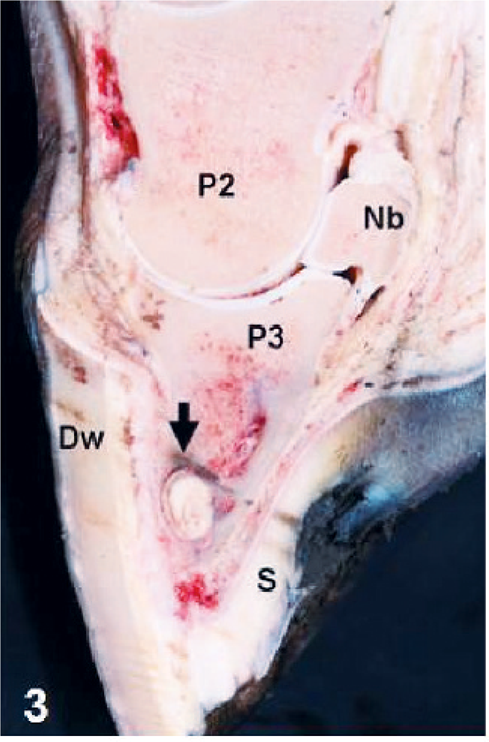
Sagittal section. Distal extremity of hind leg; horse. There is a compact intraosseous cyst (arrow) at the distal extremity of the third phalanx (P3). Nb = navicular bone; S = sole; P2 = second phalanx; P3 = third phalanx; DW = dorsal wall.
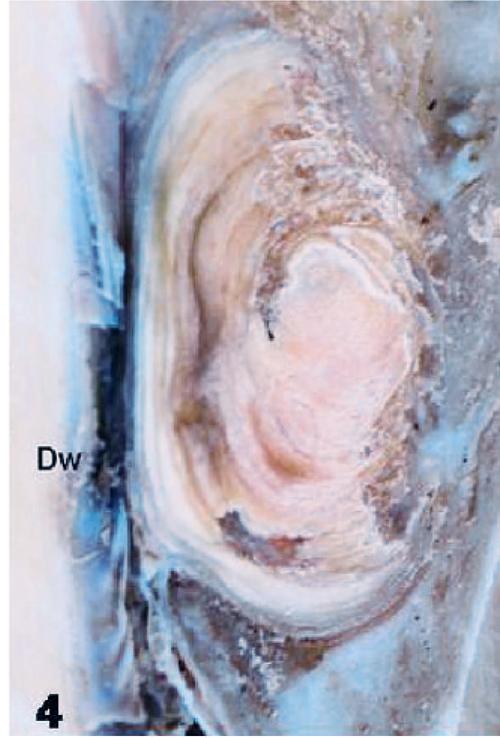
Formalin-fixed specimen. Third phalanx; horse. Closer view of medially located cyst with several laminated formations close to the dorsal wall (DW).
Differential diagnoses
The most important differentials for the lesion in this case are intraosseous epidermoid cyst and equine keratoma 2 ; and might possibly include benign bone tumors. Epidermoid cyst and the equine keratoma are nontumorous lesions, but keratomas are abnormal masses of keratin produced by the epidermal cells of the coronary band 4 and are not intraosseous lesions. Keratomas contain accumulations of keratin cells and granulation tissue, 4, 5 with an associated purulent inflammatory reaction. 5 However, differential diagnosis becomes difficult in unusual cases of keratomas where there is not an associated inflammation or granulation tissue. 3 In these cases, the anatomic location of the lesion (intraosseous or not) might be the best way to characterize the alteration.
Microscopic findings
The cavitating lesion was not totally demarcated and consisted of an external layer of stratified squamous epithelium that lined a centrally located cystic structure. The center of the cyst had ghost-like remnants of keratinized epithelial cells. Adjacent to the central region were layers of keratinized squames arranged in ill-defined patterns, being predominantly concentric or in a herringbone-like formation (Fig. 5). A layer of fibrous connective tissue demarcated this structure externally and separated the lesion from the adjacent bone (Fig. 6). Inflammatory or proliferative reactions were not observed within or adjacent to the lesion. Histochemical evaluation with Masson's trichrome stain (not shown) highlighted the presence of fibrous connective tissue between the squamous epithelium that lined the keratinized squames and adjacent pedal bone. Based on the findings, a diagnosis of intraosseous epidermoid cysts of the distal phalanx was made.
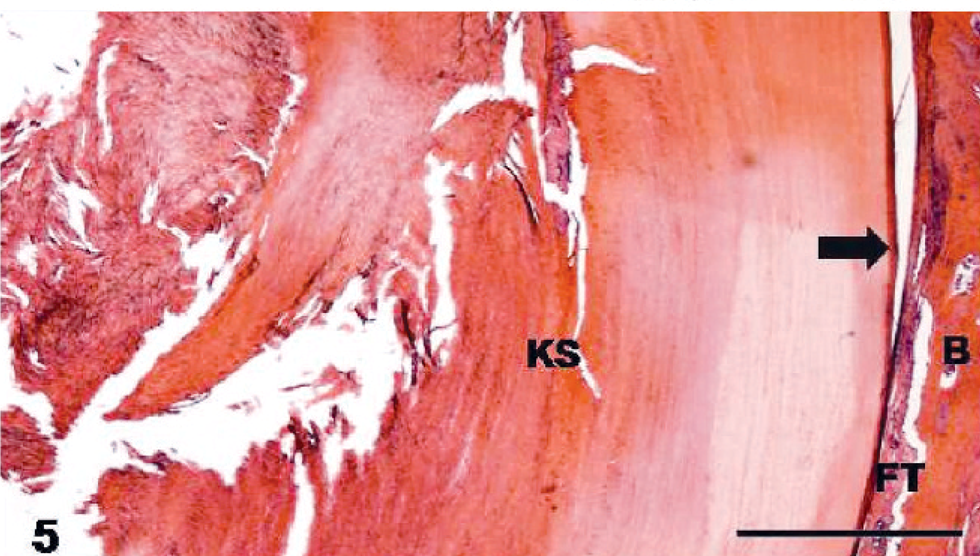
Intraosseous epidermoid cyst, third phalanx; horse. There is a centrally located accumulation of keratin squames (KS) that is surrounded by a layer of squamous epithelium (arrow) within the pedal bone (B), and fibrous tissue (FT) between the bone and epithelial layer. HE. Bar = 1 mm.
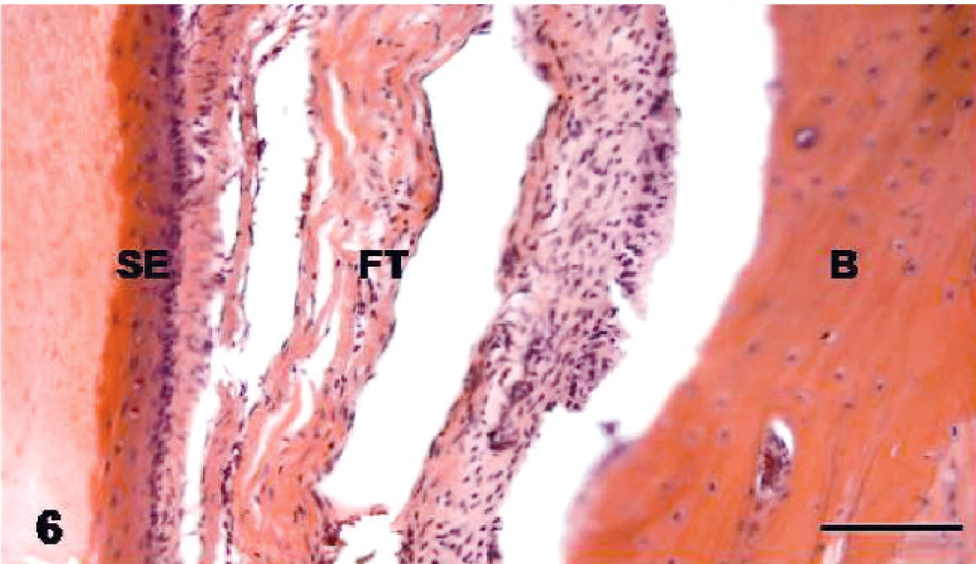
Intraosseous epidermoid cyst, third phalanx; horse. The wall of the cyst consists of a thickened layer of squamous epithelium (SE) that is separated from the pedal bone (B) by accumulation of fibrous tissue (FT). HE. Bar = 100 µm.
Discussion
Intraosseous epidermoid cysts are rare pseudoneoplastic lesions formed by the proliferation of epidermal cells within osseous tissue 6 and are characterized histologically by the accumulation of laminated keratin demarcated by an external layer of squamous epithelium. 8 The pathogenesis of this lesion is obscure but has been related to posttraumatic implantation of epidermal fragments in domestic animals. 8 In human medicine, there are 2 additional theories, embryonal misplacement of epithelial cells or erosion of soft epidermal tissue into bone. 6 This mare had no prior history of injury/surgery to the hoof, but limping began 6 months earlier. Therefore, embryonal misplacement might have been responsible for the development of this lesion.
A diagnosis of intraosseous epidermoid cysts of the distal phalanx was made owing to typical morphologic features and the anatomic location of the lesion, which are consistent for this nonneoplastic growth. 8 A similar case was described in the distal phalanx of a gelding 2 ; in that report only 1 cyst was observed: this mare had 2 cysts within the same phalanx. Other previously described localizations of this lesion in horses include the mandible 1 and the deep digital flexor tendon. 7 In addition, cases of intraosseous epidermal cysts were reported in dogs, 8 but not in other domestic animals as of the time of writing.
Although clinical, radiographic, ultrasonographic, or other imaging-based interpretation of this lesion might offer a diagnostic challenge, 2 the macroscopic features of intraosseous epidermoid cysts in the phalanx of horses are unique. Grossly, the finding of odorless, nonsuppurative, cream-colored, compacted, laminated-to-concentric, cyst-like intraosseous structures observed by sagittal sections through the affected phalanx of horses, as occurred in this and another similar case, 2 is characteristic for intraosseous epidermoid cysts; histopathology then confirms the diagnosis. 8 However, magnetic resonance imaging was considered of significant importance to characterize this lesion in a horse 7 and is an alternative for an efficient clinical diagnosis.