
Abstract
Invasive Klebsiella pneumoniae is an emerging disease of humans characterized by abscesses in the liver or other sites involving bacteria with the unique hypermucoviscosity phenotype. Over several months, 7 African green monkeys in our research colony developed abscess formation in multiple locations and succumbed to disease. K. pneumoniae was identified by bacterial culture in 6 monkeys and immunohistochemistry in 1 additional monkey. All monkeys had been housed in, or had contact with monkeys housed in, 1 animal room in our facility. All affected monkeys had 1 or more abscesses, most notably in the abdomen, but also affecting the lungs, cerebellum, and skin. Abdominal abscesses and associated adhesions entrapped loops of bowel, forming palpable masses. Abdominal masses were located at the root of the mesentery, the ileocecocolic junction, or the pelvic inlet. In 1 case, culture, serotyping, and polymerase chain reaction (PCR) analysis of the bacterial isolate identified K. pneumoniae expressing the hypermucoviscosity phenotype and capsular serotype K2 and determined that the K. pneumonia was genetically rmpA+/magA-.
Klebsiella pneumoniae is a gram-negative, aerobic, nonmotile bacillus and is a common cause of a wide range of infections in humans and animals. 8, 12 In Old and New World monkeys, infection with K. pneumoniae causes pneumonia, meningitis, peritonitis, cystitis, and septicemia. 7, 14 K. pneumoniae also constitutes normal fecal and oral flora in many nonhuman primates. In the past 2 decades, a new type of invasive K. pneumoniae disease has emerged in humans in Taiwan and other Asian countries, and more recently from non-Asian countries, including the USA. 2, 10, 11, 13, 17 Fatal human infections with invasive strains of K. pneumoniae involve pulmonary emboli or abscess, meningitis, endophthalmitis, osteomyelitis, or brain abscess. 3, 10 Recently, a highly invasive K. pneumoniae causing primary liver abscesses in humans has also been reported. 2, 10, 17 These invasive, abscess-forming strains of K. pneumoniae are associated with the so-called hypermucoviscosity (HMV) phenotype, a bacterial colony trait identified by a positive string test. 5, 6, 9 The HMV phenotype is seen in K. pneumoniae expressing either the capsular serotypes K1 or K2. K1 serotypes of K. pneumoniae have 2 potentially important genes, rmpA, a transcriptional activator of colanic acid biosynthesis, 16 and magA, which encodes a 43-kD outer membrane protein. 5 K2 serotypes of K. pneumoniae also have rmpA but do not have magA. Capsular serotypes K1 and K2 are reported to play an important role in the invasive ability of HMV K. pneumoniae. 18 The role of rmpA and magA in the pathogenesis of invasive K. pneumonia, however, seems less certain.
To our knowledge, K. pneumoniae expressing the HMV phenotype has not been reported to cause natural disease in nonhuman primates, nor in other animal species. In this report, we describe the clinical, gross and histopathologic features, and the bacteriologic findings of a single African green monkey (Chlorocebus aethiops—Africa green monkey [AGM]) with invasive K. pneumoniae infection, in which the bacterial isolate expressed the HMV phenotype and 6 additional AGMs in which Klebsiella was identified by bacterial culture or by immunohistochemistry. All monkeys described in this report were maintained in a facility at the US Army Medical Research Institute of Infectious Diseases accredited by the American Association for Accreditation of Laboratory Animal Care. All research was conducted under approved animal protocols in adherence with the Guide for the Care and Use of Laboratory Animals (Committee on Care and Use of Laboratory Animals of the Institute of Laboratory Animal Resources, National Research Council, National Institutes of Health Publication No. 86–23, revised 1996).
During a routine physical examination, an adult male AGM, V513, presented with an 8- to 10-cm-diameter mass on the right dorsal flank. No other abnormal findings were observed at the time, and the animal had no history of illness or injury before being transferred to our facility in 2003. One day after the initial presentation, the fluid-filled mass ruptured and was draining a thick, mucoid discharge. The abscess was cultured, surgically debrided and lavaged, a Penrose drain was placed, and antibiotic treatment was initiated. An abdominal mass was palpated 24 hours following surgery and was described as a 3 cm × 1 cm irregularly shaped, firm mass in the cranial abdomen. The mass enlarged over several days, and exploratory laparotomy revealed mesenteric abscesses centered at the ileocecocolic junction and also involving the duodenum, ileum, cecum, colon, the right ureter, and the body wall inferior to the right kidney. Surgical removal was not possible, and the animal was euthanatized. A complete necropsy was performed, samples were taken for bacterial culture, and a full set of tissues was fixed in 10% neutral buffered formalin and processed routinely for histopathologic evaluation.
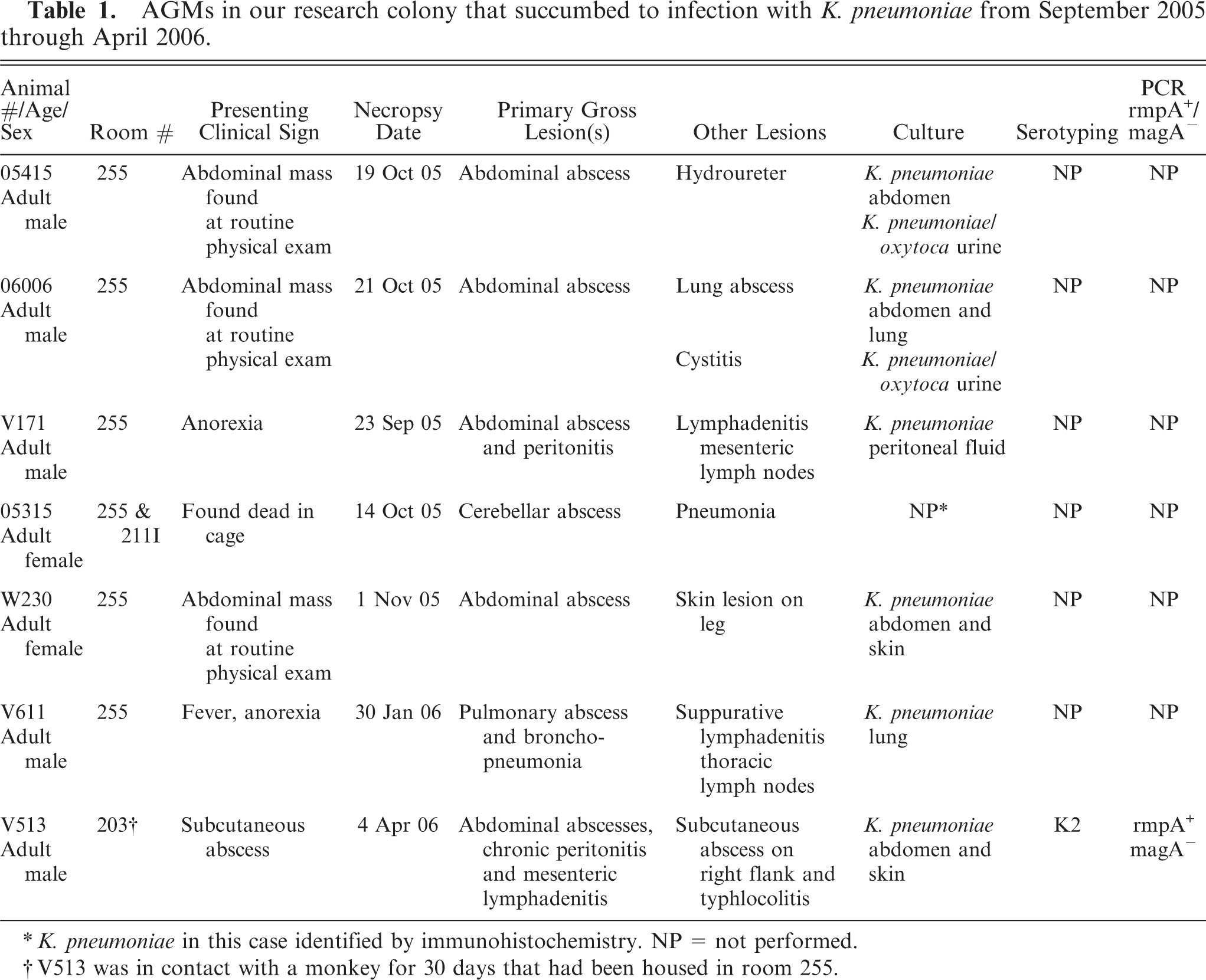
Bacteria in the abscess fluid were identified as K. pneumoniae by routine culture and biochemical methods and were further characterized as K. pneumoniae subsp. pneumoniae serotype K2 by capsular serotyping using a slide agglutination technique. 1 Furthermore, bacterial colonies plated on a blood agar plate exhibited a hypermucoviscosity phenotype, as demonstrated by a positive string test (formation of a >5 mm mucoviscous string when a loop is passed through a colony; Fig. 1). Genetic analysis of the sequence of a 760-bp amplicon of the bacterial 16S rRNA from the isolate was submitted to a basic local alignment search tool search and found to be 99% identical to several K. pneumoniae entries. Additional analysis for 2 novel genes, magA (mucoviscosity-associated gene A) and rmpA gene (regulator of the mucoid phenotype) suggested as potential hypermucoviscosity-associated genes in human cases, 5, 6 was performed by PCR using previously described primers. 4, 19 The bacterial isolate from this case was positive for the rmpA gene and was negative for the magA gene.
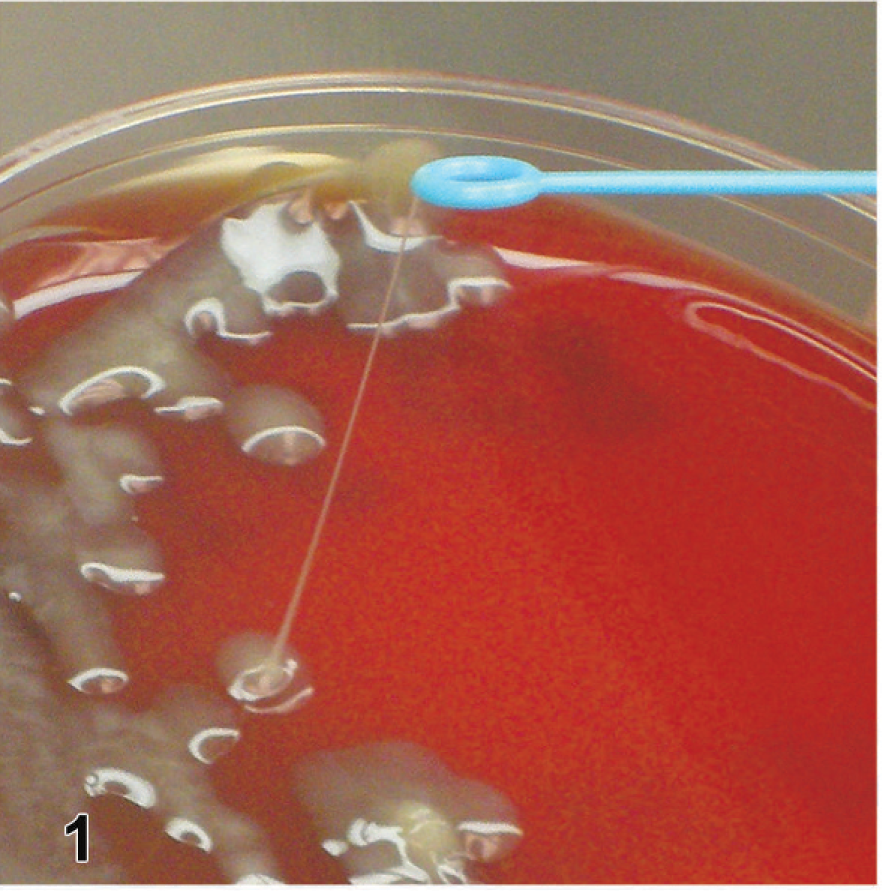
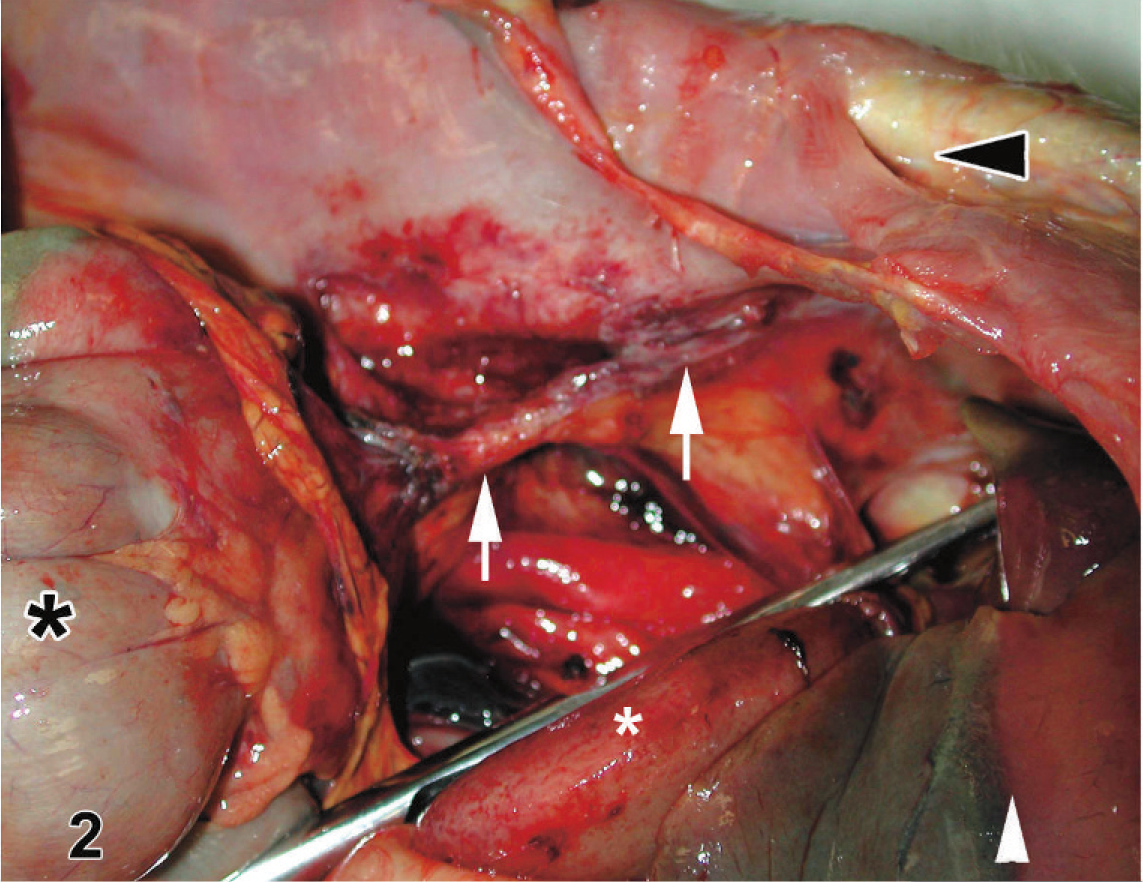
The most significant findings at necropsy were chronic pyogranulomatous peritonitis and polyserositis; chronic pyogranulomatous panniculitis of the right flank (surgical abscess site); and a defect in the abdominal wall subjacent to the panniculitis (Fig. 2). There were multiple fibrous adhesions present in the cranial abdomen. Buried within these adhesions were multiple chronic abscesses that sometimes contained a viscous fluid (Figs. 3, 4). Serosal and mesenteric adhesions enveloped and intertwined loops of small and large bowel, adhered to the right ureter and kidney, and extended into the retroperitoneal space with fingerlike projections. The abdominal wall inferior to the subcutaneous lesion of the right flank was disrupted, or breached, and an abdominal fibrous band of tissue was present extending to the cecum.
Histologically, the mesentery, mesenteric lymph nodes, and serosa of multiple organs contained multifocal abscesses composed of viable and degenerate neutrophils and cellular debris surrounded by many macrophages, fewer lymphocytes, plasma cells, and a fibrous connective tissue capsule. The macrophages contained abundant, often granular or vescicular cytoplasm (Fig. 6a). Chronic abscesses were also present in the mesentery and serosa of multiple abdominal organs. The mesenteric lymph nodes at the ileocecocolic junction contained multiple areas of necrosis, hemorrhage, and degenerate neutrophils that were surrounded by many macrophages with abundant foamy cytoplasm (Fig. 5). Fibrosis was present in the capsule, subcapsular sinus, and surrounded and replaced necrotic follicles. Some mesenteric lymph nodes were nearly replaced by fibrosis, and only remnants of their architecture were identifiable. The subcutis of the right flank contained histiocytic panniculitis with hemorrhage, necrosis, collagenolysis, and neutrophilic inflammation. Immunohistochemistry was performed on select tissue sections by the immunoperoxidase method (Envision System, DAKO Inc., Carpinteria, CA) using a rabbit antiserum to K. pneumoniae proteins (United States Biological, Swampscott, MA) diluted 1 : 4000 following heat-induced antigen retrieval with Tris base/Ethylenediamine Tetraacetic Acid (Tris/EDTA) buffer. Macrophages in sections of mesentery, serosa, and the mesenteric lymph nodes contained many immunolabeled bacteria (Figs. 5b, 6b).
Six additional AGM with clinical and pathologic features similar to animal V513, in which Klebsiella with the HMV phenotype was demonstrated, were positively diagnosed with K. pneumoniae by bacterial culture and/or immunohistochemistry (Table 1). Clinical signs in these monkeys varied from none to palpable abdominal masses noted during routine clinical examination. One monkey, 05315, was found dead in its cage with no premonitory clinical signs. All 7 affected monkeys were either housed within, or were in contact with monkeys housed within, 1 animal room in our facility. No other risk factors (i.e., sex, age, medical history, protocol manipulations, etc.) were identified. The most notable gross lesions in these additional cases were multifocal abscesses filled with a viscous mucoid material present in varying locations that included the abdomen, lung, brain, and skin (Table 1). Multiple abdominal abscesses were seen. These were associated with peritonitis and mesenteric adhesions that entrapped loops of bowel and enlarged or abscessed lymph nodes, constituting the palpable masses noted clinically. These masses were noted in 3 key areas, the root of the mesentery, the ileocecocolic junction, and the pelvic inlet, and they appeared to be centered on the lymph nodes in those areas. Bacteria in culture samples identified as K. pneumoniae were present in 5 of the additional cases by an external diagnostic laboratory but were not available for further diagnostic analysis. In the sixth additional case, the cerebellar abscess was not noted until after fixation of the brain, so culture was not possible. However, a histologic section of cerebellum from this monkey did have bacteria labeled by the K. pneumoniae antibody using immunohistochemistry.
AGMs in our research colony that succumbed to infection with K. pneumoniae from September 2005 through April 2006.
K. pneumoniae in this case identified by immunohistochemistry. NP = not performed.
V513 was in contact with a monkey for 30 days that had been housed in room 255.
The pathologic presentation of multisystemic abscessation in this group of AGMs, especially in the abdominal cavity, is unique in our experience. In 1 monkey, the bacterial isolate of K. pneumoniae was shown to express the HMV bacterial colony phenotype, K2 capsular serotype, and rmpA+/magA− genotype similar to the highly invasive K. pneumoniae with HMV phenotype that has emerged as a human pathogen in the last 2 decades. 2, 10, 11, 13, 17 We were only able to demonstrate the HMV/K2 phenotype in a single affected case. However, the remaining cases in which K. pneumoniae was diagnosed had similar clinical and pathologic features indicating invasive disease. These similarities, along with the shared temporal and spatial factors of these cases, lead us to conclude that all 7 monkeys probably were infected by the same strain of K. pneumoniae. Our finding that invasive K. pneumoniae most frequently manifest as abdominal abscessation may be a feature unique to AGMs compared with humans. Additionally, extensive fibrosis is not discussed in the human literature; yet, this was a prominent feature in our AGMs, especially in those with abdominal lesions. We are not certain whether fibrosis is a species-specific response, an indication of chronicity, a response caused by a specific characteristic of the bacteria, or a result of combined factors.
The rmpA+/magA− genotype demonstrated in the bacterial isolate from 1 monkey is consistent with human HMV isolates of K. pneumoniae, in which the rmpA gene is present in both K1 and K2 capsular serotypes, as well as nearly 67% of non–K1/K2 serotypes, 17 but the magA gene appears restricted to isolates of the K1 serotype. 15 Furthermore, the magA gene appears to correlate particularly with the development of primary liver abscesses, or liver abscesses combined with metastatic abscesses, in humans. 2, 10, 16 Of note in that regard, liver abscesses were not evident in any of the monkeys at our facility, all of which were presumably magA−.
Our demonstration of the K2 capsular serotype in the one monkey isolate is of particular significance, as capsular serotype appears to play a key role in the virulence of invasive K. pneumoniae. Serotype K1 and K2 isolates of K. pneumoniae have been reported to be significantly more resistant to phagocytosis and more virulent in the mouse model than non-K1/K2 isolates, 17 even non-K1/K2 isolates that were rmpA+. However, among the non-K1/K2 strains, those that possessed the rmpA gene were more resistant to phagocytosis than the rmpA− strains, so rmpA may still contribute to the pathogenesis of K. pneumoniae in vivo. The magA gene may also contribute to virulence, but like rmpA, it does not appear to be as significant a contributor to virulence as the K1 or K2 phenotype. 17
The means by which the causative K. pneumonia may have spread or caused disease in individual monkeys in our colony is unknown. The only significant epidemiologic factor we identified was that affected monkeys were maintained in the same room or had contact with a monkey housed in that room. Of note, no clinical or pathological cases have been identified in the 14 months between the last identified case and the preparation of this manuscript. Also, bacteriological testing of fecal and oral swabs of 20 African green monkeys in our colony did not yield any isolates of K. pneumoniae (data not shown). However, as we were completing this manuscript in June 2007, a routine oral swab from a recently obtained AGM in quarantine at our institute yielded K. pneumoniae showing the HMV phenotype and rmpA+/magA− genotype. This AGM exhibited no abnormal clinical signs during quarantine. The animal was euthanatized for precautionary reasons and a full necropsy was performed which revealed no gross abnormalities. The epidemiological significance of this case remains uncertain.
Mice are susceptible to experimental infection with HMV strains of K. pneumoniae and appear to provide a useful model for pathogenesis studies of invasive K. pneumoniae. To our knowledge, however, this report represents the first time that invasive K. pneumoniae with the HMV phenotype associated with abscess formation has been identified to occur spontaneously in animals. The fact that 7 AGMs over a few months' time demonstrated abscessation in multiple tissues shows that this species is quite susceptible to invasive K. pneumoniae infection. Therefore, veterinarians, laboratory workers and research pathologists should be aware of this pathogen as a cause of abdominal masses and multisystemic abscessation in the AGM. In addition, the AGM may provide another useful animal model to understand the pathogenesis of this emerging human pathogen.
Isolate (KPV513) plated on a blood agar plate; AGM V513. A positive string test (>5 mm string length) distinguishing the hypermucoviscosity phenotype. Oval tip of inoculating loop is approximately 7 mm.
Subcutaneous tissue of right flank (black arrowhead), liver (white arrowhead), left kidney reflected by hemostat (white asterisk), cecum (black asterisk); AGM V513. Note the peritoneum of abdominal wall and mesentery, plus the serosa of abdominal organs, are irregularly red and have a dull, granular appearance consistent with peritonitis and polyserositis. Inferior to the subcutaneous tissue of the right flank, an irregular fibrous band of tissue (white arrows) extends from the serosa of the cecum in a fingerlike projection to the abdominal wall.

Ileum, cecum, colon; AGM V513. Note the red, enlarged, and irregular serosa of the ileocecocolic junction.
Ileocecocolic junction; AGM V513. Further dissection of the region shows chronic abscesses (arrows), one of which has ruptured and drained. Highly viscous and mucoid material draining from an abscess (box insert).
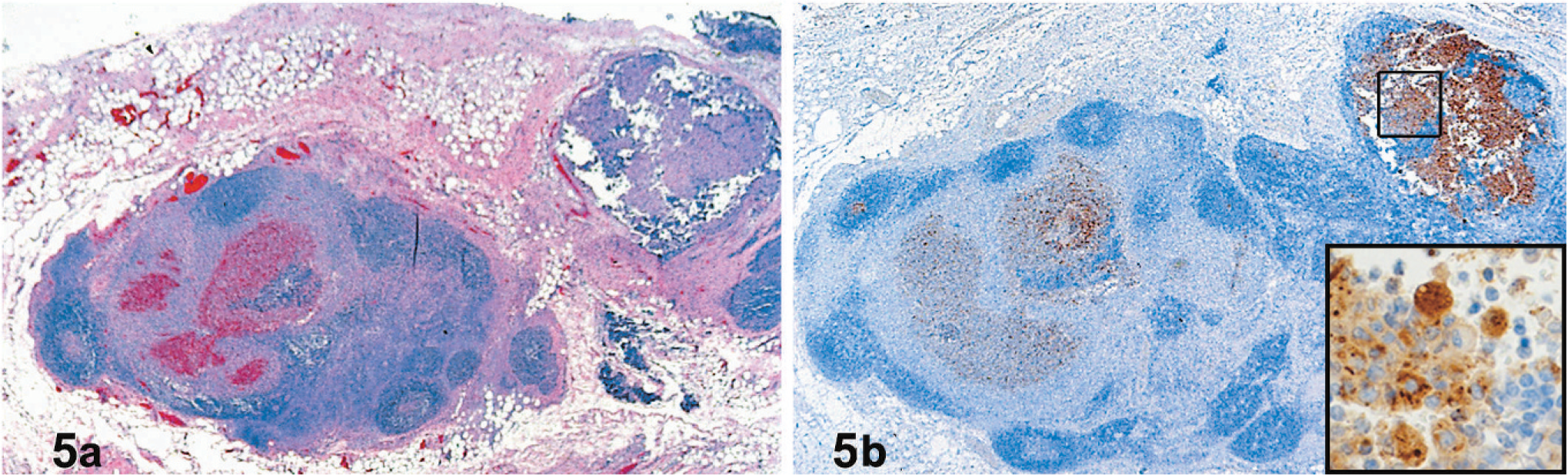
Lymph node, mesenteric; AGM V513. There is irregular widening of lymph node sinuses by many macrophages. There is hemorrhage and necrosis with loss of lymphocytes. HE.
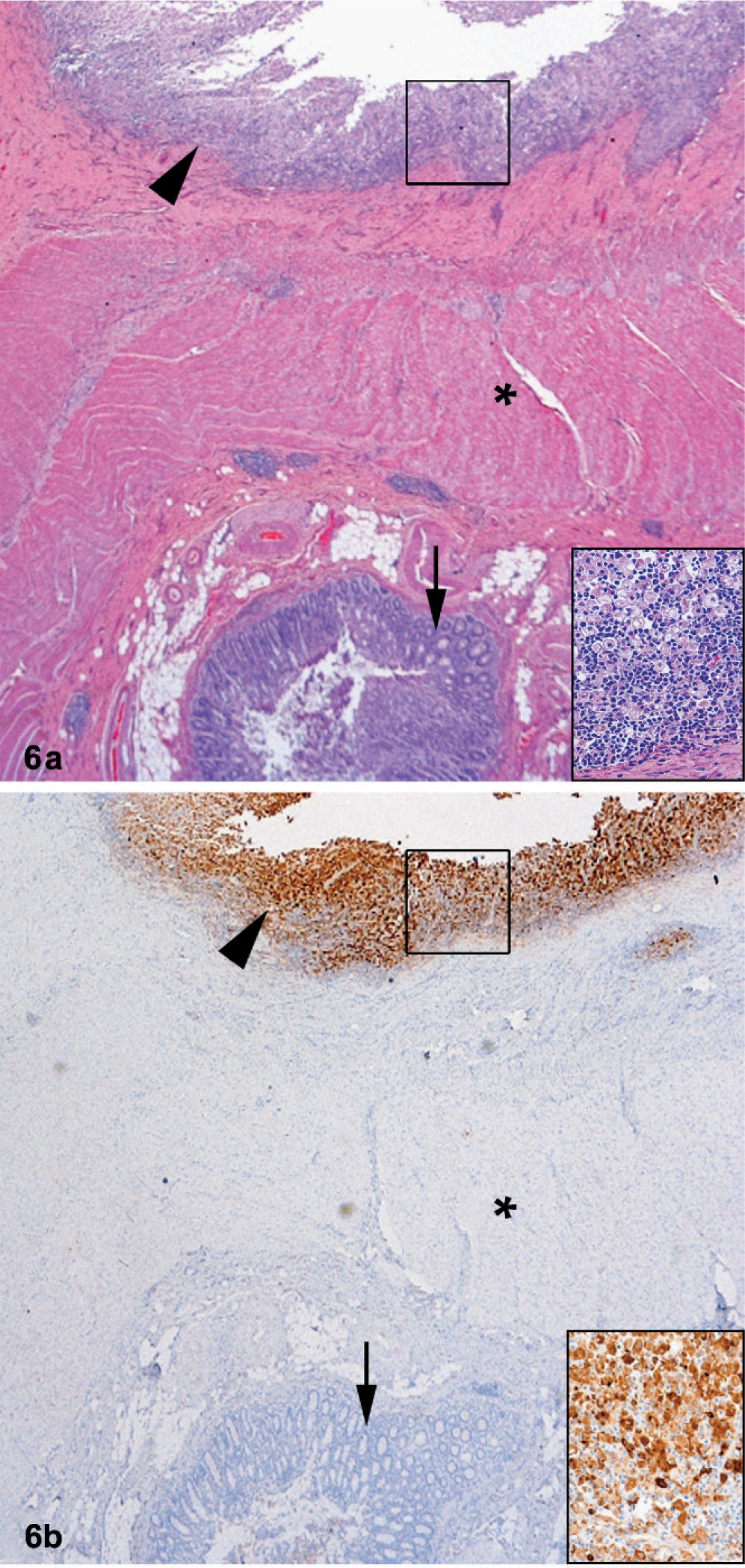
Ileum, tunica mucosa (black arrow), tunica muscular (black asterisk), serosa (arrowhead); AGM V513. Note the fibrosis and inflammation within the serosa. HE. Inflammation is composed of many large macrophages with abundant cytoplasm, lymphocytes, and neutrophils. HE (box insert).
Footnotes
Acknowledgements
We are grateful to Stephen Libby, Department of Laboratory Medicine, University of Washington for providing us with the magA+ K. pneumoniae strains used as positive controls and to Polly Kaufmann, Health protection Agency, Centre for Infections, London, UK, for K1 and K2 antisera. We also thank Jeff Brubaker, Neil Davis, Gale Krietz, John Kondig Chris Mech, and Larry Ostby (USAMRIID) for assistance in their respective fields of expertise. The views, opinions, and/or findings contained herein are those of the authors and should not be construed as official government position, policy, or decision unless so designated by other documentation.