
Abstract
Juvenile onset renal disease is described in 2 male and 2 female young Rottweiler dogs. Histologic changes in all dogs were cystic dilatation of Bowman's space, mesangial hypercellularity, and glomerulosclerosis. Three dogs also had glomerular crescents and moderate to severe interstitial fibrosis. Electron microscopy revealed glomerular basement membranes of variable thickness, with extensive splitting or lamellation of the lamina densa. These ultrastructural findings are similar to those found in people and in other breeds of dogs with inherited defects in type IV collagen.
Familial renal disease, typically resulting in chronic renal failure, has been reported in several breeds of dogs. 15, 17 Changes in the kidney described in these diseases include agenesis, hypoplasia, dysplasia, glomerulopathy, tubulointerstitial nephropathy, and tubular transport dysfunction. 17 Primary inherited glomerular basement membrane abnormalities have been described in the juvenile onset renal diseases of Samoyeds, 1, 9 Doberman Pinschers, 2, 18 English Cocker Spaniels, 12, 13 Bull Terriers, 7, 15 Dalmatian dogs, 6 and mixed breed “Navasota” dogs; 11 these diseases share similarities with Alport syndrome in people. 10
Alport syndrome is the result of congenital defect in the molecular structure of type IV collagen, which is the major structural component of the glomerular basement membrane (GBM). Type IV collagen in the mature GBM is present predominantly as extensively cross-linked trimers of α3, α4, and α5 type IV isoforms. 8, 10 Mutations of the COL4A3, COL4A4, or COL4A5 genes result in a structurally and functionally abnormal GBM, which becomes progressively thickened and split, with the eventual development of glomerulosclerosis. 20 Clinically, Alport syndrome is characterized by hematuria; progressive nephritis with proteinuria; declining renal function; and, in some people, hearing and ocular abnormalities. Histologic renal findings in people include mild mesangial hypercellularity; global to segmental glomerulosclerosis; immature glomeruli; tubular atrophy; and interstitial fibrosis, with eventual evolution to end stage renal disease. Although the light microscopic findings in this disease are nonspecific, the ultrastructural changes are diagnostic. The GBM is less electron dense and of variable thickness because of a complex interwoven “basket-weave” replication of the lamina densa. 21 There may be podocyte foot process effacement, and the epithelial aspect of the capillary wall is typically irregular. 10 Canine models of Alport syndrome have been described in Samoyed, “Navasota,” Doberman Pinscher, Dalmatian, and Bull Terrier dogs. Dogs with Alport syndrome have proteinuria and progressive renal disease, without hematuria, hearing, or visual abnormalities. Histologic and light microscopic findings are similar to those described in people. 19 These canine models have made significant contributions to the understanding of the pathogenesis and pathology of Alport syndrome in people.
A single report has previously described the clinical and light microscopic findings in 4 related Rottweiler dogs that developed renal failure with proteinuria before 1 year of age. 3 We report here an additional 4 cases of similar renal disease in young Rottweiler dogs, 2 of which are related. In addition to clinical and histologic findings, ultrastructural features of this renal disease are described.
The cases in this report were referred to the University of Georgia Veterinary Medical Teaching Hospital or the Athens Diagnostic Laboratory. In all cases, renal tissues were fixed by immersion in 10% neutral buffered formalin and were routinely processed into paraffin, and 3-μm sections were cut for hematoxylin and eosin staining to be evaluated histopathologically. Renal tissue from dog Nos. 2 and 3 were obtained from the paraffin-embedded tissue blocks after being deparaffinized with 100% xylene. After postfixation by osmication for 1 hour, the tissues were dehydrated and embedded into Epon and were processed routinely for transmission electron microscopic examination.
An 8.5-month-old male Rottweiler (No. 1) was admitted to a private veterinary practice because of vomiting and weight loss. According to the owner, the dog was clinically normal until 4 months of age but was currently much smaller than its litter mates. Abnormal laboratory findings included azotemia (blood urea nitrogen, BUN 55 mg/dl; reference interval, 8–28 mg/dl), 14 hyperphosphatemia (phosphorus, 21.1 mg/dl; reference interval, 2.9–5.3 mg/dl), 14 hypoalbuminemia (albumin, 2.2 g/dl; reference interval, 2.3–3.1 g/dl), 14 and mild anemia (hematocrit [Hct], 32.5%; reference interval, 35–57%). 14 The urine was isosthenuric (urine specific gravity, 1.012), with proteinuria on dipstick (the degree not available). Juvenile onset glomerulopathy was suspected, based on clinical signs, laboratory findings, and signalment. The dog was euthanized because of continued clinical deterioration, and a necropsy was performed (results of gross findings not available). Histologic examination revealed moderate cystic dilatation of Bowman's spaces, with small associated glomerular tufts. Glomeruli were hypercellular because of mesangial-cell hyperplasia, and there was moderate mesangial-matrix expansion (mild glomerulosclerosis). There was irregular thickening of some glomerular capillary loops, rare glomeruli were focally adhered to Bowman's capsules, and there was focal crescent formation. Renal tubules were often dilated, some contained hyaline casts, and there was moderate cortical interstitial fibrosis and tubular atrophy.
An 8.5-month-old spayed female Rottweiler (No. 2) had a gastrotomy for foreign-body removal by a referring veterinarian. During the 1.5 months after surgery, the dog had vomiting, anorexia, polyuria, polydipsia, lethargy, and weight loss. The dog was reevaluated by the referring veterinarian, and abnormal laboratory findings of azotemia with isosthenuria were detected (data not available). The dog was referred to the University of Georgia Veterinary Medical Teaching Hospital for further evaluation and treatment. Laboratory findings included azotemia (BUN, 71 mg/dl), hypoproteinemia (total protein, 4.3–5.0 g/dl; reference interval, 5.4–7.5 g/dl), 14 hyperphosphatemia (phosphorus, 12.3–15.9 mg/dl), and mild anemia (Hct, 32.9%). Urinalysis revealed isosthenuria (urine specific gravity, 1.010–1.012), 2+ positive for protein on dipstick, and an elevated ratio of urine protein to urine creatinine (5.4–8.8; reference interval, less than 0.5). 14 Leptospirosis titers were negative. Abdominal radiographs were unremarkable, and the abdominal ultrasound revealed that both kidneys were normal in size and shape but were hyperechoic. Based on these findings, glomerulonephritis was suspected and tests to rule out underlying inflammatory diseases that are potential causes of glomerulonephritis were performed. An antinuclear antibody titer was negative, making lupus nephritis unlikely. An occult heartworm test and titers for Ehrlichia, Rocky Mountain spotted fever, and Lyme disease were negative. Two Tru-cut biopsy specimens were taken from the left kidney for microscopic examination. Histologically, there were markedly dilated Bowman's spaces, and Bowman's capsules were slightly thickened. The glomerular capillary tufts appeared small, with mild mesangial-cell hypercellularity and slight thickening of capillary loops. Sections of kidneys stained with Masson's trichrome did not demonstrate any capillary-wall immune deposits (data not shown).
A 9-month-old female Rottweiler (No. 3) was admitted to a private veterinary practice because of acute onset of abdominal pain. The dog had azotemia (BUN, 60–70 mg/dl), hyperphosphatemia (phosphate, 16 mg/dl), and anemia (Hct, 24%). Serum albumin was slightly low (specific values not available) but still within the normal reference range. The urine was isosthenuric (urine specific gravity, 1.008–1.017) and was 4+ positive for protein on dipstick. Leptospira titers were negative. Chronic renal failure was suspected, and the dog was treated with fluids and ampicillin. The dog was euthanized because of continued azotemia and anorexia, and a necropsy was performed. Both kidneys were grossly pale, and the cortex was granular. Histologically, glomeruli were hypercellular because of mesangial-cell hyperplasia, and there was mesangial-matrix expansion. There was irregular thickening of the glomerular capillary loops, and occasional crescents were observed. Bowman's capsule was often dilated. There was severe cortical interstitial fibrosis, with diffuse tubular and capsular basement membrane mineralization and tubular atrophy (Fig. 1). Moderate numbers of tubules contained eosinophilic hyaline casts, indicative of proteinuria. Congo red staining for amyloid and trichome staining for immune deposits were negative (data not shown).
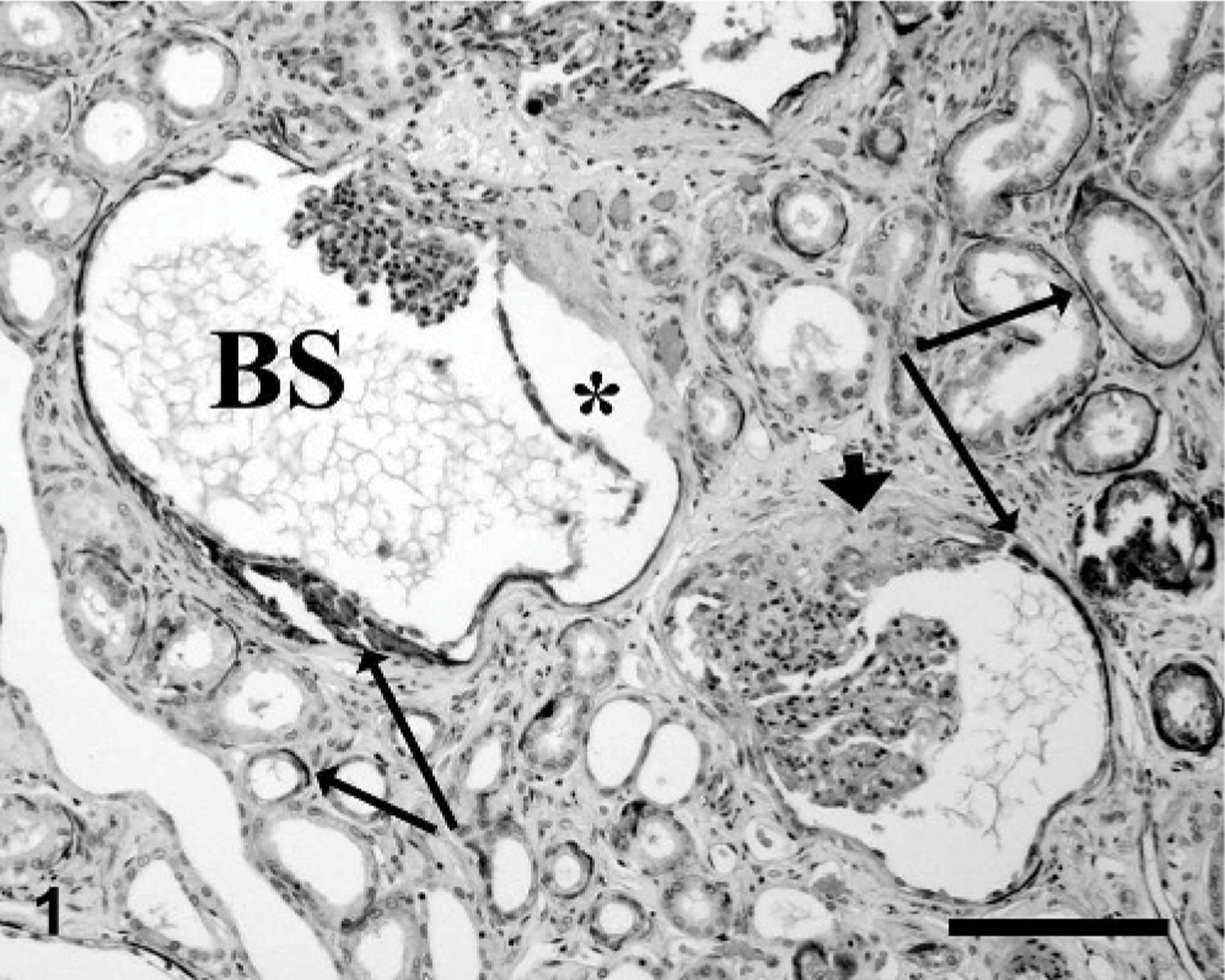
Kidney, renal histology; dog No. 3. Bowman's space (BS) is expanded, there is diffuse basement membrane mineralization (long arrows), tubular atrophy, and the interstitium is fibrotic. The glomerular capillary tufts are hypercellular, and there are occasional glomerular crescents with synechia (short arrow). There is artifactual separation of the mineralized capsule from the adjacent interstitium (asterisk). HE. Bar = 100 μm.
A male litter mate (No. 4) of dog No. 3 was admitted at 10 months of age to a private veterinary practice because of weight loss. The dog was reported to be azotemic (data not available) and was euthanized. Formalin-fixed kidney tissue was submitted for histologic evaluation. The histologic changes were similar to those seen in the other affected litter mate (dog No. 3), consisting of mesangial-cell hyperplasia, mesangial-matrix expansion, irregular thickening of glomerular capillary loops, occasional crescents, mild dilatation of Bowman's capsule, moderate basement membrane mineralization, tubular atrophy, and moderate to severe interstitial fibrosis (Fig. 2).
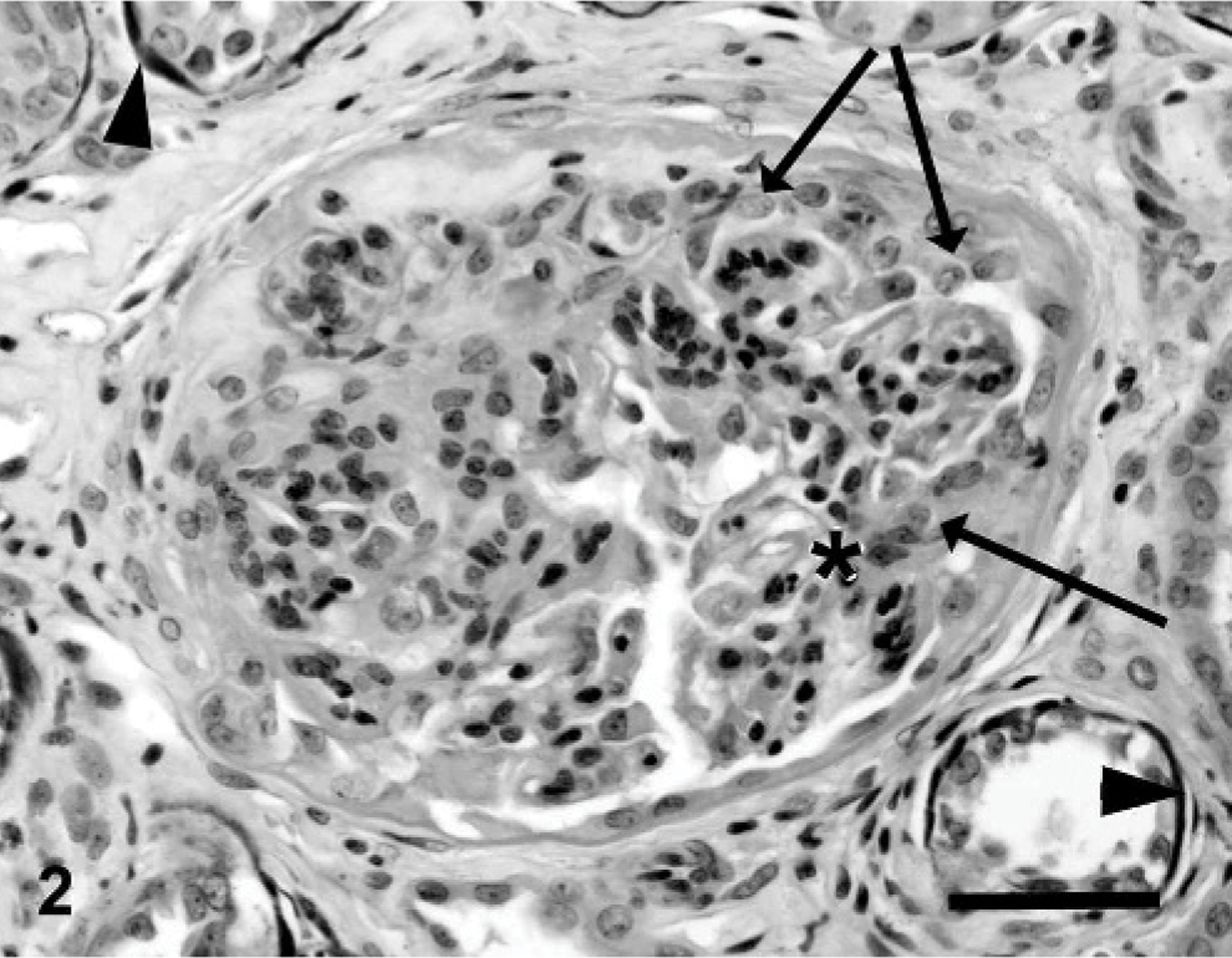
Kidney, glomerular histology; dog No. 4. The glomerulus is hypercellular, the capillary loops are collapsed, and there are large fibrocellular crescents (arrows). The capillary tuft is focally adhered to these crescents (asterisk). There is moderate interstitial fibrosis and basement membrane mineralization (arrowheads). HE. Bar = 50 μm.
To more accurately define the glomerular changes present in these dogs, kidney tissue from dog Nos. 2 and 3 were further examined by transmission electron microscopy. Abnormal ultrastructural changes were observed in the GBM in both dogs. The GBM was of irregular thickness, with extensive splitting and thickening of the lamina densa (Figs. 3 and 4). There was diffuse podocyte foot process effacement, with scalloping of the epithelial aspect of the capillary wall. Paraffin-embedded blocks of renal tissue from an age matched control dog (1.5-year-old female Rottweiler with fatal parvoviral enteritis) were also examined ultrastructurally (Fig. 4. Inset ). Although the tissue from the control dog had moderate autolysis, the homogeneous nature of the normal GBM and the normal structure of the podocyte foot processes could still be appreciated. These findings also confirmed that the ultrastructural GBM changes seen in dog Nos. 2 and 3 were not artifacts caused by processing of paraffin-embedded tissue for electron microscopy.
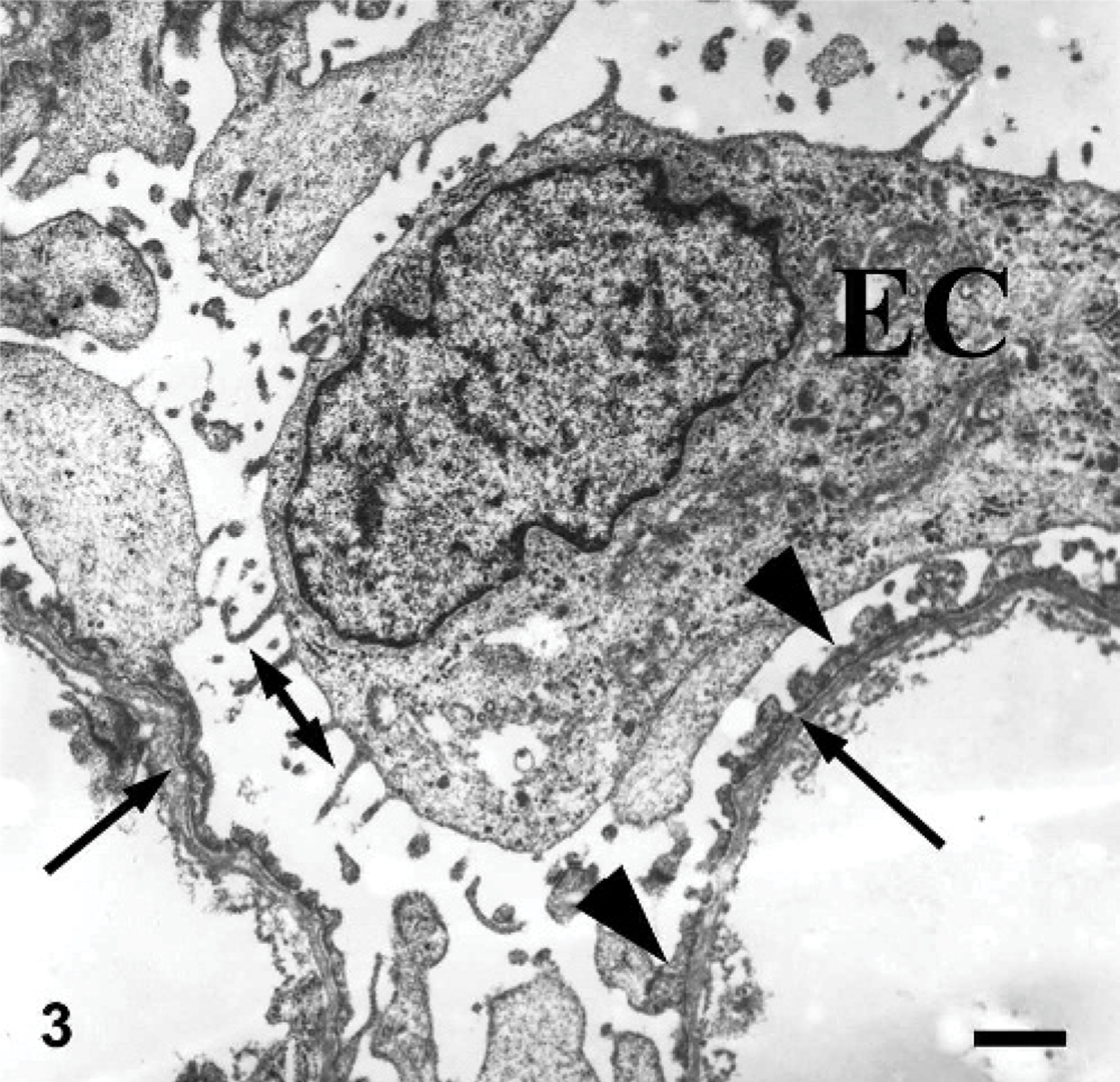
Kidney, glomerular capillary loop ultrastructure; dog No. 2. The glomerular basement membrane is of irregular thickness, with longitudinal multilaminar splitting of the lamina densa (arrows). There is epithelial cell (EC) foot process effacement (arrowheads) and villous transformation (double arrows). Bar = 1 μm.
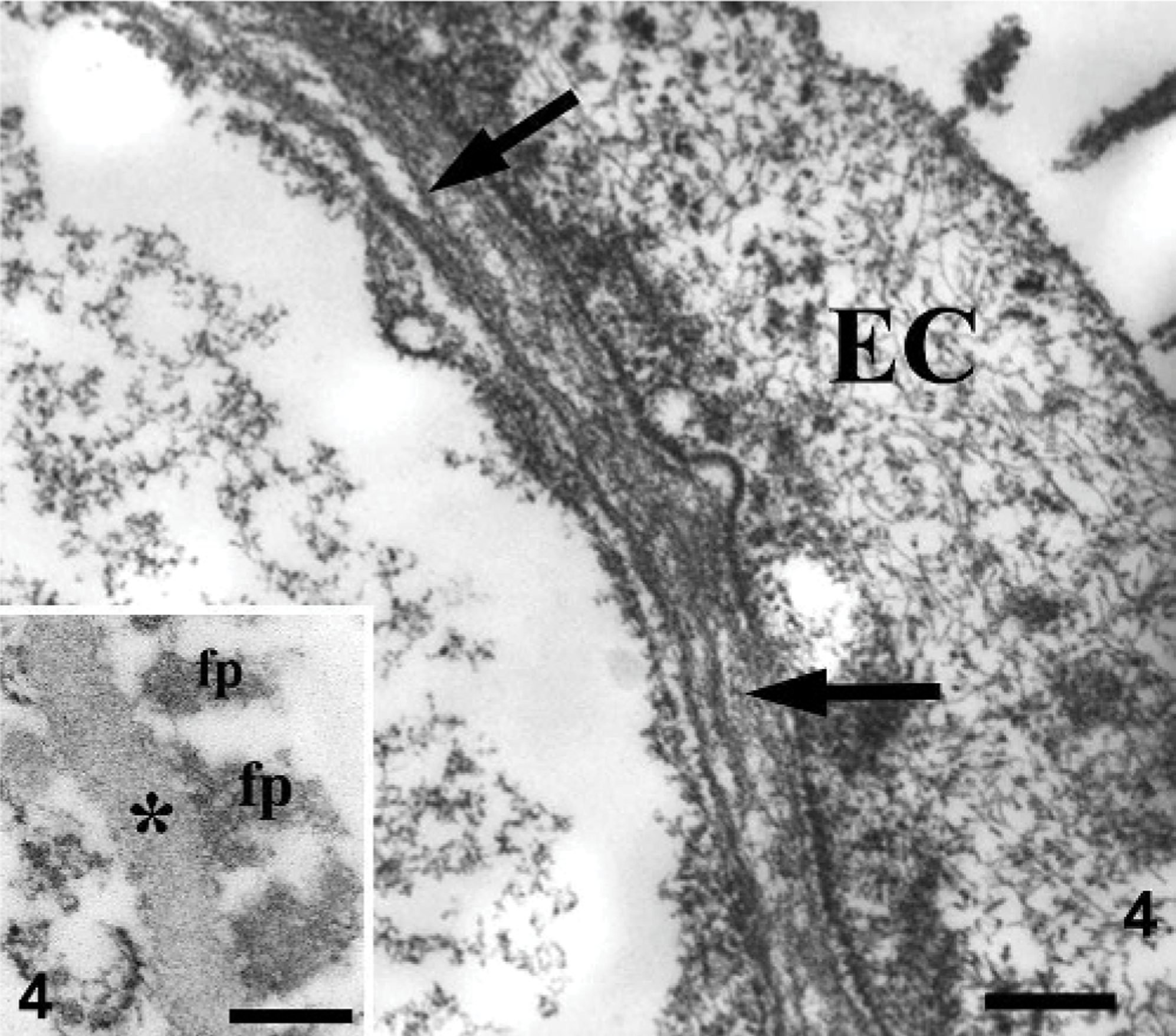
Kidney, glomerular ultrastructure; dog No. 2 and normal dog (inset). Note the “basket-weave” splitting of the thickened lamina densa (arrows) and effacement of the overlying epithelial cell (EC). In contrast, the normal (inset) GBM is homogeneous and epithelial foot processes (fp) are present. Bars = 300 nm.
We described 4 young Rottweilers (2 males, 2 females) with renal disease. All 4 dogs were azotemic. Three of the 3 tested dogs (dog Nos. 1, 2, and 3) had evidence of proteinuria, and 2 of the dogs were hypoalbuminemic. Dog Nos. 1, 3, and 4 were euthanized because of severe renal disease by 10 months of age; however, dog No. 2 was confirmed to be alive at 16 months of age. On microscopic examination, the kidneys of all dogs had cystic dilatation of Bowman's spaces, mesangial hypercellularity, glomerulosclerosis, and irregular thickening of glomerular capillary loops, which were consistent with findings described previously in 4 related young Rottweilers. 4 Glomerulosclerosis may be a relatively nonspecific reflection of glomerular injury or scarring, as occurs in dogs with decreased functioning renal mass, and is characterized by mesangial-matrix expansion and mesangial-cell hyperplasia, which may cause segmental solidification of peripheral capillary loops. Although only mild glomerulosclerosis was observed in one dog (No. 2), the 3 remaining dogs had morphologic evidence of more severe renal injury. Adhesions of sclerotic portions of the tuft to Bowman's capsule are common secondary changes associated with more severe glomerulosclerosis and were present in dog Nos. 1, 3, and 4. These 3 dogs also had occasional crescents, which form after breaks in the GBM, with leakage of fibrinogen into Bowman's space and resultant macrophage infiltration, proliferation of parietal epithelial cells, and fibrosis. These 3 dogs also had moderate to severe interstitial fibrosis and tubular atrophy, indicative of progression to end stage renal disease.
The histologic and ultrastructural lesions seen in these Rottweiler dogs are similar to those described in other dog breeds and in people with Alport syndrome. The cystic glomerular capsular change, which was present in these Rottweilers, has been described in Bull Terriers 5, 7 and some Doberman Pinschers 2 but has not been reported in people and other dog breeds with Alport syndrome. This lesion has been termed “cystic glomerular atrophy,” based on the small size of some glomeruli within the dilated Bowman's space. Immature glomeruli, which have been described in Bull Terriers 7 and people 10 with Alport syndrome, were not observed in these Rottweiler dogs. The glomerular changes of increased glomerular cellularity and irregular thickening of the capillary loops were initially misinterpreted as membranoproliferative glomerulonephritis (MPGN) in some dog breeds with Alport syndrome. Although MPGN is characterized by increased glomerular cellularity and thickened capillary loops, MPGN is a consequence of immune complex or complement deposition in the glomerular capillary wall. A diagnosis of MPGN is dependent on the demonstration of these immune deposits by electron microscopy and, for optimal characterization, immunofluorescent techniques. Immune deposits are not a feature of Alport syndrome. Although there is variability in the light microscopic renal lesions among breeds of dogs and people with Alport syndrome, the GBM ultrastructural changes of lamellation are pathognomonic for this disease. 6, 7, 9, 10, 11, 13, 18 Therefore, a diagnosis of this disease is absolutely dependent on ultrastructural examination of the kidney. Further studies are needed to define the suspected collagen defect present in Rottweiler dogs with this juvenile onset renal disease.
Footnotes
Acknowledgements
The authors thank Mary Ard for help with electron microscopy.