
Abstract
A 3-year-old female Alaskan Malamute was submitted to the Veterinary Teaching Hospital of Madrid with a mass in the right maxilla. It was ulcerated, covered by a yellowish infected membrane, and painful. The histologic examination showed a neoplastic proliferation of palisading cells distributed irregularly in cords. The tumor was diagnosed as an ameloblastic carcinoma because of the histologic signs of malignancy, the aggressive behavior, and the absence of distal metastasis. This is the first description of an ameloblastic carcinoma in a dog.
Odontogenic tumors in domestic animals are rare. Initially these were classified according to a simple human classification based on histopathologic diagnosis. 6 The actual human classification is much more accurate and complete but cannot be used in veterinary medicine since not all human tumors have yet been described in animals and some animal tumors are different from human tumors.
Tumors of odontogenic origin may arise from the epithelium or the connective tissue of the developing tooth, the surface epithelium, or odontogenic epithelium once dental formation is complete. 6, 14 Among these tumors we can find the ameloblastoma, which is a rare tumor, but the most frequent, clinically significant, epithelial odontogenic tumor described both in animals and in humans. 10 It has been reported before in horses, dogs, sheep, cats, and cattle. 5, 7, 9, 11, 15
Ameloblastomas may have different origins such as the dental lamina, the outer enamel epithelium, the dental follicule around retained unerrupted teeth, or odontogenic epithelium in extraoral locations. 13 These tumors have an invasive and aggressive nature, being able to destroy bone, and extend to the oral cavity or sinuses. There is no age predisposition; they do not depend on gender and usually affect the mandible. They have a high tendency to recur if not excised properly but do not present signs of cytologic malignancy and do not metastasize.
Ameloblastomas have been reported in many domestic animal species, but particularly in the horse and the dog, with the acanthomatous ameloblastoma being the most common form in the latter. 5, 7 In human medicine, 5 clinical/radiographic subtypes of ameloblastomas have been described: unicystic, multicystic, desmoplastic and peripheral variants, and several histologic types including plexiform, follicular, granular cell, acanthomatous, and basaloid forms. 4
Malignant forms of ameloblastomas are rare and are not included in the veterinary classification. However 2 cases have been reported in animals, an ameloblastic carcinoma in a horse 3 and an ameloblastoma in a dog with prominent formation of bone and cytologic signs of malignancy. 16 We describe the third case of a malignant form of ameloblastoma in domestic animals, an ameloblastic carcinoma located in the right maxilla of an Alaskan Malamute.
A 3-year-old female Alaskan Malamute was submitted to the Veterinary Teaching Hospital of Madrid for a second opinion over a previously diagnosed tumor in the right maxilla. The owners had first noticed it 4 months before and described a moderately fast growth of the mass since its detection. The mass was ulcerated, covered by a yellowish, infected membrane, and painful. It included the area from the upper right second incisive to the upper right second premolar. The hard palate was also invaded by the mass. Radiographic survey of the area showed a severe osteolisis of the right incisive and the maxilla, and radiolucent areas in the center of neoplasm compatible with fluid. The dog presented a good body condition. Hematology and the biochemical profile were normal.
A second incisional punch biopsy of the mass was taken in 3 different areas, and the samples were submitted to the Pathology Service of the Veterinary Teaching Hospital. The histologic examination revealed a neoplastic proliferation of palisading cells with nuclei in the apical poles, distributed irregularly in cords. In some areas, the center of the epithelium was degenerated and originated cysts. The diagnosis of a peripheral ameloblastoma was given and a partial hemi-maxillectomy was programmed because of the radiologic signs of bone involvement. The radiologic image of the thorax was not compatible with metastasis. Lymph nodes were normal in size and did not seem to be affected.
The hemi-maxilla containing the mass and dental pieces 102 to 106 was submitted for histologic examination. It presented a bone deformity of 10 cm in diameter. Once sliced, the tumor presented large, black, cystic cavities (Fig. 1). The sample was routinely fixed in buffer formalin and processed in 4-mm paraffin-embedded cassettes; 5-μm cuts were obtained and stained with hematoxylin and eosin for histology. Since the sample was now larger, a more detailed observation of the cytologic features of the tumor was permitted.

Hemi-maxilla; dog. Gross morphology of the sliced tumor. Presence of large cystic cavities. A hemi-maxilectomy was performed because of the bone invasion of the tumor.
In some areas, the neoplasm presented a proliferation of epithelium in irregular cords and islands dispersed in a fibrous tissue. Sparsely, the center of the epithelium degenerated and formed cysts. The basal cells of the epithelium tended to be in palisade with nuclei at the apical poles, and central masses of cells resembled the “stellate reticulum” of the enamel organ. The cells were pleomorphic, varying from round to spindle shaped, and the cytoplasm could be dark and eosinophilic or very vacuolar. The nuclei also presented pleomorphism, varying from large and round, oval to picnotic, or small and hyperchromatic (Fig. 2). The nucleus/cytoplasm ratio in general was high, and the mitotic figures were counted 5 to 6 per high magnification field. In some areas the epithelial cells invaded the stroma, becoming undifferentiated. The tumor was very aggressive and invaded bone tissue.
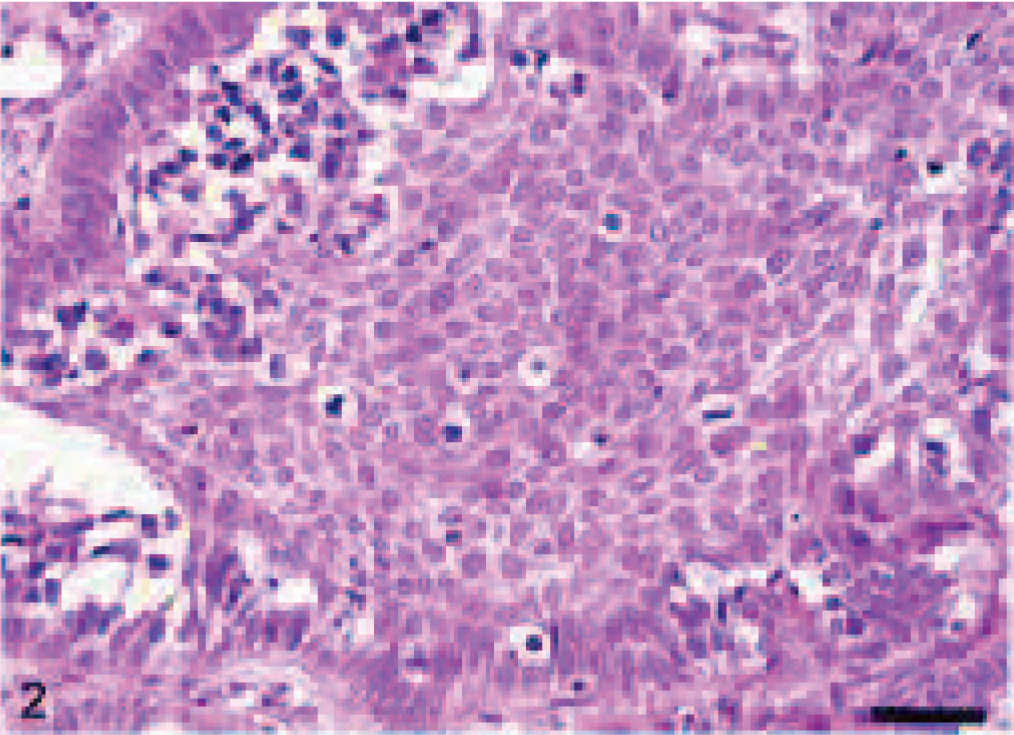
Ameloblastic carcinoma; dog. Palisaded basal cells of the epithelium with nuclei at the apical pole, and areas of cells resembling the “stellate reticulum” of the enamel organ. HE. Bar = 75 μm.
Studies in human odontogenic tumors have found co-expression between cytokeratins and vimentin in certain neoplasms; and in the oral cavity, the only ones that presented this feature were those of ameloblastomatous epithelial origin. 12 Antibodies against both intermediate filaments were used for immunohistochemical labeling. An indirect streptavidin-biotin immunoperoxidase method was used, and the tumor was strongly positive for cytokeratin AE1/AE3 (Master Diagnostica) (includes acid and basic cytokeratins I and II) (Fig. 3a), while for vimentin expression (Master Diagnostica, Oficina, Granada), it was negative (Fig. 3b). Immunohistochemical labeling for melan A (Novocastra, Newcastle upon Tyne, UK) yielded a negative result, so melanoma was ruled out.
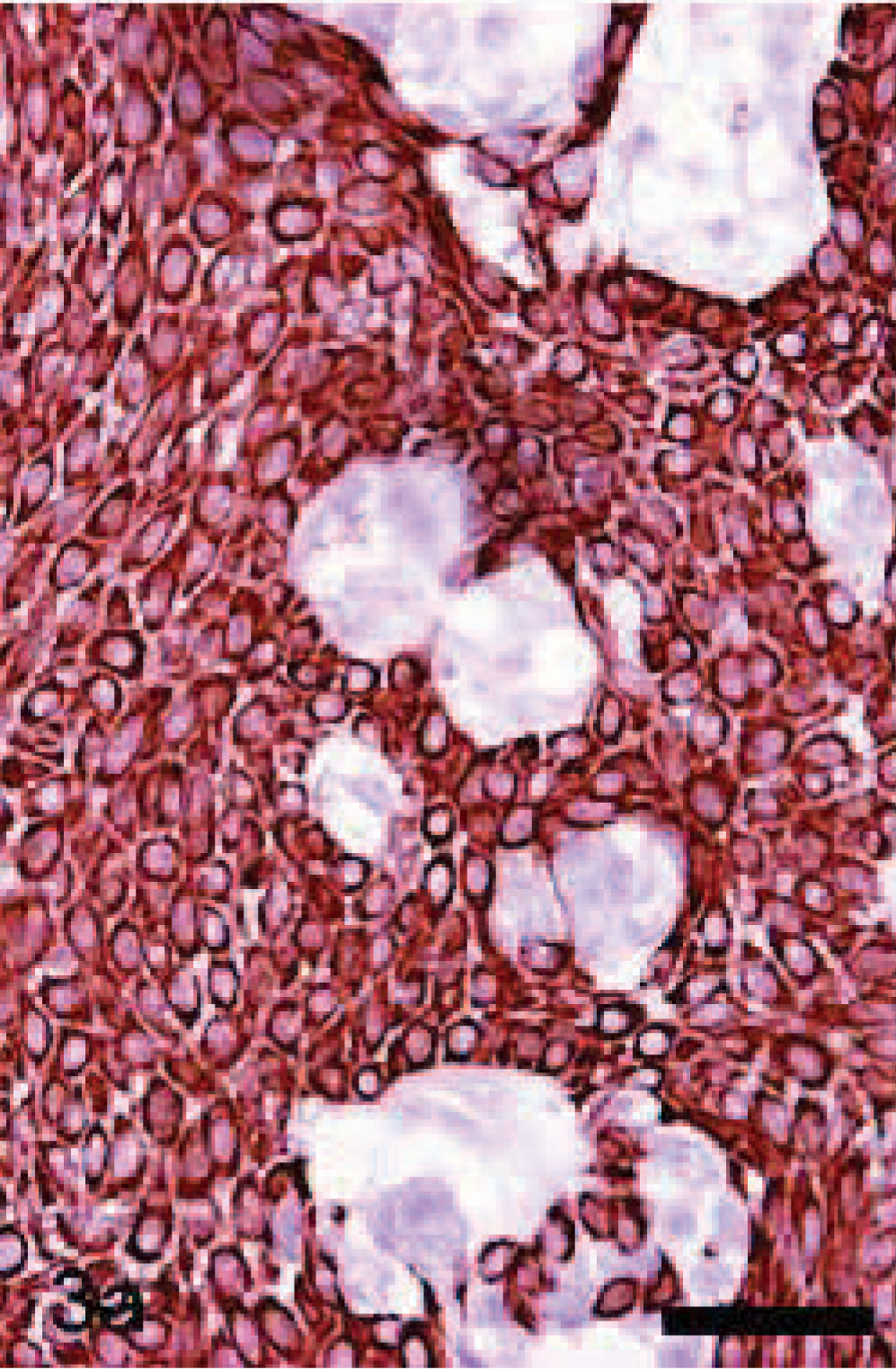
Ameloblastic carcinoma; dog. Positive immunohistochemical labeling for cytokeratin AE1/AE3 in the epithelium. Bar = 75 μm.
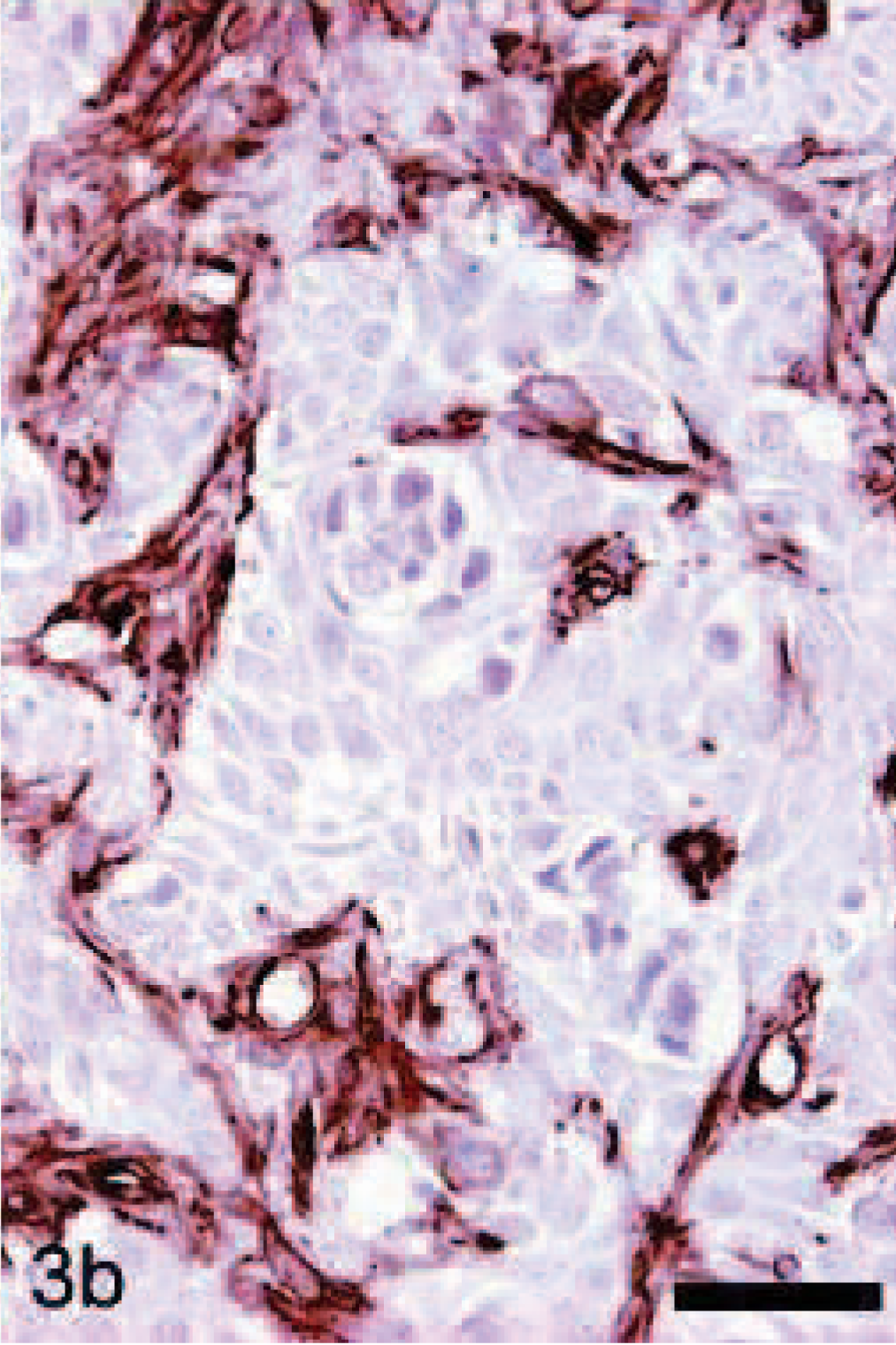
Ameloblastic carcinoma; dog. Negative immunohistochemical labeling of the tumor for vimentin. Bar = 75 μm.
The tumor was diagnosed as an ameloblastic carcinoma because of the histologic signs of malignancy, the aggressive behavior, and the absence of distal metastasis.
The patient presented some postsurgical complications because of the large defect of bone and tissue. Consequently, an oral-nasal fistula occurred, and the dog had to go through surgery 3 more times to solve the problem. Revisions every 6 months were scheduled to check for tumor recurrences. Neither radiotherapy nor chemotherapy was recommended. At the present time, 2 years after surgical treatment, the dog is in good condition (except for a chronic bronco-pneumonia caused by the postsurgical complications), and there are no signs of recurrence.
In humans, ameloblastomas represent only 1% of tumors and cysts in the jaw. 1 In dogs they are also rare but are the most common of the odontogenic tumors. 10 They have also been reported in other species such as in cattle and less frequently in horses. 5, 8 The ameloblastoma is benign, yet very aggressive, invading bone and even causing death owing to invasion of vital organs, but it does not metastasize. The tumor can appear at any age and does not present a tendency for gender. The mandible is its usual location both in humans and dogs.
The term ameloblastic carcinoma is also subject of controversy in the human classification. In this case report we are going to refer to the definition given by Slootweg and Muller, 17 in the current classification system, which categorizes them as tumors that retain features of ameloblastic differentiation and present cytologic features of malignancy regardless of whether there is metastasis or not. The clinical behavior of this tumor is very important for its classification; neoplasms that do not follow these premises should not contain the word ameloblastoma. 10
Malignant forms of ameloblastoma are rare. They have been under discussion for many years and are not included in the veterinary classification. In human medicine, 2 forms are described in the current classification system: 17 the malignant ameloblastoma and the ameloblastic carcinoma. The first is categorized as a tumor that, despite its cytologic benign appearance, metastasizes with well-differentiated lesions and presents no signs of cellular features of malignancy. The ameloblastic carcinoma combines features of ameloblastoma and carcinoma, regardless of metastasis at the time of the diagnosis.
This Alaskan Malamute presented histologic evidence of an ameloblastoma (presence of ameloblastic epithelium spread in a fibrous stroma), but with cellular pleomorphism, high mitotic rate, high cytoplasm/nucleus ratio, and hyperchromatism, which are clear signs of malignancy along with the rapid growth and aggressive invasiveness of the tumor. The positive immunohistochemical labeling to cytokeratin confirmed the epithelial origin of the tumor, although slight differences with human odontogenic tumors of ameloblastomatous epithelial origin were observed. Vimentin expression is restricted to early developing stages of the tooth, but co-expression of cytokeratins with vimentin has been found in human ameloblastomas. 12 An ameloblastic carcinoma described in a horse presented similar labeling to the human pattern 3 ; but in the dog, cytokeratin expression in an ameloblastoma has been reported with vimentin labeling only in the stroma surrounding the canine tumor. 16 The same expression pattern was detected in this dog, where the fibrous stroma around the ameloblastic epithelium in the tumor was strongly positive for vimentin.
In humans, the ameloblastic carcinoma is more aggressive than the ameloblastoma. The age range of appearance is similar to that of the ameloblastoma but has a mean age of 53.5 years. 4 The maxilla is also a rare location for this neoplasm. Metastasis, though rare, usually occurs in the lungs, followed by the cervical lymph nodes, spine, and bone. 2 In this case, the dog was only 3 years old, but the clinical features were similar to those of ameloblastic carcinoma in man. There were no signs of metastasis at the moment of surgical removal.
The tumor was diagnosed based on the histologic characteristics of malignancy. Previously, in biopsy it had been diagnosed as an ameloblastoma; this original diagnosis stresses the importance of a careful and thorough histologic evaluation in order to detect these uncommon malignant forms and reach an accurate diagnosis in veterinary medicine.
This is the second report in veterinary practice presenting signs of ameloblastic carcinoma. It was first reported in a horse, and now in a dog, so it would be interesting to consider these forms for differential diagnoses of masses in the oral cavity in animals. These findings may add important information to the actual classification system, since it does not include this type of odontogenic tumor because it had never before been described.