
Abstract
Protein gene product 9.5 (PGP 9.5), a ubiquitin COOH-terminal hydrolase initially considered specific for neural and neuroendocrine tissues, is expressed in a variety of epithelial and mesenchymal tumors. During immunohistochemical evaluation of a cutaneous epitheliotropic T-cell lymphoma (mycosis fungoides [MF]) in a dog, strong reactivity for PGP 9.5 was observed. This unexpected result prompted us to examine PGP 9.5 immunoreactivity in 13 additional cases of canine mycosis fungoides. All tumors were confirmed as T-cell epitheliotropic lymphoma by histopathology and immunohistochemistry for CD3. Eight of 14 cases were positive for PGP 9.5, with reactivity mainly in the cytoplasm and less commonly in the nucleus. One case had strong reactivity in the cell membrane, sometimes with concurrent paranuclear staining. Immunoreactivity did not correlate with location (epidermal, dermal, and adnexal) of tumor cells. Disease outcome did not vary between PGP 9.5-positive and negative tumors. Although PGP 9.5 immunoreactivity in MF did not predict tumor behavior in these dogs, it has had prognostic value in certain human carcinomas. This unexpected staining of lymphocytes in mycosis fungoides with an antibody to PGP 9.5 demonstrates its presence in nonneuroendocrine tumors and precludes its use as the sole diagnostic marker in discrete cell tumors in the skin.
Protein gene product (PGP 9.5) is a 27-kDa protein originally isolated from the brain. 15 A ubiquitin COOH-terminal hydrolase, PGP 9.5 forms part of the ubiquitin-proteasome system, a nonlysosomal proteolytic pathway involved in the regulation of cell growth, modulation of some membrane receptors, and turnover of cytoskeletal elements. 12, 20, 33 Ubiquitin COOH-terminal hydrolases separate ubiquitin from its substrate during protein degradation in the proteasome, regulating protein catabolism. 12 The ubiquitin-proteasome pathway is involved in cancer-related deregulation. 28 PGP 9.5 expression has been implicated in tumor progression in non-small-cell lung cancer 13, 24 and unfavorable outcome in pancreatic cancer. 29 PGP 9.5 was initially considered to be confined to neurons and neuroendocrine cells. 30 However, later studies detected PGP 9.5 in cells of the male genital system (epididymis, ejaculatory duct cells, spermatogonia, Leydig cells, prostatic secretory epithelium), female genital system (mammary epithelial cells, oocytes), skin (melanocytes, Langerhan's cells, Merkel cells, fibroblasts), and renal epithelial cells. 2, 5, 7, 10, 14, 18, 19, 25, 26, 34 PGP 9.5 has also been detected in lymphocytes of germinal centers, occasional lymphocytes of interfollicular regions 16 and thymic epithelial cells. 3 Antibodies to PGP 9.5 are commonly used to characterize tumors of nervous (neuroblastoma, peripheral primitive neuroectodermal tumor, Ewing's sarcoma, malignant peripheral nerve sheath tumor, perineuroma, and neurofibroma) and neuroendocrine systems (melanoma, carcinoid, paraganglioma, and pheochromocytoma). 4, 11, 22, 32 The sensitivity of PGP 9.5 for neural or neuroendocrine tumors is higher or similar to that of neuron-specific enolase or synaptophysin. 11, 22 However, PGP 9.5 is no longer considered specific for neuronal or neuroendocrine tumors because it has been immunohistochemically detected in unrelated tumor types, particularly of mesenchymal origin 4 and in several types of lymphoma. 17, 27, 32
Canine cutaneous epitheliotropic lymphoma (mycosis fungoides [MF]) is a T-cell lymphoma that shares many histologic features with its human counterpart. In dogs, MF pursues a progressive course of disease with several months to 2 years before death. MF neoplastic lymphocytes in humans and dogs are CD3-positive, 9, 23 but canine neoplastic T cells are CD8-positive as opposed to CD4-positive in humans, except in some cases with aberrant expression of CD8. 8, 9, 23 Although the presence of cerebroid cells is characteristic of MF in humans and animals, other lymphomas and some lymphocytes in dermatitis have similar nuclear features. 23 In dogs, the differential diagnosis for MF includes histiocytoma, round cell amelanotic melanoma, and Merkel cell tumor. 9 During a routine diagnostic work-up of a cutaneous round cell tumor in a dog, we found strong positivity for PGP 9.5 in a tumor with some features of endocrine differentiation (e.g., packeting, high cellularity) but no reaction to other neuroendocrine markers and strong reaction to leukocytic markers, including CD3, confirming a diagnosis of mycosis fungoides. Because of this unexpected PGP 9.5 staining we decided to examine a group of cutaneous lymphomas (MF) to determine the degree of reactivity of an antibody to PGP 9.5 in neoplastic lymphocytes.
Methods
Fourteen cases of canine MF in the archives of the Animal Disease Diagnostic Laboratory-Purdue University diagnosed by histopathology and immunohistochemistry were selected in this study. Only excisional biopsies were examined. Slides and records were reviewed, and follow-up information obtained.
Surgical biopsies were fixed in neutral buffered formalin and embedded in paraffin. Four-micrometer-thick tissue sections were stained with HE. Immunohistochemical staining was done in an automatic stainer following previously reported protocols. 21 The antibodies used were rabbit polyclonal antibody to CD3 (A0452, Dako, Carpinteria, CA), mouse monoclonal antibody to canine CD18 (CA 16.3C10, Dr. Moore, University of California-Davis), mouse monoclonal antibody to canine CD45 (CA12.10C12, Dr. Moore), mouse monoclonal antibody to CD79a (M7051, Dako), mouse monoclonal antibody to cytokeratins AE1/AE3 (M3515, Dako), mouse monoclonal antibody to Melan A (M7196, Dako), rabbit polyclonal antibody to PGP 9.5 (Z5116, Dako), rabbit polyclonal antibody to S100 (Z0311, Dako), and rabbit monoclonal antibody to synaptophysin (RM-9111, LabVision, Fremont, CA). Immunohistochemical staining for CD3, CD79a, and PGP 9.5 was done in all cases. Additional antibodies were used in individual cases to confirm leukocytic origin and to rule out other tumor types (e.g., melanoma, neuroendocrine carcinoma). There are no antibodies available to canine CD4 or CD8 reactive in formalin-fixed, paraffin-embedded tissues. Antigen retrieval was used as follows: pressure cooker with citrate buffer, pH 6.0 (CD3, CD45, CD18, cytokeratins, and S100); pressure cooker with EDTA buffer, pH 9.0 (CD79a, Melan A). Antibodies to PGP 9.5 and synaptophysin did not need antigen retrieval. The peroxidase-based detection systems used were LSAB2 (CD3, S100), LSAB+ (CD45, cytokeratins, synaptophysin), and ENVISION+ (CD18, CD79a, Melan A, PGP 9.5), all from Dako. Slides were counterstained with Mayer's hematoxylin. Immunoreactivity for PGP 9.5 was scored from 0 to 3 depending on the number of positive neoplastic cells: 3, >75% positive cells; 2, 30 to 74% positive cells; 1, 10 to 29% positive cells; 0, <10% positive cells. Location of the PGP 9.5 was recorded as cytoplasmic membrane, cytoplasmic, paranuclear, or nuclear reaction. To determine the specificity of the reaction, the primary antibody was replaced with commercially available negative control reagent containing rabbit immunoglobulins (Dako, N1699) for polyclonal antibodies or mouse immunoglobulins (Dako, N1698) for monoclonal antibodies. Positive controls for each antibody (e.g., normal canine lymph node for leukocytic markers and normal canine adrenal gland for PGP 9.5) were also included.
Results
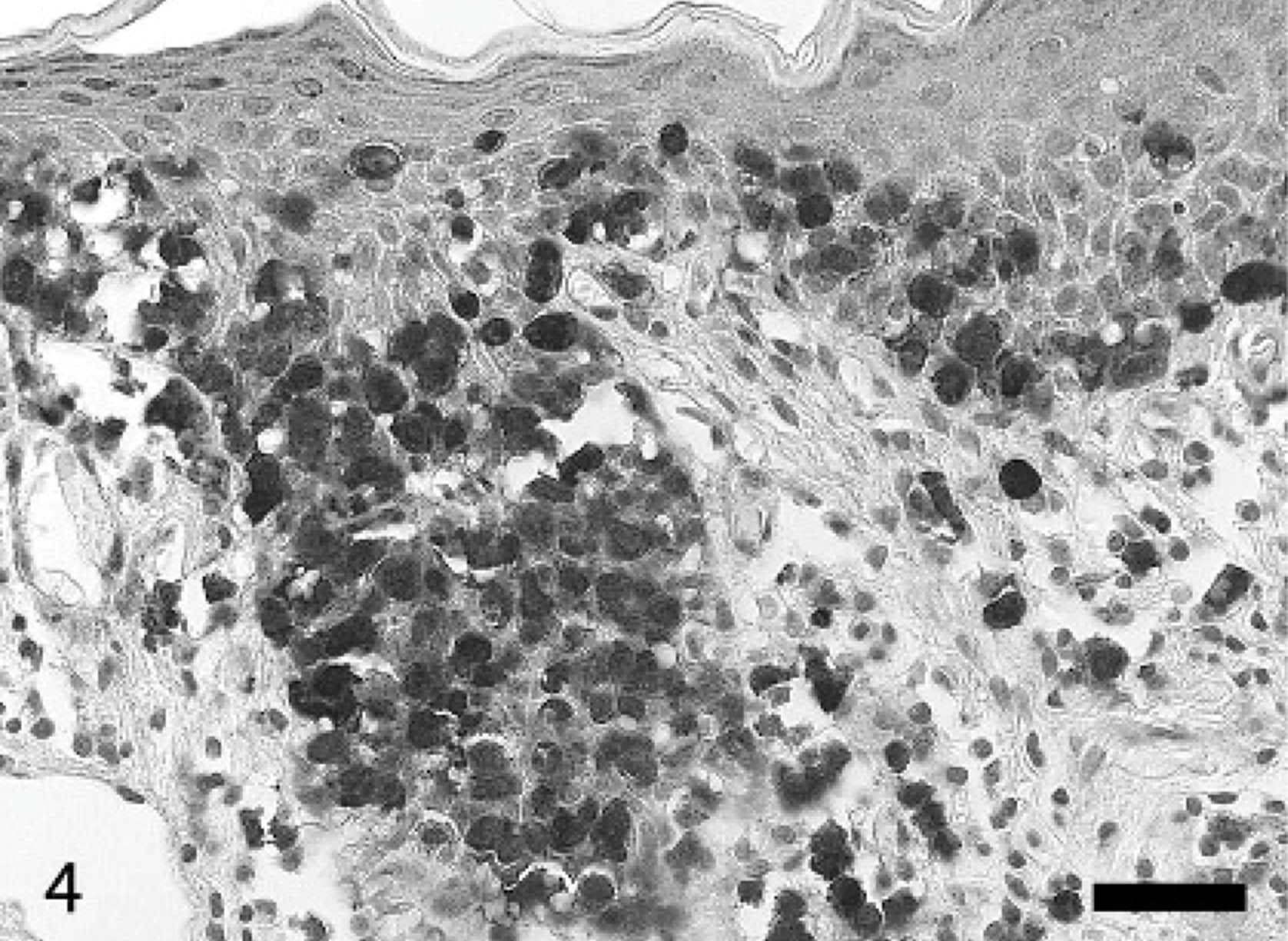
Clinical data are summarized in Table 1. The age of the dogs ranged from 1.5 to 14 years (8.5 years on average). Eight dogs were male and six were female. A variety of medium-sized or small breeds were represented. The lesions were located in multiple cutaneous sites (8 cases), solitary (2 cases), and the lips or oral cavity (4 cases). One animal had only oral lesions. Lesions consisted of masses (10 cases), patches, plaques, ulcers, or pustules (1 case each). In only 2 cases was there a clinical diagnosis of MF with the rest considered to be dermatitis, sebaceous adenitis, or other tumors. The time between the onset of clinical signs and the biopsy ranged from 1 week to 6 months. Only 1 animal remained alive 7 months after diagnosis. The other animals were euthanized because of disease progression or died of undetermined causes 1 week to 1 year after the diagnosis. Four animals were lost to follow-up. Three animals were treated with chemotherapy. Twelve cases had the classical tumor stage form of MF with neoplastic cells infiltrating the epidermis, dermis, and subcutis (Fig. 1). 9 The other 2 dogs had the pagetoid reticulosis form characterized by neoplastic lymphocytes confined to the epidermis and adnexal structures. 9 One case had several lesions in the tumor stage and 1 lesion consistent with pagetoid reticulosis. In all cases more than 90% of neoplastic lymphocytes were reactive with antibody to CD3, highlighting their intraepithelial and intrafollicular location (Fig. 2). None of these cases reacted with antibody to CD79a. PGP 9.5 immunoreactivity on the neoplastic cells was present in 8 cases (57%), being strong in 5 cases, weak in 3 cases, and not detected in 6 cases. PGP 9.5 antigen was usually diffuse in the cytoplasm with fewer cells having strong nuclear staining (Figs. 3–6). In only 1 dog (case No. 12) was staining distinctly in the cell membrane with the cytoplasm less intensely stained. Paranuclear staining was also seen in several areas in this case, sometimes combined with cell membrane and cytoplasmic stain. Nuclear stain was not seen in this case (Figs. 7–8). PGP 9.5 staining was observed at all levels of the neoplastic growth (intraepidermal/intramucosal, intrafollicular, dermal/submucosal) although the intensity of the reaction sometimes varied within a tumor. We did not observe significant differences in the outcome between positive and negative tumors to PGP 9.5 in our series.
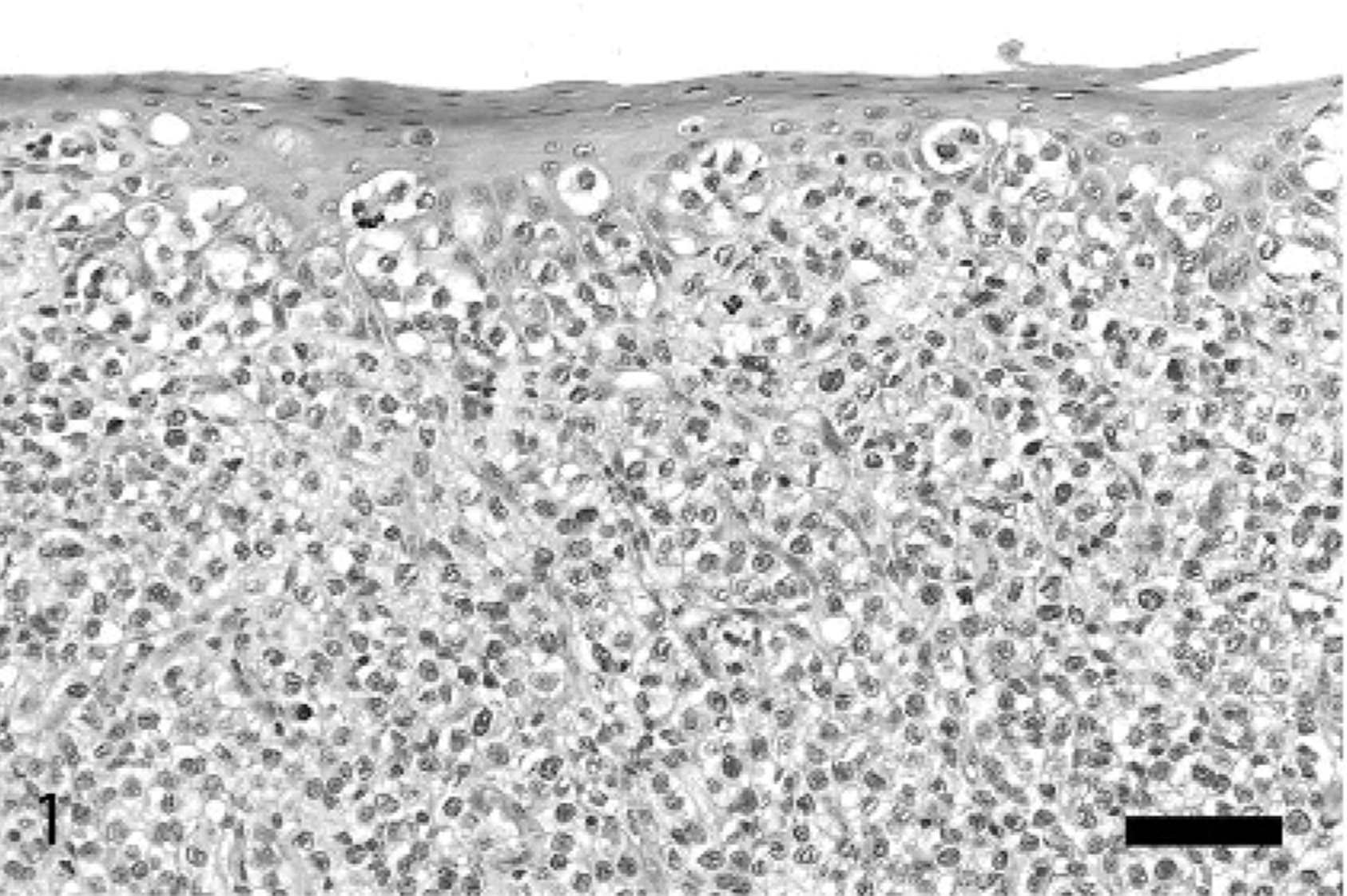
Skin; dog, case No. 8. Epitheliotropic lymphoma. Neoplastic cells infiltrate the epidermis. HE. Bar = 100 μm.
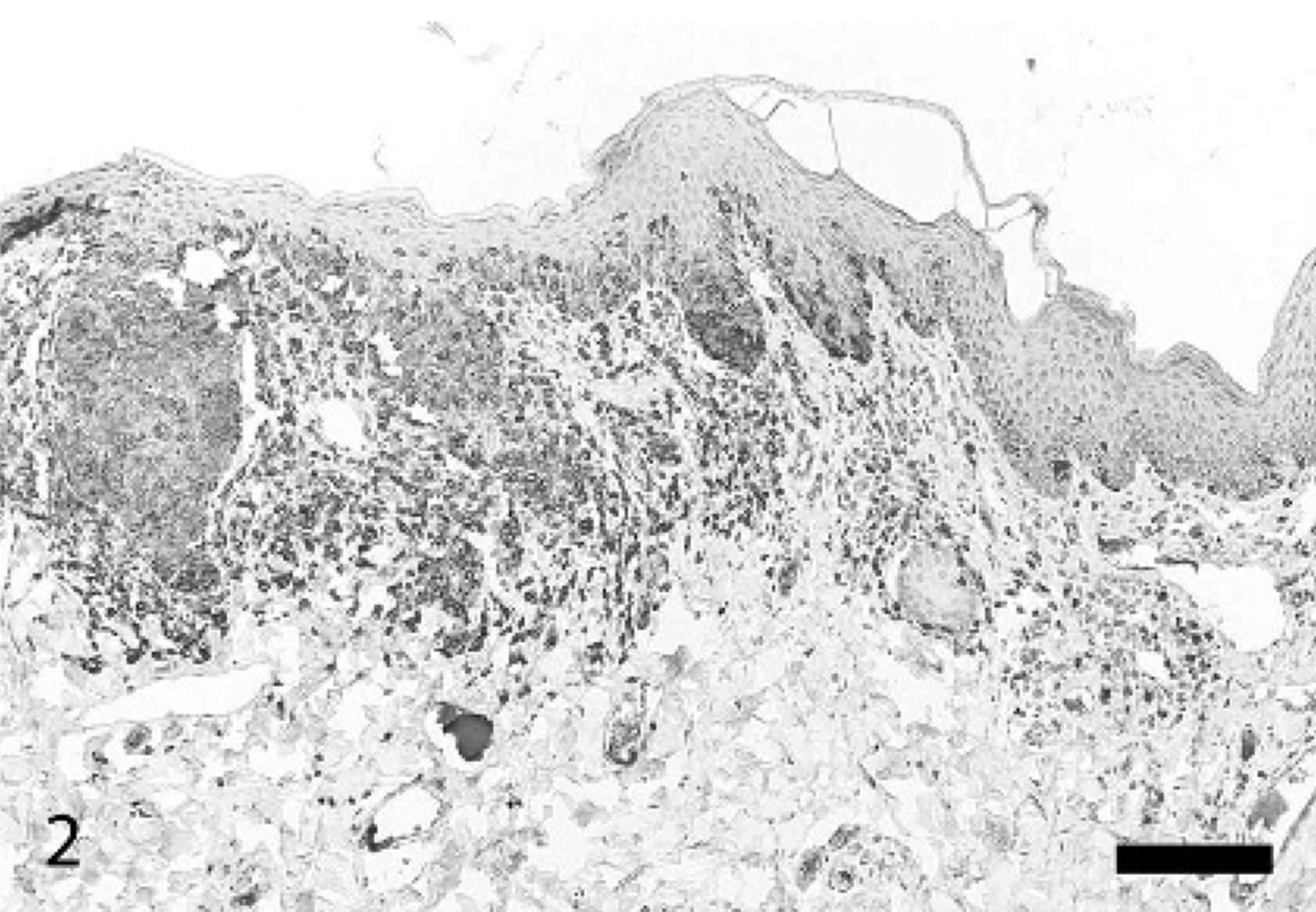
Skin; dog, case No. 8. Epitheliotropic lymphoma. Strong reactivity for CD3 in the epidermis and dermis. LSAB2-peroxidase immunohistochemistry for CD3, Mayer's hematoxylin counterstain. Bar = 200 μm.
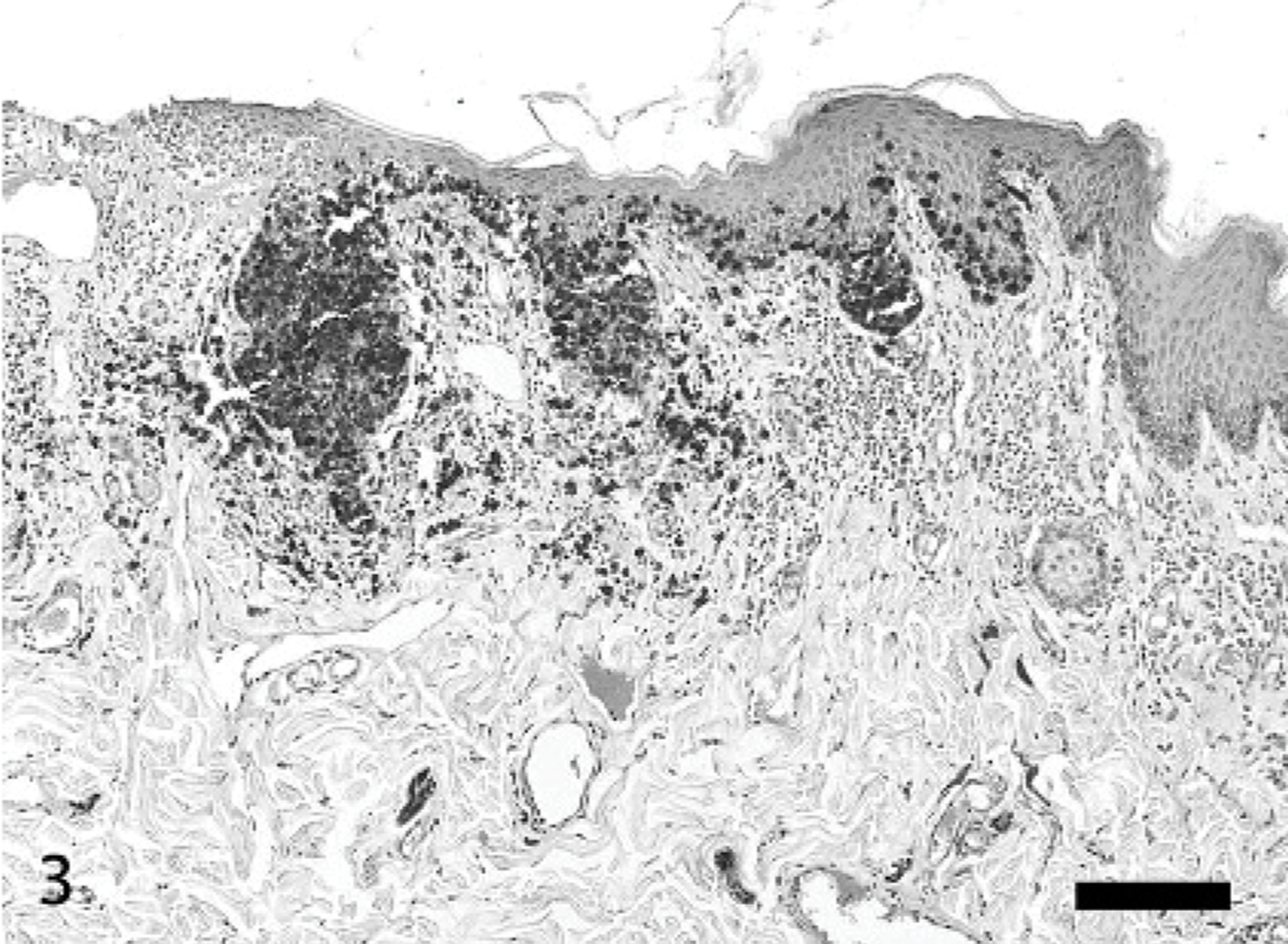
Skin; dog, case No. 8. Epitheliotropic lymphoma. The pattern of staining for PGP 9.5 is similar to that for CD3. ENVISION+-peroxidase immunohistochemistry for PGP 9.5, Mayer's hematoxylin counterstain. Bar = 200 μm.
Skin; dog, case No. 8. Epitheliotropic lymphoma. Numerous intraepithelial lymphocytes are positive for PGP 9.5. ENVISION+-peroxidase immunohistochemistry for PGP 9.5, Mayer's hematoxylin counterstain. Bar = 50 μm.
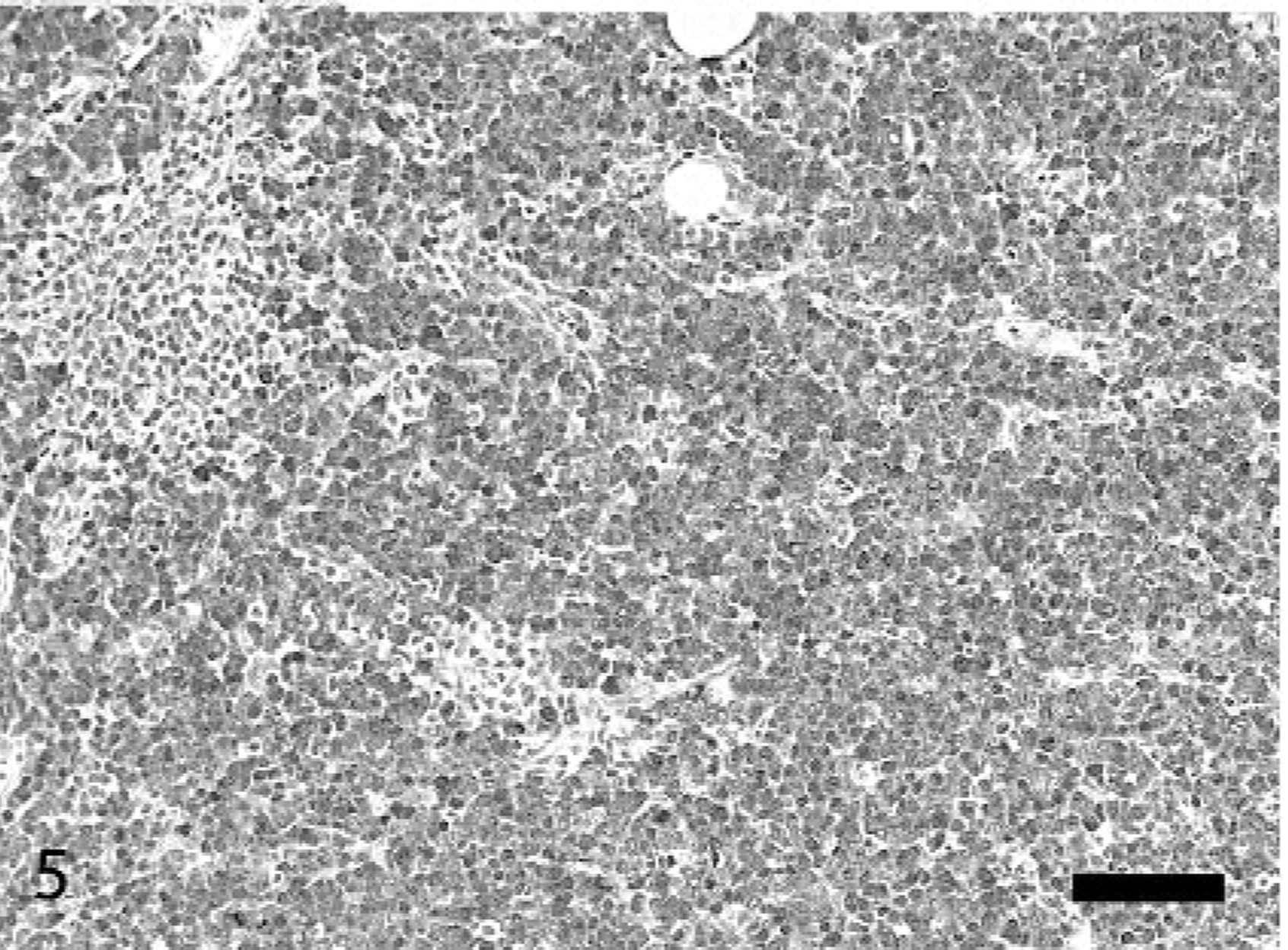
Skin; dog, case No. 3. Epitheliotropic lymphoma. A dermal lymphoid infiltrate is diffusely positive for PGP 9.5. ENVISION+-peroxidase immunohistochemistry for PGP 9.5, Mayer's hematoxylin counterstain. Bar = 100 μm.
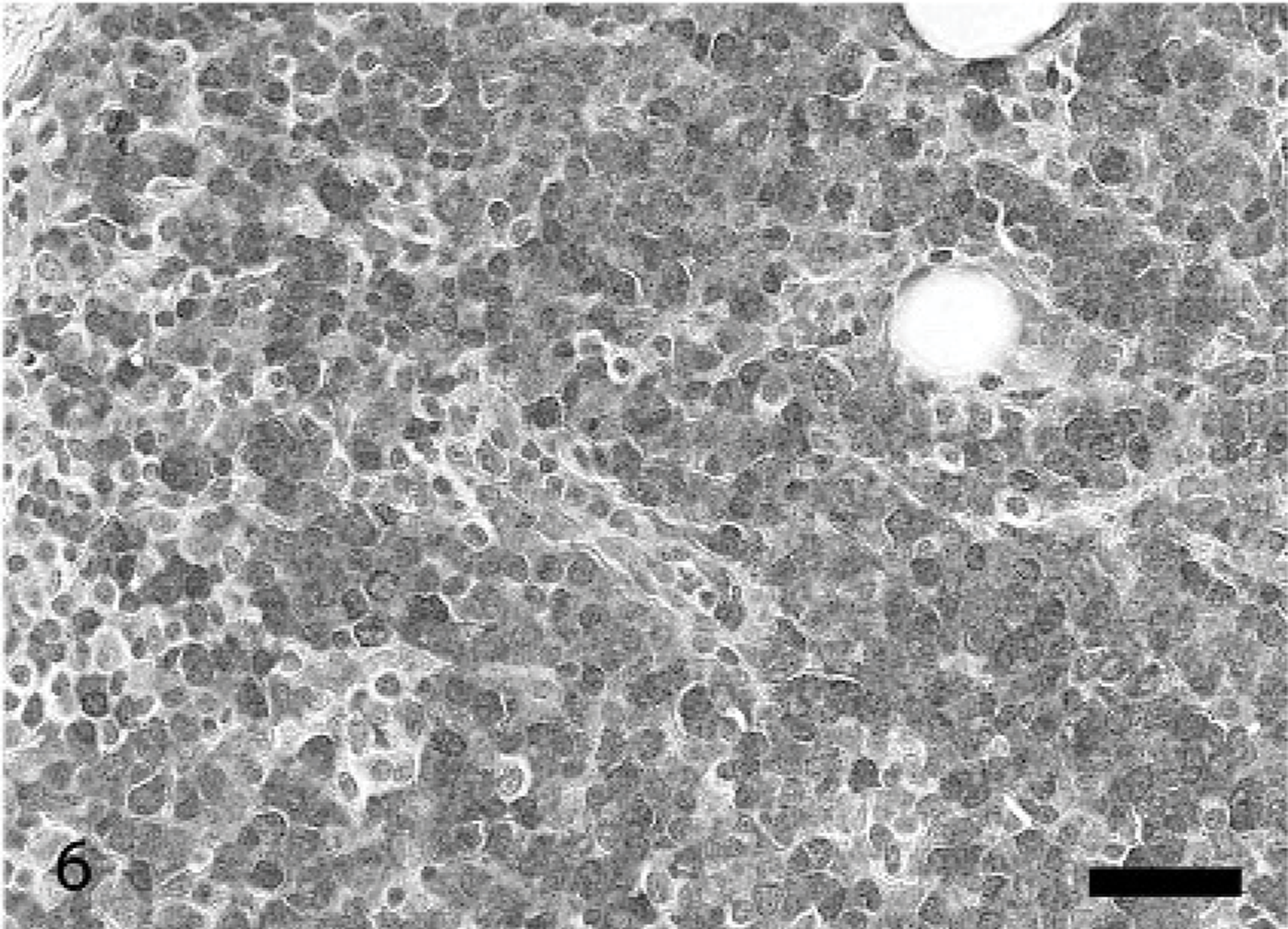
Skin; dog, case No. 5. Epitheliotropic lymphoma. Strong nuclear and cytoplasmic immunoreactivity. ENVISION+-peroxidase immunohistochemistry for PGP 9.5, Mayer's hematoxylin counterstain. Bar = 50 μm.
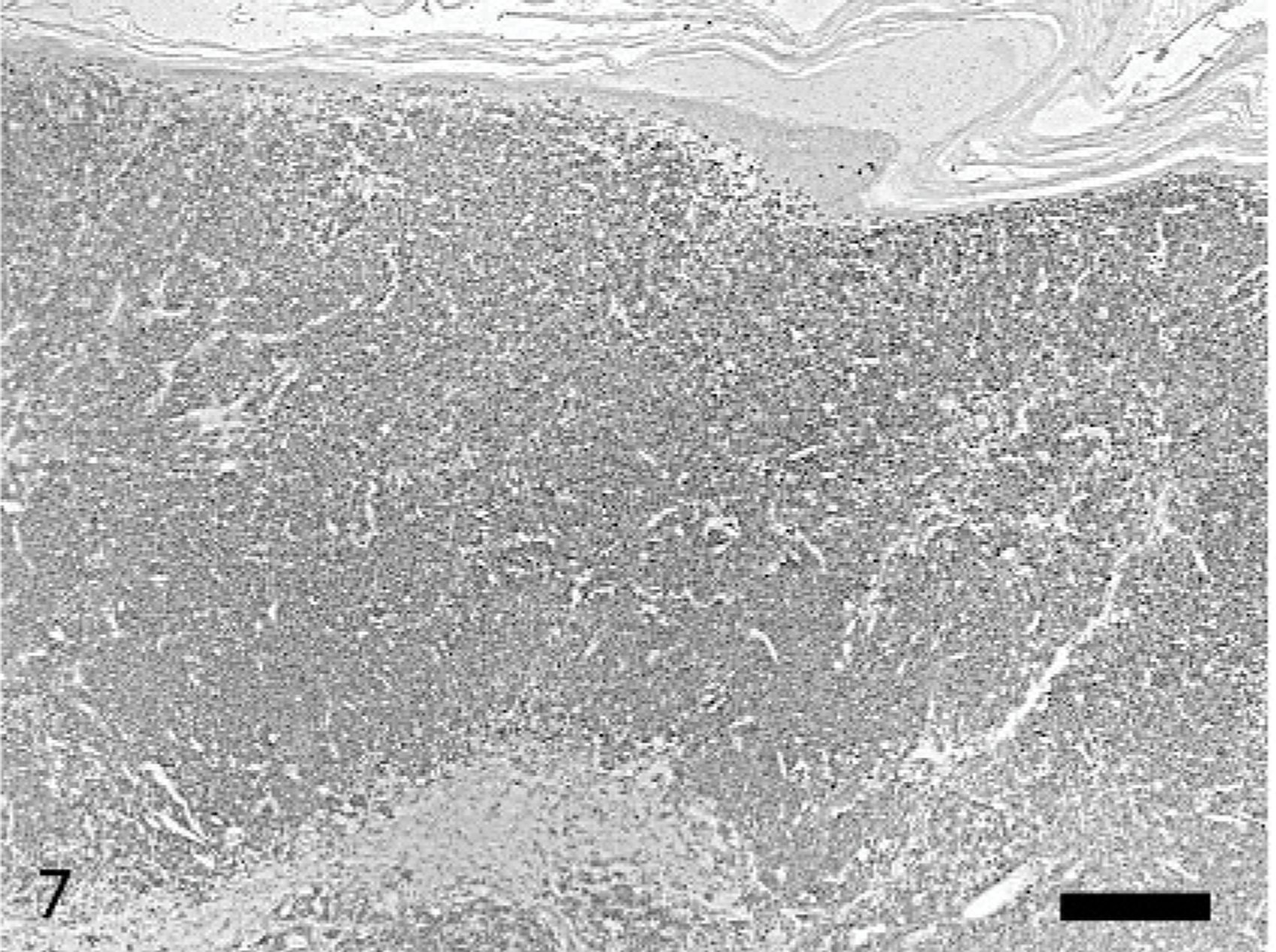
Skin; dog, case No. 12. Epitheliotropic lymphoma. Infiltrating lymphocytes in the epidermis and dermis have PGP 9.5 immunoreactivity. ENVISION+-peroxidase immunohistochemistry for PGP 9.5, Mayer's hematoxylin counterstain. Bar = 200 μm.
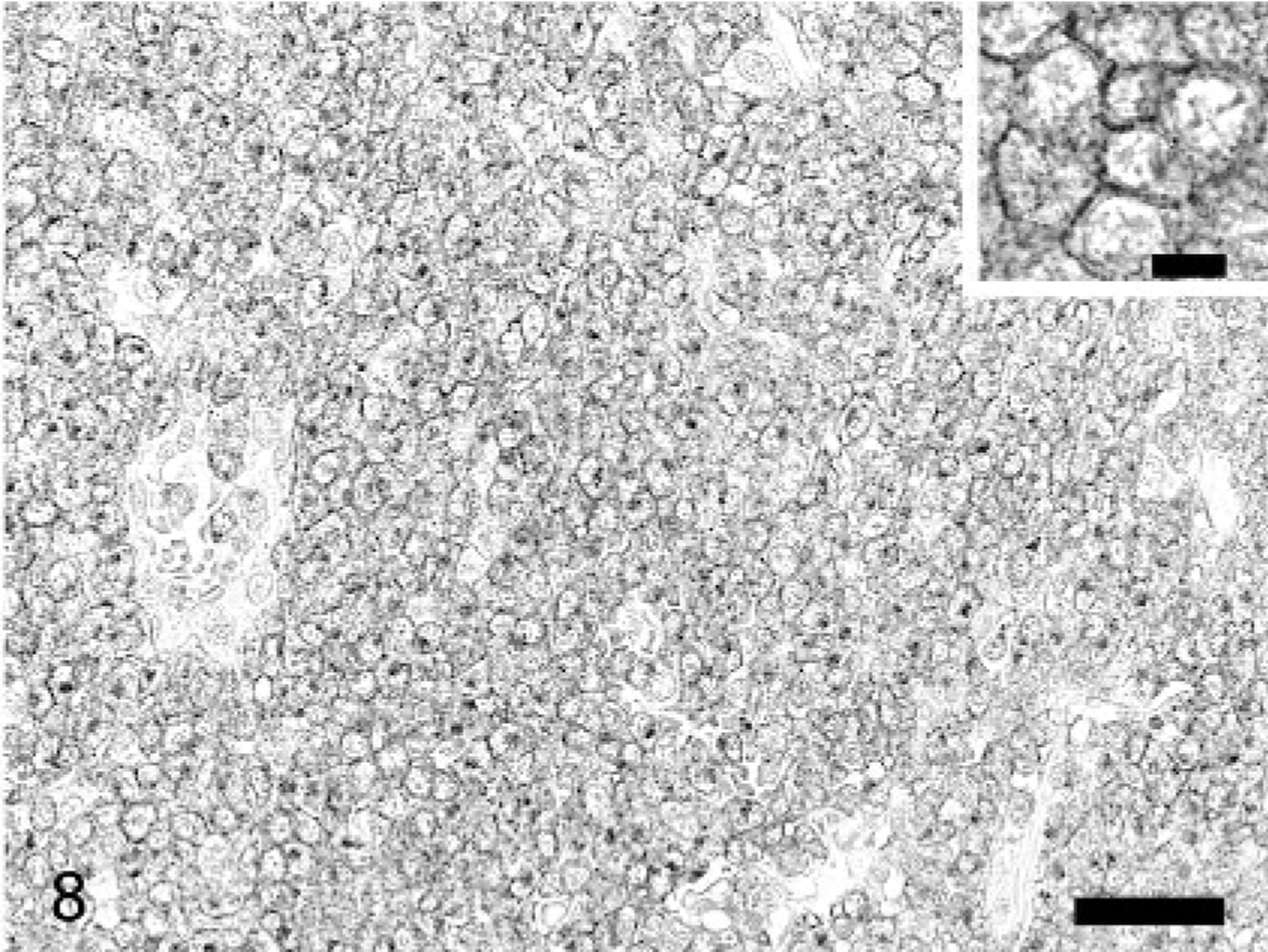
Skin; dog, case No. 12. Epitheliotropic lymphoma. Distinct cell membrane staining in most cells. Many cells also have paranuclear staining. ENVISION+-peroxidase immunohistochemistry for PGP 9.5, Mayer's hematoxylin counterstain. Bar = 50 μm. Inset: Detail of membrane staining. Bar = 10 μm.
Summary of clinical data, histologic type, PGP 9.5 staining, and outcome in 14 dogs.
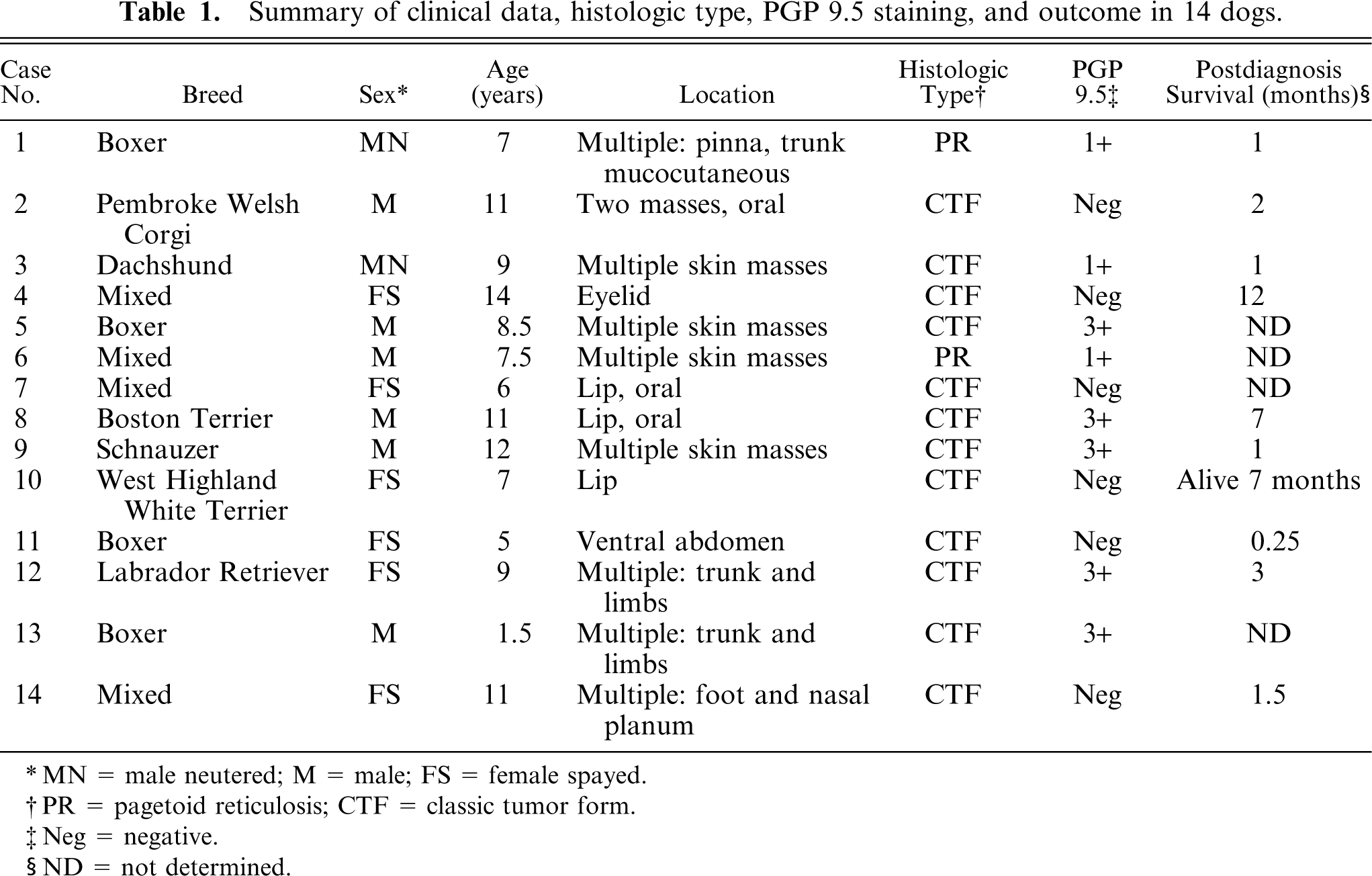
MN = male neutered; M = male; FS = female spayed.
PR = pagetoid reticulosis; CTF = classic tumor form.
Neg = negative.
ND = not determined.
Discussion
MF is an uncommon cutaneous disease of dogs. 9 Oral involvement is even less common and rarely reported. 1 However, 1 of the 14 cases in our series had only oral involvement. Human MF with primary oral involvement or secondary to cutaneous disease is also uncommon. 6, 31 To our knowledge, there are no reports examining PGP 9.5 immunoreactivity in epitheliotropic T-cell lymphomas. Some researchers have detected PGP 9.5 in lymphocytes and their tumors, 16, 17, 27, 32 with only one group observing PGP 9.5 immunoreactivity in T-cell lymphomas. 17 In one study, PGP 9.5 was detected in most (98%) mantle cell lymphomas with fewer cases (58%) and weaker reactivity in B-small lymphocytic lymphoma. 27 In another study PGP 9.5 was detected in centrocytic lymphoma, lymphoblastic lymphoma, immunoblastic lymphoma, and pleomorphic large T-cell lymphomas. 17 PGP 9.5 has also been reported in anaplastic large cell lymphoma. 32 It is interesting that some authors report PGP 9.5 immunoreactivity in lymphocytes and their tumors only after heat-induced epitope retrieval (HIER). 16, 17 In our case we did not use antigen retrieval because during standardization of the procedure following a published protocol 21 we observed more background with HIER than with no antigen retrieval at all; enzymatic retrieval did not demonstrate any reactivity. This disparity may reflect use of different PGP 9.5 polyclonal antibodies in those studies. 16, 17, 27 The cause of immunoreactivity of PGP 9.5 in MF or other nonneuroendocrine tumors is unknown. Two possible explanations have been given: 1) cross-reactivity of the antibody with epitopes in other ubiquitin hydrolases, or 2) abnormal upregulation of PGP 9.5 in mesenchymal and lymphoid neoplasms. 4
The clinical significance of our findings is undetermined. Immunohistochemical staining with PGP 9.5 has been used to predict tumor progression in human lung cancer 13, 24 and the outcome in pancreatic cancer. 29 However, PGP 9.5 immunoreactivity was not associated with type or grade of human lymphoma. 17 MF in dogs is usually fatal with little improvement in the outcome regardless of the chemotherapy protocol. 9 Our results are in line with multiple reports in humans indicating the wide range of cell types and tumors that may express PGP 9.5 2, 4, 5, 7, 10, 14, 17– 19, 25– 27, 32, 34 despite the early claims that PGP 9.5 was a specific marker of neural and neuroendocrine tissues. 30 This unexpected staining of MF with an antibody to PGP 9.5 highlights the need of a wide variety of cell markers to characterize some cases of discrete cell tumors (e.g., leukocytic, endocrine, melanocytic) in the skin. Further validation studies are needed to determine the expression of PGP 9.5 in canine nonendocrine tumors. Because MF in humans and dogs share many similarities it is expected that some human epitheliotropic lymphomas will show reactivity to PGP 9.5.
Footnotes
Acknowledgements
We appreciate the technical expertise of Dee DuSold in performing immunohistochemistry and Drs. A. Abbo, D. Bevier, S. Borter, G. Boyd, E. Greene, M. Hohenstein, P. Jackson, J. Lortie, L. Mehringer, D. Morgan, R. Rudolph, D. Turmail, and A. Zwingleberg for submitting the biopsy specimens and providing follow-up information.