
Abstract
AL amyloidosis is the most common type of systemic amyloidosis in humans, and it is frequently associated with multiple myeloma. But, AL amyloidosis is very rare in domestic animals. A 16-year-old Quarter horse gelding was diagnosed with systemic AL amyloidosis associated with multiple myeloma. Clinical problems were rapid weight loss, muscle atrophy, soft unformed stool, and ventral edema. Grossly, diffuse gastrointestinal hemorrhage, markedly thickened jejunal mucosa, and splenomegaly were present. Microscopically, diffuse severe amyloid deposits were present in the lamina propria of glandular stomach, duodenum, and jejunum. Much of the spleen and sternal bone marrow was replaced by neoplastic round cells, and multiple foci of amyloid were also present in the spleen and bone marrow. Electron microscopy revealed the neoplastic round cells to be of plasma cell origin, and the amyloid showed a strongly positive immunoreactivity with polyclonal anti-human immunoglobin lambda light-chain antisera. To our knowledge, this is the second report describing systemic AL amyloidosis in domestic animals-associated plasma cell neoplasia and the first associated with multiple myeloma, as is common in humans.
Amyloid is a compound of insoluble, toxic protein aggregates that are systemically or locally deposited in tissues in bundles of β-sheet fibrillar protein. There are two major forms of systemic amyloidosis. The most common form in domestic animals is reactive (secondary) amyloidosis due to chronic inflammatory diseases. In reactive amyloidosis, the deposited amyloid protein is AA type that is derived from serum amyloid A synthesized in the liver. The other form of systemic amyloidosis is light-chain (AL) amyloidosis, which is the most common type in human beings but very rare in domestic animals. One of the common underlying causes of human AL amyloidosis is multiple myeloma, which accounts for 12% to 15% of the cases. 14 Systemic AL amyloidosis has been only reported in a mare 5 and in a cow, in which it was associated with bovine leukocyte adhesion deficiency. 16 Here, we describe a case of systemic AL amyloidosis associated with multiple myeloma in a horse.
A 16-year-old Quarter horse gelding presented to the Louisiana State University Veterinary Teaching Hospital Equine Clinic with a clinical history of rapid weight loss for a month despite a good appetite, severe muscular atrophy, soft unformed stool for 3 weeks, and ventral edema. The gelding was current on all vaccines and was dewormed 3 weeks before presentation. Hematologic abnormalities included severe anemia (packed cell volume was 9%) with increased mean corpuscular volume (71.1 fl; reference range [ref], 34–58) and increased mean corpuscular hemoglobin concentration (MCHC) (36.4 g/dl; ref, 30–35), thrombocytopenia (55,000/µl; ref, 100,000–600,000) with few clumps, leukocytosis (20,100/µl; ref, 5,500–12,500), neutrophilia (17,600/µl; ref, 2,700–6,700) with left shift and toxic changes (cytoplasmic basophilia and Dohle Bodies), and lymphopenia (1,000/µl; ref, 1,500–5,500). The abnormal serum biochemical values included hyperglycemia (135 mg/dl; ref, 70–105), hypocalcemia (10.6 mg/dl; ref, 11.3–13.4), hypoproteinemia (4.1 g/dl; ref, 6.1–8.1), hypoalbuminemia (2.1 g/dl; ref. 3.0–4.1), and hypoglobulinemia (2.1 g/dl; ref, 2.5–5.0). Abdominal ultrasound revealed multiple hypoechoic foci in the spleen. Because of a possible splenic tumor, the owner elected euthanasia.
At necropsy, there was hemorrhagic ingesta throughout the stomach, duodenum, and the jejunum. The proximal half of jejunal mucosa was markedly thickened with prominent rugae (Fig. 1). The spleen was enlarged and homogeneously red and firm with no recognizable lymphoid follicle; no tumor was observed.
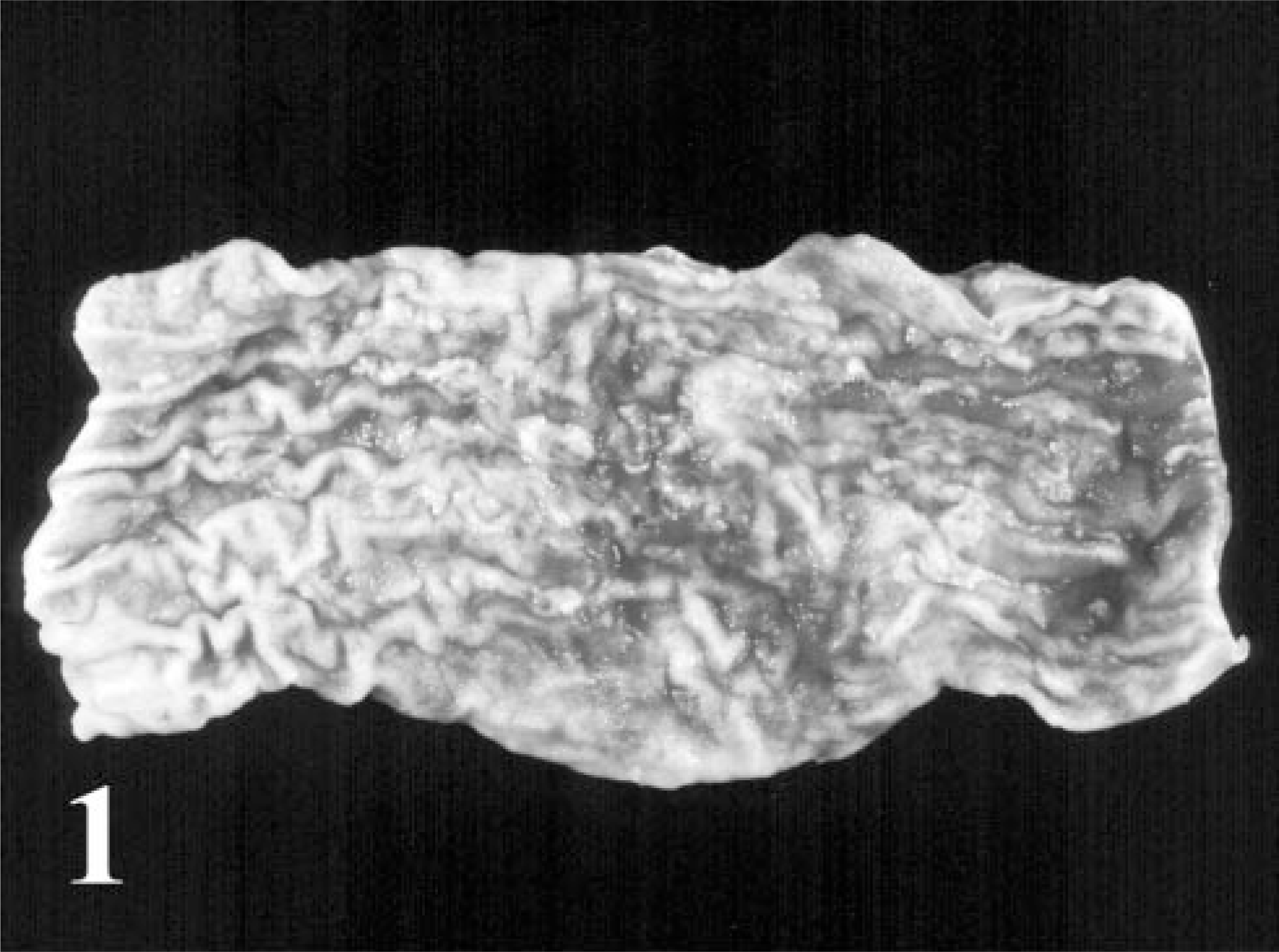
Jejunum; horse with multiple myeloma. The jejunal mucosa is hemorrhagic and markedly thickened with prominent rugae.
Microscopically, much of the spleen and bone marrow from the sternebrae were replaced by a homogenous population of neoplastic round cells in solid cellular sheets. The tumor cells had hyperchromatic, sometimes eccentrically located nuclei and moderate to abundant eosinophilic cytoplasm with distinct cellular outlines (Fig. 2). Mitotic figures were rare, with 0–1 present per 10 high power fields. Mega-karyocytes, myeloid and erythroid precursor cells were occasionally noted among the neoplastic cells. In the bone marrow, trabecular bone was sparse and the remaining bone was atrophic and necrotic. There were multifocal extracellular deposits of eosinophilic amorphous proteinaceous material that was occasionally surrounded by macrophages in the spleen and bone marrow. Diffusely in the glandular stomach and small intestine, the lamina proparia was severely expanded with the same proteinaceous materials, infiltration of macrophages, and lesser numbers of lymphocytes and neutrophils. There was loss of gastric glands and intestinal crypts (Fig. 3). Villous blunting and fusion, epithelial necrosis, and multifocal hemorrhage were evident in the small intestine. No significant microscopic changes were noted in the kidneys, liver, and lungs.
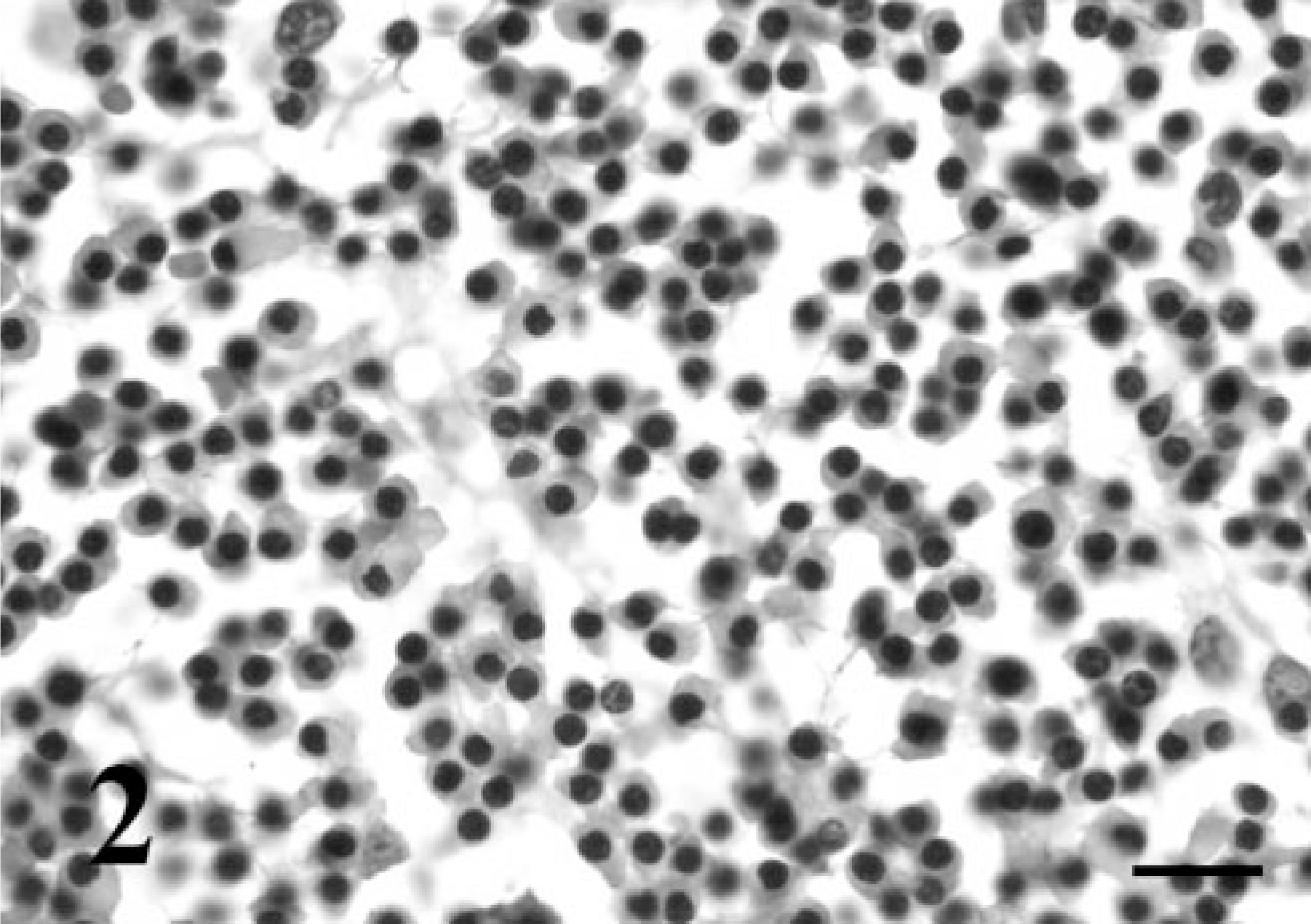
Bone marrow; horse with multiple myeloma. The bone marrow contains a homogeneous population of neoplastic plasma cells that often have hyperchromatic eccentric nuclei. HE. Bar = 15 µm.
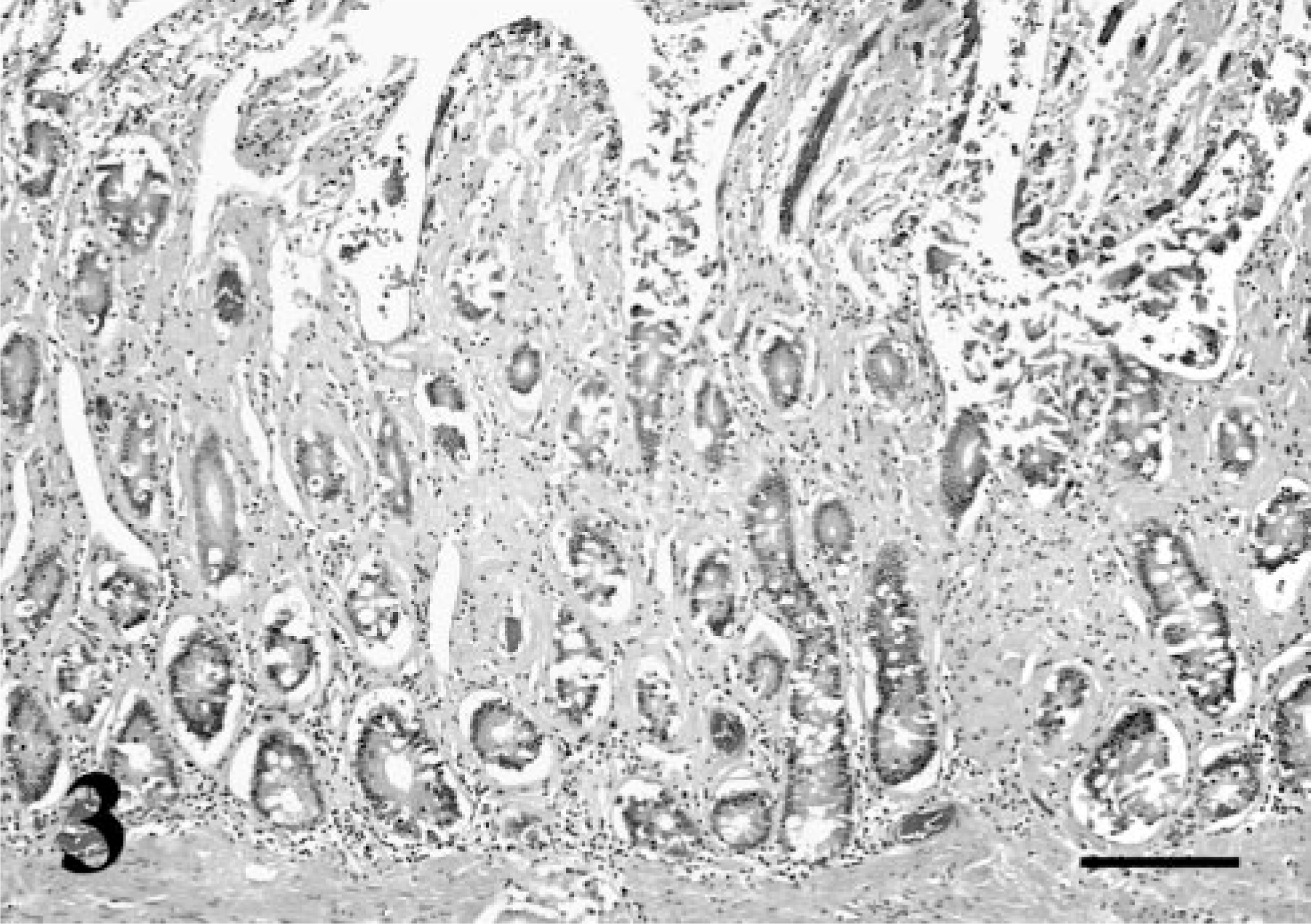
Jejunum; horse with multiple myeloma. The lamina propria is severely expanded with homogeneous amorphous proteinaceous material (amyloid). The intestinal mucosa is attenuated with blunted villi and irregular loss of crypts. HE. Bar = 200 µm.
For transmission electron microscopy, formalin-fixed spleen and bone marrow were postfixed in osmium tetroxide, embedded in epoxy resin (EMbed 812®, Electron Microscopy Sciences, Hatfield, PA), sectioned with an ultramicrotome, and stained with uranyl acetate and lead citrate. Electron microscopy revealed the tumor cells to be neoplastic plasma cells characterized by a cartwheel-like nucleus and a cytoplasm filled with dilated rough endoplasmic reticulum (Fig. 4).
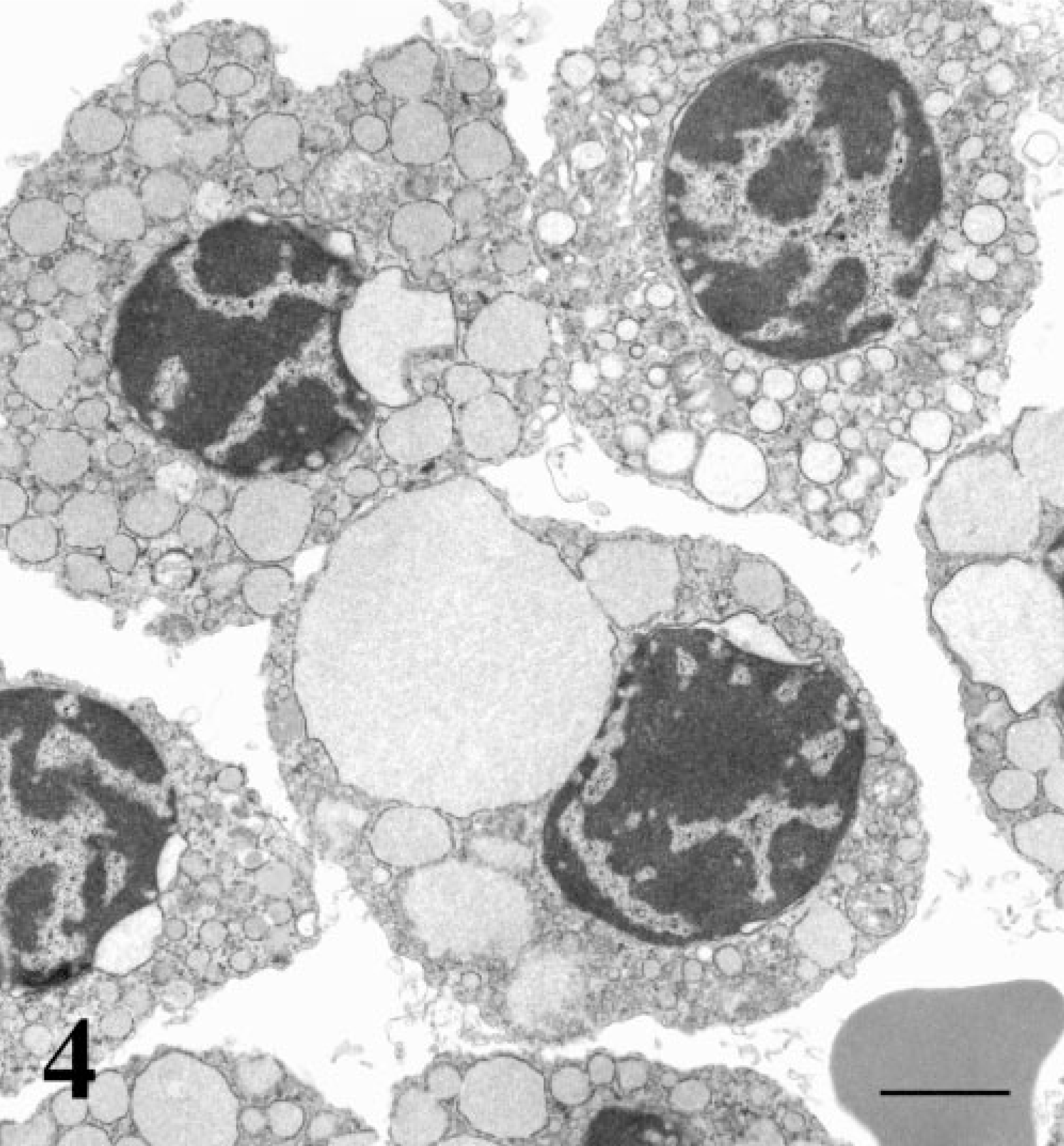
Bone marrow; horse with multiple myeloma. Note the characteristic features of cartwheel-like nucleus and the cytoplasm filled with dilated rough endoplasmic reticulum. Uranyl acetate and lead citrate. Bar = 1 µm.
In the sections stained with Congo red either with or without pretreatment of 5% potassium permanganate solution for 5 minutes, the proteinaceous material in the spleen, bone marrow, stomach, and small intestine displayed characteristic apple-green birefringence under polarized light, identifying it as primary (AL) amyloid. In addition, immunohistochemistry with rabbit anti-human immunoglobin lambda light-chain polyclonal antisera (DakoCytomation, Carpinteria, CA) was performed on the amyloid and revealed strongly positive immunoreactivity, supporting the fact that the amyloids deposited in the multiple organs were AL amyloids expected with multiple myeloma (Fig. 5). Immunohistochemistry with rabbit anti-human AA protein polyclonal antibody (DakoCytomation) was negative for the amyloid. Reactions without primary antisera or with nonimmune rabbit sera were carried out as negative controls. The slides contained AL amyloid associated with extramedullary plasmacytoma in a dog, and AA amyloid in renal amyloidosis in a dog served as the positive control.
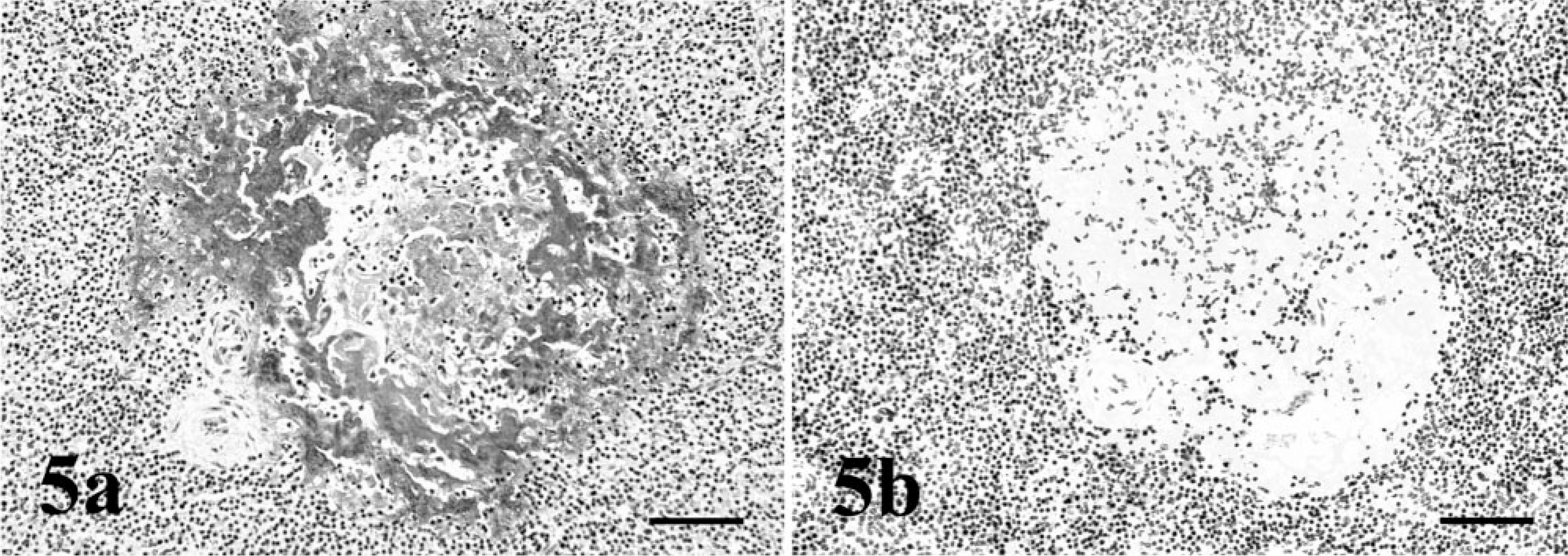
Spleen; horse with multiple myeloma. The deposited amyloid shows strong immunopositivity with anti-human immunoglobin lambda light-chain antisera.
Multiple myeloma is a rare malignant neoplasm of plasma cells (B cells) in bone marrow of multiple locations and in other organs such as lymph node, kidney, spleen, liver. 3 , 9 Multiple myeloma has been reported in horses. 2 , 3 , 7 , 12 , 13 The characteristic serum biochemical changes of multiple myeloma are monoclonal gammopathy (with hyperproteinemia, hypoalbuminemia, and hyperglobulinemia) and Bence Jones proteinuria. Occasionally renal azotemia, hypercalcemia due to osteolysis, and hypocholesterolemia can be seen, 3 but, in this case, the horse had hypoproteinemia, hypoalbuminemia, hypoglobulinemia, and hypocalcemia. Severe malabsorption (protein-losing enteropathy) and gastrointestinal (GI) bleeding (loss of vascular integrity) due to the diffuse severe GI amyloidosis most likely contributed to the unusual serum biochemical changes in this multiple myeloma case. Because multiple myeloma was not a differential diagnosis, due to the serum protein profiles, serum electrophoresis was not performed. Also, urinalysis was not performed because serum creatinine levels were normal. The kidney was microscopically normal and no amyloid deposit was noted. Hypocalcemia in this horse was likely associated with the hypoalbuminemia. Anemia is common in multiple myeloma due to myelophthisis, and macrocytosis has been reported in horses and humans with myeloma. 3 In this case, macrocytosis could be explained by possible regenerative anemia due to GI hemorrhage or dyserythrocytosis due to myelophthisis. The cause of the increased MCHC was undetermined, and clinical significance was questionable. GI amyloidosis, hemorrhage, and inflammation may be the cause of the inflammatory leukogram (leukocytosis, neutrophilia with left shift and toxic change). The lymphopenia and hyperglycemia were likely associated with stress.
Equine amyloidosis is very uncommon with few reported cases. 4–6 , 8 , 15 , 17 , 18 Almost all equine cases were localized, AA amyloidoses associated with chronic inflammation such as severe strongyle infection 18 and tuberculosis 17 or neoplasia such as lymphoma 4 and adrenal cortical adenoma. 17 Nasal cavity and skin are the two most frequently affected sites, and often the exact cause cannot be identified. Five cases of equine AL type amyloidosis have been described: idiopathic systemic amyloidosis of unknown cause in a 14-year-old thoroughbred mare; 5 localized cutaneous amyloidosis associated with lymphohistiocytic lymphosarcoma in an 11-year-old stallion; 17 localized cutaneous amyloidosis in a horse with extramedullary plasmacytoma; 10 and nasal amyloidosis in two horses. 11
There is only one case report of myeloma-associated systemic AL amyloidosis in domestic animals. A 10-year-old cat was reported to have systemic AL amyloidosis associated with an extramedullary plasmacytoma on the right tarsus. 1 To our knowledge, this is the second report describing systemic AL amyloidosis in domestic animals–associated plasma cell neoplasia and the first associated with multiple myeloma, as is common in humans.