
Abstract
The Fusarium species are a group of saprophytic fungal organisms that are occasionally the cause of opportunistic infections in humans and animals. Central nervous system disease associated with a Fusarium species is most commonly described in horse, resulting in equine leukoencephalomalacia. This report describes a 2-year-old, spayed, female German Shepherd Dog with meningoencephalitis secondary to infection with Fusarium spp. Meningoencephalitis in dogs secondary to a species of Fusarium has not been previously reported. The diagnosis was made based on the histopathologic examination of brain tissues postmortem and special immunohistochemical stains specific for Fusarium solani. The clinical signs in this dog were indicative of multifocal brain disease and included seizures and a paradoxical vestibular syndrome. The clinical findings, diagnostic and histopathologic test results, and the comparative characterizations of other disseminated fungal diseases, especially aspergillosis, are described.
Keywords
The Fusarium species are a group of saprophytic fungal organisms that inhabit the soil and are commonly isolated from plants. 22,33 Some of the Fusarium organisms are important pathogens of plants and are occasionally the cause of opportunistic infections in humans and animals. 21 Several different fungal organisms have been shown to cause meningitis and encephalitis in both large and small animals. Fungal organisms commonly reported to infect the central nervous system of small animals are Cryptococcus neoformans, 35,42 Blastomyces dermatiditis, 3,20 Histoplasma capsulatum, 32 Coccidiodes immitis, 27 Cladophialophora bantiana, 2 and several species of Aspergillus including Aspergillus fumigatus and A. terreus. 7,23,24 Meningoencephalitis in dogs secondary to a species of Fusarium has not been previously reported.
A 2-year-old, spayed, female German Shepherd Dog was presented to the Veterinary Neurological Center (Las Vegas, NV) for evaluation of a 2-week history of generalized seizure activity and a 3-day history of ataxia, circling, and nystagmus. Before the onset of the neurologic signs, the dog had been healthy and was current on vaccinations. On neurologic examination, the dog was moderately ataxic, had a head tilt to the right, had a persistent left horizontal nystagmus, and compulsively circled to her right. Dysconjugate oculovestibular eye movements were present when the head was moved horizontally in both directions. The remaining cranial nerve examination findings were normal as were postural placing reactions and segmental spinal reflexes. The general physical examination findings were normal. The history and presenting clinical signs were consistent with multifocal brain disease. The history of seizures suggested involvement of the cerebrum, whereas the vestibular signs suggested involvement of the right brain stem or right vestibulocochlear nerve.
A complete blood count and serum chemistry profile were unremarkable. Thoracic and abdominal radiographs were normal. A contrast-enhanced computed tomography (CT) brain scan was done and showed multiple, diffusely coalescing areas of contrast enhancement in the left cerebrum involving the left occipital and parietal lobes and internal capsule. Smaller multifocal contrast-enhancing lesions were also identified in the cerebellum at the left cerebellopontine angle. There was extensive white matter edema in the left cerebral hemisphere collapsing the left lateral ventricle and deviating the falx cerebri to the right of midline (Fig. 1). Spinal fluid collected from the cerebellomedullary cistern was xanthochromic and showed elevations of protein (154 mg/dl; reference range, 18–24 mg/dl) and white blood cells (306 cells/mm3; reference range, 0–4 cells/mm3). White blood cell distribution of the spinal fluid after cytocentrifugation showed 50% neutrophils, 36% monocytes, and 14% lymphocytes. No organisms were identified. Serum A. fumigatus, A. niger, A. flavus, and A. terreus, C. immitis, and Ehrlichia canis titers were negative. Urinalysis, urine aerobic and anaerobic bacterial and fungal cultures, as well as aerobic and anaerobic bacterial cultures performed on the spinal fluid were also negative.
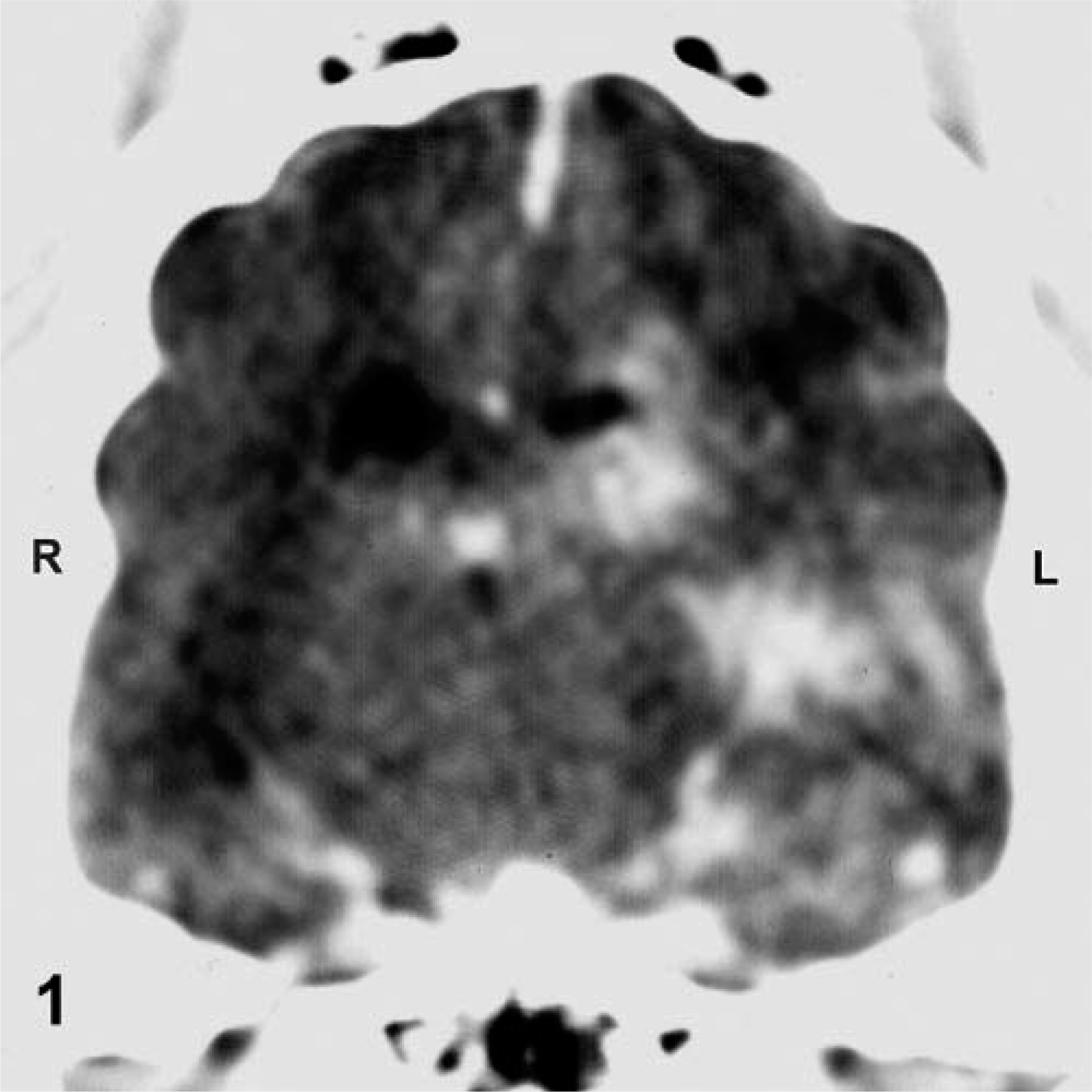
Transverse contrast-enhanced CT image of the brain at the level of the dorsum sellae of a dog with intracranial fusariosis. There are multiple, diffusely coalescing areas of contrast enhancement centered in the left hippocampus, with ventrolateral and medioventral extension into the adjacent internal capsule and rostral midbrain, respectively. There is extensive white matter edema in the left cerebral hemisphere collapsing the left lateral ventricle and deviating the falx cerebri to the right of midline. R, right; L, left.
The dog was empirically treated with dexamethasone sodium phosphate for the brain inflammation and associated edema, and the recovery from anesthesia was uneventful. The morning after the testing, the dog was bright, alert, and responsive, and the vestibular signs had resolved. The dog was discharged and oral prednisone prescribed pending the results of the submitted serum, spinal fluid, and urine tests. Two days after discharge, the dog was returned to the hospital in status epilepticus. Shortly after presentation, the dog developed decorticate rigidity followed by respiratory arrest and was then humanely euthanatized.
At necropsy, gross lesions were restricted to the central nervous system. The external surface of the brain appeared normal except for a few small swellings of the basilar artery on the ventral medulla. On the transverse sections, the caudal aspect of the caudate nucleus and the amygdala in the left pyriform lobe were enlarged, firm, irregular, and gray. This lesion extended into the left parahippocampal gyrus, adjacent hippocampus, and left claustrum and continued caudally in the ventral and lateral aspects of the temporal and occipital lobes. On microscopic examination, the gross lesions all related to an extensive granulomatous disease. On the hematoxylin and eosin–stained sections, there were focal and coalescing foci of inflammation consisting predominately of macrophages, some lymphoplasmacytic cells, and a few neutrophils. Reactive astrocytes were abundant on the borders of the inflammation. A severe vasculitis was present in many of the larger vessels in the leptomeninges, some of which extended into the adjacent parenchyma. The walls of these vessels were thickened with fibrosis and inflammatory cells. There was occasional necrosis of vessel walls, and intravascular thrombosis was common. The larger portions of the parenchymal lesion represented a coalescence of variably sized perivascular granulomas. Perivascular collagen was abundant in these lesions. Several small granulomatous lesions were also present in the cerebellum but were not as profound as the cerebral lesions. Periodic acid–Schiff (PAS) and Grocott's methenamine silver (GMS) stains were applied to the sections of the lesions and identified an abundance of short, septate hyphae with dichotomous branching characteristic for Ascomycete fungi 25 but not specifically for Aspergillus (Fig. 2). In addition, the PAS stains showed the fungal organisms better than the GMS stain, which was considered unusual for Aspergillus. The type of inflammatory lesion observed in the brain of this dog and the extensive vascular thrombosis were typical for encephalitis caused by fungal organisms such as Aspergillus; however, the poor staining of the organism with the GMS stain suggested that a fungal agent other than an Aspergillus was present.
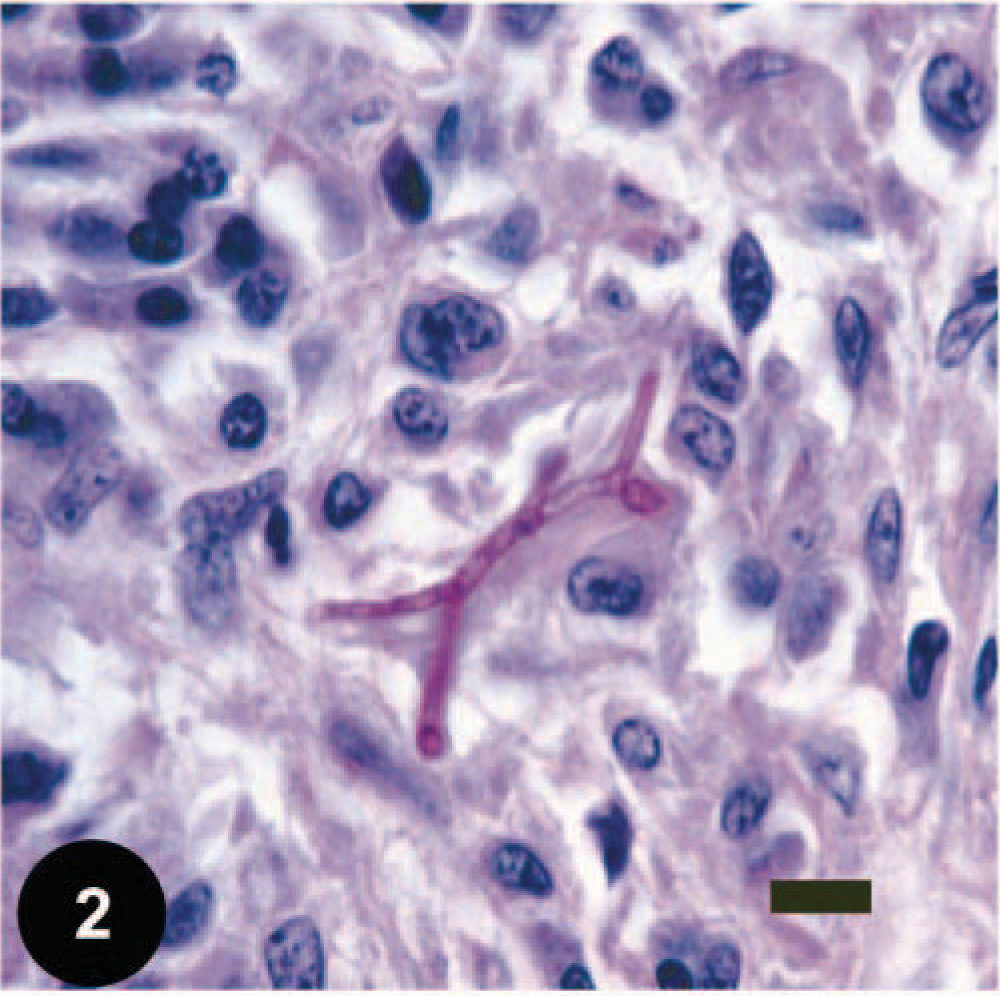
Photomicrograph of a fungal granuloma from the cerebral cortex of a dog with intracranial fusariosis. There were multiple, short, septate hyphae with dichotomous branching, such as demonstrated in Fig. 2, surrounded by variably sized macrophages, giant cells, and neutrophils. PAS. Bar = 25 µm.
Immunohistochemistry was used to identify the etiologic agent. The principles of the peroxidase-antiperoxidase (PAP) technique have been previously described.
14,15,17
In this case, tissue sections were mounted on poly-
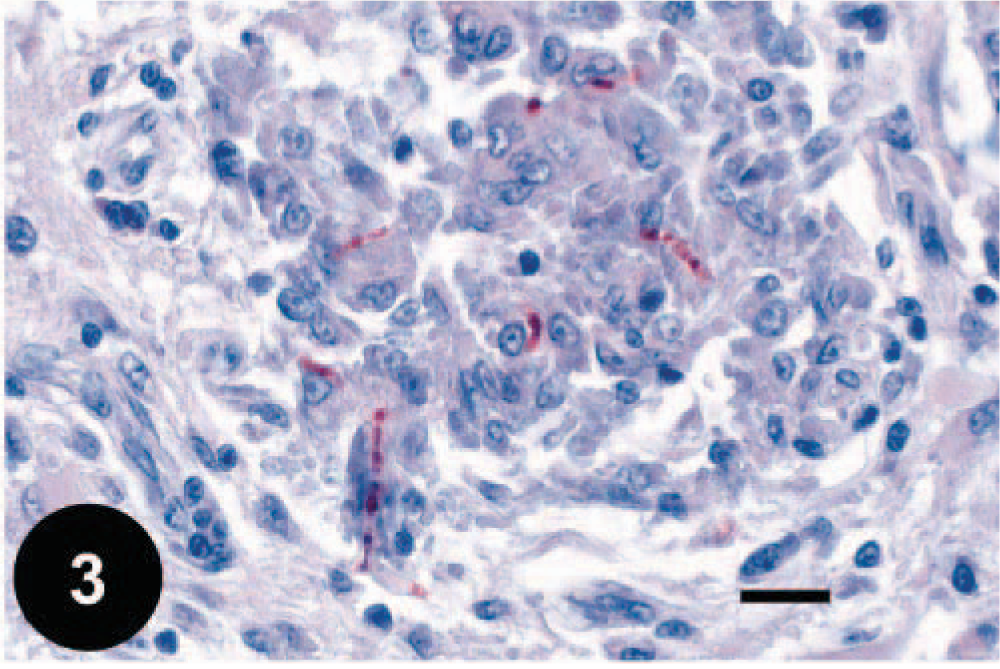
Photomicrograph of a fungal granuloma from the cerebral cortex of a dog with intracranial fusariosis. Positive immunohistochemistry reaction using an indirect PAP technique with heterologously absorbed anti-Fusarium antibodies. 17 Harris' hematoxylin counterstain. Bar = 25 µm.
Central nervous system disease associated with a Fusarium species is best known in horse. Equine leukoencephalomalacia, also known as “moldy corn disease,” is a disease caused by the ingestion of corn-based feed contaminated with the fungus F. moniliforme. 11,22 The mycotoxin of F. moniliforme, fumonisin B1, is thought to selectively destroy the blood vessels of the cerebral white matter, leading to perivascular edema and eventual necrosis of the glial cells. 21,29,39,43 Similar lesions of liquifactive necrosis may also occur in the brain stem, cerebellum, and spinal cord white matter. 43 Histopathologic lesions in the liver such as portal fibrosis and hepatocellular lipidosis are also common in horses with fumonisin B1 mycotoxicosis, but the neurologic signs typically dominate the clinical picture. 5,21 Other forms of Fusarium mycotoxicosis, such as F. tricinctum, affecting the central nervous system of rabbits 9 and white-tailed deer 12 have been reported. Central nervous system Fusarium mycosis has also been reported to occur in humans. Most human patients with disseminated fusariosis suffer a condition of general immunosuppression, such as secondary to leukemia 1,30,34,38 or advanced human immunodeficiency virus infections. Disseminated fusariosis is also an uncommon complication of bone marrow transplantation. 8,18,30 In most cases, the skin was the reported portal of entry. 1,10,18,38 Fusarium spp. have infrequently been isolated from the hair coat 4 or from cutaneous lesions in dogs 13 but are usually only encountered in the summer months and are typically considered environmental contaminants rather than pathogens. 4
The fact that the dog in this report was a German Shepherd Dog may be coincidental, but there is an apparent predisposition for this breed to develop disseminated aspergillosis. German Shepherd Dogs are thought to have a defect in the production of IgA antibodies 6,7,40 which may lead to their susceptibility to opportunistic disseminated Aspergillus-related osteomyelitis and diskospondylitis. 6,7 Though not proven, it seems reasonable that this dog may have had some type of underlying immunodeficiency. It is also interesting that the dog in this report lived on a horse ranch. Central nervous system Fusarium-related lesions have been best characterized in the horse, but the significance of the relationship of intracranial fusariosis in this dog and the proximity of horses is not known.
The generalized seizures combined with the presence of right-sided vestibular signs suggested a multifocal intracranial disorder primarily affecting the right brain stem or right vestibulocochlear nerve and cerebrum. The CT brain scan and gross necropsy findings showed the lesions to be primarily affecting the left side of the brain. Though the majority of the parenchymal destruction from the fungal granuloma and vascular infarctions were in the left cerebrum, the involvement of the left caudal cerebellar peduncle of the brain stem likely contributed to the paradoxical vestibular signs.
Aspergillosis was the primary differential due to the predisposition of the German Shepherd breed for this specific fungal organism. 6,7,40 Though the serologic tests for aspergillosis were negative, such results do not always preclude an Aspergillus organism as the underlying cause of infection. Some commercial laboratory assays may test only for antibodies to A. fumigatus and may not react positively if A. terreus or some other species is responsible for a disseminated infection. 31 False negatives may also occur. 19,36,41 The serologic tests used in this case, however, screened for antibodies against A. fumigatus, A. terreus, A. niger, and A. flavus. Urinalysis and urine fungal cultures are often effective methods for diagnosing disseminated aspergillosis, 7 but in this case they were negative, further strengthening the case against aspergillosis. The histopathologic appearances of the parenchymal lesions within the brain were consistent with a fungal infection, but the poor GMS staining of the organism was not completely characteristic of aspergillosis. Though fungal cultures on the cerebrospinal fluid or central nervous system tissues were not done, immunohistochemistry has proven to be an effective tool for the accurate diagnosis of a number of mycoses in humans and ani mals. 14–17 Attempts to isolate fungi even from fresh tissue specimens may be unrewarding, especially because contamination may be a problem when dealing with opportunistic fungi. 15,28 The hyphal forms of several opportunistic pathogen fungal genera, such as Candida spp., Aspergillus spp., Fusarium spp., Scedosporium apiospermum (anamorph of Pseudallasceria boydii), and to a certain extent, the species of the Zygomycetes are indistinguishable. 15,17,26 To meet the demand for in situ identification of opportunistic fungal genera, different indirect immunohistochemical procedures 15,17 using a series of genus-specific monoclonal and polyclonal antibodies toward Candida spp., Aspergillus spp., Fusarium spp., S. apiospermum, and Zygomycetes have been developed and widely used on human and animal tissues. 15,17,18,37 In the present study, immunohistochemical techniques resulted in definitive identification of F. solani as the causative organism.