
Abstract
Myocardial ischemia, an uncommon cause of sudden death in dogs, usually results in infarction and fibrosis of the myocardium. Necropsy examination of a 13-year-old German Shepherd dog that died suddenly demonstrated multifocal myocardial thinning and loss in the left and right ventricular free wall and right atrium. Histopathologic examination confirmed the myocardial thinning to be sites of myocyte atrophy and loss, with loose reticulin-positive fibrovascular tissue and adipocytes and little fibrosis. Many intramural coronary arteries were irregularly thickened and partially occluded by segmental intimal and medial deposits of periodic acid-Schiff-positive, Congo red-negative amorphous extracellular material. This finding is consistent with hyaline arteriosclerosis. These vascular lesions likely lead to insufficient perfusion of the affected myocardium and gradual loss of myofibers without the acute necrosis and fibrosis characteristic of infarction.
Arteriosclerosis is a nonspecific term for changes in arteries that result in a loss of elasticity in the vessel wall. 6 Atherosclerosis, the most common form of arteriosclerosis in humans, is the result of lipid and inflammatory cell accumulations (plaques) within the arterial intima. 6 Atherosclerosis in dogs is usually associated with hypercholesterolemia and hyperlipidemia coincident with hypothyroidism; myocardial infarction is reported to be common in hypothyroid dogs. 3 Arteriolosclerosis, a subtype of arteriosclerosis specifically involving small arteries, has been found to be an important cause of ischemic heart disease in the dog, usually resulting in myocardial infarction. 2 This case involves intramural hyaline coronary arteriolosclerosis associated with atrophy and loss of the myocardium without evidence of myocardial infarction.
A 13-year-old German Shepherd dog had been considered healthy until the owners reported a 24-hour period of lethargy and recumbency before death. The animal was subsequently submitted to the College of Veterinary Medicine at Michigan State University for necropsy.
At necropsy, approximately 100–150 ml of serosanguineous fluid was present in the thoracic cavity, and the lungs contained diffuse moderate edema. Scattered within the free wall of both the right atrium and the right ventricle, there were multifocal discrete foci of myocardial thinning (Fig. 1). The myocardial thinning formed depressions within the wall of both the atrium and the ventricle; however, there was preservation of the normal epicardial vasculature overlying these sites (Fig. 1). The periphery of the myocardial lesions were demarcated by a thin (1–2 mm), pale rim; centrally, the myocardium was thin and translucent (Fig. 2). Depressions in the myocardium were not present on the epicardial or endocardial surfaces of the left ventricle; however, the cut section of the free wall of the left ventricle contained several depressions within the myocardium (Fig. 2).
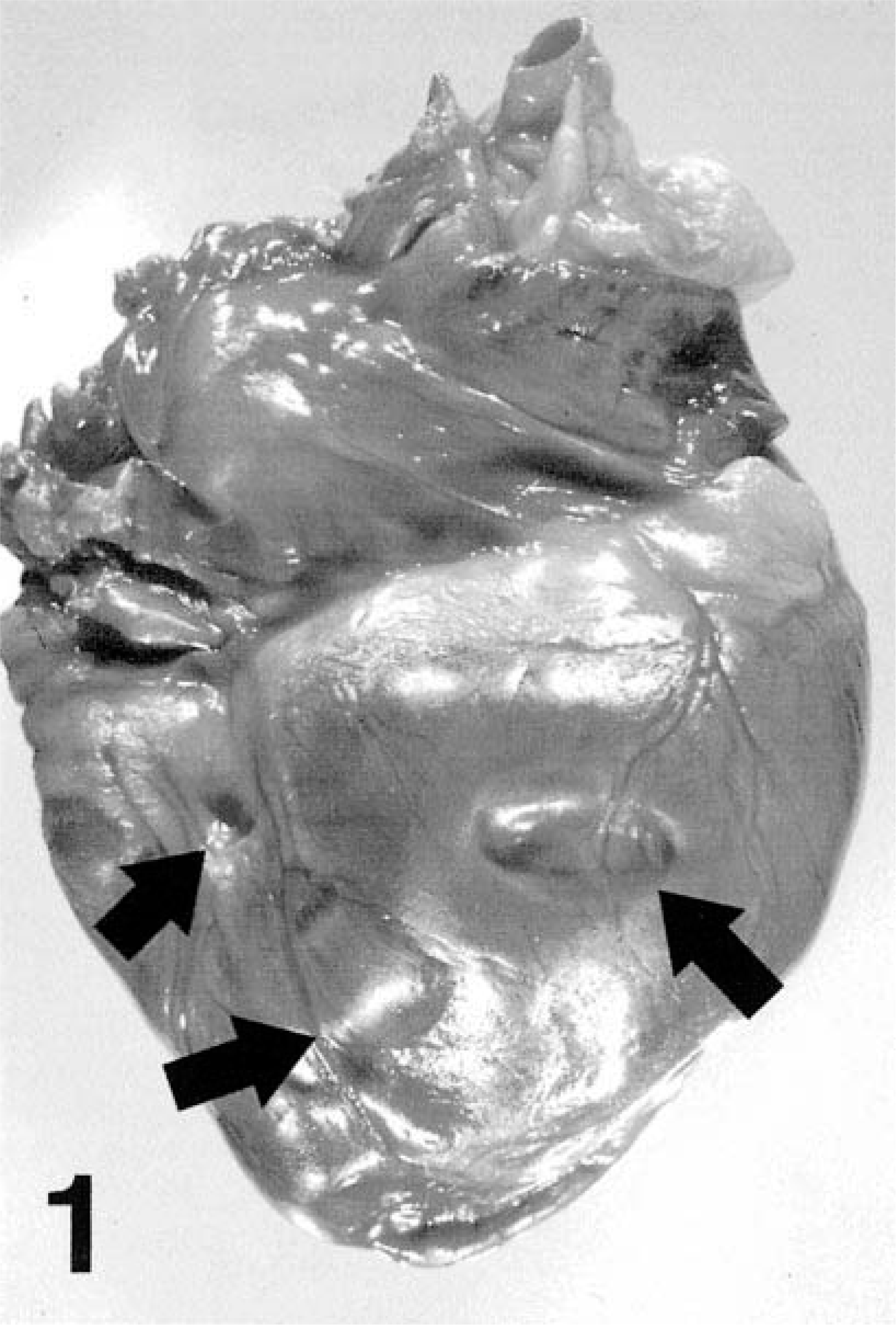
Heart; dog. Multifocal myocardial atrophy (arrows), right ventricle characterized by depressions in the free wall, with preservation of the epicardial vasculature.
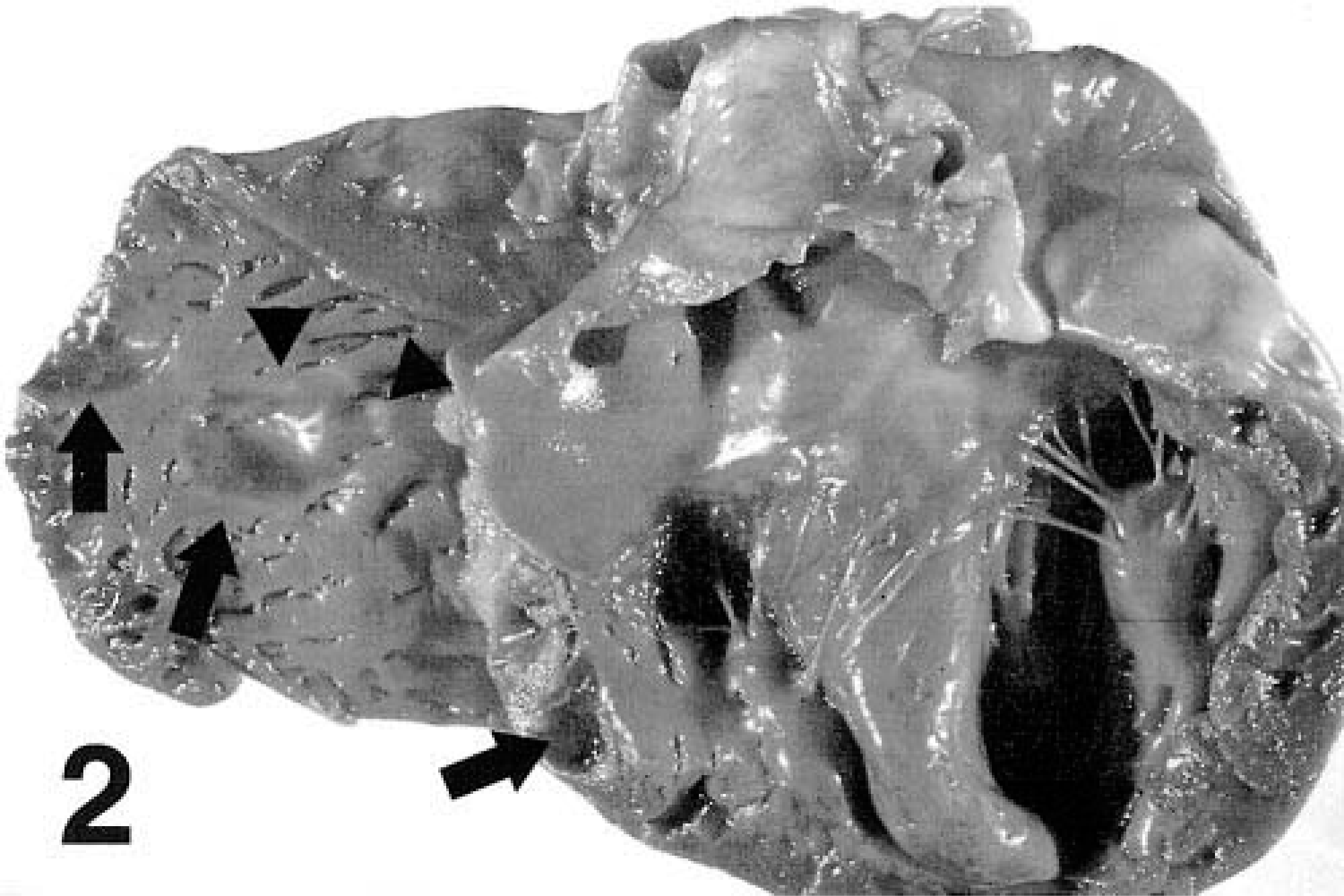
Heart; dog. Multifocal myocardial atrophy (arrows), left and right ventricle. Note the accumulation of inflammatory cells at the periphery of the foci of right atrial atrophy (arrowheads).
Tissues collected at the time of necropsy were immersion-fixed in 10% neutral buffered formalin and embedded in paraffin for histopathologic examination. Separate, successive 6-µm sections of the myocardium were stained using hematoxylin and eosin, periodic acid–Schiff (PAS), Masson trichrome, reticulin stain, or Congo red.
At histopathologic examination, the affected regions of the heart were devoid of cardiac myocytes but contained condensed and collapsed stroma, with sparse mature collagen bundles and adipocytes (Fig. 3). The affected regions of the right ventricle were transmural, with atrophy of the myocytes. In the left ventricle the myofiber loss involved primarily the subendocardial myocardium but did not extend to the epicardial surface. Reticulin and Masson trichrome staining of the stroma revealed an abundance of loose reticulin fibers in the regions of myocardial atrophy (Fig. 3). At the periphery of the myocardial thinning, there was a prominent band of infiltrating lymphocytes and plasma cells with smaller numbers of macrophages (Fig. 3), consistent with nonsuppurative inflammation. The myocytes interspersed with these cells were atrophied and often degenerate (Fig. 4). The walls of multiple intramural coronary arteries, both within and adjacent to the myocardial atrophy, were markedly segmentally thickened (Fig. 5). The intima and media were expanded and disrupted by irregular deposits of pale, eosinophilic, amorphous hyaline material (Fig. 5). This material stained positively with PAS and Masson trichrome and did not stain with Congo red. These hyaline deposits elevated the endothelium, and the lumen of many of the vessels was markedly diminished.
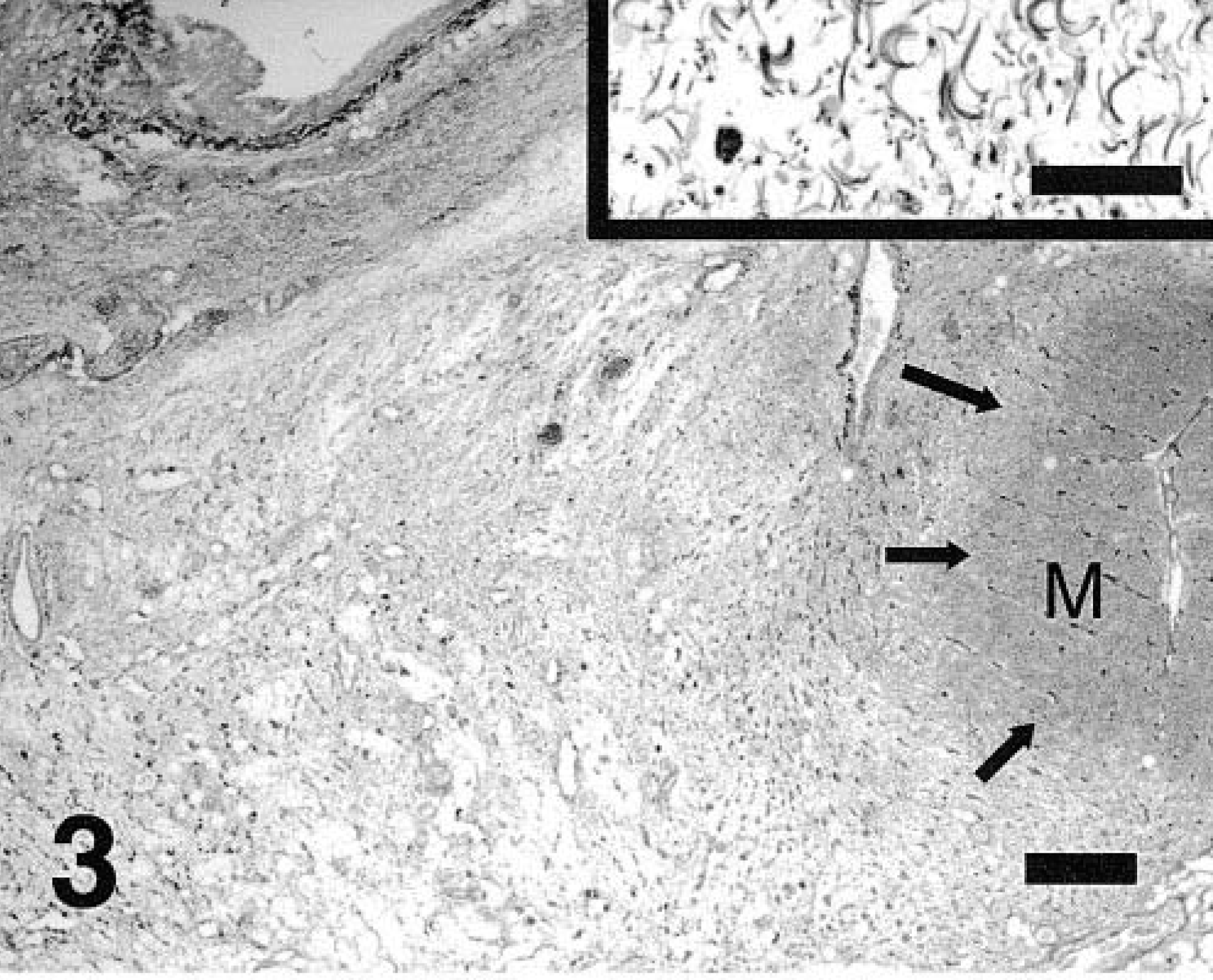
Myocardium; dog. Myocardial atrophy with myocyte loss and replacement with loose reticulin-positive stroma. Note the adjacent myocardium (M) with band of lymphoplasmacytic inflammation (arrows). Inset: High magnification of reticulin stroma. Snooks reticulin stain. Bar, low magnification = 400 µm; bar, inset = 50 µm.
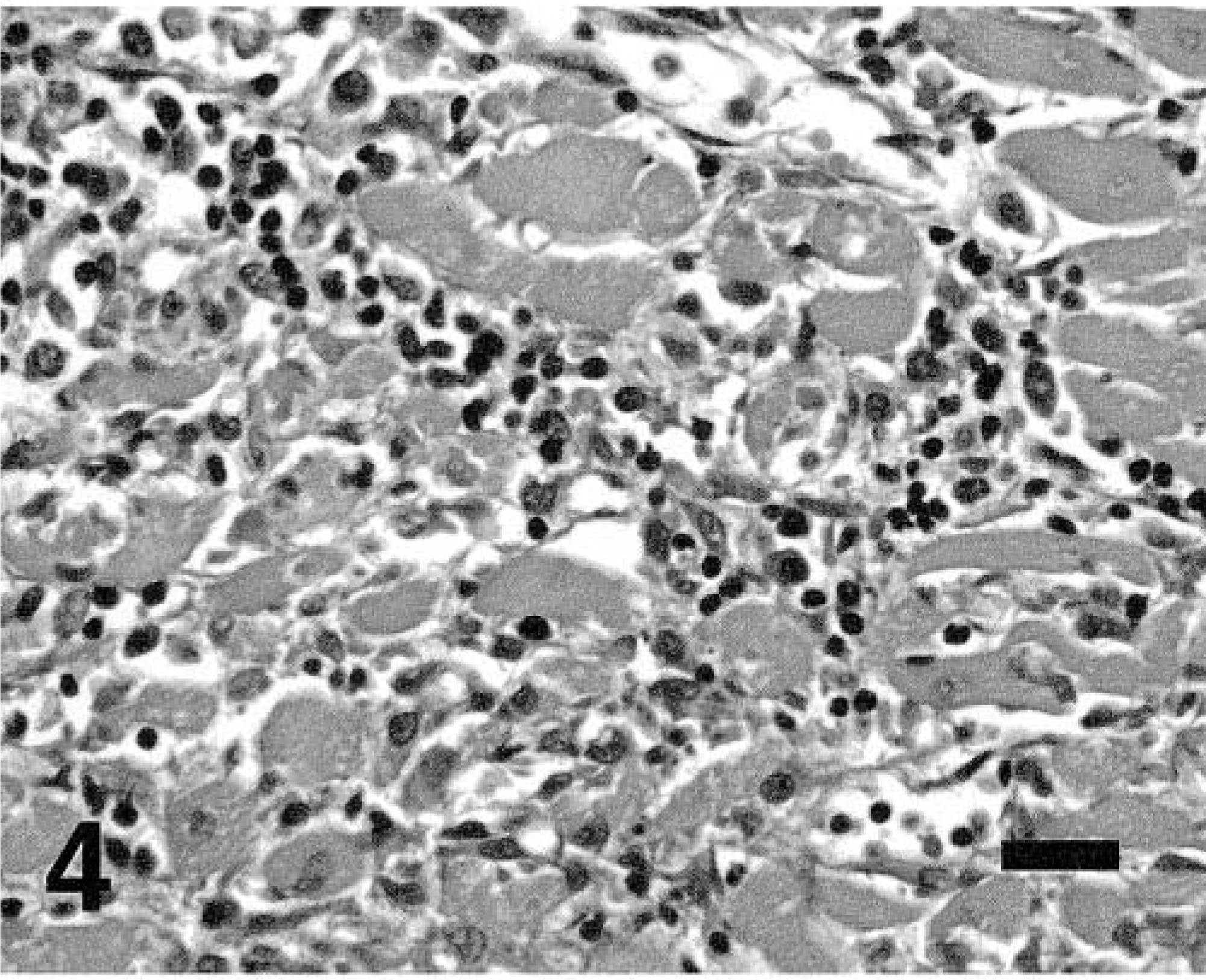
Lymphoplasmacytic myocarditis with myocyte degeneration. HE. Bar = 50 µm.
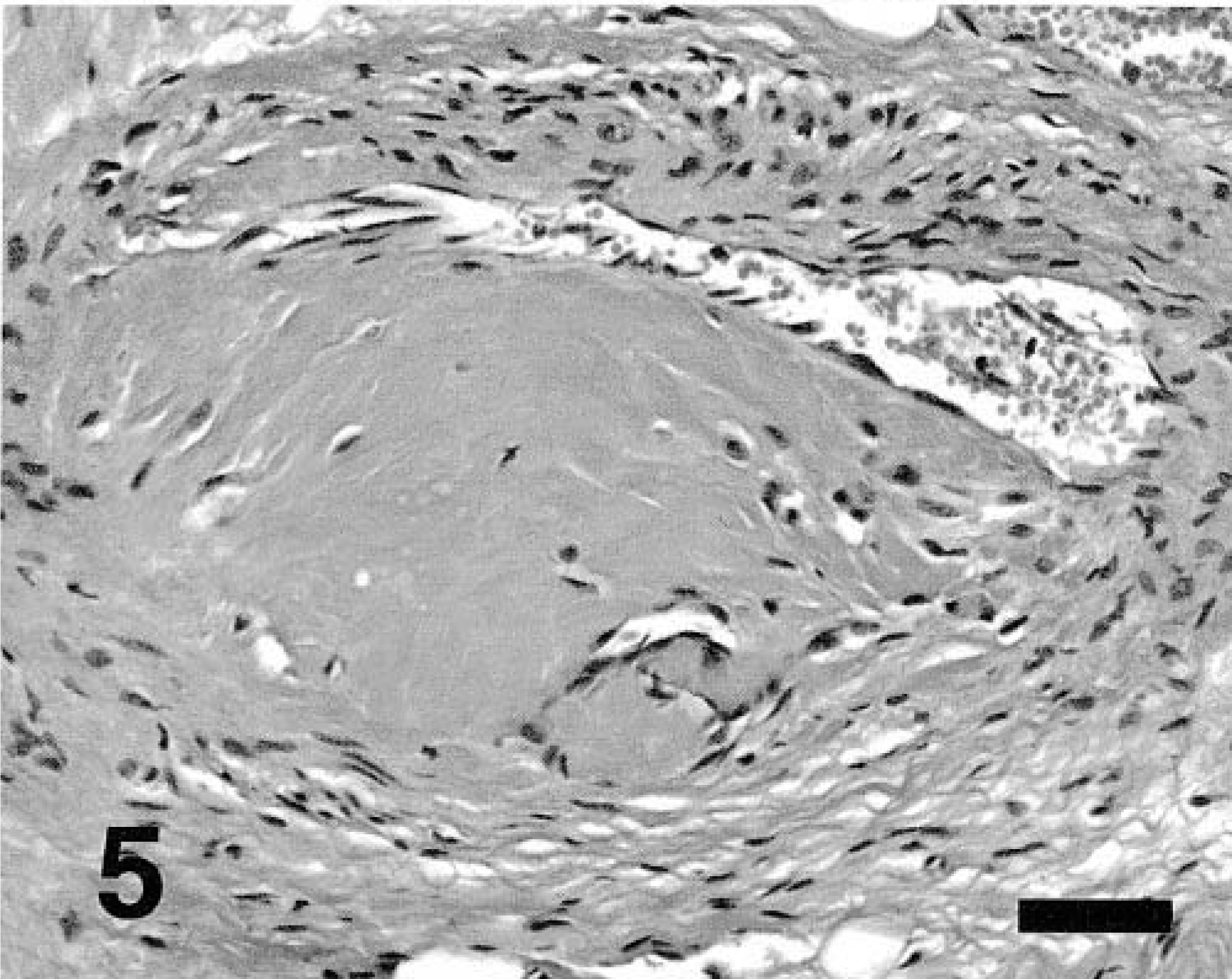
Hyaline arteriolosclerosis with partial lumen occlusion, intramural coronary artery, left ventricle. HE. Bar = 50 µm.
Myocardial atrophy, without evidence of other sites of infarction, is an unusual manifestation of arteriosclerosis. The development of infarction in the myocardium as the result of primary coronary arteriosclerosis is well described in humans, dogs, and experimental models of cardiovascular disease. 2,3,5,6 The sequence of events in myocardial infarction has been documented in humans and experimental models of infarction after coronary arterial occlusion in rabbits. 5,6 In both, the chronic manifestations are characterized by myocyte replacement with granulation tissue followed by dense collagen deposition. 5,6 This process leads to grossly discernable, pale, shrunken foci of scarring after the initial ischemic event. Neither the necropsy nor the histopathologic features of this heart are consistent with prior infarction underlying the lesions in this animal.
Decreased blood supply is a common cause of atrophy, irrespective of tissue type. 1 Apoptosis of cardiomyocytes, a known consequence of hypoxia, may have been a factor in the development of myocardial atrophy in this animal. 4 Experimental myocardial infarction and chronic heart failure in dogs, induced through intracoronary microembolization, resulted in cardiocyte apoptosis adjacent to the foci of infarction. 7,8 A similar process may occur in hypoxic but not ischemic myocardium when there is insufficient myocardial perfusion because of arteriolosclerosis. Falk and Jönsson described 65 cases of ischemic heart disease in dogs with histopathologically confirmed arteriosclerosis. 2 Myocardial infarction with fibrosis was found in 51 of the 65 dogs with arteriolosclerosis, but there is no mention of focal myocardial atrophy as was seen in the dog in this study. 2
The mononuclear inflammation in the myocardium was restricted to the peripheral regions of myocardial degeneration. Lymphocytic inflammation occurs after myocardial ischemia, typically interspersed with the granulation tissue and macrophage infiltrates common to early infarction, but these findings were absent in the myocardium of the dog in this study. 5
The pathogenesis of hyaline coronary arteriolar lesions in the dog is not well understood. Arteriolosclerosis can be subdivided into hyaline and hyperplastic subtypes. 6 Hyperplastic arteriolosclerosis is characteristic of hypertensive states, particularly acute, severe elevations in blood pressure. 6 The vascular wall in such patients is characterized by concentric, laminar proliferations of smooth muscle cells and basement membrane, with the lesions most common in the kidney. 6 In contrast, hyaline arteriolosclerosis may be seen in normotensive individuals and is considered a common finding in elderly people. When it occurs in hypertensive people, hyaline arteriolosclerosis is generalized and more severe. 6
Fibromuscular intimal thickening and hyalinosis were reported in the coronary arteries of the 65 dogs with ischemic heart disease, with no disease reported in organs other than the heart. 2 The lesions in the present animal were also restricted to the heart, and there was no histopathologic evidence of generalized hypertension or additional disease processes in other organs. Pure hyaline arteriolosclerosis is assumed to be the result of earlier endothelial injury, allowing leakage of plasma proteins into the subendothelial space and deposition of smooth muscle–derived extracellular proteins. 2,6
Myocardial atrophy, without coexistent infarction, is an unusual manifestation of arteriolosclerosis in dogs. The diagnosis of atrophy can be made by documenting the lack of fibrosis in the regions of myocardial fiber loss with concomitant condensation of the reticulin stroma. This myocardial change may be associated with rapid clinical deterioration and death in dogs.