
Abstract
The placenta from a 300-day-gestational age, female, Arabian equine fetus was examined. Multifocal to coalescing, 0.5- to 4-cm-diameter, white, smooth nodules covered 50% of the placenta. Microscopic evaluation of the nodules revealed undifferentiated germ cells and a haphazard arrangement of immature, mesenchymal stroma, cartilage, squamous cornifying epithelium, scattered ducts and secretory acini lined by cuboidal to columnar epithelium, and mineralized foci. No umbilicus, arrangement about an axial skeleton, or organized polarity of structures was present. The lesion was diagnosed as a placental teratoma, a lesion not reported in species other than man.
A 16-year-old multiparous Arabian mare aborted a 300-day-old, small, but otherwise normal, fetus. The placenta was passed along with clear, nonodoriferous, watery fluid. The referring veterinarian submitted the placenta for examination. Multifocal to coalescing, 0.5- to 4-cm-diameter, white and grey, smooth nodules covered 50% of the placenta (Fig. 1). The nodules were disseminated throughout the fetal surfaces of the chorioallantois, the vessels, and the umbilical cord, but the greatest density of nodules was in the placental horns, away from the insertion of the umbilical cord. The centers of the nodules were red, moist, and malacic or white and gritty. Aerobic bacterial and fungal cultures of the nodules were negative. Sections of placenta were fixed in 10% neutral buffered formalin and processed routinely for histology.

Placenta; 300-day–gestational age aborted equine fetus. Numerous nodules, 0.5- to 4-cm diameter, efface over 50% of the placenta.
Microscopic examination of the placenta revealed the stroma of the chorioallantois to be multifocally expanded and effaced by nodules composed of packets of poorly differentiated, round to polygonal cells separated by short, anastomosing, fibrovascular bands (Fig. 2). These cells had hyperchromatic nuclei with radiating chromatin and 1–2 large nucleoli. Mitoses were infrequent (1–2 per 10 hpf). These nodules resembled nodules of undifferentiated germ cells. Other nodules contained a haphazard admixture of embryonic layers that recapitulated, in order of abundance, immature mesenchymal to myxomatous stroma, cartilage, squamous cornifying epithelium, ducts lined by cuboidal to columnar epithelium, and acini lined by cuboidal cells having nuclei with basal polarity, apical vacuoles, and luminal amorphous eosinophilic material (Fig. 3). Foci of coagulative and liquefactive necrosis with variable amounts of edema, hemorrhage, neutrophils, lymphocytes, macrophages containing erythrocytes and hemosiderin, and mineralization were present multifocally throughout the tumor. The presence of multiple germ layers lacking organization was consistent with a placental teratoma.
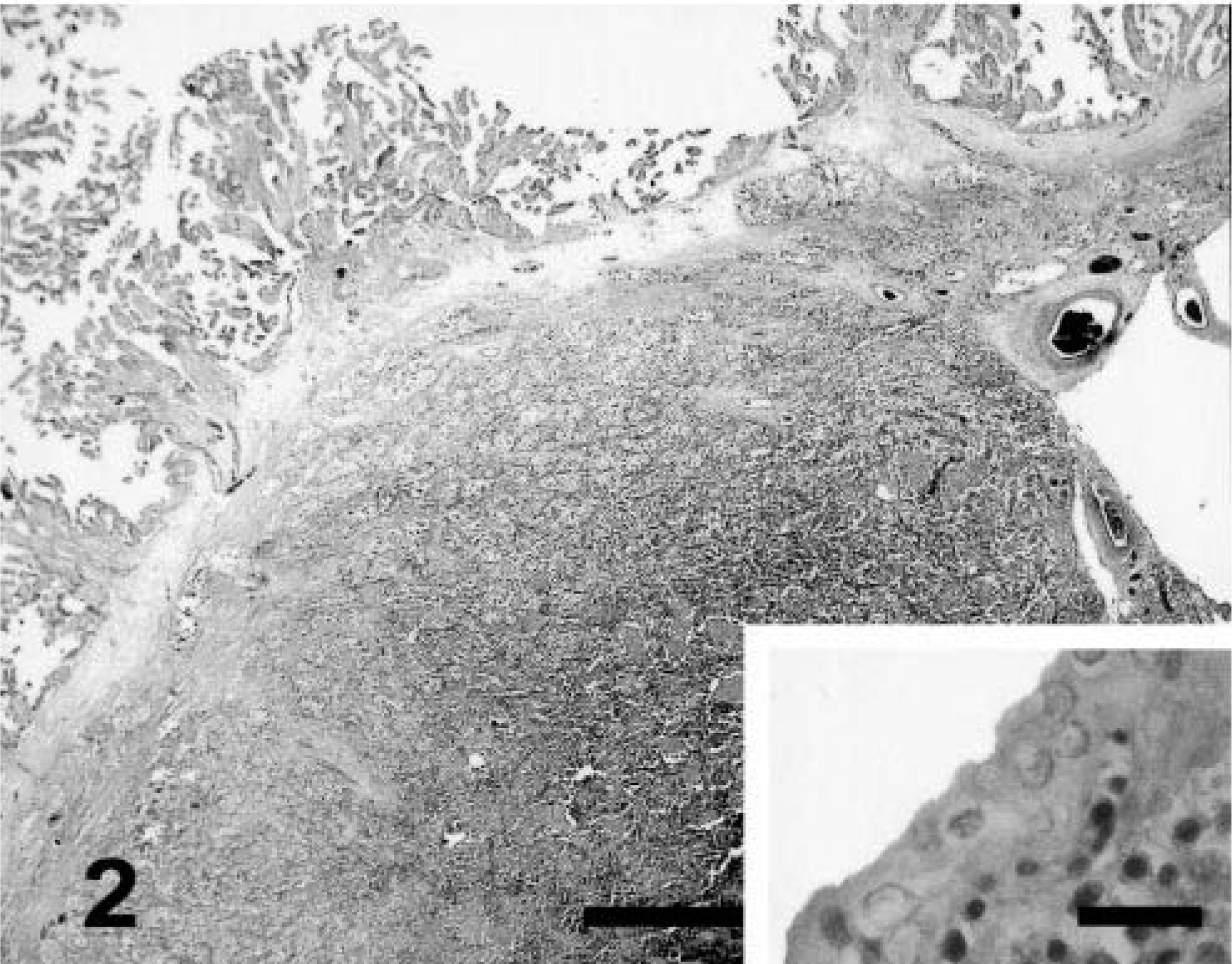
Placenta; equine. A nodule composed of undifferentiated germ cells expands the chorioallantoic stroma. Bar = 1 mm. Inset: A single layer of normal allantoic epithelium overlays the germ cells. HE. Bar = 30 µm.
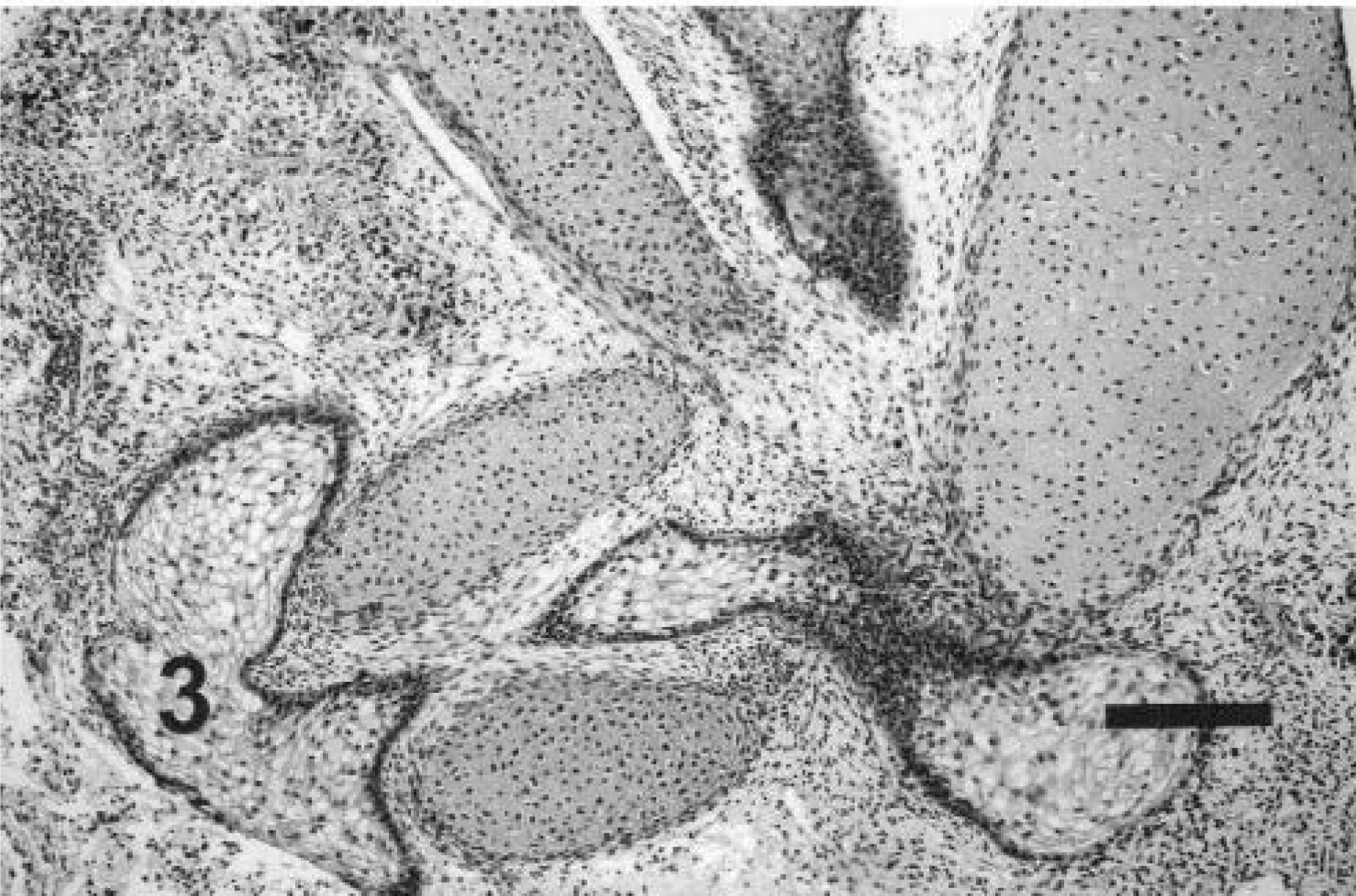
Placenta; equine. This teratoma nodule contains a haphazard arrangement of squamous epithelium, epithelium with ballooning degeneration, cartilage, and undifferentiated mesenchymal cells. HE. Bar = 130 µm.
Teratomas arise from pluripotent germ cells that differentiate into tissues from two or three of the embryonic layers: endoderm, mesoderm, and ectoderm. 13 Monodermal or specialized teratomas contain only a single tissue. 5,12 Teratomas are infrequently observed in domestic animals and are most commonly reported in the ovaries of bitches. 15 In horses, occurrences in the ovary and cryptorchid testes have been reported. 1,23,24,26 Although reported with frequency in humans, review of the literature failed to identify the occurrence of a placental teratoma in any other species. Differential diagnoses for placental nodules include trophoblastic diseases, such as partial and complete hydatidiform moles and choriocarcinoma; germ cell tumors, such as dermoid cyst (benign mature cystic teratoma) and dysgerminoma; metastatic tumors; and granulomas. One of the primary differentials for a placental nodule with fetal features is fetus acardius amorphous. Fetus acardius amorphous is a blighted dizygotic or monozygotic twin fetus. 2,4 Morphologically, it differs from a placental teratoma in that the former has a separate umbilical cord and sufficient organization of the tissues to distinguish cranial and caudal poles of the fetus. The axial skeleton also is recognizably formed. Placental teratomas lack organization and polarity, and they do not have separate umbilical cords. Metastasis of a teratoma to the placenta was considered; however, no other masses or illness of the mare was observed in the 12 months after the diagnosis of placental teratoma. Metastasis from another site was therefore considered unlikely.
A unique lesion of the equine placenta that might be confused grossly with this teratoma is adenomatous hyperplasia of the equine allantoic epithelium. 9,16,21 The advanced stages of this latter lesion consist of multiple firm nodules on the allantois, ranging from 1 to 60 cm in diameter, most often clustered near the umbilical stalk. Histologically, nodules consist of variably sized glands extending from the allantoic surface down to the arteries of the chorion. 16 The lesions are classified from stages 1 to 3 based on the increasing severity of allantoic epithelial hyperplasia and gland formation. 9 Chronic placentitis may be a predisposing cause. 9,21 The lesions in the placenta of this mare differ from adenomatous hyperplasia of the equine allantoic epithelium in several ways. First, the nodules were concentrated away from the umbilical cord rather than clustering around it. Second, the microscopic morphology of the nodules was entirely different. Hyperplasia of the allantoic epithelium was either absent or minimal. Nodules consisted predominantly of undifferentiated germ cells, poorly differentiated mesenchymal stroma, islands of cartilage, and squamous epithelium. Unlike adenomatous hyperplasia of the allantoic epithelium, glandular structures were the smallest component of the nodules and not continuous with the overlying allantoic epithelium. In addition, cartilage has not been described in adenomatous hyperplasia of the equine allantoic epithelium. For these reasons, the placental lesion observed was considered to be a distinct lesion, not previously described in domestic animals.
The similarity to the human syndrome gliomatosis peritonei was assessed. In gliomatosis peritonei, peritoneal nodules composed of mature, glial fibrillary acidic protein (GFAP)–positive glia are disseminated throughout the peritoneum. 8 They are associated with ovarian teratomas. 19 The nodules were thought to arise from implantation or angiolymphatic spread of neuroectodermal cells of a teratoma to the peritoneum. A recent study, however, compared polymorphic microsatellite genetic loci from teratomas to their glial implants. It demonstrated that the glial implants were maternally derived and did not originate from the teratomas. 6 Investigators theorized that the nodules arose from the metaplasia of pluripotent peritoneal Müllerian stem cells rather than from implantation of the teratomas. Immunohistochemical stains for GFAP were applied to the equine placental teratoma nodules and to control equine brain tissue. Whereas equine brain astrocytes were positive, placental nodules were negative (data not shown). Because of the morphology and phenotype differences, it was concluded that the equine lesion differed from gliomatosis peritonei in humans. Comparison of genetic sequences from the placental teratoma nodules and the mare was not performed but may be illuminating in future cases.
Teratomas have been postulated to develop from parthenogenesis of a germ cell after the first meiotic division. 5,14,25 Other theories, such as mitosis after the fusion of germ cells, also have been proposed. 10 In a normal embryo, primitive germ cells originate from the dorsal wall of the yolk sac, migrate through the primitive gut wall into the mesentery, and then travel to the dorsal body wall and genital folds. 18 Aberrant germ cells may instead migrate from the root of the mesentery to other locations, such as the mediastinum, the pineal gland, or the placenta. Subsequent growth and differentiation of the germ cells can give rise to teratomas in these locations. The close approximation of the evaginated primitive gut with the umbilical cord and the placenta during the first several months of gestation may promote placental migration of germ cells in some instances. Supporting this theory is the occasional finding of mature intestinal epithelium in the umbilical cord during early fetal development. 7
The effect of a placental teratoma on human pregnancy is often minimal. Parturition is normal or, in some cases, premature. 3,17,20,22 Babies from placentas containing a teratoma are usually normal. Reports of human placental teratomas describe a single nodule, several centimeters in diameter, between the chorion and the amnion. 7,11,27 Tumors consist of multiple germ layers or, in some cases, are monodermal. 12 In contrast, this equine placental teratoma consisted of multiple nodules disrupting 50% of the placenta, which resulted in abortion. The topological differences of this equine placental teratoma from human placental teratomas, as well as the type of placentation (diffuse epitheliochorial versus discoid hemochorial, respectively), may have compromised the placental exchange of nutrients and metabolic products sufficiently to have resulted in abortion. The long-term effects of the teratoma on the mare appear to be negligible. The mare was rebred the following season and foaled successfully.
Footnotes
Acknowledgements
We graciously thank Dr. Suzanne Quenneville for submitting this case and providing the history and clinical follow-up of the mare.