
Abstract
A tumor located in the optic nerve extended through the optic chiasm, involving the hypophysis and the hypothalamic area in a 3.5-year-old male Boxer dog. It showed a biphasic pattern in which numerous highly fibrillated, well-differentiated pilocytic areas were intermingled with pleomorphic, microcystic tumor tissue. Immunohistochemical analysis of the tumor revealed that most of the neoplastic cells were immunore-active for S-100 protein, with less intensity for glial fibrillary acidic protein (GFAP) and vimentin. A diagnosis of anaplastic astrocytoma was made on the basis of the histopathologic findings and immunohistochemical results. Moreover, there were similarities with the malignant variant of pilocytic astrocytoma described in human adults as an optic chiasmatic-hypothalamic glioma.
Keywords
Glioma tumors in dogs are among the common primary tumors of the central nervous system (CNS), and they tend to occur in aged patients, with the brachycephalic breeds being more predisposed. 7,9 Canine astrocytomas and oligodendrogliomas each have about the same occurrence of about 10% of all primary tumors. 7 Astrocytomas usually involve the cerebral hemispheres, predominantly in the temporal-pyriform region, and the diencephalon, but they may be located in almost any area of the CNS. 7 Optic pathway gliomas in animals are extremely rare, 13 and they almost always adopt an anaplastic form.
In human beings, optic pathway gliomas account for approximately 3–5% of intracranial gliomas, occurring mainly in childhood. 11 In many instances, these gliomas are part of a more diffuse neoplasia involving the optic chiasm and the hypothalamus, classified as optic chiasmatic-hypothalamic gliomas (OCHGs). 11
A 3.5-year-old male Boxer dog was presented to the Centro Veterinario Prado de Boadilla with progressive blindness affecting the left eye. A mass involving the optic nerve and optic chiasm, progressing caudally up to the hypophyseal area and compressing ventrally the diencephalon, was detected by magnetic resonance imaging. After complete necropsy, the left eye and the corresponding optic pathway and samples of the intracranial tumor were sent to our neuropathology service. The optic nerve was grossly enlarged and distorted by growth; on sectioning, the cut surface was grayish, with a low consistency, and showed hemorrhagic and necrotic foci (Fig. 1). The mass seemed to protrude through the optic disk into the vitreous body. The intracranial mass was poorly circumscribed, with an appearance similar to that of optic nerve mass. Samples of the tumor were fixed in neutral buffered 10% formalin and embedded in paraffin. Serial 3-µm-thick sections were made and stained with hematoxylin and eosin (HE) as well as Masson's trichromic stains. Sections also were examined for reactivity to a panel of immunohistochemical markers (Table 1), using a commercial avidin–biotin–peroxidase complex kit (Dako Corporation, Glostrup, Denmark). Biotinylated mouse, rabbit, and goat antisera (Dako) were used as secondary antibodies and 3′3-diaminobenzidine tetrahydrochloride–hydrogen peroxide as the chromogen.
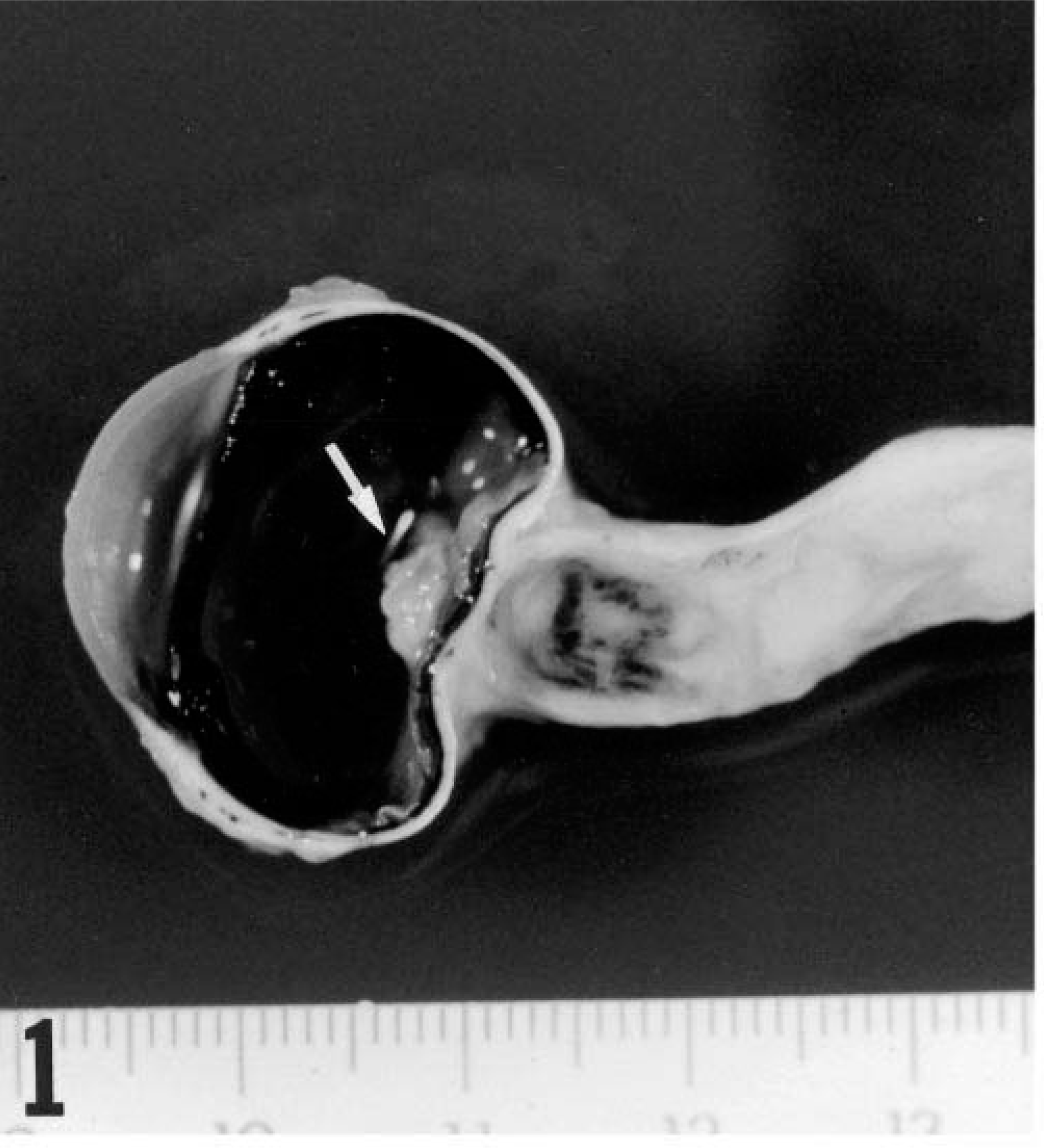
Left eye and optic nerve; dog. The optic nerve appears enlarged and distorted by growth and includes dark areas corresponding to necrosis and hemorrhages. Note the protrusion of the tumor through the vitreous body (arrow).
List of antibodies used in immunohistochemistry (IHC) to characterize the neoplastic cell population and carry out the immunoreactivity evaluation.
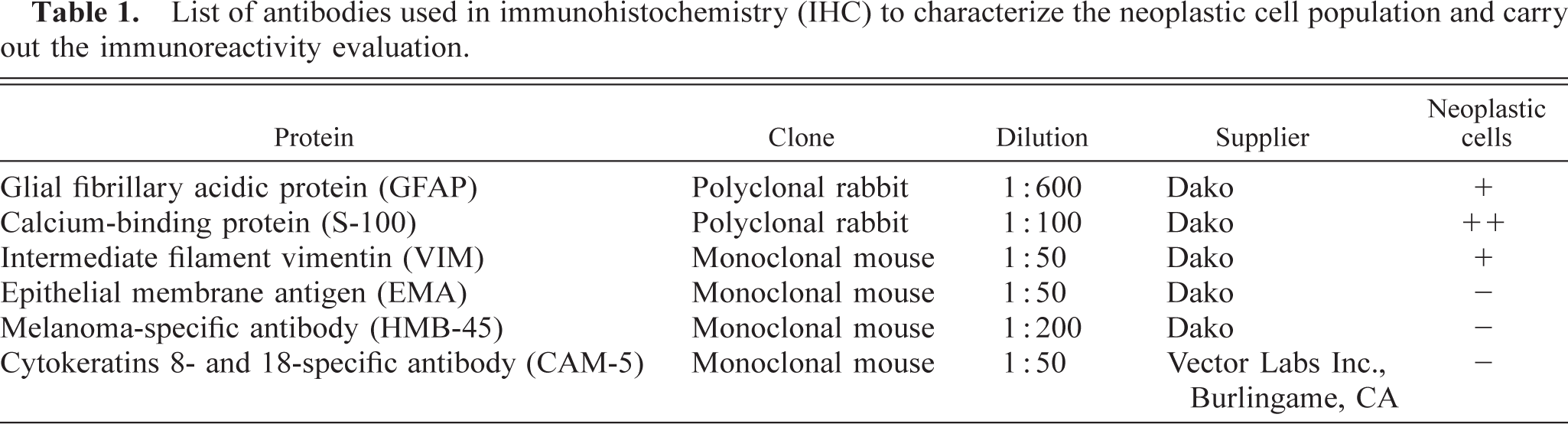
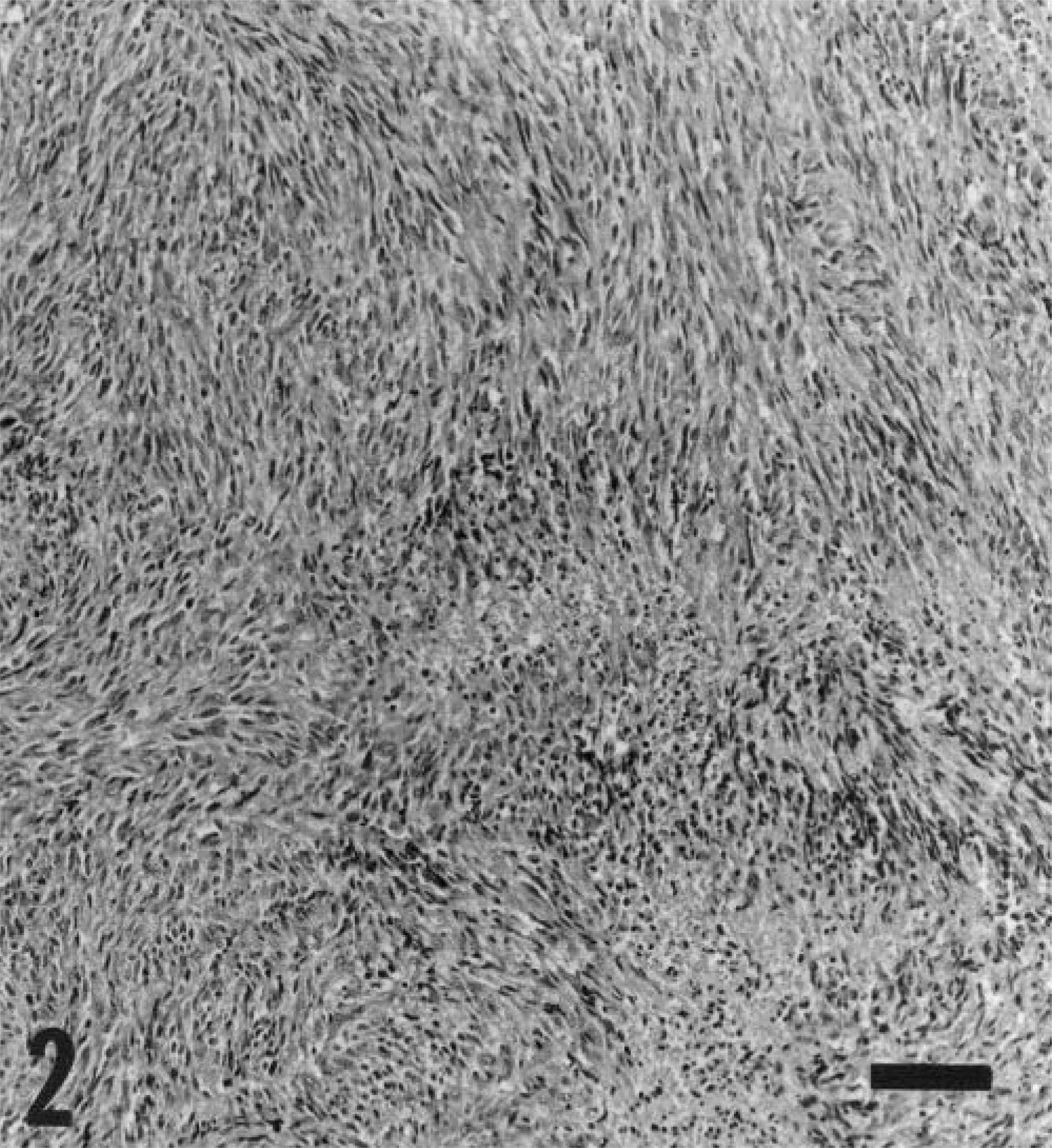
Microscopically, the tumor showed a biphasic pattern. Extensive, highly fibrillated pilocytic areas were intermingled with a second pattern having a loosely microcystic appearance. In the optic nerve, tumor cells had totally replaced nerve fibers without breaching the nerve capsule. In pilocytic areas (Fig. 2) a bipolar fusiform cell with eosinophilic cytoplasm with long processes, resembling those of the “hair-like” (pilos-like) neoplastic astrocytes, predominated, although unipolar cells also were present; both were intermingled with Masson's positive collagen fibers. A remarkable degree of nuclear polymorphism was seen. Microcystic formation was associated with marked changes in morphology: cells became round or stellate, with clear nuclei and scant cytoplasm and with plump or nondiscernible processes, in effect mimicking protoplasmatic astrocytes or oligodendrocytes. Mitosis was scanty in both patterns. Eosinophilic hyaline granules also were present among neoplastic cells. Extensive foci of necrosis and multiple foci of hemorrhages were present. Neoplastic cells infiltrated the optic papilla and the retina, causing its detachment. The intracranial part of the tumor involved the optic chiasm almost in its entirety and progressed caudally up to the hypophysis, compressing the ventral diencephalon and infiltrating adjacent structures such as third ventricles and meninges. In those areas, the tumor was highly cellular with a poor connective component. It had a dense pilocytic pattern occasionally organized as a radially oriented mass around blood vessels. Neoplastic “hair-like” astrocytes with anaplastic changes predominated in it and exhibited nuclear pleomorphism (Fig. 3). Isolated picnotic cells were frequently observed. Mitotic figures were more numerous than in the optic nerve. Eosinophilic hyaline granules were abundant, and some focal multinuclear giant cells occurred. A few microcystic areas were present. Prominent vascular proliferation was observed (Fig. 4). Intracranial neoplasm contained multiple foci of necrosis and hemorrhages surrounded by prominent pseudopalisades of pleomorphic neoplastic cells.
Optic nerve mass; dog. Pilocytic astrocytoma. Neoplastic cells grow in a typically highly fibrillated pilocytic pattern. HE. Bar = 146 µm.
Intracranial mass; dog. The cell that prevailed is a bipolar fusiform cell showing marked nuclear pleomorphism. Note mitosis figures (arrows) and isolated picnotic elongated cells (arrowheads). HE. Bar = 14.6 µm.
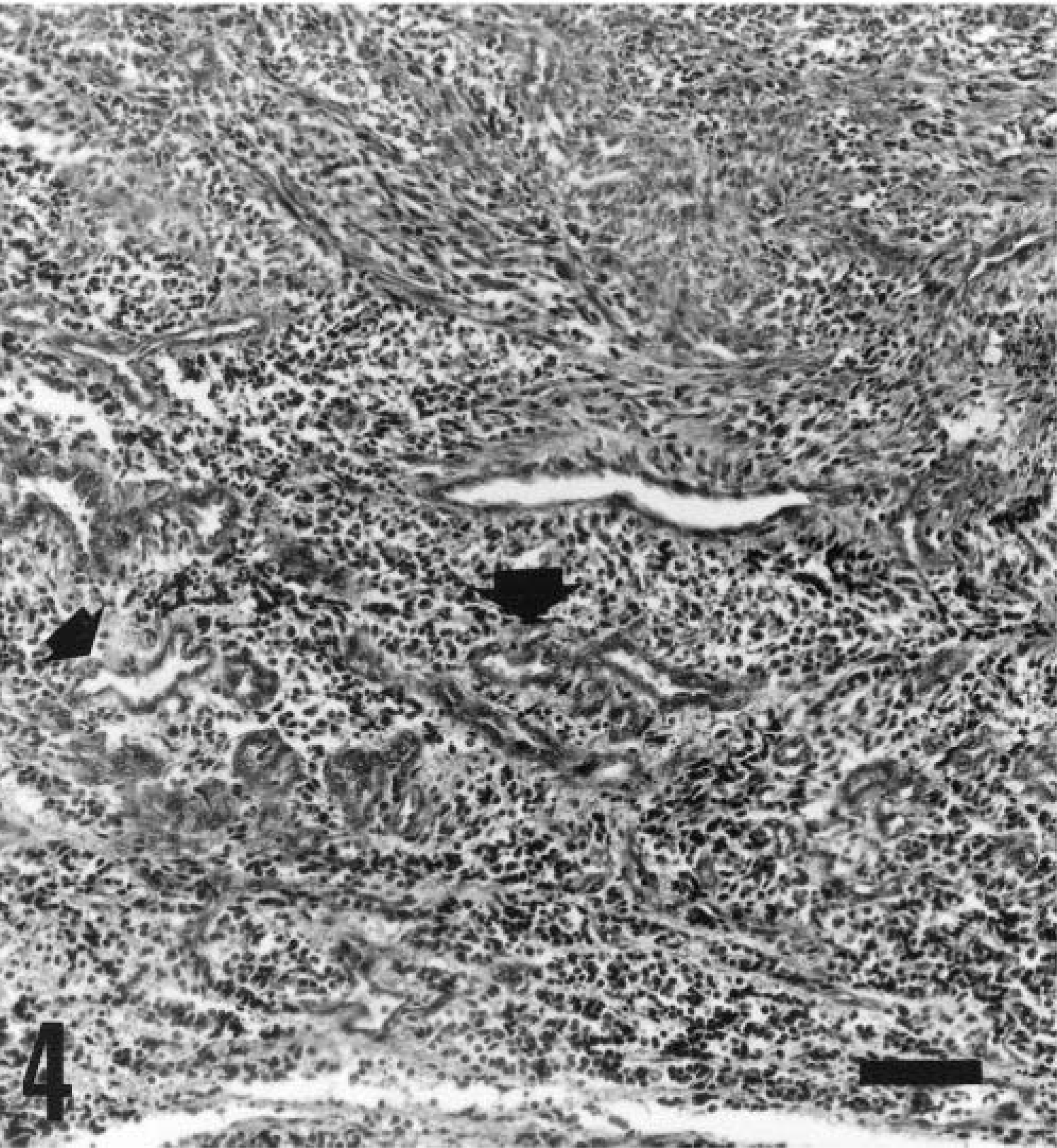
Intracranial mass; dog. Prominent proliferating capillaries indicative of malignancy were observed (arrows). HE. Bar = 93.45 µm.
A diagnosis of anaplastic astrocytoma was made based on the histopathologic findings and immunohistochemical results (Table 1).
Astrocytoma of the optic nerve and retina have been documented in dogs and cats as sporadic, very rare neoplasms. 4 Most primary optic gliomas involving the optic nerve reported in dogs did not show brain involvement. 2,3,6,10 There is only one description of an anaplastic astrocytoma 12 with the same brain structure involvement as that of the tumor described herein. Nevertheless, they differ histologically and immunohistochemically. Our diagnosis of anaplastic astrocytoma was based on the pilocytic-microcystic pattern, high cellularity with marked nuclear pleomorphism, frequent mitosis, necrosis, and prominent neovascularization. The marked positivity shown by neoplastic cells to S-100 and glial fibrillary acidic protein (GFAP) allowed for the confirmation of the glial origin of the neoplastic cells. In less differentiated areas where collagenous fibers were abundant, the majority of neoplastic cells showed marked positivity against the S-100 protein, against Vimentin, and, to a lesser degree, against GFAP. Moreover, neoplastic cells do not react against EMA, HMB-45, and CAM-5 antisera.
In human beings, 8,11 the term anaplastic astrocytoma refers to malignant astrocytomas with a pilocytic-type histopathologic background. Two variants of human pilocytic astrocytoma are recognized. 8 The first is an adult type, with closely packed, interwoven bundles of elongated cells, on which a Masson stain reveals high amounts of collagen; the second, a juvenile type, in which fibrillary patterns are mixed with extensive microcystic areas, has no tendency to form an intercellular connective matrix. The two variants show differing degrees of positivity to GFAP, depending on their differentiation. 5,8,11 Our tumor showed more similarities to the human adult type of pilocytic astrocytoma. In humans, tumors of the optic pathways rarely involve the retina, but approximately 50–80% of all human optic pathway gliomas involve the chiasm or hypothalamus. 1 Because retina involvement would appear not to be rare in optic tumors in dogs, 2,8,11,13 in our opinion, detachment of the retina of this dog was due to the optic nerve tumor's protrusion. OCHG is the term applied to human optic pathway gliomas also affecting hypothalamic and hypophyseal areas. 11 Histologically, OCHGs in children are typically benign pilocytic astrocytomas (World Health Organization [WHO] Grade I), whereas in adults they may exhibit the characteristics of a highly malignant tumor best described as anaplastic astrocytoma (WHO Grade III). 1,5,8,11 The glioma described here shares histological characteristics with the human malignant astrocytoma, pilocytic type, described in adults. 1,5 In our opinion, based on the similarities of this tumor to its counterpart in humans, OCHG should be recognized as a type of anaplastic optic nerve glioma in veterinary medicine.