
Abstract
A 12-year-old crossbred female cat was presented for necropsy with a history of anorexia, ataxia, convulsions, and blindness. Grossly, a whitish, firm, and well-circumscribed nodule with an irregular surface of approximately 1.5 cm in diameter was observed in the right dorsal, parietal, and occipital lobes of the brain. Histologically, the tumor was composed of neoplastic astrocytes forming irregular interweaving sheets and bundles. These cells were elongated, spindle-shaped, and bipolar, and some had clear cytoplasm and a dense nuclear chromatin pattern. Extensive areas of cartilaginous and osseous metaplasia were observed. By immunohistochemistry, the neoplastic cells were found to be markedly positive for S-100 protein and glial fibrillary acidic protein. On the basis of morphologic and immunohistochemical features, the diagnosis of pilocytic astrocytoma was made.
Primary tumors of the central nervous system (CNS) are rarely reported in domestic animals, except in the dog.5,6,10,15 Meningioma7,11 and lymphoma account for most of the CNS neoplasms in cats, whereas astrocytomas are extremely rare.15,16 Zaki and Hurvitz16 reported only one case of astrocytoma in 87 spontaneous neoplasms of the CNS in cats. This tumor can occur in all domestic species, mainly in brachycephalic breeds of dogs. Usually, astrocytomas occur in older animals. Nonetheless, breed or sex predilections have not been determined.8
This report describes the pathologic and immunohistochemical findings of a pilocytic astrocytoma in a 12-year old, crossbred, female cat. The animal was previously euthanized on account of anorexia, ataxia, convulsions, and blindness and was admitted to the Veterinary Teaching Hospital of the Federal University of Minas Gerais for necropsy. The owner reported that the animal was being treated with a home-made sucrose plus isotonic sodium chloride solution orally and that the clinical course lasted 4 weeks.
At necropsy, gross pathologic findings were limited to the brain. A whitish, firm, and well-circumscribed nodule, with an irregular surface of approximately 1.5 cm in diameter, was observed in the right dorsal, parietal, and occipital lobes of the brain without macroscopic involvement of the meninges or periosteum of the skull. In addition, an exostosis of the skull of approximately 1 cm in diameter was detected adjacent to the tumor mass, but the neoplastic nodule was not connected to the exostotic bone. Brain neoplasm samples were fixed in buffered 10% formalin and routinely embedded in paraffin. Four-micrometer sections were stained with hematoxylin and eosin (HE) and Masson's trichromic.13
In order to establish a final diagnosis of the neoplasm, the following antibodies were applied in appropriate dilutions on the brain sections: anti-protein S100 (polyclonal, 1:100; Dakopatts, Copenhagen, Denmark) and anti-glial fibrillary acidic protein (GFAP) (polyclonal, 1:400; Dako, Carpinteria, CA). The streptavidin–biotin–peroxidase complex (Dako) and diaminobenzidin (Sigma Chemical Co., St. Louis, MO) were used as the detection system.4 Sections were counterstained with Harris hematoxylin.
Microscopically, neoplastic astrocytes were arranged in irregular interweaving sheets and bundles (Fig. 1). The neoplastic tissue was encapsulated because abundant connective tissue was evidenced in sections stained with Masson's trichromic (data not shown). Astrocytes were elongated, spindle-shaped, and bipolar, and some had clear cytoplasm and a dense nuclear chromatin pattern (Fig. 1). Mitotic figures were rare. In addition, extensive areas of cartilaginous and osseous matrix were observed (Fig. 2). By immunohistochemistry, the neoplastic cells were found to have a strong and multifocal labeling for S-100 protein (Fig. 3) and GFAP (Fig. 4). In areas of metaplasia a strong labeling for S-100 protein was also detected. Astrocyte processes strongly labeled for GFAP were observed at the margin of the neoplastic tissue in the brain. This finding served as an internal positive control for GFAP.
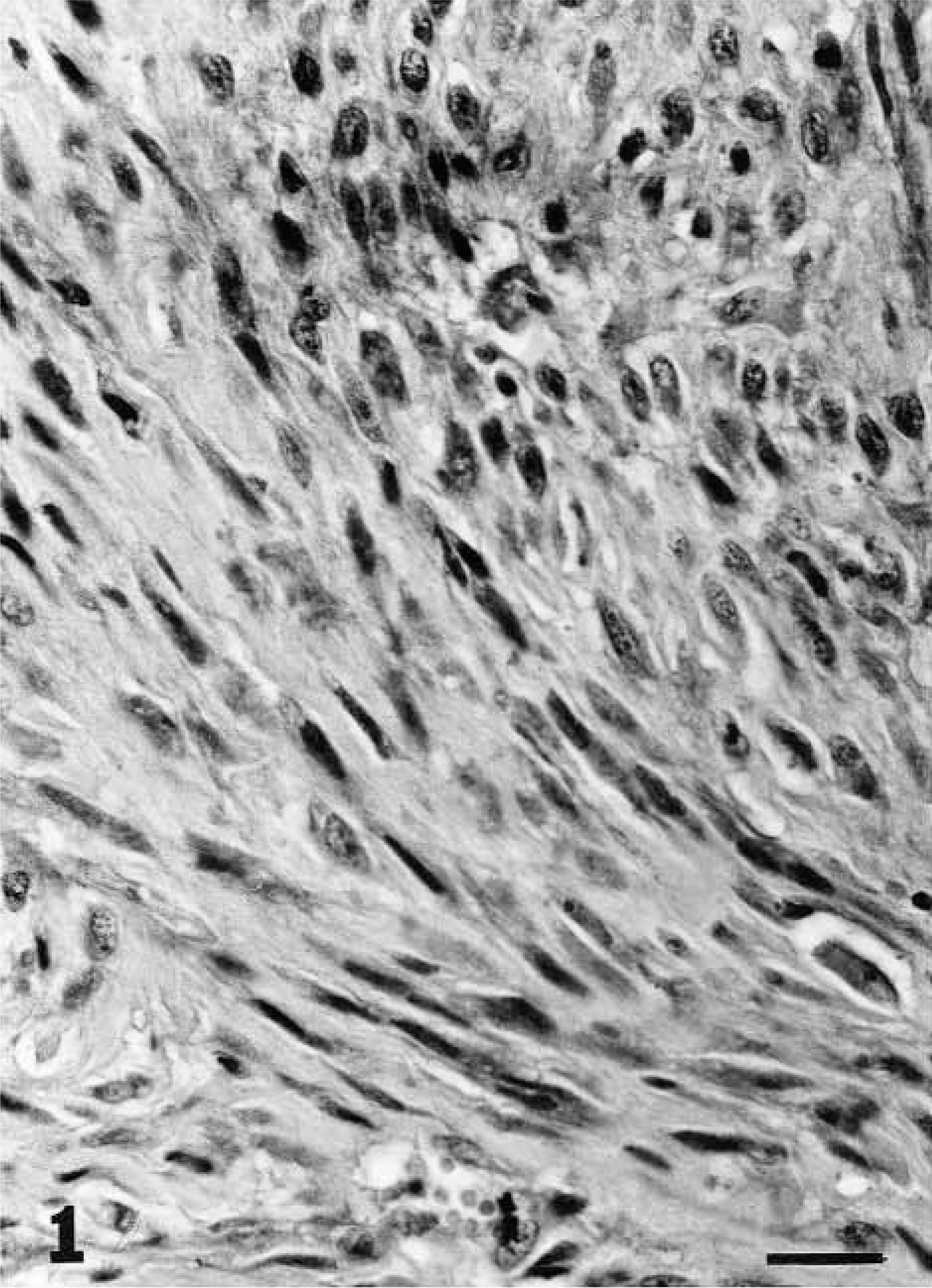
Brain; cat. Pilocytic astrocytoma. Elongated bipolar spindle-shaped astrocytes are arranged in interweaving sheets and bundles. HE. Bar = 18.66 μm.

Brain; cat. Pilocytic astrocytoma. Extensive area of cartilaginous and osseous metaplasia. HE. Bar = 46.66 μm.
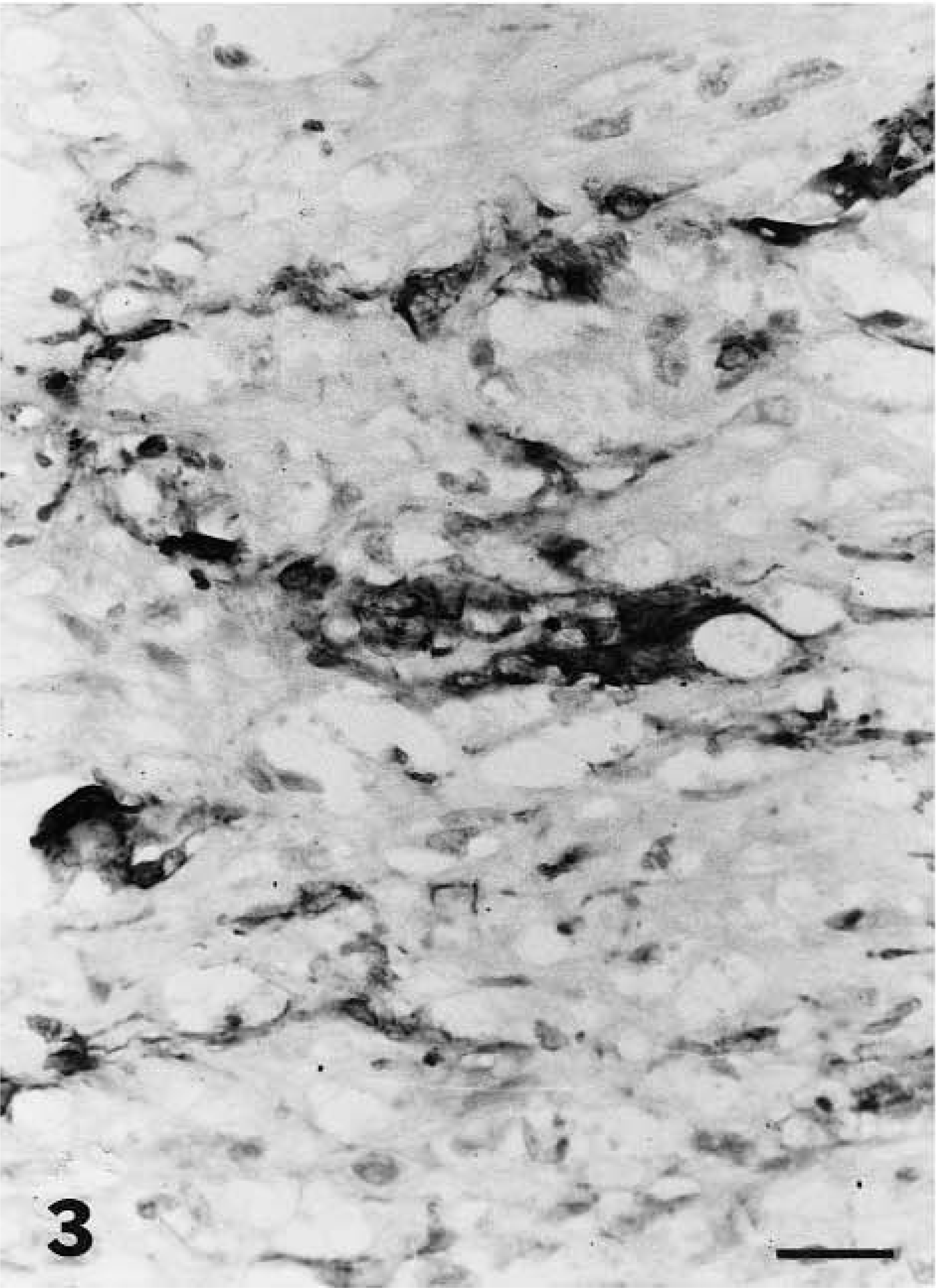
Brain; cat. Pilocytic astrocytoma. Neoplastic astrocytes stained positively for S-100 protein. Streptavidin–biotin–peroxidase method, Harris hematoxylin counterstain. Bar = 23.33 μm.
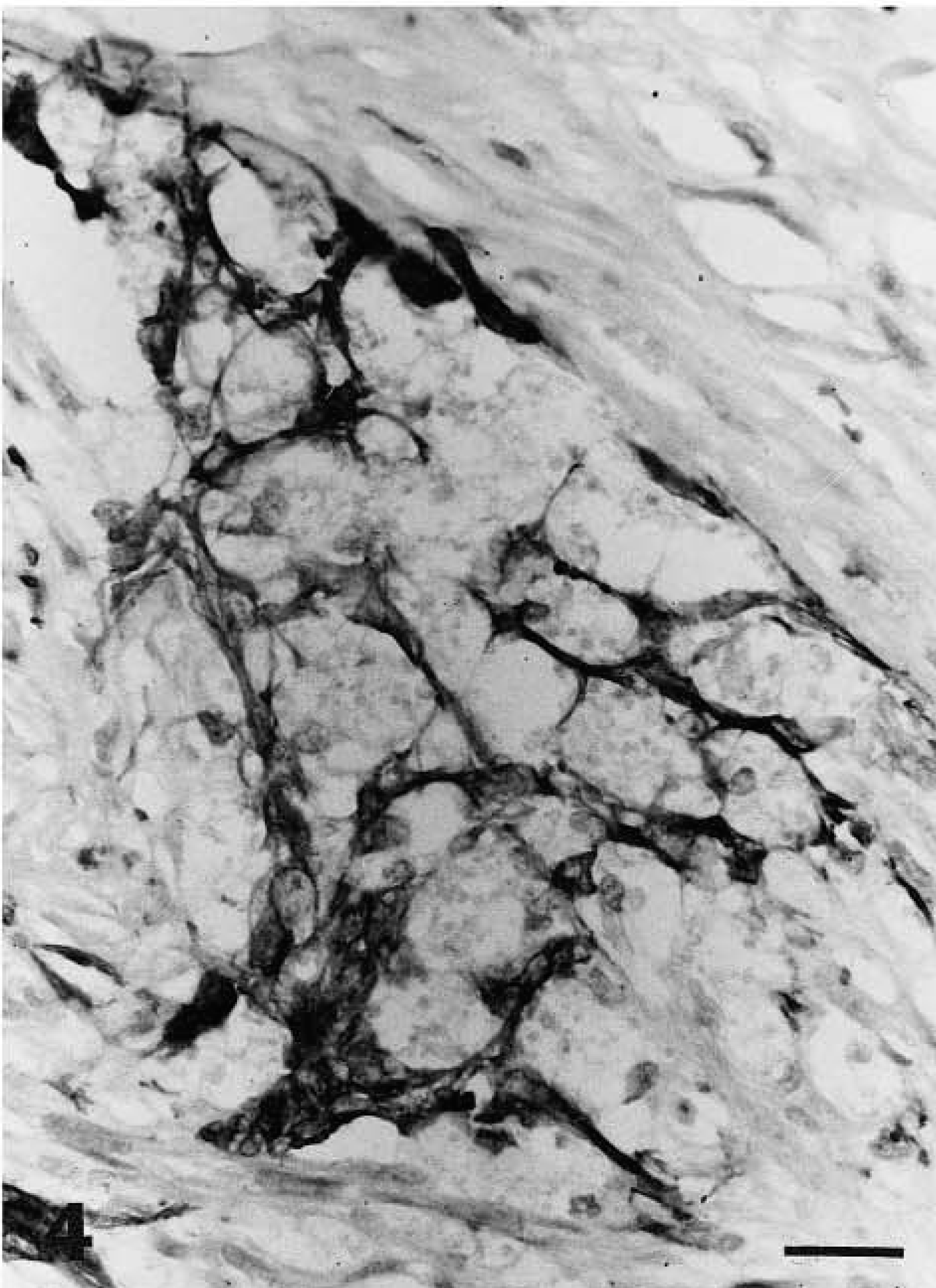
Brain; cat. Pilocytic astrocytoma. Neoplastic cells showed prominent immunoreactivity for GFAP. Streptavidin–biotin–peroxidase method, Harris hematoxylin counterstain. Bar = 31.11 μm.
Astrocytomas may be derived from fibrillary or protoplasmatic astrocytes, and fibrillary astrocytomas account for the majority of these neoplasms.15 These tumors are divided into differentiated and undifferentiated types. The differentiated category includes the fibrillary, protoplasmic, gemistocytic, and pilocytic types. The undifferentiated category includes the glioblastoma multiforme, which is a malignant form of astrocytic neoplasm.10
With the exception of lymphomas, intracranial neoplasms usually develop in cats older than 9 years of age, which is the age range recorded in this case. In human subjects pilocytic astrocytoma occurs mainly in children and young adults.2,3
Brain tumors in cats present a diagnostic challenge to the veterinary practitioner. Presenting signs can be diverse and usually have an insidious onset.8 Possibly, the anatomic location of the tumor nodule was responsible for the clinical signs observed in this animal because the occipital and parietal lobes of the cortex were affected. The gross pathologic findings described in this report may be related to the visual and locomotion disturbances observed clinically. Some fast growing tumors may compress the adjacent nervous tissue causing necrosis and edema.14 But those features were not observed in the present case.
The presence of connective tissue and cartilaginous and osseous metaplasia associated with the neoplasm made microscopic interpretation more difficult. Therefore, immunohistochemical techniques were critical for establishing the diagnosis. The presence of bone and cartilage in cerebral gliomas is not common. That tissue may result from metaplastic transformation of the connective tissue stroma of the tumor.1,9 More often the stromal metaplasia results in membranous bone, although occasionally cartilage is formed with secondary endochondral ossification.9
Although the genesis of cartilaginous and osseous metaplasia is not known in astrocytomas of domestic animals, this alteration has been randomly observed in humans on account of aberrant differentiation of the neoplasm.12 Necrosis and calcification have been pointed out as necessary precursors that stimulate the differentiation of young fibroblasts into osteoblasts and chondrocytes.9 Neither areas of necrosis nor areas of calcification were detected in the present case.
On the basis of anatomopathologic and immunohistochemical findings, a diagnosis of pilocytic astrocytoma was made.