
Abstract
Four birds in a flock of 125 purebred Crested ducks (Anas platyrhynchos f. dom.) had cerebellar signs of unknown etiology. They had radiographically evident perforations of various sizes in the parietooccipital calvaria. Gross necropsy of euthanatized ducks revealed yellow intracranial masses in the brain of each. Histologically, these masses were intracranial lipomas consisting of univacuolated fatty tissue separated into lobules by strands of connective tissue. The masses had caused serious deformation of the rostral part of the cerebellum, leading to a nearly complete flattening of cerebellar folia, and were interpreted as the cause for the central nervous clinical signs observed. These intracranial lipomas were similar to those previously reported in other animals and humans.
Four birds in a flock of 125 purebred Crested ducks (Anas platyrhynchos f. dom.) had central nervous signs of unknown etiology. As a duckling, duck No. 1 did not demonstrate any clinical signs referable to the central nervous system. At 6 months of age, abnormal equilibrium was present for approximately 1 week, but food and water intake were normal. Thereafter, duck No. 1 had no clinical signs until approximately 8 months of age, when it developed violent ataxia that prevented eating and drinking. At this time, the duck also showed a severe disturbance of balance and convulsions, during which it rotated in a circle for 2 minutes and then was still, with the neck extended towards the back. After a recuperative phase, this duck was clinically normal until the next convulsion. Duck No. 2 started to show a persistent, distinctive left-side posture of the head directly after hatching, which became more pronounced in stressful situations. Tremor of the head and ataxia were not present, and food and water intake were normal. Duck No. 3 had torticollis right after hatching. At 28 days of age, this duck demonstrated severe spontaneous ataxia and incoordination. These signs disappeared after 7 days, but a stress-induced caudal torticollis of more than 180 degrees persisted. Duck No. 4 had violent incoordination and a slight permanent tremor of the head 1 week after hatching.
Multiple pathologic changes in the cranium and the brain are found in Crested ducks and may lead to clinical signs of central nervous disorders.1–4,10,11 Infectious (parasitic infections, Salmonella spp., and paramyxovirus) and noninfectious (vitamine E defiency and tumors) may cause similar clinical signs.7–9 Ducks in this report were initially examined for infectious agents using previously described methods and for cranial and cerebral morphologic alterations using radiography.7,8
No infectious agents were isolated, but radiographs showed various cranial deformations and/or atypical ossified structures in the crest cushions (Table 1). In duck No. 1 the caudal cranium was slightly sunken and interrupted by a smooth-edged perforation about 15 mm in diameter, and there was an isolated 16-mm-long osseous projection in the crest cushion. Duck No. 2 had a bilobed crest cushion at the caudal part of the head. Beyond the thickening of the skin, a persistent 20-mm-diameter fontanel with an irregular margin was present (Fig. 1). The crest cushion of duck No. 3 had an abnormal arched osteophyte inserted in the parieto-occipital cranium and a cranial 4-mm perforation at the occiput. Inside the cranial cavity, there was an ossified 16-mm-long, 2–3-mm-wide growth and a caudally localized circular 12-mm spot. Duck No. 4 had a trilobed crest cushion and a 16-mm-long osteophyte in its parieto-occipital region. The skull of this bird had a 5-mm-diameter calvarial perforation and asymmetry in the axis of rotation at the point of bill attachment. No intracranial soft tissue alterations were seen radiographically.

Head; duck No. 2. Left to right radiograph reveals a large perforation of the calvaria beyond the crest cushion (C), a hypodermal thickening in the parieto-occipital region.
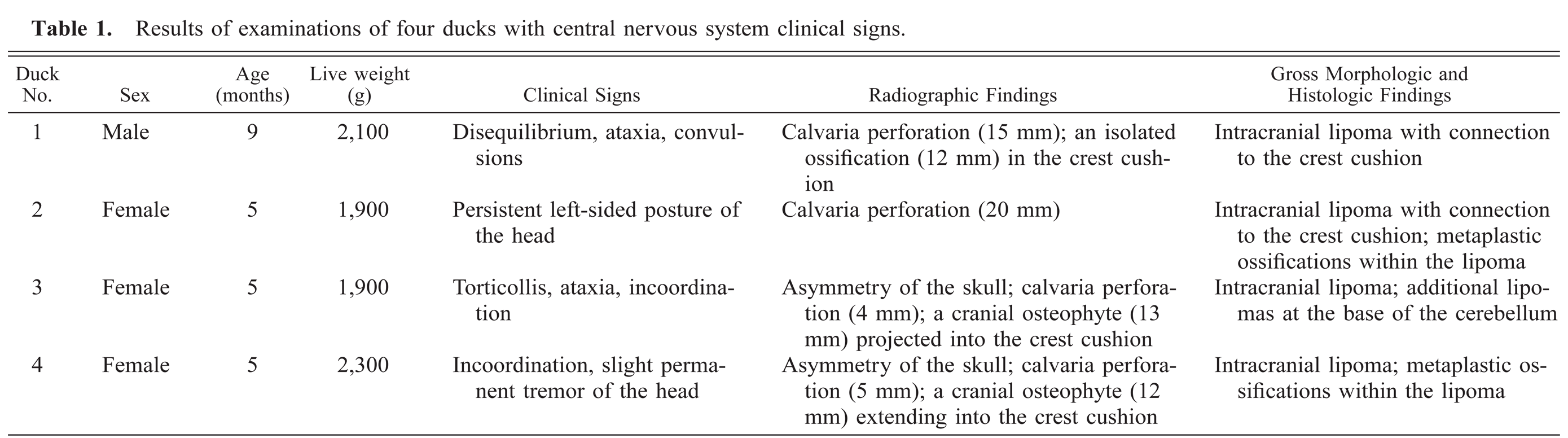
Results of examinations of four ducks with central nervous system clinical signs.
Brains of all four ducks were dissected, and samples of the cerebellum and the adjoining intracranial masses were fixed by immersion in 3.7% formaldehyde, dehydrated, cleared, and embedded in paraffin using routine methods. Sagittal 15-μm sections were stained with hematoxylin and eosin (HE).
Gross morphologic examinations confirmed the antemortem radiographic findings. Additionally, yellow intracranial masses between the telencephalon and the cerebellum at the tentorium cerebelli were present in all four ducks. These masses were smooth, in some cases unevenly shaped, and glassy yellow on cut surface. Masses in duck Nos. 1 and 2 were connected to the crest cushion by a straight-edged calvarial perforation. Histologically, there was massive deformation of the rostral cerebellum, leading to a nearly complete flattening of folia in all four birds (Fig. 2). The cerebellum was compressed by ovoid or cone-shaped encapsulated infiltrations of univacuolated fatty tissue that was lobulated by strands of connective tissue (Figs. 2, 3). Two ducks also had intratumoral small metaplastic ossifications consistant with lipoma ossificans. In duck No. 3, an additional lipoma at the base of the cerebellum contained numerous myelinated nerve fibers (Fig. 3). No histologic alterations were observed in the cerebellar cortex.

Cerebellum; duck No. 2. Sagittal section. An intracranial infiltration (asterisk) causes a nearly complete loss of cerebellar folia of the rostral part of the cerebellum (arrows). Arrowhead indicates fourth ventricle and choroid plexus. HE. Bar = 600 μm.
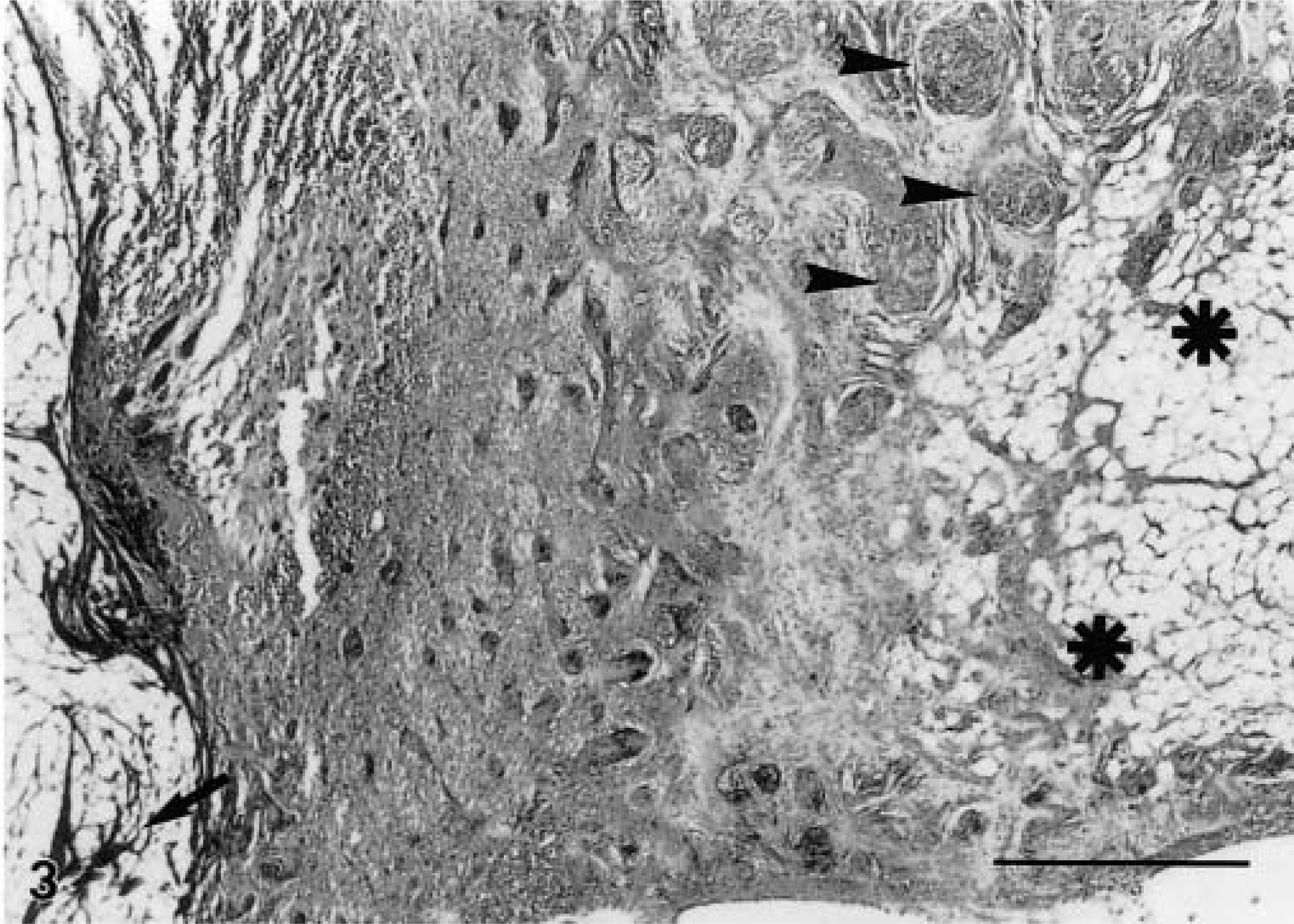
Cerebellum; duck No. 3. Sagittal section. The intracranial infiltration consists of univacuolated fatty tissue lobulated by strands of connective tissue (arrow). The base of the cerebellum is infiltrated by an additional body of fatty tissue (asterisks) with myelinated nerve fibers (arrowheads) in its periphery. HE. Bar = 600 μm.
Intracranial lipomas caused massive deformation of the rostral cerebellum and compression of the cerebellar folia in these affected ducks. These deformations likely produced the observed clinical signs because of increased intracranial pressure. Intracranial lipomas are very rare but have been described in humans and several other mammal species.5,6,14 In humans, they are very often asymptomatic, but seizures, headache, mental retardation, and behavioural disorders have been described in affected children and in adults.6,13
Intracranial fat bodies occur in 82.3% of domestic ducks with feather crests.1 The gross and histologic appearance of these intracranial fat bodies is similar to that of intracranial lipomas reported in humans and other mammals.5,6,12,14 Paradoxically, intracranial lipomas are often clinically silent in affected ducks, possibly because the skull is pliable until cranial bone fusion.2,4 Increased cranial volume may delay or avoid increased intracranial pressure by neurocranial enlargement and may account for the rare occurrence of central nervous system clinical signs in spite of the high incidence of intracranial lipomas in this breed of ducks.1 However, lipoma-induced central nervous clinical signs can appear previous to suture closure in humans and other animals.5,6,10,11,13 More subtle neurologic defects may be present in morphologically abnormal Crested ducks.
Intracranial lipomas are usually regarded as congenital malformations and may result from abnormal differentiation of the meninx primitiva, the mesenchymal anlage of the meninges.5,6,13,14 Localization of these lipomas to the tentorium cerebelli in Crested ducks agrees with this hypothesis. The high incidence of intracranial lipomas in Crested ducks points to either a linkage between their formation and that of feather crests or to pleiotropic effects of the gene for crests. The frequent occurrence of intracranial lipomas in Crested ducks indicates that these ducks may be useful as a model for the study of the development of intracranial lipomas in humans.
Footnotes
Acknowledgements
This study was supported by the Federal Ministry of Consumer Protection, Food and Agriculture of Germany.