
Abstract
Malignant neuroendocrine carcinoma of the skin (Merkel cell tumor) was diagnosed in an 18-year-old spayed female Maine Coon Cat. The diagnosis was made on the basis of morphologic and electron microscopic findings. The cat was euthanatized 321 days after surgical excision of the tumor. The tumor's malignancy contrasted with the benign nature of Merkel cell tumors reported in dogs and was consistent with the malignancy of Merkel cell tumors reported in humans.
Merkel cells are the neuroendocrine cells of the skin, a rare component of the normal follicular epidermis. In hair follicles, a few Merkel cells are always present in the bulge of the isthmus. Merkel cells are widely dispersed in the skin, adnexa, oral cavity, and other sites. 2,6
Merkel cell carcinoma in humans is considered to be a relatively high-grade malignant tumor; 50–66% of patients have regional lymph node metastasis. 9–11 This tumor has also been reported at other sites, such as the oral cavity, eyelid, and ear canal, in addition to the skin. 4,5
In companion animals, Merkel cell carcinoma of the skin with metastasis was first described in a 14-year-old dog in 1983. 1 Four cases of Merkel cell tumor of the oral cavity and 20 cases of the skin have been reported in dogs. 7,12 All Merkel cell carcinomas identified in dogs have been considered benign except one. 1,3,7,12 To the best of our knowledge, this is the first report of Merkel cell carcinoma in a cat.
An 18-year-old spayed female Maine Coon Cat was referred to the Animal Medical Center (New York) with a diagnosis of cutaneous lymphoma. The cutaneous mass was 1 cm in diameter, was reported to have been growing for 120 days, was located in the dorsolateral cervical area, and had been resected. Sections of the tumor prepared routinely for histopathologic examination were reviewed by one of us (A. K. Patnaik). The diagnosis was changed to neuroendocrine carcinoma with involvement of the margins.
Ninety-nine days after the first surgery, a 1.5-cm recurrent lesion was seen at the surgical site, and there were two smaller satellite lesions close to the surgical site. The recurrent tumor and the prescapular lymph node were resected. Radiographs showed cardiomegaly but no lesions in any of the visceral organs, including the lungs. Ultrasound revealed a polypoid mass of 0.7 × 0.8 cm in the gallbladder, but no lesions were observed in any other organs.
Fifty-eight days after the second resection, the cat was reexamined because of coughing. Radiographs showed a pulmonary mass in the left lateral lobe. The gallbladder mass remained unchanged, as revealed by ultrasound examination. The cat was treated with thalidomide (25 mg every 24 hours), an antiangiogenic agent.
Ninety-three days after the second surgery (196 days after the first), the tumor recurred (4.3 cm) at the site. Radiographs showed multiple pulmonary nodules and a mass at the base of the heart and mediastinum. The coughing diminished but the tumor did not decrease in size, so the dosage of thalidomide was increased (25 mg every 12 hours). No response was observed, even after the higher dosage. The lesions in the lungs and mediastinum progressed. The cat was euthanatized 321 days after the first resection. Necropsy was not permitted.
Tissues were fixed in 10% buffered formalin, routinely processed, and stained with hematoxylin and eosin (HE). One section was available from the first resection. Small pieces of tissue from the second resection were processed for electron microscopic examination. Additional 3-µm sections were immunohistochemically stained by use of a supersensitive multilink immunodetection system, following the instructions of the manufacturer (Biogenex, San Ramos, CA). The sections were stained with commercially available antibodies against AE1/AE3, neuron-specific enolase (NSE), synaptophysin, somatostain, serotinon, gastrin, and S100 protein, with appropriate controls for each.
The morphologic features of the various biopsy specimens were similar, except that the recurrent and metastatic lesions looked more aggressive than the primary lesion. The infiltrating dermal and subcutaneous lesions were characterized by groups and sheets of round to oval cells separated by thin fibrovascular or vascular stroma. In other areas, close to the necrotic areas, the stroma was thickened and eosinophilic. Focal areas with neoplastic cells in rows and rarely in rosettelike structures were observed.
The neoplastic cells were round to oval and hyperchromatic; and their nuclei had scattered chromatin and prominent nucleoli, with scanty eosinophilic cytoplasm. The mitotic figures ranged from zero to two per high-power field in the primary lesion and from five to eight per high-power field in the recurrent and metastatic lesions (Fig. 1). There were large areas of tumoral necrosis with scattered blood vessels containing perivascular arrangement of neoplastic cells. In the first biopsy, the neoplastic cells extended to a few adjoining hair follicles and adnexal structures, partially or completely replacing the follicles (Fig. 2). The lymph node metastasis replaced the lymph node except for a few subcapsular follicles.
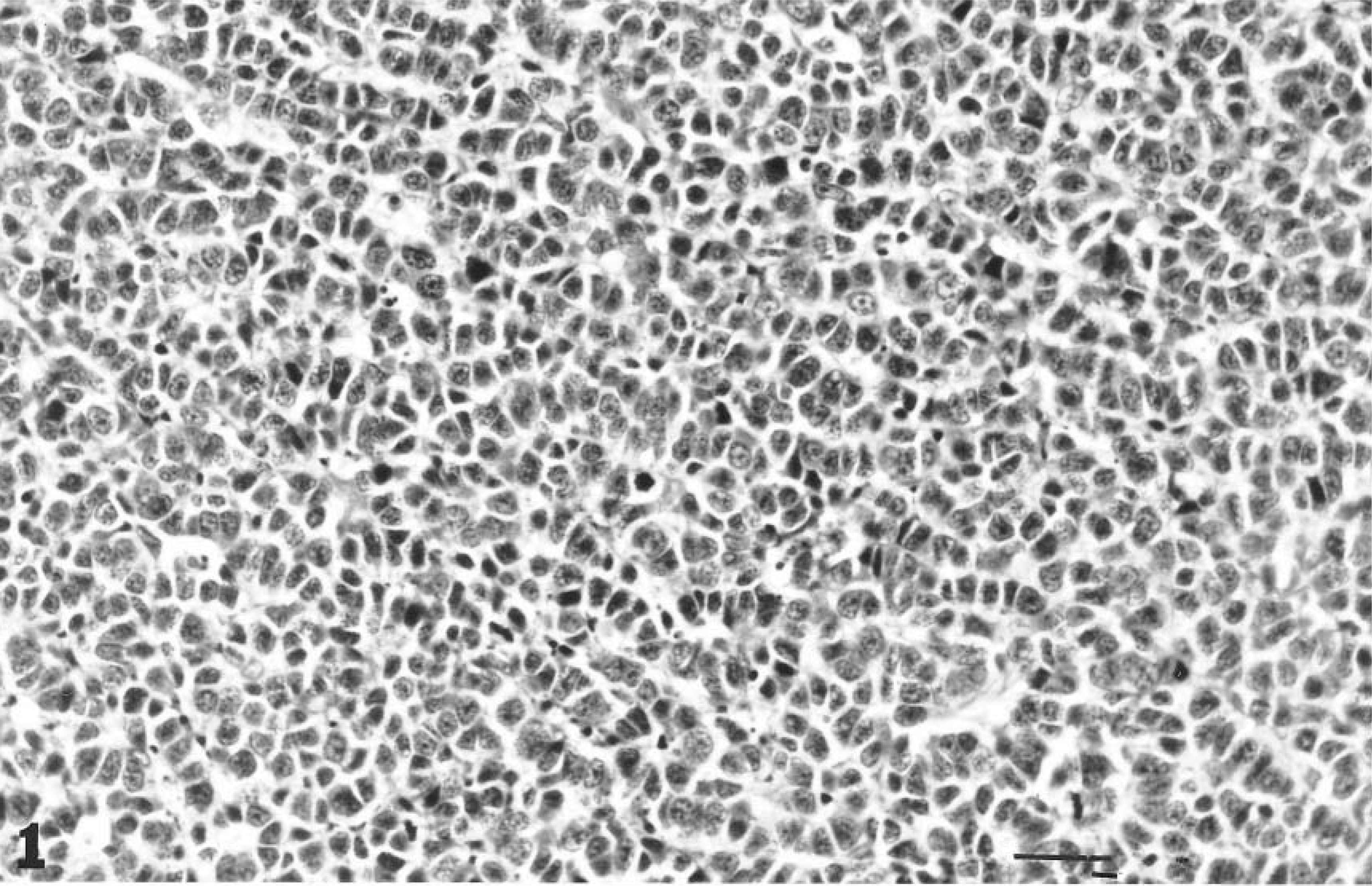
Recurrent Merkel cell carcinoma; cat. Anaplastic neoplastic cells with mitotic figures and indistinguishable vascular stroma. HE. 1 cm = 20 µm.
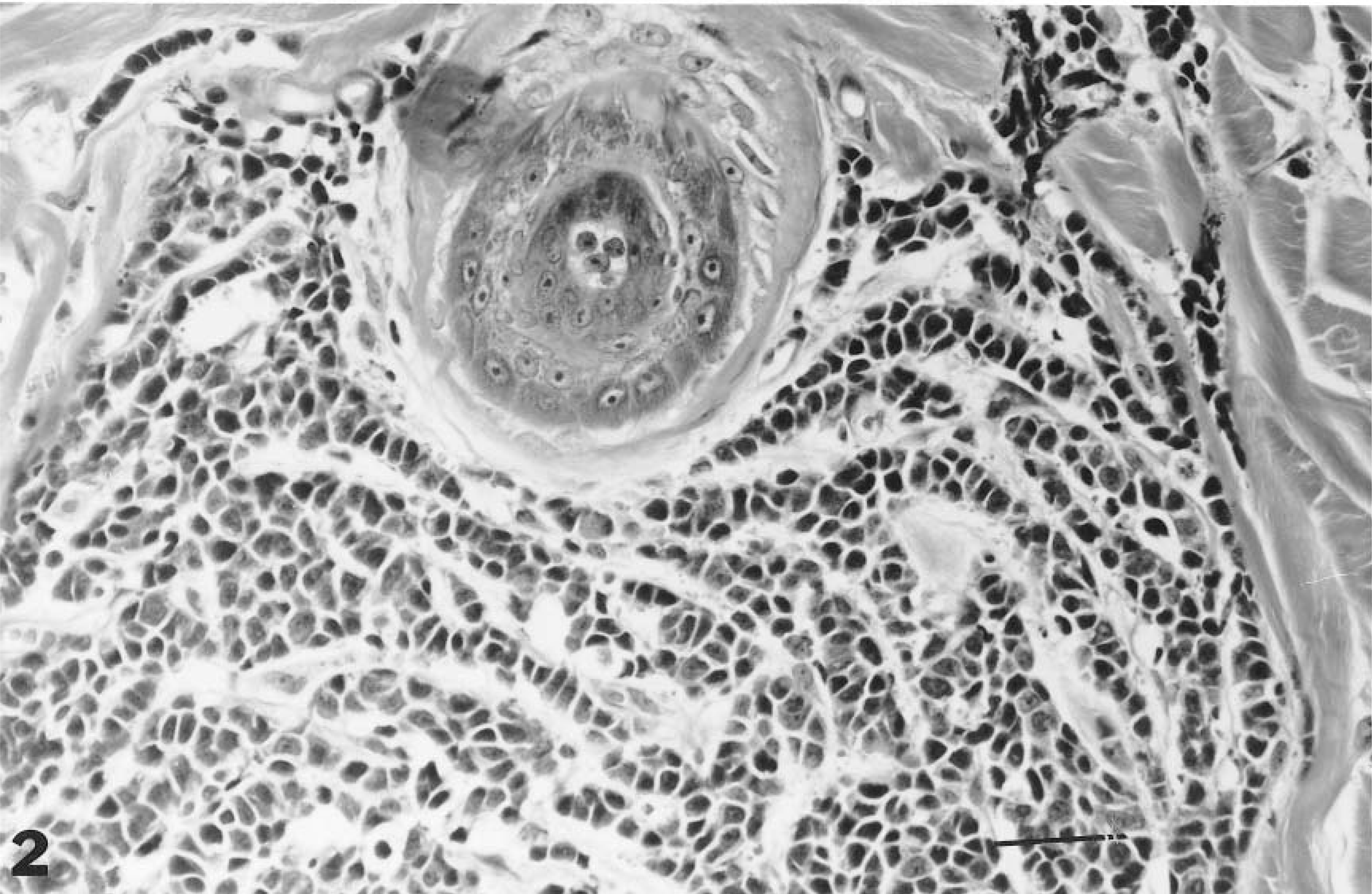
Merkel cell carcinoma; cat. Perifollicular infiltration of neoplastic cells in the skin. HE. 1 cm = 40 µm.
Immunohistochemically, the neoplastic cells from specimens of the recurrent lesion did not react to any of the antibodies tested, except for a minimal reaction to NSE.
The specimen submitted for ultrastructural evaluation consisted of sheets of somewhat poorly preserved cells with uniform round nuclei. These cells were joined by scattered small desmosomes (Fig. 3). The cytoplasm contained scattered, round, dense-core neurosecretory granules with a mean diameter of 110 nm and pleomorphic mitochondria (Fig. 4).
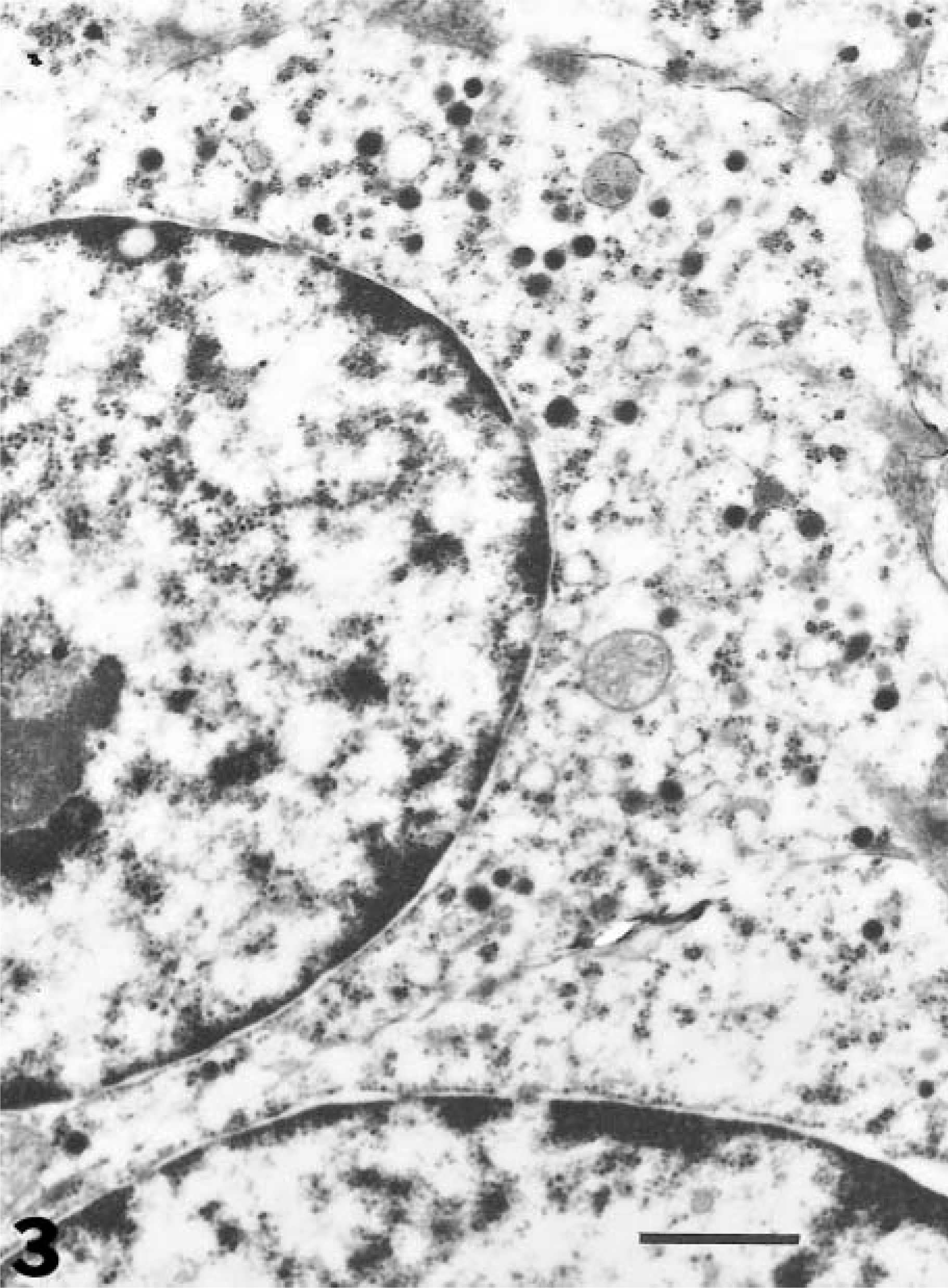
Electron micrograph. Merkel cell carcinoma; cat. Portions of two tumor cells revealing uniform nuclei and cytoplasmic, electron-dense neurosecretory granules. Bar = 1.0 µm.
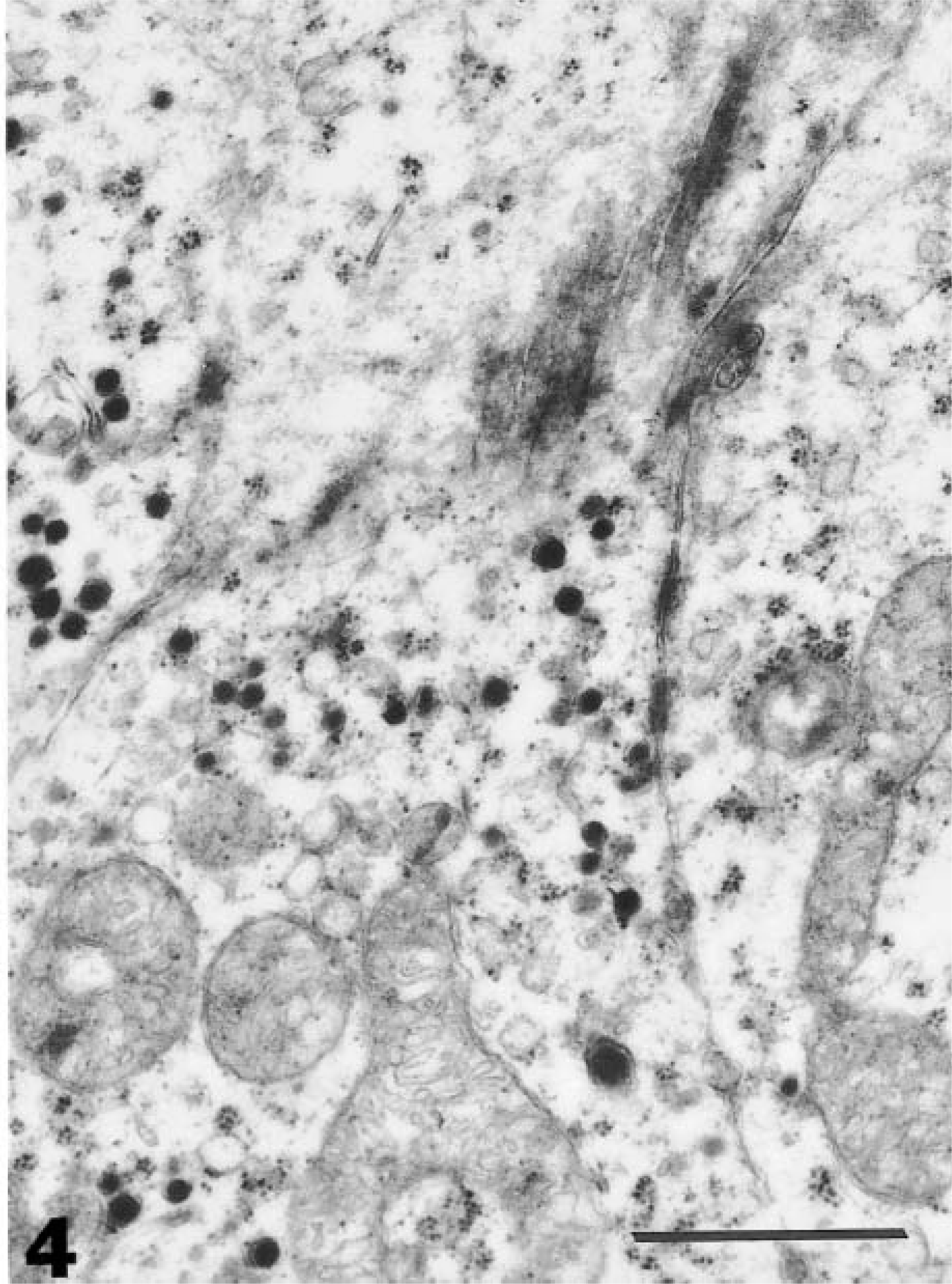
Electron micrograph. Merkel cell carcinoma; cat. Note intercellular junctions, pleomorphic mitochondria (bottom), and neurosecretory granules with an average diameter of 110 nm. Bar = 1.0 µm.
The final diagnosis of this tumor was made on the basis of typical peritheliomatous arrangement of small hyperchromatic cells and the presence of intracytoplasmic dense-core neurosecretory granules as revealed by electron microscopy. Morphologically and biologically, this malignant tumor with progressive metastasis was unlike most cases of Merkel cell carcinoma described in dogs. 1,3,7,12 The Merkel cell carcinoma in this cat is similar, in many respects, to that found in humans; most of these human tumors are considered malignant. 9–11
The differential diagnoses considered in this case were cutaneous lymphoma, melanoma, and metastatic neuroendocrine carcinoma of other sites. Cutaneous lymphomas are usually multicentric. Cutaneous malignant melanomas are uncommon in cats and are clinically nonaggressive. 8 The epidermal changes in T-cell lymphoma (e.g., upper dermal infiltrate and Pautrier microabscess) and melanoma (e.g., junctional changes) should differentiate these tumors from Merkel cell carcinoma.
Metastatic neuroendocrine carcinoma of other sites was eliminated from the differential diagnosis because the cat did not have any other tumor except for a mass in the gallbladder at the time of examination. The mass in the gall bladder remained stationary throughout the case study, and it was considered to be a polyp.
Normally, Merkel cells in the skin are present in the hair follicles. 6 Partial and complete involvement of some of the hair follicles adjoining the mass lesion suggest that these follicles could have been the primary site.
Footnotes
Acknowledgements
We thank Mrs. R. Petter and Ms. C. MacMurray for their editorial assistance.