
Abstract
Actinomyces sp. are commensal, filamentous, gram-positive, acid-fast-negative bacteria that can cause pyogranulomatous inflammation in animals and humans. Central nervous system (CNS) disease is a rare presentation of actinomycosis and is usually due to extension from infected wounds or seeding from distant sites. A dog with progressive, poorly localized neurologic signs had primary CNS actinomycosis without history or evidence of previous trauma or other organ involvement. Histologically, there was a severe pyogranulomatous meningoencephalitis with intralesional filamentous bacteria that were also visible on cytology of the cerebral spinal fluid (CSF) postmortem. Actinomyces sp. was cultured postmortem from the CSF, confirming the diagnosis. This case demonstrates that Actinomyces sp. can be a causative agent of primary CNS disease in dogs.
Actinomyces sp. are gram-positive, acid-fast–negative filamentous bacteria that cause pyogranulomatous infections in dogs, cats, cattle, goats, swine, horses, foxes and human beings. 5 These anaerobic or microaerophilic commensal organisms are found in the oral cavity of animals and humans. 3 Cutaneous actinomycosis is the most common manifestation in dogs, especially in large breed male dogs, and Actinomyces viscosus is the most frequent isolate. 3–5 These infections are usually secondary to perforating injuries caused by bite wounds or foreign bodies. In the most common forms of clinical disease in the dog, the cervicofacial, abdominal, and thoracic regions are involved. 4 7 In humans, central nervous system (CNS) infection with Actinomyces is rare and usually results from extension of an adjacent focus or from hematogenous seeding from a distant site. 7 Risk factors include dental caries or infections, recent tooth extraction, head trauma, gastrointestinal tract surgery, chronic otitis, mastoiditis or sinusitis, chronic osteomyelitis, tetralogy of Fallot, and Actinomyces infection of an intrauterine device. 7 A cerebral abscess is the most common manifestation of human CNS actinomycosis. Other infrequent presentations are meningitis or meningoencephalitis, actinomycomas, subdural empyema, and epidural abscesses. 7 There are two unconfirmed reports of Actinomyces causing CNS disease in animals: spinal meningitis in an Arctic fox and encephalitis associated with hydrocephalus in a dog. 1 6 In both cases, the diagnosis of actinomycosis was assumed based on morphologic characteristics and staining properties of the bacteria on histologic examination. Culture of Actinomyces from the CNS and a definitive diagnosis has not been previously reported in domestic animals.
A 1-year-old intact female German Shepherd Dog was presented to the Veterinary Medical Teaching Hospital of the University of California–Davis for apparent cervical pain of 2 months duration. All vaccinations were current, travel history was restricted to northern California and Idaho, and the animal had been exposed to ticks periodically. No history of trauma was noted. On physical and neurologic examination, the dog was quiet and alert and had pain on movement or palpation of the head and neck. Results from complete blood count (CBC), serum chemistry analysis, urinalysis, thoracic radiographs, abdominal ultrasound examination, joint fluid analysis from several joints, and complete spinal radiographs were within normal limits. Cisternal cerebrospinal fluid (CSF) analysis revealed neutrophilic pleocytosis with increased protein (Table 1). Neutrophils were nondegenerate, and no organisms were seen on direct smears. Aerobic and fungal CSF culture were negative for pathogens. Serologic analyses for common infectious agents such as Cryptococcus sp., Toxoplasma sp., Aspergillus sp., Neospora sp., Coccidioidomyces sp., Ehrlichia canis, E. platys, E. equi, and Rickettsia rickettsii were negative.
A provisional diagnosis of pathogen-free inflammatory CNS disease was made, and symptomatic treatment was initiated with prednisone (1 mg/kg orally twice daily). The animal showed marked clinical improvement over the next 10 days but was presented again after 2 weeks with recurrence of the initial clinical signs. A CBC revealed leukocytosis (32,900 cells/µl, normal = 6,000–17,000 cells/µl) with neutrophilia (23,359 cells/µl, normal = 3,000–11,500 cells/µl) and monocytosis (1,654 cells/µl, normal = 150–1,350 cells/µl). A CSF analysis revealed increases in total nucleated cells and protein (Table 1). Myelography was normal. Aerobic and fungal cultures of the CSF were negative, and anaerobic culture revealed very small numbers of Fusobacterium nucleatum after 8 days of growth. Treatment with enrofloxacin (4.5 mg/kg orally twice daily), metronidazole (8 mg/kg orally three times daily), and prednisone (0.5 mg/kg orally twice daily) was initiated. Intracranial magnetic resonance imaging was declined by the owner. After 1 month of moderate improvement, the animal acutely decompensated, was presented obtunded with ataxia, vocalization, and loss of vision following generalized seizures, and subsequently died after a cardiac arrest.
Cerebrospinal fluid (CSF) analysis of a dog with CNS actinomycosis at presentation (sample 1) and 2 weeks after corticosteroid treatment (sample 2). Total nucleated cell counts and protein levels increased following symptomatic treatment.
On necropsy, the superficial blood vessels of the cerebral cortex were hyperemic, and the cerebellum was mildly coned, protruding slightly through the foramen magnum. There was approximately 1 ml of purulent material in the subdural space, mainly located over the brain stem. The leptomeninges overlying the midbrain, pons, and medulla, and the dura mater lining the corresponding ventral portions of the calvarium were thickened, hyperemic, roughened, and opaque. Sagittal sections of the brain showed symmetrically dilated lateral ventricles, consistent with moderate hydrocephalus. The superficial blood vessels of the spinal cord were diffusely engorged. The head, including oral cavity and teeth, ear canals, tympanic bullae, nasal choanae, and nasal sinuses, was examined, and no evidence of inflammation or trauma was found in any of these locations. The dog also had multiple dark red, 0.5-cm-diameter, consolidated pulmonary nodules located in the periphery of the right and left cranial lung lobes.
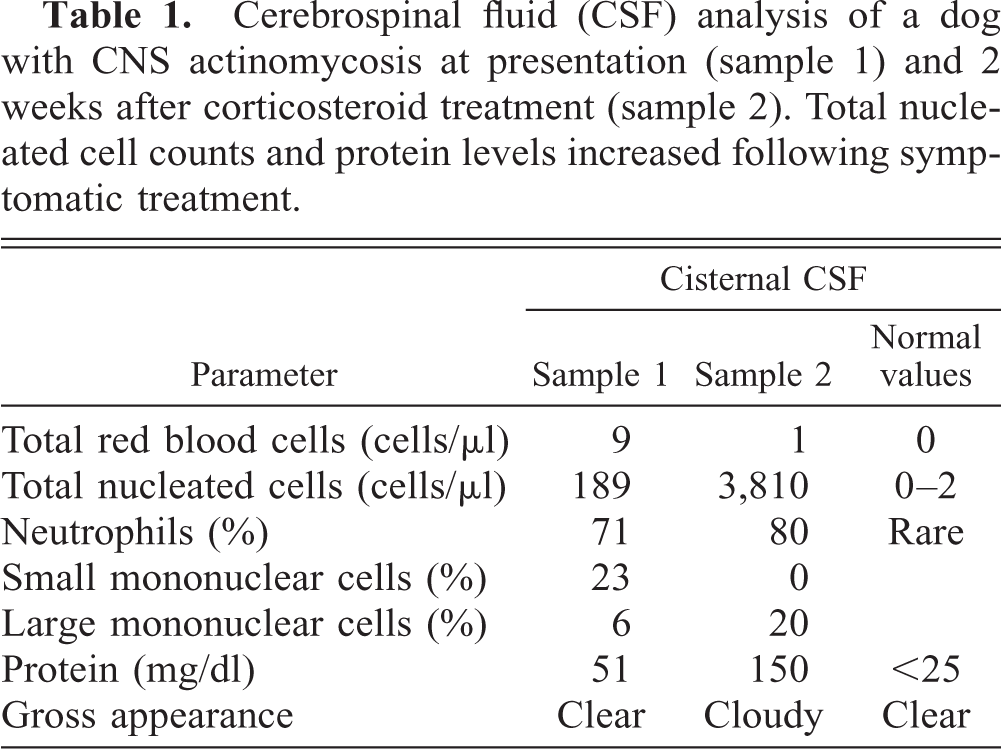
Cytology smears of the CSF obtained from the subdural space and stained with Diff Quik (Baxter Scientific Products, Mc Gaw, IL) showed abundant neutrophils and a few aggregates of degenerated neutrophils (Fig. 1). These aggregates were characterized by radiating gram-positive, acid-fast–negative filamentous organisms surrounded by a corona of elongated club-shaped neutrophils. Culture of the CSF was performed in 5% sheep blood agar with 5% carbon dioxide at 37C, and a pure culture of Actinomyces sp. was obtained.
Cerebral spinal fluid: dog. Central radiating aggregate of Actinomyces sp. surrounded by a corona of neutrophils. Diff Quik. Bar = 15 µm.
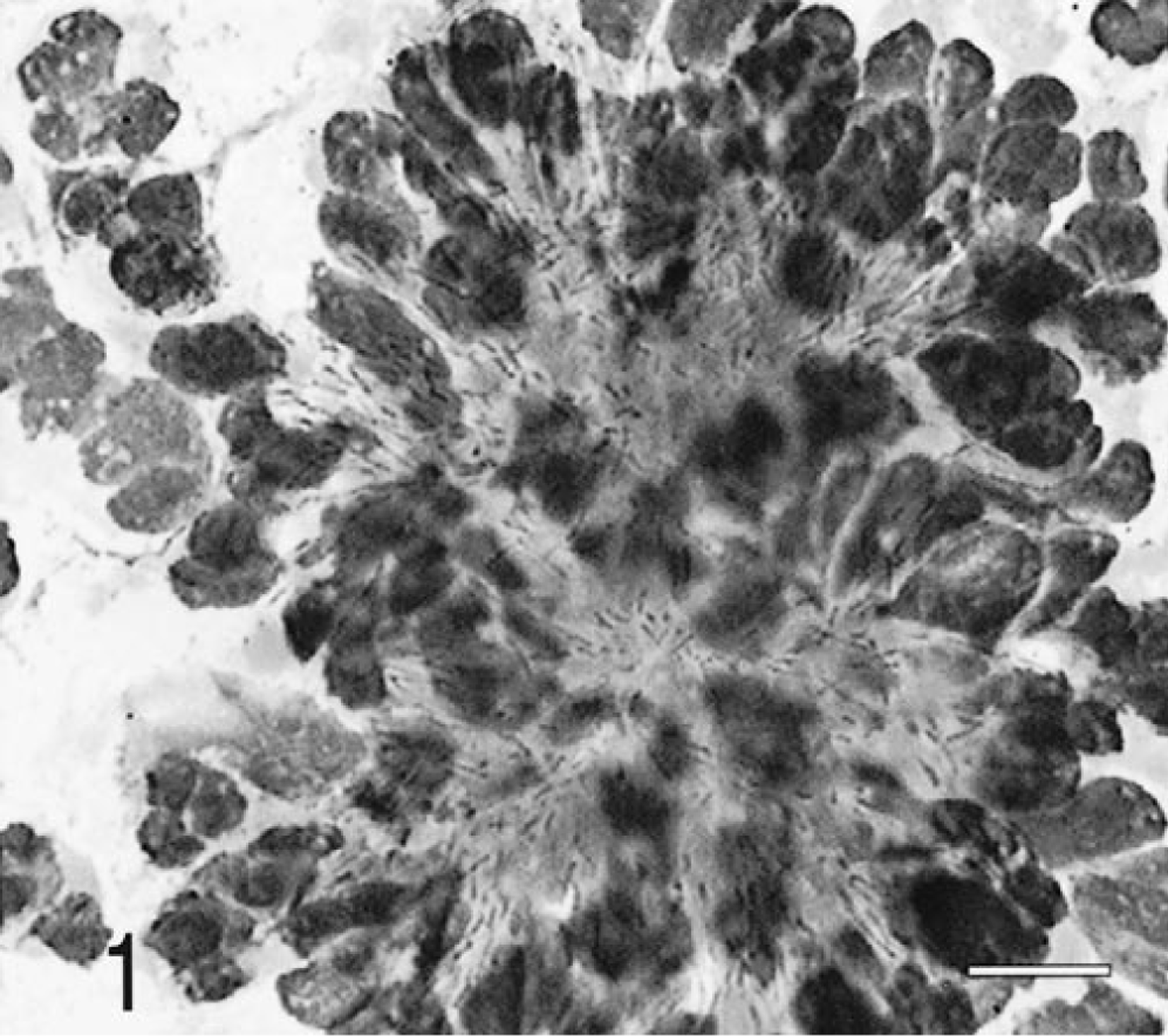
Histologically, there was severe suppurative and granulomatous meningoencephalitis and ventriculitis that involved the brain stem and the subependymal white and gray matter along the lateral third and fourth ventricles (Fig. 2). Rare radiating bacterial colonies surrounded by neutrophils and a Splendore-Hoeppli reaction were found within the meninges of the caudal brain stem (Fig. 3). The pulmonary nodules were areas of bronchopneumonia, characterized by hemorrhage, and neutrophilic infiltrates surrounding small airways. There also was a single small granuloma within the pulmonary parenchyma, characterized by an accumulation of epithelioid macrophages surrounded by a rim of lymphocytes. No organisms were seen within this granuloma with Giemsa, Brown and Brenn, or acid-fast (Fites Faraco) stains.

Brain and meninges; dog. Severe pyogranulomatous meningitis with a bacterial colony (arrow). HE. Bar = 700 µm.
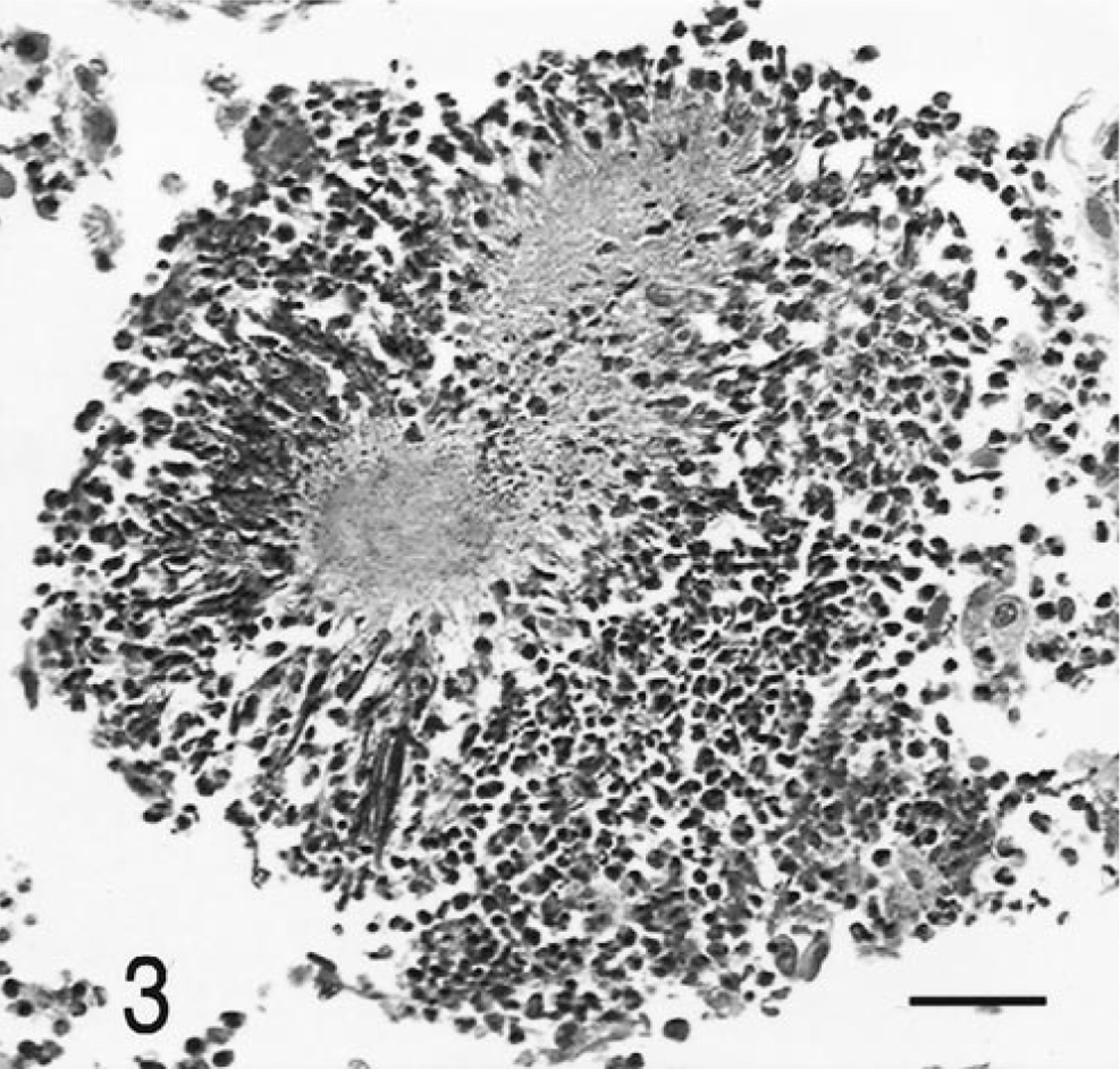
Meninges; dog. Higher magnification of Fig. 2, with radiating aggregate of Actinomyces sp. and Splendore-Hoeppli reaction. HE. Bar = 70 µm.
Actinomycosis of the CNS in animals has not been previously confirmed by culture of the organism. In the previously reported cases of meningitis in a fox and a dog, the diagnosis was assumed based on the histologic appearance of the filamentous organisms. Furthermore, both animals had facial or head bite wounds that probably were the source of infection. The present case is unusual in the absence of previous history of trauma or other sites of infection. The multifocal bronchopneumonia affected mainly cranioventral portions of the lungs and was interpreted to be due to aspiration, secondary to seizures. These lesions were acute and not considered to be associated with the actinomycosis. The single small pulmonary granuloma was a resolving lesion that was considered unrelated because of its chronicity and the absence of microorganisms.
This case is also unusual because of the disparity of bacterial culture results ante- and postmortem. Fusobacterium nucleatum was not considered a contaminant and was possibly a causative agent of a mixed anaerobic meningitis and ventriculitis, resulting in the clinical signs observed. Different antibiotic therapies are used to treat these two anaerobic organisms; Fusobacterium can be treated with metronidazole, whereas penicillin derivatives are recommended for the treatment of Actinomyces infections. In this case, the antibiotic therapy with metraonidazole could have suppressed the growth of Fusobacterium, facilitating the overgrowth of Actinomyces, which had not been detected in antemortem cultures.
Because there was no history of trauma, a migrating foxtail (seed of Hordeum murinum or wild barley) was considered a potential source of infection. Migrating foxtails are a common cause of granulomas and abcesses due to anaerobic or mixed bacterial and fungal infections in the western United States. Actinomyces hordeovulneris sp. nov. has been isolated from infections caused by migrating plant awns in California. 2 However, the present isolate of Actinomyces did not have the culture characteristics of this species.
Hydrocephalus was common to both this case and the previously reported canine case and is likely secondary to blockage of the mesencephalic aqueduct by the florid pyogranulomatous ventriculitis. Therefore, some of the chronic, progressive, poorly localized neurologic signs may be caused by secondary hydrocephalus in dogs with CNS actinomycosis.
Actinomyces sp. should be considered as a potential cause of pyogranulomatous meningoencephalitis in dogs even in the absence of a positive antemortem CSF bacterial culture. Postmortem cytology of the purulent CSF was preferable to histology in identifying the causative organisms.
Footnotes
Acknowledgements
We thank Dr. R. J. Higgins for valuable assistance with photomicroscopy.