
Abstract
Aseptic and noninfectious diseases of the central nervous system are being recognized with increasing frequency. After multiple episodes of neurologic illness, this 7-year-old Weimaraner dog was euthanatized and submitted for postmortem examination. Lesions in the central nervous system were found mainly in the white matter of the cerebral cortex and cervical spinal cord and represented acute and more chronic injury. Necrotizing vasculitis with fibrinoid change and a marked neutrophilic infiltrate dominated the acute lesions. More chronic changes consisted of perivascular demyelination and accumulation of foamy macrophages with positive staining for myelin. An immune-complex (Arthus-type) vasculitis is suspected.
Inflammation of the brain and spinal cord in dogs may be caused by a variety of microorganisms. With increasing frequency, inflammation of the brain, spinal cord, or associated structures unassociated with detectable infection by microorganisms is being recognized. 3 5 7 8 This report describes leukoencephalitis, myelitis, and vasculitis with perivascular demyelination in an 8-year-old Weimaraner dog.
The initial presenting complaint was left rear limb lameness with swelling of the stifle. The lameness progressed to rear limb ataxia with proprioceptive deficits and dysuria by the following day. These clinical signs subsided but 3 days later the dog was presented with mydriasis, ptyalism, muscular rigidity, and tremors. Again, these symptoms regressed. Eleven days later the dog was admitted to the veterinary hospital with ataxia of all four limbs and aggressive behavior. The dog's condition deteriorated with increased incoordination, proprioceptive deficits, and running into objects. The dog became recumbent and groaning suggested pain. Examination of a cerebrospinal fluid sample revealed pleocytosis and elevated protein (109 mg/dl). The dog was euthanatized and a postmortem examination was performed.
No gross lesions were detected in any organ or tissue. Because of the predominance of neurologic symptoms, microscopic examination was limited to the brain and spinal cord. Tissues were processed and sections were stained with hematoxylin and eosin according to accepted histologic techniques. Additional staining included Bodian/Luxol fast blue. Immunohistochemical stains for the detection of canine distemper virus antigen, canine immunoglobulin, and complement (C3) were performed using appropriate controls.
Microscopic lesions in the brain were scattered throughout the neuraxis with a striking affinity for white matter. Areas most severely affected were the centrum semiovale and corpus callosum. Changes in the white matter could be divided into acute and more chronic lesions. Acute lesions consisted of perivascular deposition of amorphous eosinophilic fibrinoid material and a marked accumulation of neutrophils and fewer histiocytes in perivascular spaces with a broad zone of extension into the neuropil (Fig. 1). The vascular endothelium was often intact but the remainder of the vessel walls was obliterated by the severe inflammatory reaction. Vascular thromboses were not observed. In more chronic lesions, perivascular accumulations of foamy macrophages were present with an overall paucity of myelin staining (Fig. 2). Bodian/Luxol fast blue staining confirmed perivascular myelin loss and preservation of axons (Fig. 3). Lesions in the gray matter of the brain were limited to mild perivascular cuffing with a few lymphocytes, occasional histiocytes, and rare plasma cells. The choroid plexus of the lateral ventricle and leptomeninges contained a similar but negligible infiltrate. The cervical spinal cord was similarly affected but white matter lesions were more typically of the chronic type. Immunohistochemical staining for canine distemper virus antigen was negative. No deposition of complement or immunoglobulin was demonstrable in the acute vascular lesions.
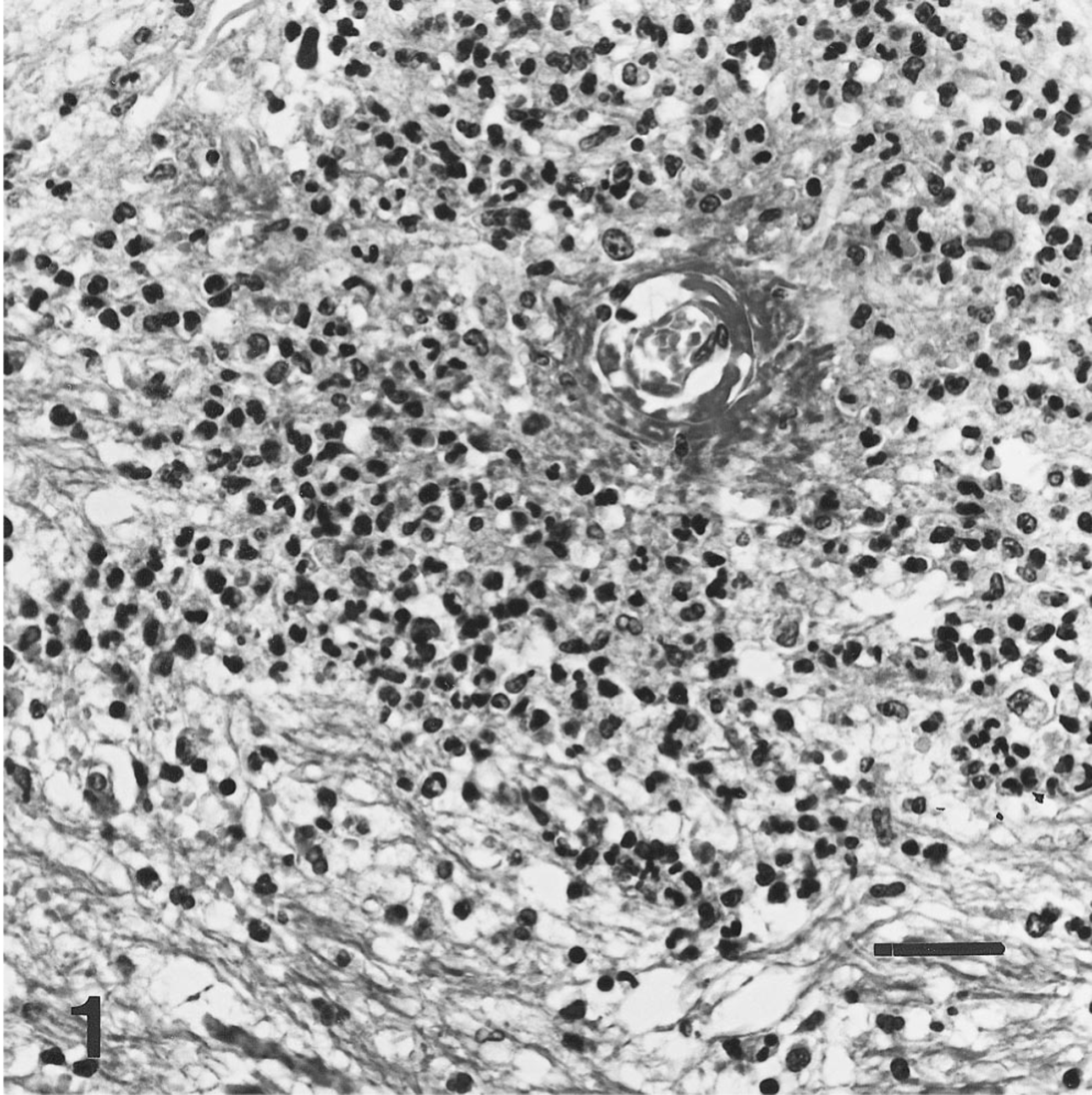
Brain, centrum semiovale; dog. Severe necrotizing vasculitis with deposition of fibrinoid material and perivascular infiltration of neutrophils. HE. Bar = 60 μm.
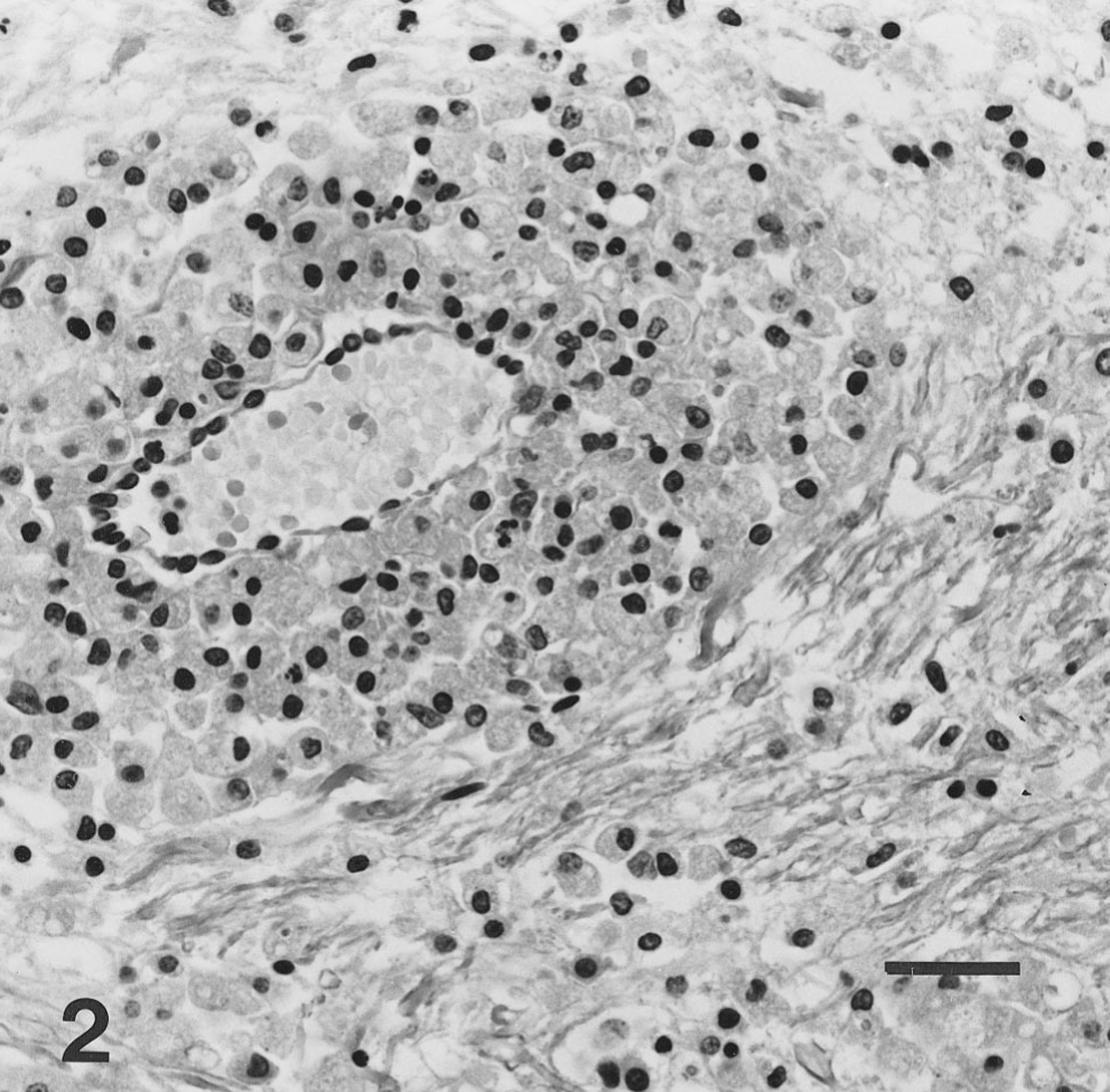
Brain, centrum semiovale; dog. More chronic lesion with perivascular accumulation of foamy macrophages. HE. Bar = 60 μm.
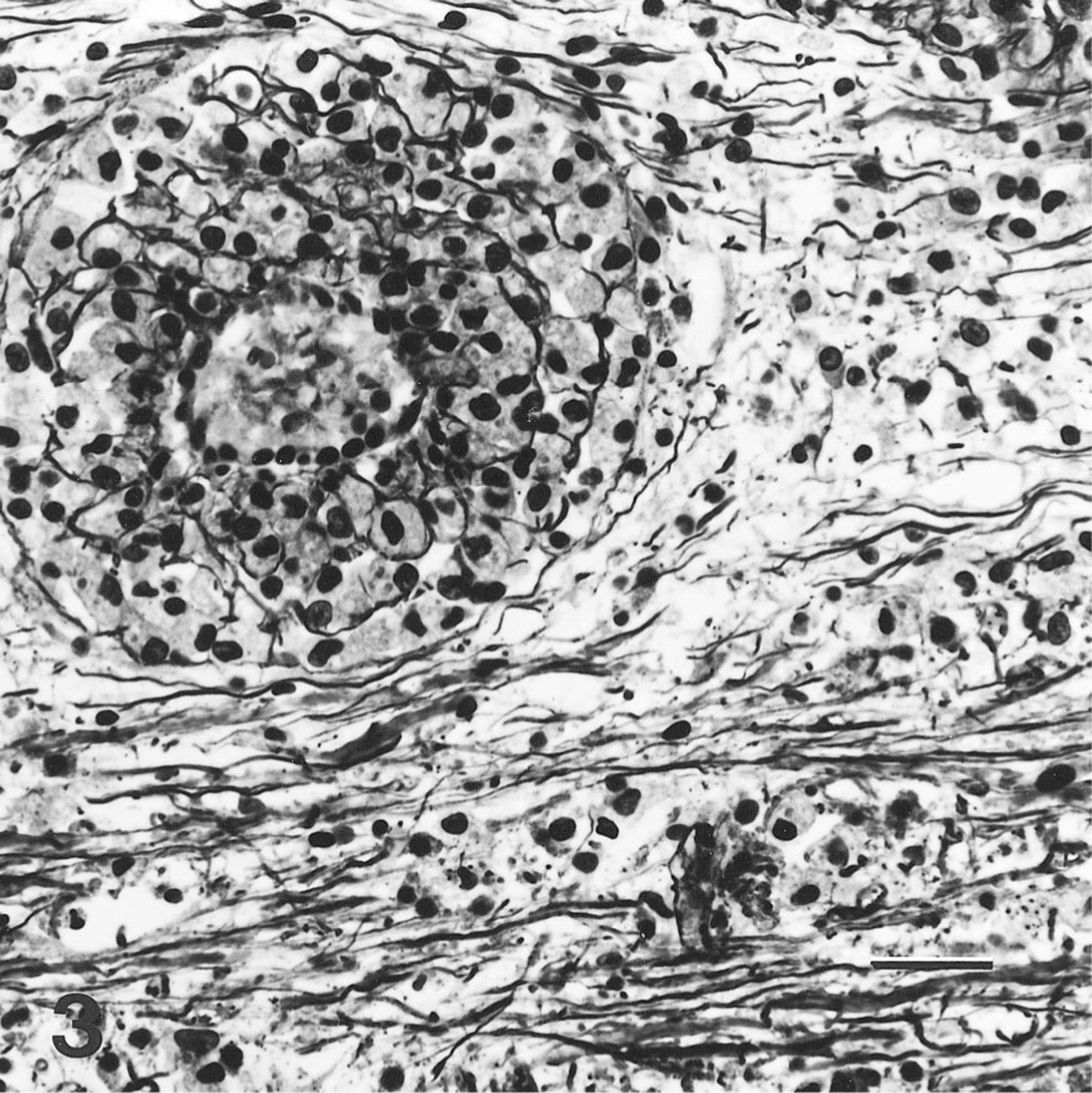
Brain, centrum semiovale; dog. Paucity of myelin staining in perivascular areas with preservation of axons. Bodian/Luxol fast blue. Bar = 60 μm.
Lesions in this dog are dominated by acute vasculitis in white matter leading to perivascular demyelination. Other diseases in the dog with either prominent cerebral white matter involvement or vasculitis, and possibly having an immune basis include Pug dog encephalitis 4 6 and related syndromes, 6 necrotizing meningeal vasculitis in Beagles and other breeds, 3–7 and steroid-responsive meningitis in mainly large dog breeds. 5 The prominent neutrophilic response and fibrinoid change in the acute vasculitis and/or the affinity for white matter areas rather than meninges reported in this Weimaraner are not typical of these syndromes.
The cause of the lesions in this dog is undetermined. Based on the character of the brain changes, an immune-mediated mechanism is suspected. The vasculitis is compatible with a localized Arthus reaction secondary to deposition of antibody–antigen complexes in blood vessel walls and activation of complement with an acute influx of neutrophils. 2 The finding of lesions representing both acute and more chronic vascular injury with perivascular demyelination would be atypical of an infectious or septic process and would support an immune-mediated pathogenesis. White matter diseases in humans thought to have an immune-mediated basis and that are characterized by vasculitis and perivascular demyelination include postinfectious or postvaccinal encephalomyelitis and acute hemorrhagic leukoencephalopathy. 1 The latter is thought by some to represent an acute form of postinfectious encephalomyelitis because of the frequent association with a previous viral infection. Except for the conspicuous absence of hemorrhage in this dog, the lesions are most analogous to those of hemorrhagic leukoencephalopathy including vasculitis, frequent severe involvement of the cerebral white matter, and preponderance of neutrophils in the acute lesions. Postvaccinal or postinfectious encephalomyelitis has rarely been reported in the dog. 4 Although perivascular demyelination is present in these cases, little vascular necrosis is present and the perivascular infiltrate is predominantly lymphocytes, plasma cells, and macrophages rather than the prominent neutrophilic infiltrate in this Weimaraner.
Footnotes
Acknowledgements
We wish to acknowledge Dr. Liliana Cabrera for her valuable contribution of clinical information and for submitting the case for postmortem examination.