
Abstract
Multiple myeloma was diagnosed in two cats with monoclonal hyperglobulinemia, proteinuria, and plasma cell proliferations in bone marrow. An immunoglobulin G-producing myeloma occurred in the vertebral bone marrow of one cat, and twice responded to surgical reduction followed by a combination of local irradiation and chemotherapy. The cat's survival time was approximately 2 years. The other myeloma in a cat that presented with hypercalcemia and renal insufficieny involved visceral organs and produced a biclonal peak due to immunoglobulin A dimer formation on serum electrophoresis. This cat's tumor did not respond to chemotherapy.
Multiple myeloma consists of a clonal proliferation of malignant plasma cells that usually produce an immunoglobulin. The tumor originates in the bone marrow and may involve other organs to varying degrees. Affected individuals generally are hyperglobulinemic. Leakage of free light chains into the urine results in proteinuria. The homogenous nature of the secreted paraprotein produces a narrow peak on serum and urine electrophoretograms. Multiple myeloma has been reported to constitute approximately 8% of all canine hematopoietic neoplasms, but it appears to be a relatively rare tumor in cats. 14 In small animals, the presence of at least two of four features has been described as requisite for a diagnosis of multiple myeloma: paraproteinemia, osteolytic lesions, more than 20% plasma cells in bone marrow biopsies, and Bence Jones (light chain) proteinuria. 14 Studies in human patients indicate that monoclonal gammopathies of undetermined significance may precede the development of overt multiple myeloma by years and may accompany degenerative or infectious diseases without evidence of neoplasia. 1 Similarly, multiple myeloma-like production of monoclonal immunoglobulins has been reported in dogs lacking evidence of a neoplasm but afflicted with pyoderma, leishmaniasis, plasmacytic enteritis, or ehrlichial infection. 3 , 6 , 14 Furthermore, osteolytic lesions and bone marrow infiltration with abnormal plasma cells were noted in a dog without a monoclonal gammopathy. 11 Thus, nonsecretory variants of multiple myeloma and nonneoplastic conditions mimicking multiple myeloma may exist in animals.
Classifying plasma cell proliferations in cats poses an even greater challenge. Solitary extramedullary tumors producing a cell-bound monotypic immunoglobulin or accompanied by a monoclonal gammopathy were classified as plasmacytomas. 15 , 18 A different presentation of an extramedullary plasmacytoma manifested with production of excess light chains, amyloid deposition, and tumor involvement of visceral organs. 4 Hepatic plasmacytoma or plasmacytoid lymphoma were diagnosed in cats with clonal immunoglobulin production and Bence Jones proteinuria; however, these cats lacked osteolytic lesions. 9 , 17 Osteolysis and intramedullary plasma cell proliferation in association with a polyclonal gammopathy were diagnosed as multiple myeloma. 16 Finally, feline cases more typical of “classical” multiple myeloma were reported to have bone marrow proliferation of plasma cells, paraproteinemia, and, in some cases, osteolytic lesions. 5 , 7 , 13 , 16 Thus, plasma cell proliferations in cats may range from nonsecreting solitary tumors to widespread nonsecreting extramedullary tumors to predominantly intramedullary myelomas that elaborate monoclonal proteins.
The clinical presentation of cats with multiple myeloma tends to be variable. Nonspecific presenting causes are depression, chronic infections, renal disease, vomiting and diarrhea, neurologic abnormalities, and bleeding diatheses. 5 , 16 The longest survival time reported in a cat with multiple myeloma treated with chemotherapy was 16 months; more commonly, the animals are euthanized within 6 months of diagnosis. 13 , 5 , 7 , 8 , 16 Feline tumors classified as plasmacytomas may be locally invasive or may metastasize and then have generally responded poorly to therapy. 4 , 9 , 15 , 18 In this report, features of two unusual cases of feline multiple myeloma are detailed.
A 6-year-old spayed female Maine Coone cat was referred for evaluation of neurologic signs, hyperglobulinemia, and hypoalbuminemia. On examination, the cat was thin and had a dull coat. Thoraco-lumbar hyperesthesia and pelvic limb ataxia were noted. Radiography revealed hepatomegaly and a faint osteolytic lesion in the 11th thoracic vertebra (T11). The laboratory findings are summarized in Table 1. Investigation of the hyperglobulinemia with serum and urine electrophoresis identified a monoclonal protein peak in the γ region. On immunoelectrophoretic evaluation, the predominant protein was classified as immunoglobulin G (IgG). Serologic tests for feline leukemia virus (FeLV), feline immunodeficiency virus (FIV), feline coronavirus, and toxoplasmosis were negative. A contrast myelogram showed a compressive spinal cord lesion in the region of T10 to T12. Cerebrospinal fluid examination was normal. On exploratory dorsal laminectomy, fragments of a soft T11 vertebral body were removed. Histologically, the biopsy consisted of a uniform population of large, round cells surrounded by bony trabeculae. The cells had round to oval nuclei and coarsely clumped chromatin that was occasionally in a spoked-wheel pattern (Fig. 1). Perinuclear Golgi zones were apparent in some areas, whereas binucleation or anisocytosis was rarely observed. Normal hematopoietic cells were absent except for occasional neutrophils at the margins of the biopsy. The predominant cells were identified as plasma cells. In conjunction with a monoclonal gammopathy, the tumor was diagnosed as multiple myeloma. Pelvic bone marrow aspirates revealed no abnormalities. The cat was treated postoperatively with 11 fractions of site-specific cobalt irradiation. Subsequently, prednisone (20 mg/m2) and melphalan (2 mg/m2) were administered, and the animal was discharged 5 days postoperatively.
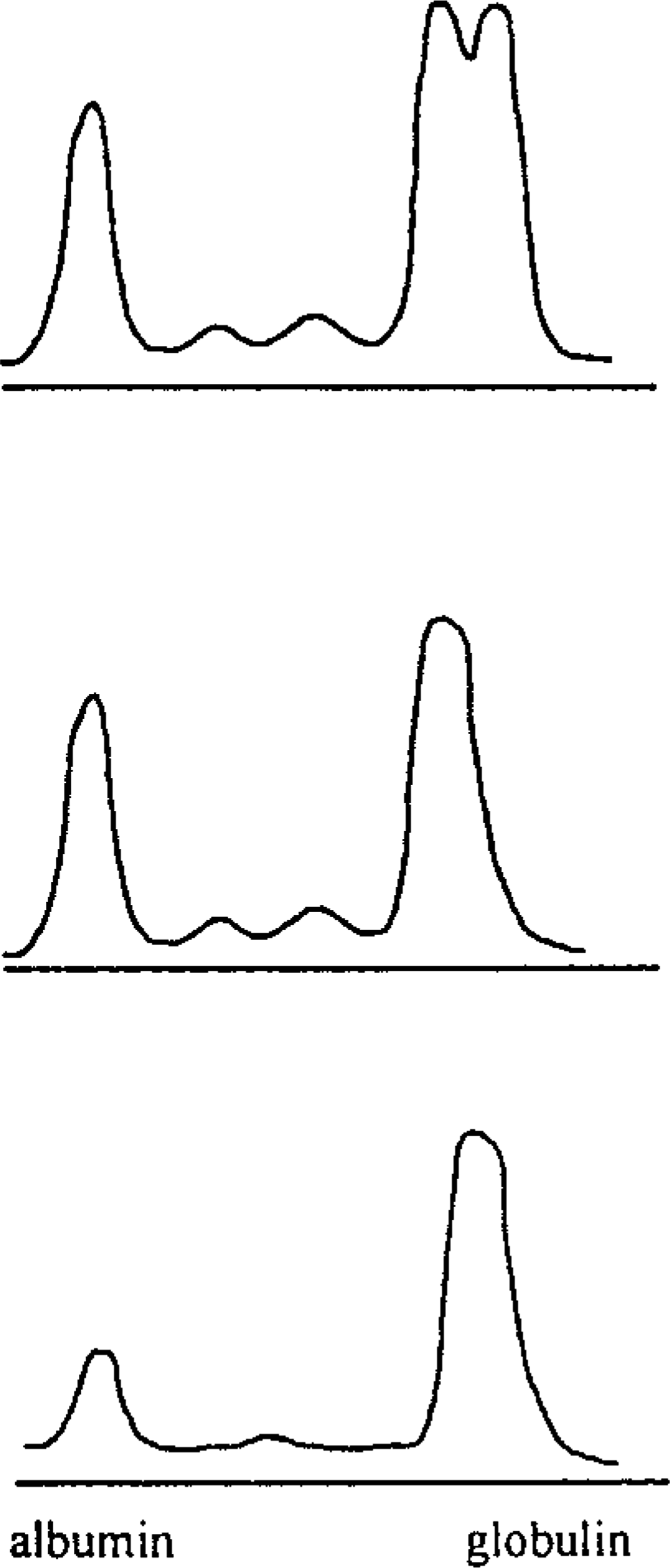
Summary of laboratory findings in two cats with multiple myeloma.
∗ adqu = judged adequate on smear examination; decr = decreased; ND = not determined; NAF = no abnormal findings; MM = multiple myeloma.
† Clinical Pathology Laboratory, University of Georgia.
‡ Determined as capillary tube transit time.
Photomicrograph of a vertebral body biopsy from cat No. 1 with multiple myeloma. The biopsy consists of loosely arranged round to oval cells with eccentric nuclei. HE. Bar = 25 µm.
The neurologic signs and hyperproteinemia resolved during the subsequent weeks. Development of neutropenia prompted reduction of the melphalan therapy on days 147 and 205. The cat was presented again because of recurrence of neurologic signs on day 451. Bone scintigraphy with intravenous technetium-99m-methylene disphosphonate identified active regions within the vertebral bodies of L2, L3, L4, L5, in the distal right tibia, and in the caudal aspect of the nasal cavity. These were interpreted as likely sites of disseminated multiple myeloma. Melphalan therapy was increased; however, profound neutropenia developed, and the animal's neurologic status did not improve. Radiography and myelography revealed a compressive mass associated with L2. The mass was surgically removed. The histologic diagnosis was a plasma cell neoplasm with cell morphology similar to the initial biopsy. No abnormalities were identified in a bone marrow aspirate. Three weekly palliative cobalt irradiation treatments were followed with biweekly vincristine therapy and continued administration of prednisone. The cat responded well, and the neurologic abnormalities resolved. Approximately 5 months later, 682 days after the initial presentation, the cat's condition gradually deteriorated, marked hyperproteinemia redeveloped, and increasing doses of melphalan were ineffective. Pelvic bone marrow aspiration did not reveal abnormalities. The owner elected to euthanatize the animal. Necropsy examination was not permitted.
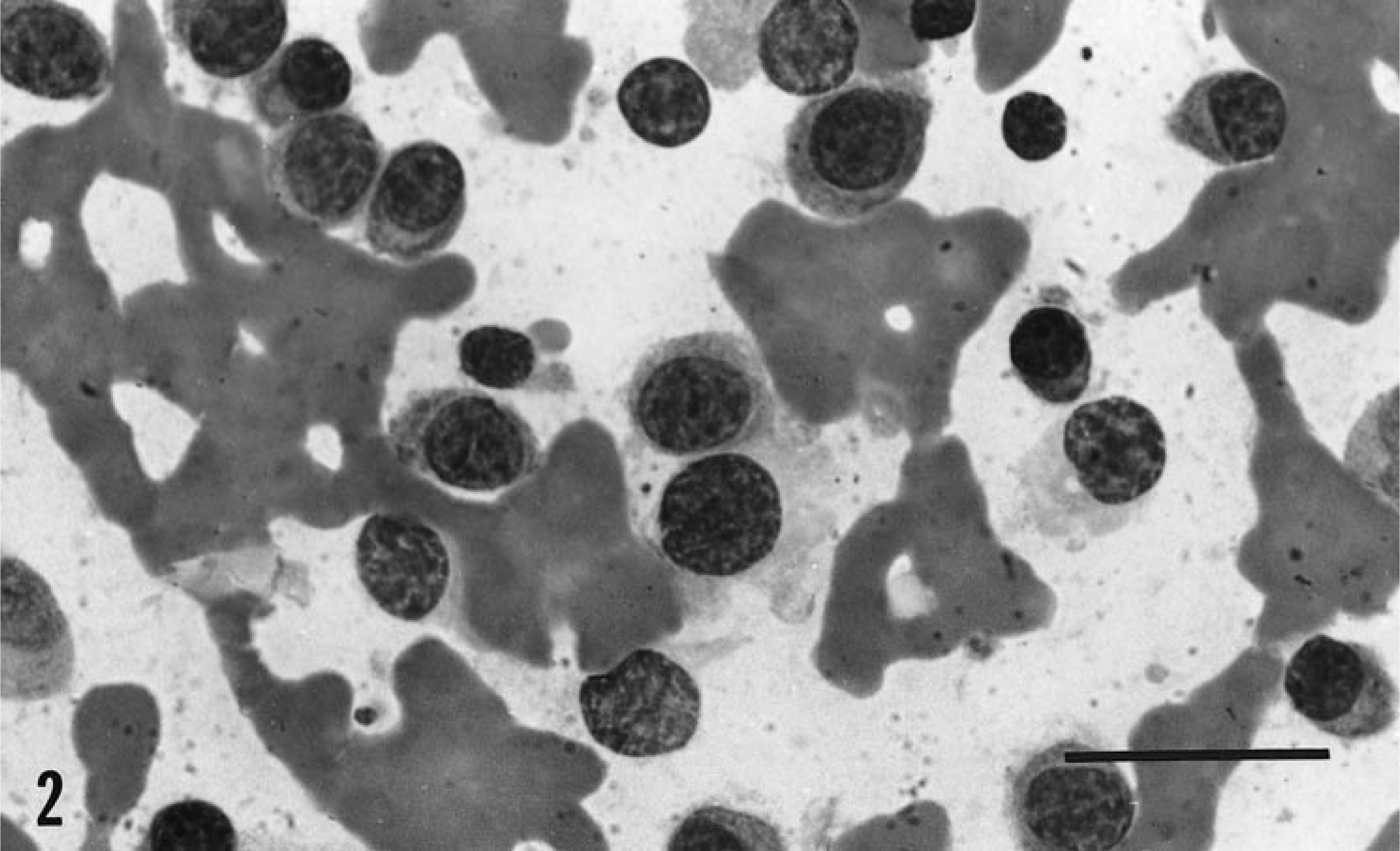
A 10-year-old castrated male Domestic Shorthair cat presented with a history of anorexia and weight loss. On physical examination, the animal was dehydrated, and an enlarged spleen and asymmetrical kidneys were palpated. Laboratory evaluation disclosed leukopenia, a marked hyperproteinemia, hypercalcemia, and renal insufficiency as indicated by an elevated creatinine concentration with concurrent near isothenuria (Table 1). Immunodiagnostic assays for FeLV, FIV, feline coronavirus, and toxoplasmosis were negative. No osteolytic foci were identified on radiography. Aspirates from the spleen and proximal humerus consisted of small- to medium-sized plasma cells with occasional bi- or multinucleation and moderate anisokaryosis and anisocytosis (Fig. 2). Hematopoietic elements comprised approximately 20% of cells in the bone marrow aspirate, and the splenic sample yielded almost exclusively plasma cells. Multiple myeloma was diagnosed subsequent to identification of a sharp biclonal peak in the γ region on serum electrophoresis (Fig. 3). The urinary protein consisted of a single peak in the β region, and following exposure of the serum to a reducing agent, only a single peak remained on the electrophoretogram (Fig. 3). Immunophoretically, the isotype was identified as IgA. Therapy with melphalan and prednisone was started, but the cat remained anorexic and depressed, and the owner elected euthanasia. Necropsy examination was not permitted.
Fine needle aspiration smear from the spleen of cat No. 2 with multiple myeloma. The nucleated cells present amidst a hemorrhagic background are round with an eccentrically located nucleus and a faint Golgi zone. Wright's stain. Bar = 25 µm.
Densitometric tracing of cellulose acetate electrophoresis of untreated serum (top), serum containing 1 M 2-mercaptoethanol (middle), and 50× concentrated urine (bottom) from case 2.
The cats in this report each had multiple myeloma as diagnosed by monoclonal gammopathy, Bence Jones proteinuria, and bone marrow infiltration with plasma cells. One cat had an exceptional response to a combination of surgery, radiation, and alkylating therapy and survived nearly 2 years following diagnosis. Alkalyting therapy with melphalan is the recommended treatment for multiple myeloma in small animals; radioresponsiveness of the tumor has not been evaluted in animals. 14 In human patients with multiple myeloma, the incidence of vertebral fractures and marrow lesions was reduced with focal irradiation; this is an effect that may have contributed to the long survival of the cat in this report and may warrant further exploration. The second cat presented with renal disease, hypercalcemia, and leukopenia; lack of response may have been due to these factors. The nonspecific nature of the historical findings in both cats was typical of other reports. The absence of osteolytic lesions in case 2 appears to be relatively common in cats with multiple myeloma, despite marrow involvement of the neoplasm. 5 , 7 , 16 This discrepancy may be due to an insensitivity of radiography to detect minute lytic foci or due to lack of osteoclast-activation by some malignant B cells.
Too few detailed cases of feline multiple myeloma are reported to correlate prognosis with immunoglobulin isotype. Although IgA appears to be less commonly produced than IgG, the five published cases (including this report) with an IgA paraprotein had visceral involvement and survival times ranging from a few days to 6 months. 5 , 8 , 12 , 13 Either immunoglobulin has been associated with clinical signs of hyperviscosity, including cardiac insufficiency, retinal hemorrhages, and neurologic signs. 7 , 8 This phenomenon relates to the size of the paraprotein and the degree of hyperglobulinemia. Since IgA may assume a dimeric or multimeric form, as in case 2 reported here, it may be more frequently associated with hyperviscosity than IgG. Reduction of the IgA dimer to a monomer with a reducing agent confirmed the monoclonal rather than biclonal nature of the paraprotein in case 2. The single cat reported with a plasmacytoid tumor and IgM paraprotein production had severe hyperviscosity consistent with the large size of the IgM molecule. 17 In humans, specific biochemical features of the monoclonal protein further contribute to clinical manifestations. Monoclonal IgG with κ light chains results in cryoprecipitates more frequently than with λ light chains. In small animals, λ chains comprise the majority of immunoglobulin light chains produced by B cell neoplasms, thus offering a plausible explanation for the infrequent occurrence of cryoglobulin-associated disorders. 2 , 4 Although the clinical manifestations of multiple myeloma in humans are known to vary with the isotype subclass, the occurrence of this in animals is unknown.
Another complication associated with multiple myeloma is hypercalcemia; it is thought to result from tumor-induced production of osteoclast-activating factors such as interleukin (IL)-6 and IL-1β by stromal and bone cells. 1 Increased ionized calcium concentration in case 2 of this report, and in a previous case, suggests paraneoplastic hypercalcemia rather than renal disease as the cause. 13 The renal disease commonly observed in cats with multiple myeloma may result from a combination of impaired tubular catabolism of excess light chains, glomerular Bence Jones protein deposits, amyloid deposits, and hypercalcemia-related tubular unresponsiveness. Bleeding diatheses arising from the interaction of the paraprotein with platelets or coagulation factors have been reported in humans and cats. 1 , 7 Finally, inadequate or abnormal production of immunoglobulins may immunocompromise some patients so that opportunistic infections may occur. 5 , 8 , 16
In summary, common features of multiple myeloma in cats are bone marrow involvement, paraproteinemia, and Bence Jones proteinuria. Plasma cell tumors lacking detectable bone marrow involvement may nevertheless be associated with paraproteinemia and Bence Jones proteinuria. Thus, there is considerable overlap between multiple myeloma and plasmacytoma. Until a greater number of feline cases with extranodal B cell tumors are analyzed, or until surface markers for assessing the maturational stage of the B lymphocyte are available, marrow involvement appears to best distinguish these different neoplasms.