
Abstract
A 10-week-old male Great Dane Puppy was presented for sudden onset tetraataxia and severe paresis of the front legs. Mineral deposits were detected radiographically, at gross postmortem examination, and light microscopically between the vertebral arches of multiple cervical and lumbar vertebrae. These deposits were associated with the interarchial ligaments (ligamentia interarcualia), along the interfaces of the synovium and articular cartilage of multiple cervical, thoracic, and lumbar facets, on the dorsal aspect of several thoracic intervertebral discs, and at the insertion of muscles at the lateral aspect of several cervical and thoracic vertebral bodies. The mineral deposits were associated with a granulomatous inflammation and synovial fibrocartilaginous metaplasia and proliferation, which was focally exuberant. X-ray diffraction analyses of the mineral deposits revealed calcium hydroxylapatite as the major component. The clinical signs in this puppy were due to focal compression of the spinal cord by marked extraarticular ligament-associated fibrocartilaginous proliferation.
In Great Dane puppies with paraplegia, calcium phosphate deposition disease has been reported in multiple diarthrodial joints of the appendicular and axial skeleton. 12 Here, we present a case of calcium hydroxylapatite deposition disease in a Great Dane puppy that was limited to the axial skeleton and included marked fibrocartilaginous proliferation, resulting in compression of the spinal cord.
A 10-week-old male Great Dane dog, weighing about 7 kg, presented to the Veterinary Teaching Hospital of the Ohio State University for a 2-day history of progressive weakness. The puppy had been fed puppy food. On physical examination, the puppy appeared slightly depressed and was tetraataxic with severe bilateral paresis of both forelimbs, although the dog could support weight with both hind limbs. Conscious proprioception was not perceived in either forelimb and was decreased bilaterally in the hind limbs. Cranial nerve reflexes were normal. Flexor reflexes were decreased in the forelimbs but normal in the hind limbs. All forelimb segmental spinal reflexes were absent bilaterally. Patellar reflexes were increased, as were clonus and anterior tibial reflexes. The puppy was consistently pained by palpation of the cervical vertebrae and lateral and dorsoventral movement of the neck. A C1–C5 transverse myelopathy was suspected, based on the clinical signs and results of neurologic examination.
Complete blood count revealed a mild nonregenerative anemia (packed cell volume = 27.1%). No abnormalities were noted on the leukogram or platelet count. In the serum biochemical profile, all parameters investigated, including total calcium (10.3 mg/dl), ionized calcium (5.68 mg/dl), and phosphorus (5.7 mg/dl), were within normal limits. Survey radiographs of the vertebral column revealed irregular mineralization in the area of the intervertebral facets throughout the cervical, thoracic, and lumbar spine up to the level of the lumbosacral junction. A mild “step” defect was observed along the floor of the vertebral canal between C3 and C4. Ventrodorsal projection revealed that the irregular areas of mineralization were associated with the intervertebral facets and also within the soft tissues lateral to the caudal cervical spine. No abnormalities were noted on radiographs of joints of the left radius and ulna and left stifle and tibia.
Treatment was initiated with an 70-mg intravenous dose of prednisolone sodium succinate. The puppy was maintained on 0.25 mg dexamethasone given orally twice daily and 33 mg cimetidine administered intravenously three times daily. Serial neurologic examinations revealed no improvement in the degree of paresis, proprioceptive deficits, and spinal reflexes to the initiated symptomatic therapy. Because of the poor response to medical treatment and poor prognosis for surgical correction of the anatomic defects, the owners elected euthanasia. Immediately postmortem, a lumbar myelogram was performed. Myelography revealed marked ventral displacement of the dorsal contrast column between C1 and C2. The dorsal contrast column was attenuated at that site (Fig. 1). Ventrodorsal projection revealed abaxial deviation of both the right and left contrast columns between C1 and C2 and thinning and axial displacement of the contrast columns between C5 and C6, C6 and C7, and C7 and T1. Lateral projection revealed marked attenuation of the dorsal contrast column on the caudal aspect of C2 up to the cranial aspect of C5. The contrast column was not visible between C7 and T1.
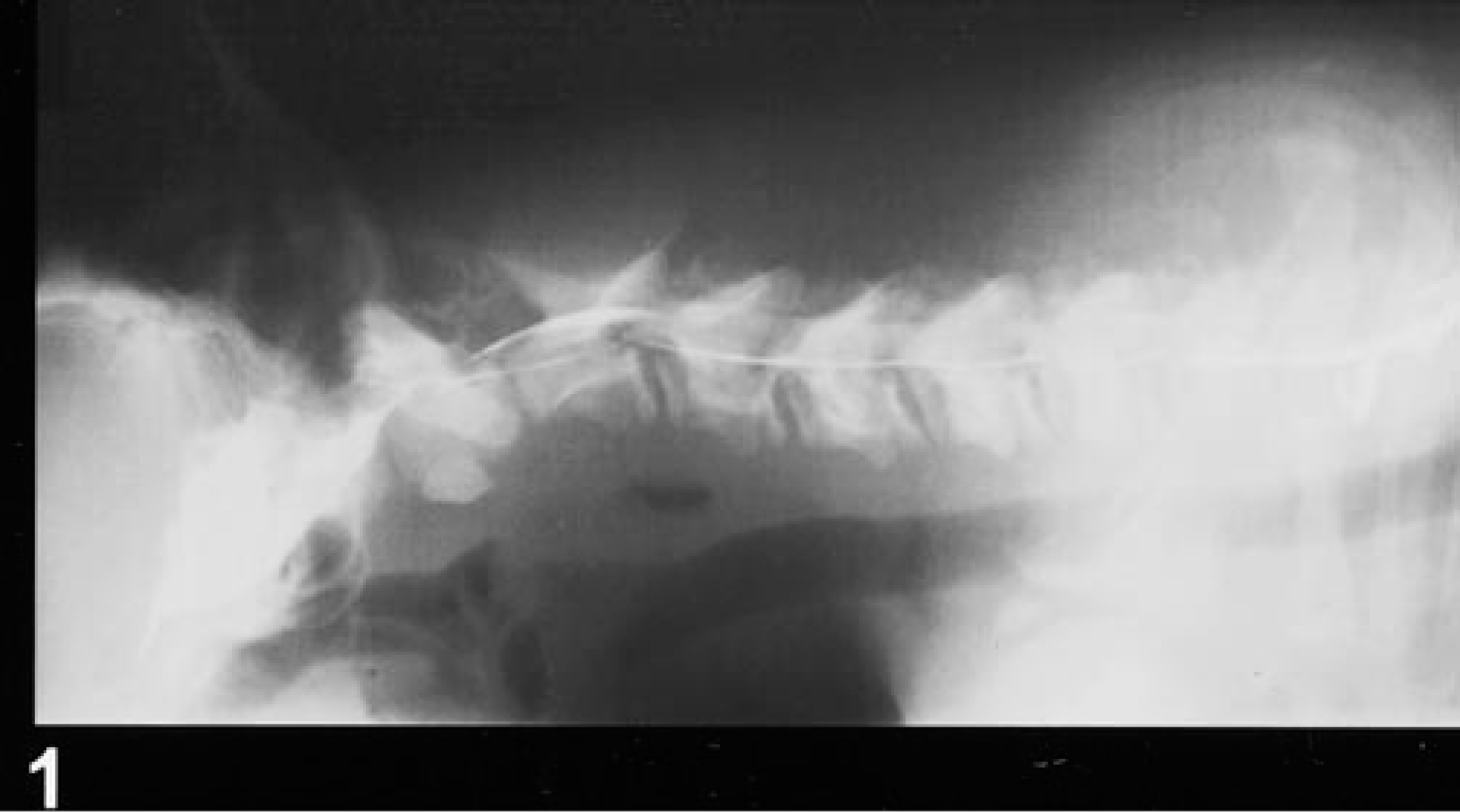
Myelogram. Cervical vertebral canal; Great Dane puppy. There is marked ventral displacement and attenuation of the dorsal contrast column between C1 and C2. Note also the irregular mineralization between the dorsal processes of C1–C2 and C2–C3.
At necropsy, a homogenous white, firm mass, approximately 1.5 cm in length, was found connecting the arches of C1 and C2, replacing the interarchial ligament, and forming the roof of the vertebral canal (Figs. 2, 3). The mass was extraarticular but continuous with the facet capsule. Within the mass were small white mineralized deposits. The mass protruded into the vertebral canal and compressed the spinal cord. It consisted of fibrocartilaginous tissue with sparse intralesional mineral deposition, which was positive with von Kossa stain in nondecalcified tissue. A mild granulomatous inflammatory reaction was associated with the mineral deposition. To a lesser extent, similar lesions were seen between several vertebral arches of other cervical, thoracic, and lumbar vertebrae (Fig. 2). The articular hyaline cartilage of the facets was normal. Intraarticular pinpoint to linear white mineral deposits were noticed along the interface of the synovium and the articular cartilage. These synovial and subsynovial mineral depositions were generally associated with a more severe granulomatous inflammatory response and a fibrocartilaginous metaplasia (Fig. 4). In the T7/T8 symphyseal intervertebral joint, two firm beige nodules, 5 mm in diameter, were found over the intervertebral disc. The intervertebral disc, including anulus fibrosus and nucleus pulposus, did not show any signs of degeneration. The nodules protruded dorsolaterally of the ventral longitudinal ligament into the vertebral canal (Fig. 5). These masses and similar, but microscopic, masses on consecutive intervertebral discs of the midthoracic spine segment consisted of nonbirefringent, amorphous to granular, amphophilic to basophilic von Kossa-positive material. In the larger masses, this von Kossa-positive material was admixed with fibrohistiocytic cells. The masses were bordered by inflammatory cells mainly composed of multinucleated giant cells and histiocytes (Fig. 6). Occasionally, the tendinous insertion of muscles inserting laterally at the vertebral body of cervical vertebrae (m. obliquus capitis, m. intertransversarii cervicis) showed pinpoint white mineral deposits.
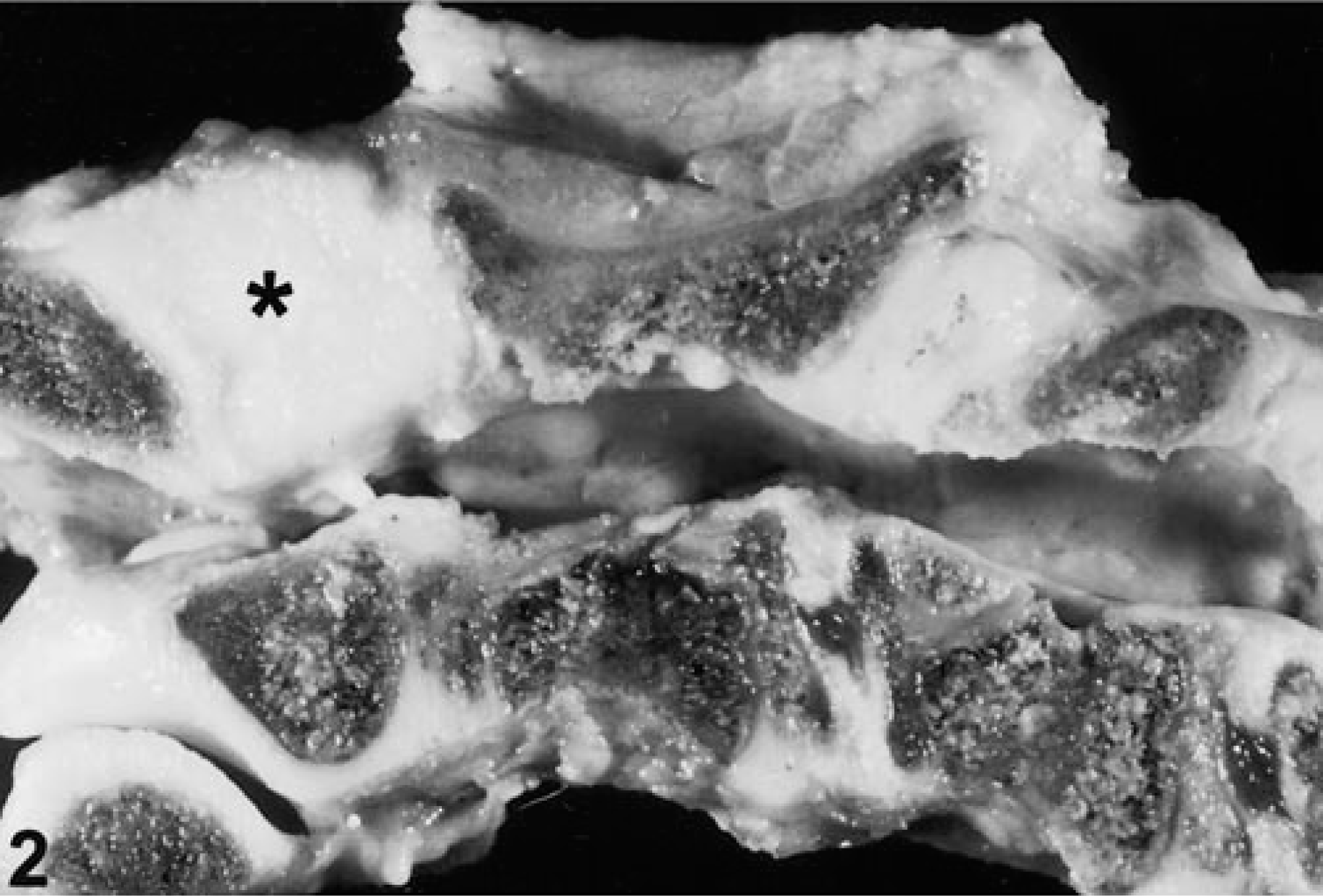
Vertebral column (C1–C4); Great Dane puppy. A prominent fibrocartilaginous mass (∗) is present between the vertebral arches of C1 and C2, reducing the diameter of the vertebral canal. A second similar mass occupies the space between the vertebral arches of C2 and C3. Formalin fixation.
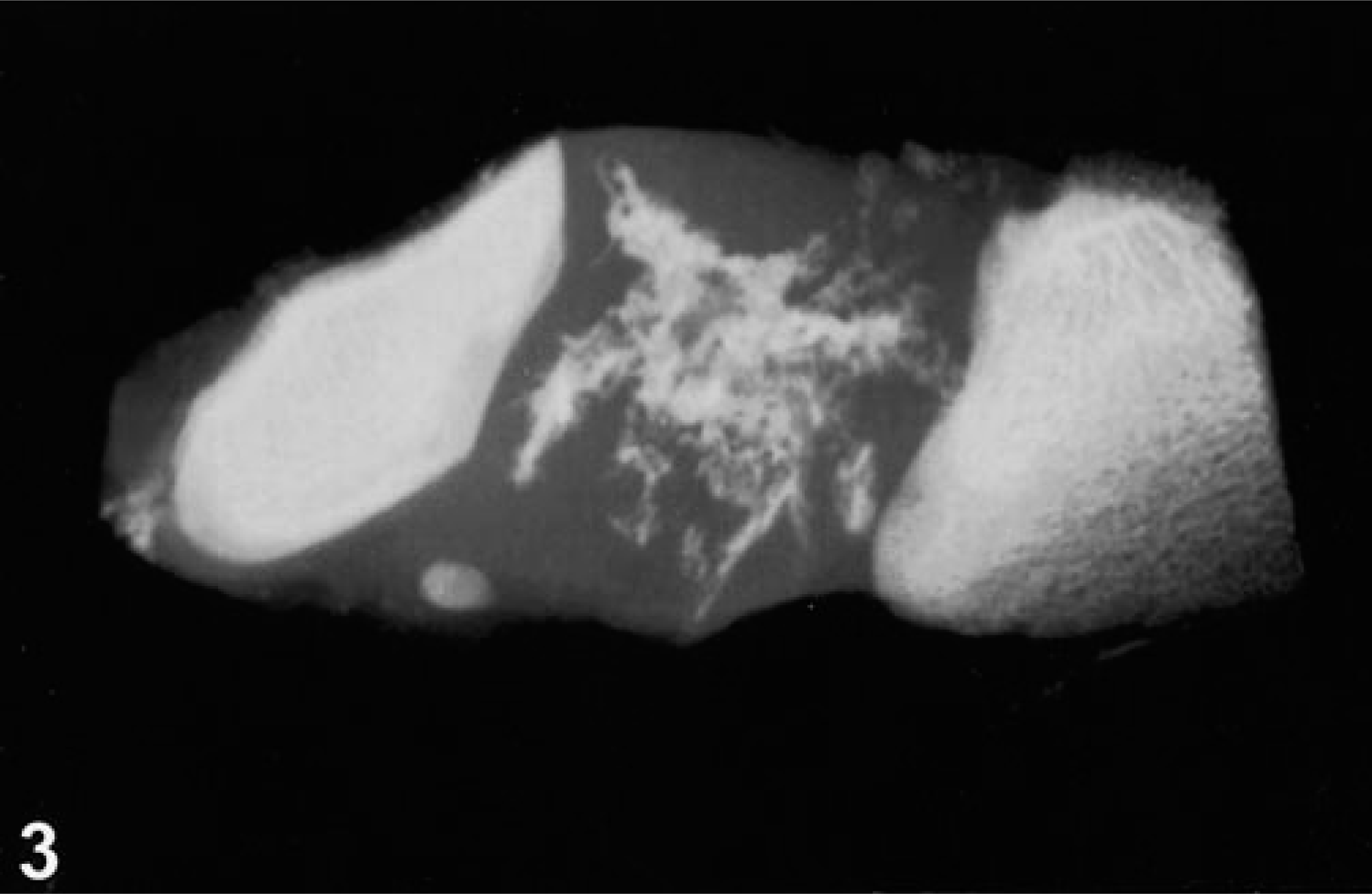
Laterolateral radiograph. Slab section of the vertebral column (C1–C2); Great Dane puppy. Irregular mineral deposits are present between the vertebral arches of C1 and C2.

Vertebral column; Great Dane puppy. Synovial membranes of a facet joint show mineral deposition, associated granulomatous reaction, and fibrocartilaginous metaplasia of underlying tissue (S = joint space). Decalcified specimen. HE. Bar = 140 µm.
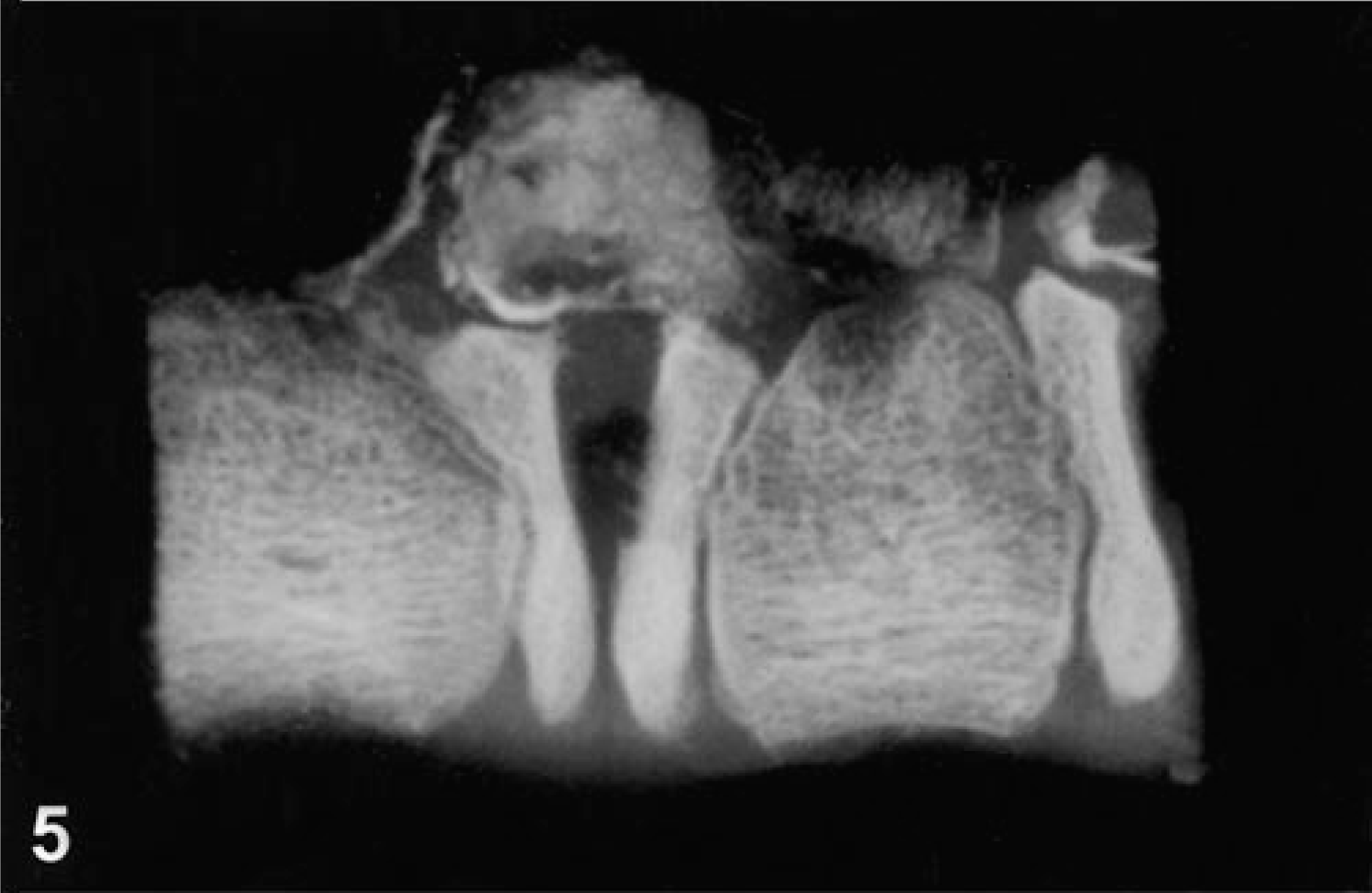
Laterolateral radiograph. Slab section of the vertebral column (T7–T8); Great Dane puppy. A mass with abundant irregular mineral deposits protrudes into the vertebral canal over the intervertebral disc.
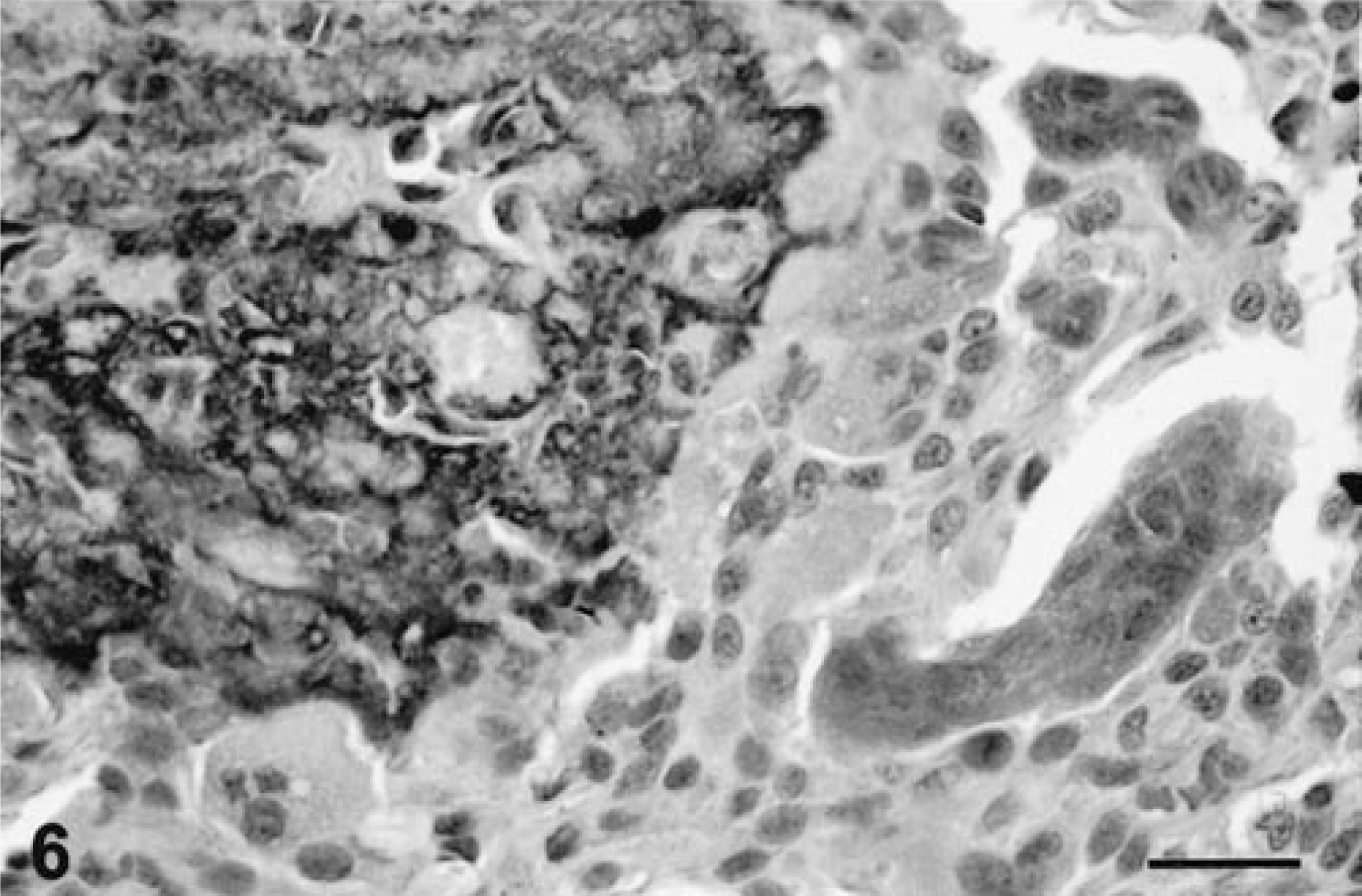
Vertebral column; Great Dane puppy. Subligamentous mass overlies the intervertebral disc between T7 and T8. Amorphous cloudy, crystalline material contains cellular debris with associated granulomatous inflammation characterized by multinucleated giant cells and histiocytes. Decalcified specimen. HE. Bar = 25 µm.
For X-ray diffraction analyses, formalin-fixed intraarticular mineral deposits were removed from the synovial tissue, avoiding contamination with underlying bone tissue. Analyses were run over a 2θ diffraction angle range from 10° to 100°, using Ni-filtered CuKα radiation on a Phillips PW 1316/90 wide-range goniometer (Eindhoven, The Netherlands) with an XRG 3100 X-ray generator and graphite monochrometer. The peak of the resulting diffractograms was near 31.80° and is diagnostic for the presence of calcium hydroxylapatite (International Center for Diffraction Data, ICDD Pattern 9-432).
In the thoracic spinal cord, an acute moderate degeneration of the white matter, characterized by myelin sheath swelling, axonal swelling, and axonophagia, was found. In particular, the ventral and ventrolateral funiculi were affected. In the cervical and lumbar spinal cord, similar lesions, albeit milder and diffusely distributed, were present. Thyroid gland, parathyroid gland, adrenal gland, kidney, liver, pancreas, spleen, thymus, salivary gland, heart, intestine, lungs, and eyes were normal. All joints of the limbs and their growth plates were grossly normal. No lesions accounting for the radiographically apparent irregular mineralization of the dens and the “step” defect between C3 and C4 were noticed.
Because of the occurrence of intraarticular calcium mineral deposition with variable degree of fibrocartilaginous proliferation, this case is considered a form of calcium mineral deposition disease. Unusual in this case is the concurrent mineralization of the interarchial ligaments and the extent of the fibrocartilaginous proliferation. The mineral deposition in this puppy probably started on the synovial surface of the diarthrodial facet joints, beneath the ventral longitudinal vertebral ligament and at the interarchial ligaments. However, in human calcium pyrophosphate deposition disease, a related disorder, the earliest deposition is thought to happen at the lacunar margin of chondrocytes and within chondrocytes. 4 , 9 In the presented case and in previous cases of calcium phosphate deposition disease in Great Danes, 12 hydroxylapatite represents the major component of the mineral deposits. The pathogenesis of hydroxylapatite deposition in joints is poorly understood. Because hydroxylapatite is the main mineral constituent of bone, its presence in joints may correlate with bone damage and resorption. 5 However, neither radiographically nor microscopically significant damage of the axial skeleton was found in this Great Dane puppy. This lack of obvious damage may be due to the early state of the disease at euthanasia, as in previous reports of calcium phosphate deposition disease in Great Danes; skeletal alterations, including deformation of vertebral articular processes, displacement of vertebrae, calcifications of growth plate cartilage, and collapse of vertebrae, were present only in older pups. 12 However, these findings may also suggest that the skeletal alterations were secondary to hydroxylapaptite-induced articular lesions.
The early onset of the disease in this Great Dane puppy supports a hypothesis of a congenital disturbance of calcium-phosphorus metabolism or a congenital defect of the intra- or extracellular matrix. The occurrence and equal sex distribution of calcium hydroxylapatite deposition disease in two Great Dane litters with common parents in a previous study suggested an autosomal dominant inheritance. 12 Unfortunately, detailed information regarding the siblings of this affected puppy was not available. The owner of one sibling reported the pup to be normal. A hereditary form of the human disease, characterized by early onset and higher familial incidence, 9 has been reported to be linked to a point mutation in the type II procollagen gene. 1
The histopathologic findings in the present case were similar to those described for calcinosis circumscripta, a disease also characterized by calcium mineral deposition, with associated granulomatous reaction and occasional cartilaginous and osseous metaplasia. It occurs usually as solitary masses in the cutis, subcutaneous periarticular connective tissue, and tongue of young large-breed dogs. 11 The pathogenesis of calcinosis circumscripta is unknown. Lesions, classified as calcinosis circumscripta or calcinosis circumscripta-like malformation and located between the dorsal arches of cervical and thoracic vertebrae were found compressing the spinal cord in eight young large-breed dogs. 2 , 7 , 8 , 10 In these dogs, the lesions were restricted to one or two intervertebral spaces, whereas in the puppy in the present case a widespread involvement of the cervical, thoracic, and lumbar spine was found. However, because only one of these dogs has been necropsied, it is possible that other sites were affected subclinically. Intraarticular mineralization of the facet joints was described in none of those eight dogs. Because of the obvious histopathologic similarities, it is reasonable to speculate on a common pathogenesis of calcinosis circumscripta and the calcium mineral deposition diseases. Alternatively, an almost identical calcinosis circumscripta-like lesion between C1 and C2 of three young large-breed dogs was interpreted as malformation of the chorda dorsalis. 2
Focally, the fibrocartilaginous proliferation in the affected puppy was extensive compared with the relatively sparse intralesional mineral deposition. Because mineral deposition was common to all lesions and because fibrocartilaginous proliferations ranged from slight to marked, the fibrocartilage was interpreted to be reactive and secondary to the mineral deposition rather than due to a malformation. A mitogenic effect of calcium pyrophosphate dihydrate and hydroxylapatite on canine synovial cells has been reported. 3 In humans, mineral deposition disease has been associated with mineral imbalances. 6 However, the biochemical serum profile and the results of the pathologic examination did not indicate any underlying disease process in the presented case.
Footnotes
Acknowledgements
We thank Mr. D. Patton (Biomedia) for photography support.