
Abstract
A 6-year-old spayed female Domestic Shorthair cat presented with a 1 to 2-month history of blindness and altered behavior. At necropsy, a 1-cm-diameter, firm white mass was found arising from the subependymal region of the right lateral ventricular wall that protruded into and partially filled the lumen. Histologically, there was a well-demarcated, expansile paraventricular neoplasm composed of moderately pleomorphic cells within a richly fibrillar matrix arranged in interlacing streams and perivascular pseudorosette-like patterns. Neoplastic cells varied in morphology from small spindloid cells to larger polygonal cells with eccentric vesicular nuclei to neuronlike cells with vesicular nuclei and prominent nucleoli. The mitotic index was low. Immunohistochemically, neoplastic cells were positive for S-100 protein, glial fibrillary acidic protein, and neuron-specific enolase and negative for neurofilament protein. Ultrastructurally, the cells contained few to abundant bundles of intermediate filaments with variable numbers of mitochondria, endoplasmic reticulum, and ribosomes. These features are characteristic of subependymal giant cell astrocytoma (SEGA) in humans. To our knowledge, this is the first reported case of SEGA in domestic animals.
In humans, subependymal giant cell astrocytoma (SEGA) is a rare central nervous system tumor affecting mostly children and young adults. 7 SEGA is most often present in the context of tuberous sclerosis, an autosomal dominant suppressor gene syndrome linked to two genetic loci: TSC1 and TSC2. 5 , 11 Tuberous sclerosis is characterized clinically by seizures, mental retardation, and autism and histopathologically by hamartomas and benign tumors arising in the brain, skin, kidney, and retina. 1 , 4 , 6 The TSC2 gene locus codes for the protein tuberin, which has GTPase activating protein (GAP) activity for Rap1 and Rab5. 3 , 5 , 9–12
This report documents the gross, histologic, immunohistochemical, and ultrastructural features of a feline tumor that are strikingly similar to those of SEGA in humans.
A 6-year-old female Domestic Shorthair presented with a 1- to 2-month history of blindness and altered behavior. Neurologic examination revealed nystagmus to the right, bilaterally decreased pupillary reflexes, proprioceptive deficits of all four limbs, head pressing, and paddling. At necropsy, there was a 1-cm-diameter, well-circumscribed, firm white mass arising from the right lateral ventricle and protruding into the lumen (Fig. 1).
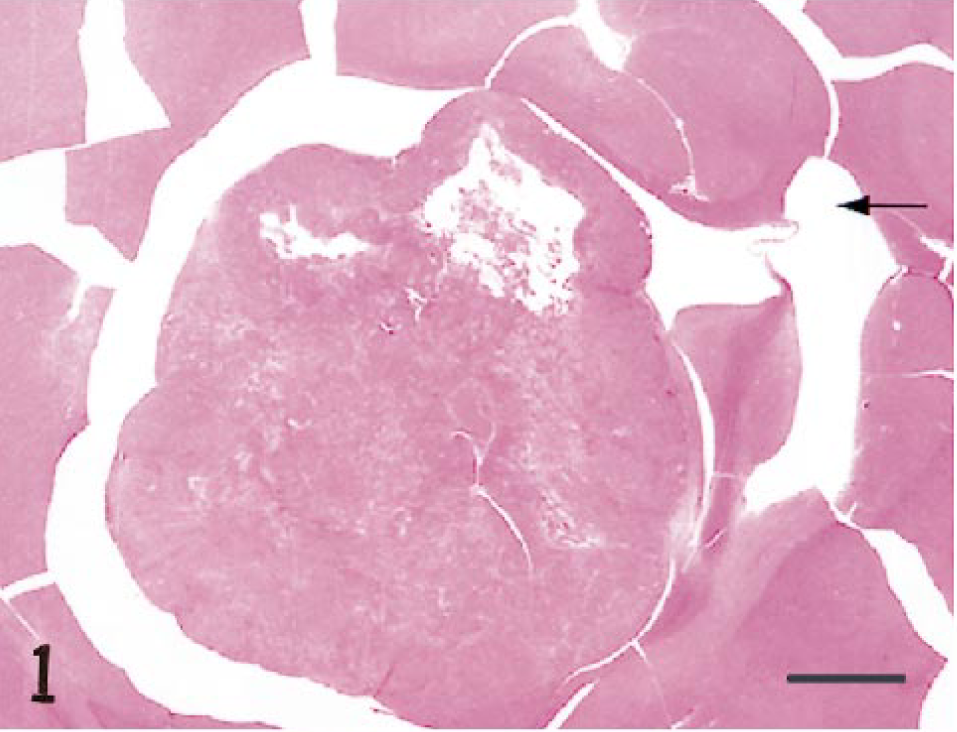
Brain; cat. Subependymal giant cell astrocytoma. A well-demarcated subependymal mass fills and expands the lateral ventricle. Note the third ventricle (arrow). HE. Bar = 3 mm.
The brain was fixed in 10% neutral buffered formalin. Samples from the intraventricular mass and surrounding brain tissue were processed routinely and embedded in paraffin blocks. Sections were cut at 6 mm, mounted on positively charged glass slides (Superfrost Plus, Fisher Scientific, Pittsburgh, PA), and stained with hematoxylin and eosin (HE).
Some formalin-fixed tissue was also postfixed in 1% osmium tetroxide, embedded in effepoxy plastic, sectioned at 800 Å, and stained with uranyl acetate and lead citrate for ultrastructural examination.
Serial sections were immunostained for reactivity to S-100 protein, glial fibrillary acidic protein (GFAP), neurofilament protein (NFP), and neuron specific enolase (NSE) by the avidin–biotin–peroxidase complex (ABC) method. Sections were also stained under identical conditions with normal mouse or rabbit serum to serve as negative controls. All immunostained sections were counterstained with Mayer's hematoxylin.
Histologically, the tumor was a well-circumscribed, moderately cellular, unencapsulated expansile neoplasm, with a fibrovascular stroma, composed of moderately pleomorphic, spindloid to polygonal eosinophilic cells arranged in short interlacing streams and perivascular pseudorosette-like patterns (Fig. 2). The spindloid cells had small amounts of eosinophilic fibrillar cytoplasm, elongated cytoplasmic processes, and round to oval nuclei with densely stippled chromatin and indistinct nucleoli (Fig. 3). The larger globoid and polygonal cells had abundant eosinophilic cytoplasm, oval, vesicular eccentric nuclei, and multifocally discernible multipolar or bipolar cytoplasmic processes (Fig. 4). Occasionally, these cells were neuronlike with large vesicular nuclei, prominent nucleoli, and occasional prominent bipolar cytoplasmic processes (Fig. 4). The remaining neoplastic cells possessed intermediate cellular morphologies. There were rare binucleate cells and few mitotic figures.
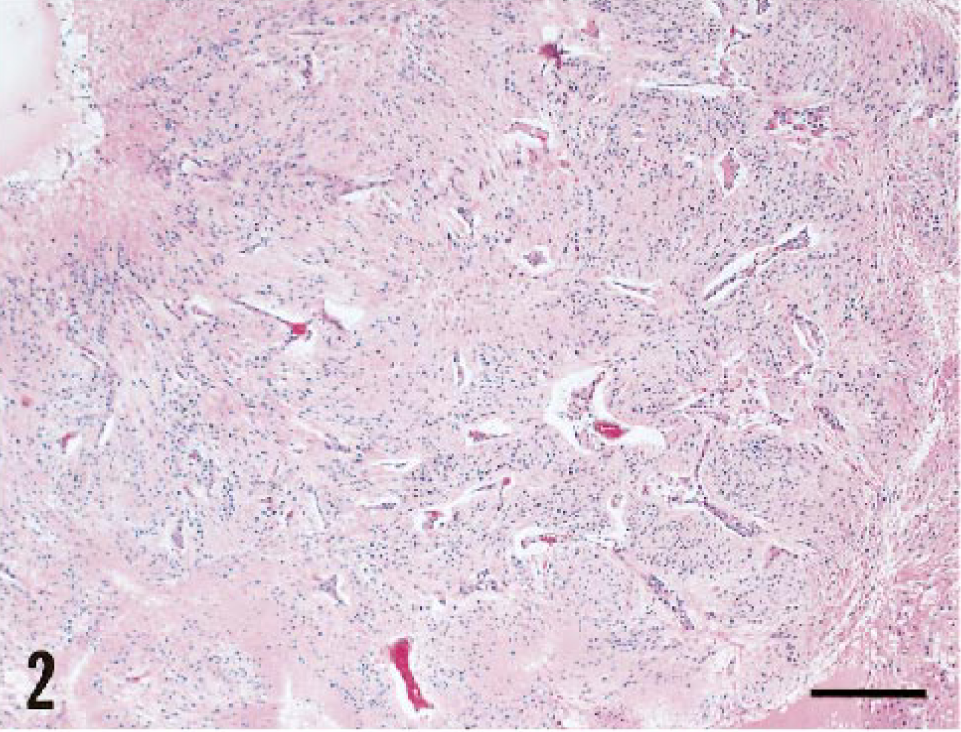
Brain; cat. Subependymal giant cell astrocytoma. Neoplastic cells are arranged in perivascular pseudorosette-like patterns. HE. Bar = 0.25 mm.
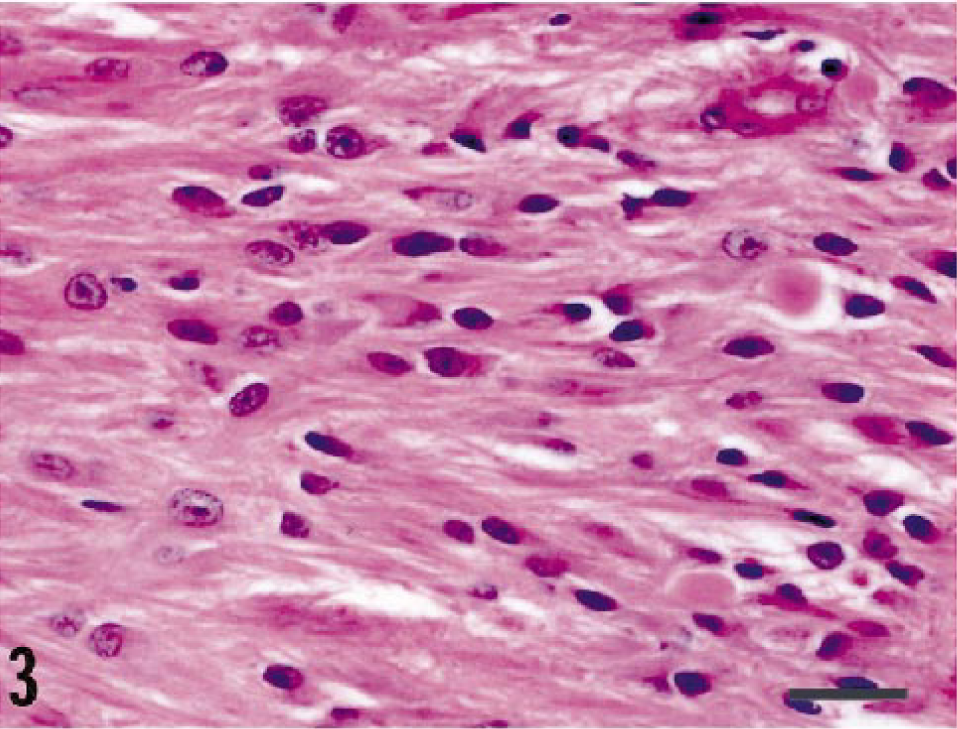
Brain; cat. Subependymal giant cell astrocytoma. Spindloid cells are arranged in streams and have oval nuclei with densely stippled chromatin. HE. Bar = 28 µm.
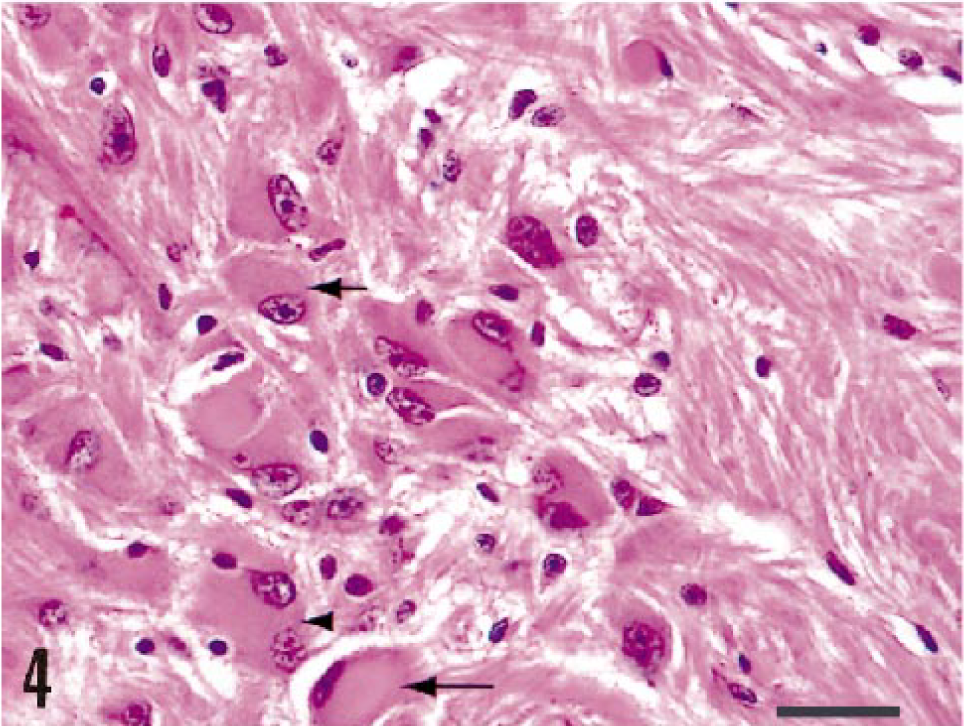
Brain; cat. Subependymal giant cell astrocytoma. Globoid cells (large arrow) have abundant eosinophilic cytoplasm and eccentric nuclei. Neuronlike cells (small arrow) have large vesicular nuclei with prominent nucleoli. Note multinucleated cells (arrowhead). HE. Bar = 33 µm.
Immunohistochemically, the cells were diffusely and strongly positive for S-100 protein (Fig. 5), multifocally positive for GFAP (Fig. 6), rarely positive for NSE, and negative for NFP. The bipolar cytoplasmic processes were occasionally highlighted by GFAP immunostaining.
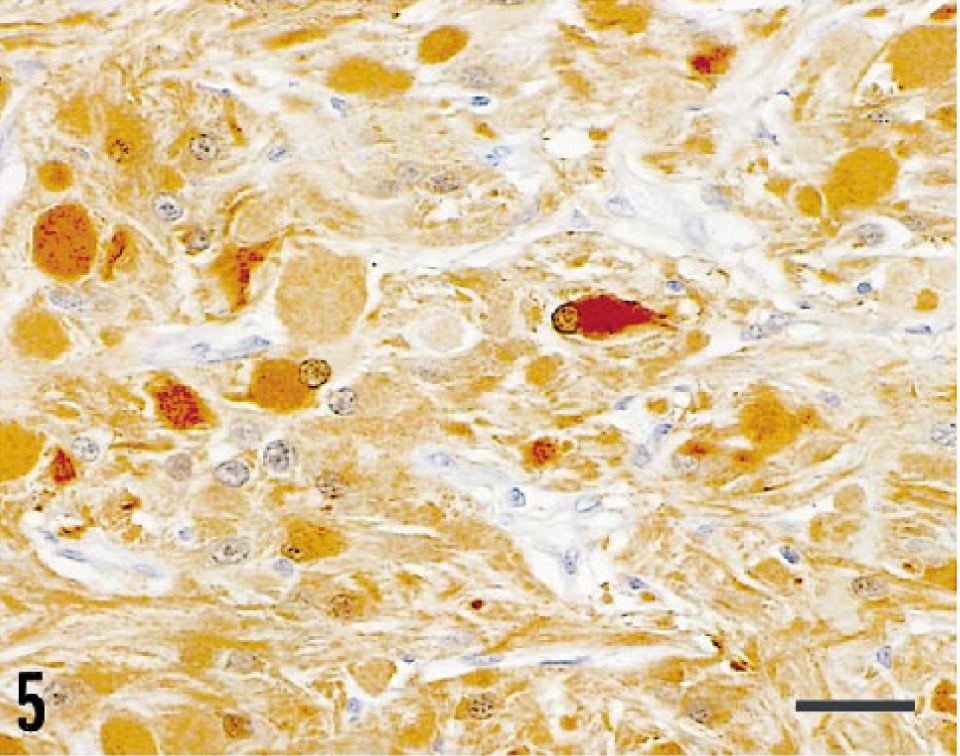
Brain; cat. Subependymal giant cell astrocytoma. The cytoplasm of neoplastic cells stains strongly and diffusely with S-100 protein. ABC and Mayer's hematoxylin counterstain. Bar = 33 µm.
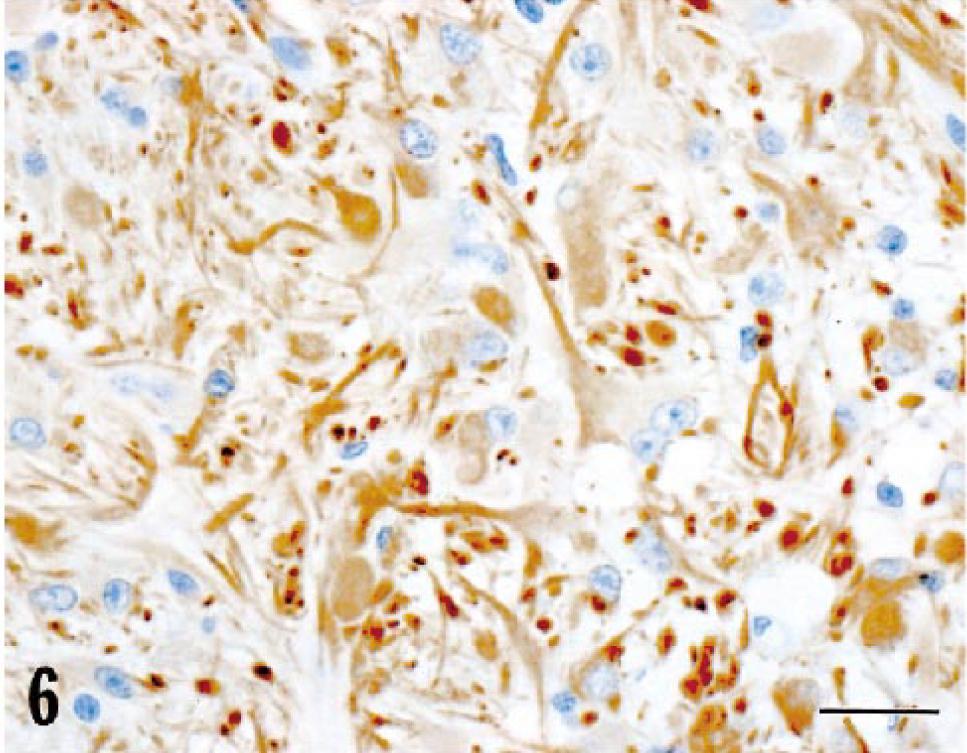
Brain; cat. Subependymal giant cell astrocytoma. Multifocally, neoplastic cells stain strongly for GFAP, and cytoplasmic processes are highlighted. ABC and Mayer's hematoxylin counterstain. Bar = 33 µm.
Ultrastructurally, the spindloid to polygonal neoplastic cells were surrounded by a rich fibrillar background and had moderate to abundant cytoplasm that was either packed with intermediate filaments with few organelles or contained small amounts of intermediate filaments with moderate amounts of endoplasmic reticulum, ribosomes, and mitochondria. There were scattered electron-dense irregular cytoplasmic densities. The nuclei were oval with smooth nuclear membrane outlines, centralized euchromatin, peripheralized heterochromatin, and a single nucleolus.
In humans, SEGAs characteristically arise from the walls of the lateral ventricles, often fill the ventricle, and even obstruct the interventricular foramen. 1 SEGAs are well-demarcated, broadly based tumors that protrude into the lateral ventricle and are often calcified. 4 They are composed of short, interlacing streams of spindloid to polygonal cells within an abundant fibrillar background without incorporation of normal preexistent neural components, and many exhibit a perivascular pseudorosette-like pattern. 2 , 4 Although neoplastic cells vary from spindloid to polygonal, a significant proportion characteristically have abundant eosinophilic cytoplasm, eccentric vesicular nuclei with prominent nucleoli, and multipolar or bipolar cytoplasmic processes. 4 A few neoplastic cells are more neuronlike characterized by large vesicular nuclei with prominent nucleoli. Except for the absence of small numbers of interspersed mast cells, calcification, and intranuclear cytoplasmic inclusions that are commonly observed in human SEGAs, 4 , 6 the gross and histologic features of this feline tumor are characteristic of a SEGA.
The immunohistochemical results are also consistent with the diagnosis of SEGA. Immunohistochemically, cells in human SEGAs are immunoreactive for S-100 protein and variably positive for GFAP. 2 , 4 Some studies have demonstrated cells positive for NFP, NSE, and β-tubulin. 4
The origin and exact nature of SEGAs remain controversial. Most agree that the predominant cellular and ultrastructural phenotype is astroglial. 7 , 11 Some studies have, however, identified scattered cells with poorly differentiated neuronal features. 4 , 8 , 11 Whether these cells represent preexisting structures 11 or neuronal differentiation of primitive neuroepithelial germinal cells 4 , 8 remains uncertain. Some authors have suggested that SEGAs arise from subependymal tuberous foci associated with the tuberous sclerosis complex. 1 Other authors have proposed that they arise from progenitor neuroectodermal cells in the subependymal germinal matrix, which are capable of differentiating into both neuronal and glial cells. 1 , 4 , 8 Both theories suggest abnormal differentiation and migration as a common factor. Whether these mechanisms represent a primary dysplastic or neoplastic process is still a subject of debate. 6 , 8 The electron microscopic findings of the tumor cells in this case are consistent with an astrocytic phenotype.
Eker rats are also affected by a germ-line autosomal dominant mutation of the TSC2 gene locus (10q12 in rats) and serve as useful animal models for tuberous sclerosis. 11 , 12 The CNS lesions in rats, however, are limited to smaller (< 2 mm), less disruptive subcortical and subependymal hamartomatous nodules. 11 Immunohistochemically, a majority of the cells are multifocally positive for GFAP, and rare cells are positive for NFP. 11
The differential diagnosis in this case includes a gemistocytic astrocytoma and medium-grade astrocytoma. 2 Unlike gemistocytic astrocytomas, this neoplasm was well demarcated. Additionally, the globoid cells in gemistocytic astrocytomas are not typically as large as the cells observed in this case. Neoplastic gemistocytic astrocytes are more diffusely distributed, rather than arranged in interlacing streams and perivascular pseudorosette-like patterns, as in this case. 2 Furthermore, the cytoplasmic processes of the cells in this tumor often emanate in a bipolar fashion that distinguishes them from the more evenly arranged short processes observed in gemistocytic astrocytomas. 2 This case markedly differs from medium-grade astrocytomas in as much as it lacks evidence of an increased mitotic rate, infiltration, and anaplastic cellular and nuclear features.
This feline intraventricular neoplasm possesses gross, histologic, immunohistochemical, and ultrastructural features that are consistent with the SEGA described in humans. To our knowledge, this is the first reported case of SEGA in domestic animals and more closely resembles human SEGA than the astrocytic hamartomas described in Eker rats. We hope this case report will alert veterinary clinicians and pathologists to include this novel feline CNS tumor in their differential diagnosis of brain neoplasms, especially those with para- and intraventricular locations.
Footnotes
Acknowledgements
We thank Dr. Paul Stromberg for contributing this interesting case, Ms. Robin-Anne V. Ferris, MFS, Ms. Tracey Hamilton, and Ms. Theresa Tezak-Reid for photographic support, and Mr. John Jenkins, HT, HTL ASCP, for electron microscopic service.