
Abstract
Neuronal vacuolation and spinocerebellar degeneration is a rare, presumably inherited condition that is reported only in Rottweilers and in crossbred dogs with known or potential Rottweiler heritage. Gross and histopathologic findings include laryngeal muscle atrophy, neuronal vacuolation, and a combined central and peripheral axonopathy. Two 6-month-old Boxer puppies from the same litter were referred for evaluation of progressive pelvic limb paresis and ataxia, upper airway stridor, and visual deficits. Examination of each dog suggested a combined myelopathy and peripheral neuropathy, as well as congenital ocular disease. Gross lesions were limited to atrophy of the intrinsic laryngeal muscles. Histopathologically, there was diffuse loss of axons and myelin in the dorsolateral and ventral funiculi throughout the spinal cord and extending into the caudal aspect of the brain stem. Vacuolation of scattered neuronal cell bodies was present in the spinal cord and selected brain stem nuclei. Multifocal axonal degeneration and demyelination was observed in the recurrent laryngeal nerve, sciatic nerve, and brachial plexus and was most severe in the recurrent laryngeal nerve. Ocular abnormalities included microphthalmia, cataracts, and retinal dysplasia. The findings in these Boxer dogs, unrelated to the Rottweiler breed, are analogous to the syndrome of neuronal vacuolation and spinocerebellar degeneration reported in Rottweilers.
Keywords
Neuronal vacuolation and spinocerebellar degeneration (NVSD) is a rare neurologic disorder that has been reported in Rottweilers and in crossbred dogs with known or potential Rottweiler heritage.1, 4–6, 8, 10–12, 14 Gross lesions attributed to the syndrome are restricted to atrophy of the intrinsic laryngeal muscles, whereas histopathologic findings include neuronal vacuolation in selected brain stem nuclei and spinal cord neurons in combination with an axonopathy in the recurrent laryngeal nerve and selected spinal cord funiculi.6 The disease manifests at an early age, and, due to time of onset and restriction to one dog breed, a genetic defect is likely.10 We report 2 6-month-old Boxer dog littermates, referred for evaluation of progressive neurologic and ocular deficits, in which postmortem examination disclosed an identical encephalomyelopathy and polyneuropathy to that described in Rottweilers.
Two 6-month-old Boxer dog littermates, 1 female (dog No. 1) and 1 male (dog No. 2), were referred independently for progressive pelvic limb paresis and ataxia, upper airway stridor, and poor vision. Physical examination of both dogs confirmed inspiratory stridor in addition to bilateral microphthalmia, cataracts, and multifocal linear retinal folds. Neurologic examination was identical for both dogs. The gait was characterized by spastic, upper motor neuron paresis and general proprioceptive ataxia in the pelvic limbs with normal thoracic limb function. Postural reactions were delayed markedly in the pelvic limbs but were normal in the thoracic limbs. All segmental spinal reflexes were normal, and cranial nerve examination was normal, with the exception of a mild menace deficit bilaterally. Neuroanatomic localization was made to the third thoracic to third lumbar spinal cord segments and to the recurrent laryngeal nerves. The differential diagnosis included neurodegenerative disorders (neuroaxonal dystrophy, atypical degenerative myelopathy, lysosomal storage disorder) and infectious/inflammatory disorders (myelitis/neuritis due to canine distemper virus, Neospora caninum, Toxoplasma gondii, or noninfectious meningomyelitis). Neurodiagnostic testing was declined by both owners, and, due to the progressive neurologic signs, both animals were humanely euthanatized, and a complete necropsy examination was performed.
After necropsy, tissue sections were fixed in 10% neutral buffered formalin, embedded in paraffin, sectioned at 5 μ, and mounted on glass slides. Transverse and longitudinal spinal cord sections were stained with hematoxylin and eosin, and selected sections were stained with Luxol fast blue and Bielschowsky silver stain. Immunohistochemical staining using a 1:300 dilution of neurofilament protein antibody (DAKO) was performed using an Austainer plus (Dakocytomation, Carpinteria, CA). Diaminobenzidine chromagen was used as the substrate, and the slides were counterstained with hematoxylin. Sections of the left and right recurrent laryngeal nerve were stained with Masson's trichrome.
Grossly, all intrinsic muscles of the larynx, except for the cricothyroideus muscle, were atrophied (Fig. 1). The degree of atrophy was variable, but the most severe atrophy was confined to the cricoarytenoideus dorsalis muscle. No other gross abnormalities were noted in either animal.

Larynx; dog No. 2. There is bilaterally symmetric atrophy of the intrinsic muscles of the larynx.
Histopathologic examination of the spinal cord revealed axonal degeneration and myelin loss that was most severe in the thoracic segments. This lesion was bilaterally symmetric and almost completely confined to the lateral (especially dorsolateral) and ventral funiculi (Fig. 2). The most superficial white matter tracts were affected to the greatest degree. Bielschowsky silver stain revealed a marked loss in axon number in the ventral and lateral funiculi with sparing of the dorsal funiculi. Luxol fast blue histochemical staining revealed a similar focused distribution of the myelin loss to the ventral and lateral funiculi (Fig. 3). Neurofilament immunohistochemical staining revealed loss of large axons in the superficial tracts, most notably in the dorsolateral funiculi (Fig. 4). These lesions were accompanied by mild to moderate astrogliosis. Roughly 5% of the neuronal cell bodies in the spinal cord gray matter contained one or more 5–30-μm-diameter clear cytoplasmic vacuoles. Additionally, several small blood vessels in the leptomeninges of dog No. 1 were partially to completely obscured by perivascular and intravascular lymphocytes and fewer macrophages and neutrophils. These blood vessels had marked, asymmetric thickening of the tunica media with decreased luminal diameter.
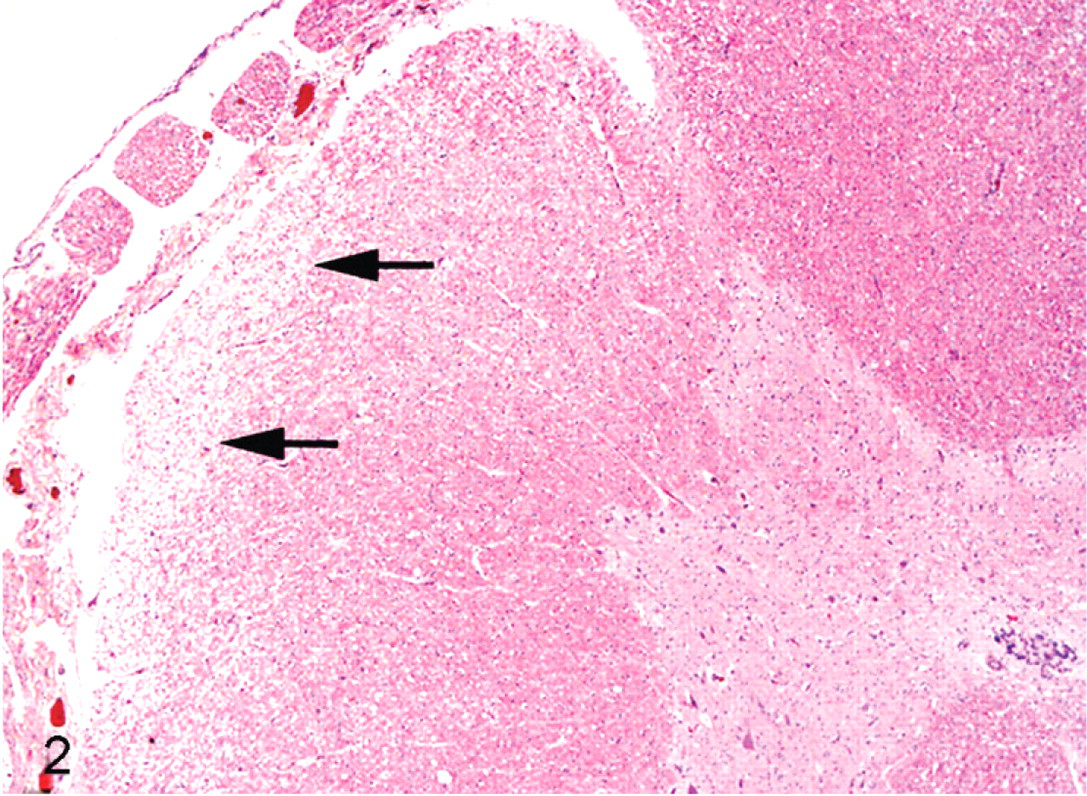
Thoracic spinal cord; dog No. 2. The superficial tracts within the lateral and dorsolateral (arrows) funiculi are diffusely pale. HE.
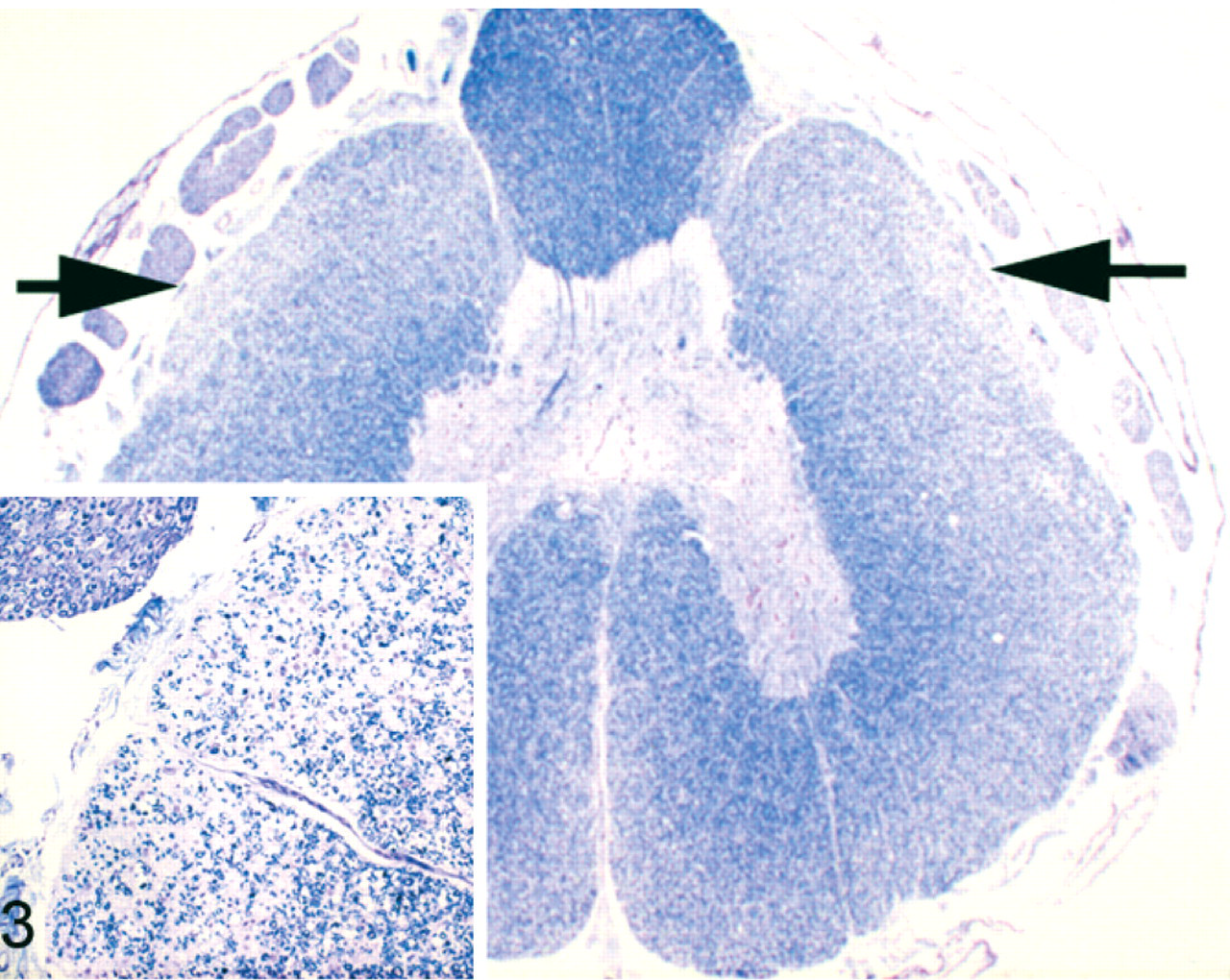
Thoracic spinal cord; dog No. 1. Pallor along the dorsolateral and ventral funiculi indicates marked demyelination (arrows). Inset: higher magnification of the affected funiculi with myelin loss and astrogliosis. Luxol fast blue.
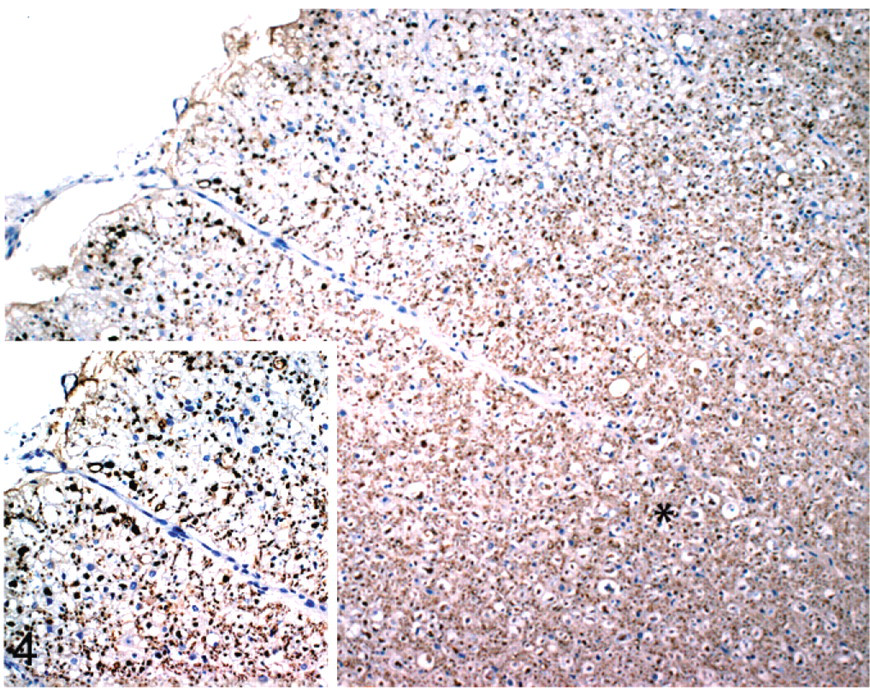
Thoracic spinal cord; dog No. 1. Decreased immunoreactivity in the superficial tracts, compared with the normal deeper tracts (asterisk), indicates axonal loss. Inset: higher magnification of affected funiculi illustrating decreased axon density and resulting gliosis. Neurofilament immunohistochemistry counterstained with Dako's hematoxylin.
Similar, albeit much less severe, axonal degeneration and myelin loss were observed in the caudal brain stem tracts that may have been an extension of the spinal cord lesions. No lesions were seen in the prosencephalon or mesencephalon. Neuronal cell body vacuolation similar to that seen in the spinal cord also was identified in the following brainstem nuclei: motor nucleus of the trigeminal nerve, vestibular nuclei, cerebellar nuclei, and lateral cuneate nucleus. The vacuolations were bilaterally symmetric and most severe in the motor nucleus of the trigeminal nerve (Fig. 5).
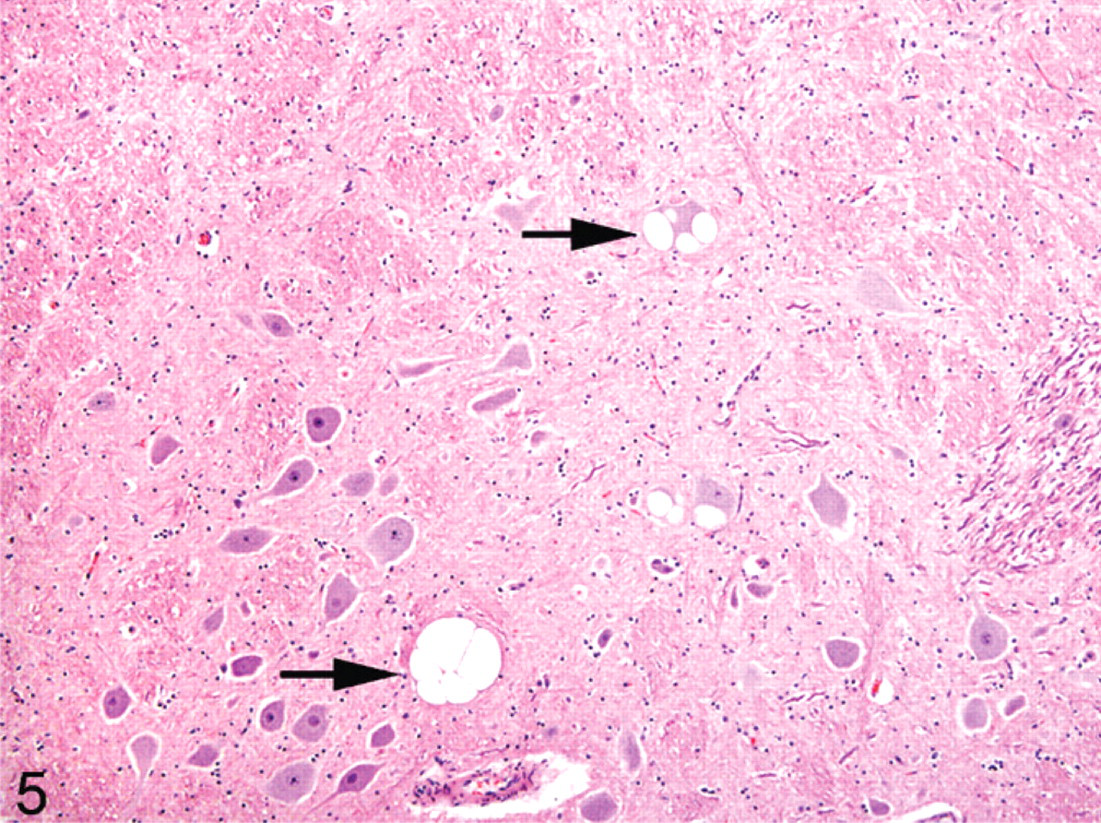
Brain stem, motor nucleus of the trigeminal nerve; dog No. 2. Expanding the cytoplasm of numerous neurons are large, occasionally multilocular, clear vacuoles (arrows). HE.
Histopathologic examination of the recurrent laryngeal nerves revealed multifocal loss of myelinated axons and numerous Büngner's bands. Masson's trichrome stain revealed marked endoneurial fibrosis in the affected nerves. The areas of fibrosis were interspersed with scattered fascicles of normally myelinated axons (Fig. 6). Myelin debris and ovoids were also found in the sciatic nerve and the brachial plexus. Histopathologic examination of the cricoarytenoideus dorsalis muscle disclosed large groups of atrophied myofibers accompanied by scattered hypertrophied myofibers. Additionally, scattered necrotic muscle fibers were undergoing phagocytosis.
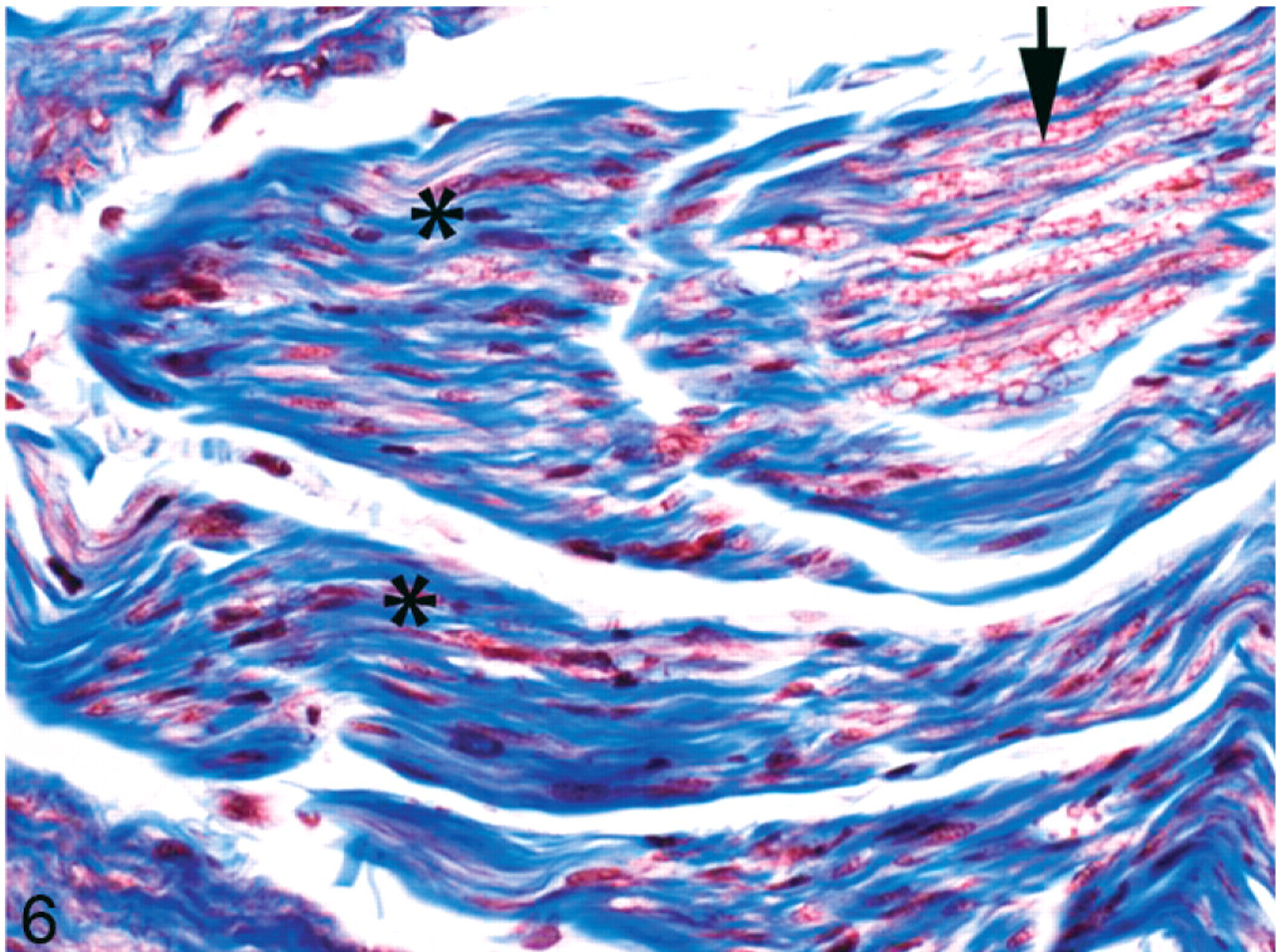
Recurrent laryngeal nerve; dog No. 1. Abundant endoneurial fibrosis (asterisks) has replaced multiple nerve fascicles. Scattered nerve fascicles remain unaffected (arrow). Masson's trichrome stain.
Histologically, the eyes were affected by bilateral microphthalmia, cataracts, and retinal dysplasia. Cataract formation was most prominent in the posterior cortical and perinuclear regions. Dysplastic retinal folding was concentrated centrally.
The clinical and histopathologic changes identified in the 2 dogs of this report are identical to those in the degenerative encephalomyelopathy and peripheral neuropathy reported as NVSD in young Rottweilers and Rottweiler crossbred dogs. Published Rottweiler cases have ranged from 3 to 13 months of age and were recognized in Europe, the USA, Brazil, and Australia.1, 3, 5, 6, 8, 10, 12, 14 A similar disease was reported in a mixed breed dog of unknown heritage.11 Before formal publication of NVSD in Rottweilers by Kortz et al.,6 2 additional dogs with identical diseases were reported2, 9 and subsequently were suggested to be cases of NVSD.3, 5
The primary clinical abnormalities in the published Rottweiler cases and in the Boxer dogs in this report include upper motor neuron paresis and general proprioceptive ataxia with variable degrees of laryngeal paresis or paralysis. In affected Rottweilers, the gait abnormalities were marked in the pelvic limbs but over time occasionally progressed to involve the thoracic limbs. Ocular lesions were found concurrently in 5 of the reported dogs and included persistent pupillary membranes, bilateral cataracts, and enophthalmos.5, 12 Similar to the Boxer dogs reported here, the only consistent gross pathologic finding in affected Rottweilers was atrophy of the cricoarytenoideus dorsalis and other intrinsic laryngeal muscles. Several reports exist of megaesophagus in affected Rottweilers, although this is an inconsistent observation.1, 4, 10 The major histopathologic findings were varying degrees of neuronal vacuolation, axonal degeneration with secondary demyelination, astrogliosis in the central nervous system, and selective axonal loss with demyelination in the peripheral nervous system, particularly in the recurrent laryngeal nerves. Neuronal vacuolation was most striking in brain stem and cerebellar nuclei, whereas white matter lesions (axonal degeneration with demyelination and astrogliosis) were confined to the dorsolateral and ventral funiculi of the spinal cord. As in the Boxer dogs of this report, the lesions were most severe in the thoracic spinal cord segments. Unexpectedly, localized arteritis and vascular thickening was observed within the caudal cervical spinal cord in dog No. 1. These lesions were mild and consistent with steroid-responsive meningitis, a disease reported commonly in the Boxer breed and unrelated to the disseminated spinal cord lesion and neuronal vacuolation.13
In addition to the central nervous system lesions, affected Rottweilers also had signs and lesions indicative of a peripheral neuropathy. The most significant peripheral nervous system lesion reported was selective loss of large myelinated fibers in the recurrent laryngeal nerves coupled with denervation atrophy of the intrinsic laryngeal musculature. An identical lesion was noted in the 2 Boxer dogs of this report, confirming a combined myelopathy and peripheral neuropathy. The necrotic myofibers and concurrent lymphocytic inflammation in the denervated muscle are likely a consequence of overexertion of the atrophied muscles rather than a direct consequence of the neuropathy.
A majority of the reports of NVSD in Rottweilers described multifocal peripheral nerve lesions beyond those in the recurrent laryngeal nerves, suggesting that a polyneuropathy accompanies the central nervous system lesions.2, 4, 6, 10, 14 Among the reports that lack explicit evidence of polyneuropathy, few document thorough collection and examination of multiple peripheral nerves. A notable exception is the detailed examination of 2 affected Rottweilers by Salvadori et al., which found only recurrent laryngeal nerve lesions despite thorough investigation.12 Because the clinical features of NVSD in Rottweilers are reported to arise over a variable period and in inconsistent order, similar variation in the range of observed histopathologic lesions can be expected.3 Although clinical signs of diffuse lower motor neuron disease are uncommon in NVSD, the consistent histopathologic finding of polyneuropathy in most reports warrants its inclusion as a feature of the disorder.
Appropriate semithin resin sections evaluated by light microscopy and ultrathin electron microscopic examination of peripheral nerves are vital to proper interpretation of suspected neuropathies.10 In the present Boxer dog cases, due to tissue submission and processing protocols, tissue was processed only in paraffin. Although exhaustive evaluation of the peripheral nerve pathology was not possible, nerve fiber loss and degeneration coupled with marked endoneurial fibrosis confirms the presence of peripheral neuropathy in this syndrome as in NVSD of Rottweilers.
The etiopathogenesis of the combined encephalomyelopathy and polyneuropathy in Rottweilers and Boxers remains elusive. Based on microscopic similarities to the transmissible spongiform encephalopathies, a prion-related disease etiology has been postulated. However, immunohistochemical and electron microscopic investigations of Rottweilers have revealed no evidence of prion disease, making such a mechanism unlikely.5, 6, 10, 14 Given the disease predilection for specific breeds, familial association, and age of onset, an inherited mechanism is strongly suspected. Although a similar human disease is not recognized, the recently completed map of the canine genome should facilitate genetic linkage studies.7
The neuropathologic and ocular lesions identified in these related Boxer dogs represent a new neurodegenerative disorder within the breed. The findings in these dogs are nearly identical to those of so-called NVSD previously described in Rottweilers.1, 3, 5, 6, 8, 10, 12, 14 We suggest that NVSD is a misleading name for this disorder in either breed. Most important, the central nervous system lesions are not confined to the spinocerebellar tracts, and the name excludes the involvement of the peripheral nervous system, which is of nosologic importance and a critical diagnostic feature. Second, the term “spongiform” overstates the distribution of neuronal vacuoles. Although the neuronal vacuolation imparts a “spongiform” quality to the neurons, there is a lack of vacuoles within the adjacent parenchyma. Due to the central and peripheral lesions in this syndrome, we suggest that this phenotype is best referred to as a combined encephalomyelopathy and polyneuropathy associated with neuronal vacuolation.