
Abstract
All male and female New Zealand white rabbits in a limbal cell graft study developed marked generalized mammary gland hypertrophy. Postprocedural medications included ophthalmic 0.1% dexamethasone, ophthalmic 0.5% cyclosporine, and subcutaneous cyclosporine A. Cytologic examination revealed epithelial clusters with minimal malignant criteria. On histologic evaluation, there was diffuse glandular hyperplasia with mild cellular atypia and ductal ectasia separated by abundant hypercellular fibrous stroma, consistent with fibroadenomatous mammary gland hyperplasia. The hyperplasia resolved within 2 weeks of cessation of cyclosporine, and at necropsy identifiable mammary masses were not found. Very little has been reported about the use of cyclosporine in laboratory rabbits and its association with development of mammary gland hyperplasia. This is the first report in which administration of cyclosporine to male and female rabbits at a dose as low as 5 mg/kg/day induced benign fibroadenomatous mammary gland hyperplasia. This change regressed after cessation of the drug.
Cyclosporine A (CSA) is a potent, commonly used immunosuppressant with selective helper T-lymphocyte action that is typically used to prevent rejection in organ transplantation.11, 23 Reported complications of cyclosporine administration in dogs include gastrointestinal disturbances, dermatologic changes (especially transient alopecia), gingivitis, and gingival hyperplasia, whereas there are few cases of gastrointestinal problems and hypertension reported in cats.1, 19 Frequent complications of CSA administration in humans include hepatic and renal toxicity, hypertension, cutaneous lesions, neurologic abnormalities, and gingival hyperplasia.11, 18 Multiple benign mammary changes have also been reported in 11–45% of women renal transplant recipients receiving CSA therapy, with variation in the duration of CSA treatment and speed of onset.3, 25 The most common lesions in women are benign fibroadenomas, fibrocystic changes, and dense fibrosis with vascular ectasia.3, 25 These lesions can regress, depending on the duration of treatment and degree of fibrosis upon drug withdrawal.25 Gynecomastia in male liver transplant patients has also been reported in association with CSA and can also resolve after cessation of treatment.14 An association between these benign mammary diseases and the circulating level of CSA has not been found, nor is there any association with mammary neoplasia.25
To our knowledge, mammary changes associated with CSA have only been reported once in the veterinary literature; this was in female New Zealand white rabbits with a continuous intravenous CSA drip at a rate of 2 mg/kg/minute for 14 days (equivalent to 10 mg/kg/day).21 CSA-induced mammary hyperplasia has not been reported at a lower dose or in male rabbits and has not been evaluated by cytology.
Rabbits are a preferred animal model for human corneal epithelial reconstruction studies. In this report, a total of 20 of New Zealand white rabbits (9 males and 11 females in staggered cohorts of 4–6 animals) received corneal transplants over a period of 5 months in a study for aniridic keratopathy treatment. The transplants were created by culturing limbal cells, harvested from 3 other New Zealand white rabbits, on human amniotic membranes. At surgery, limbal and superficial corneal tissue was removed from one of each rabbit's eyes and the limbal-seeded amniotic membrane was transplanted to cover the limbal peritomy and keratectomy site. Nine of the 20 rabbits (5 males/4 females) had ocular membrane transplants that had not been seeded with limbal cells, but all rabbits had ocular surgery and received all medications.
Rabbits were evaluated for general health after surgery daily throughout the entire experiment and were given a complete ophthalmic examination for the first 2 days and then at least twice weekly for the remaining 14 days. At the study completion, globes were removed after euthanasia and histologically evaluated for analysis of the transplants.
Postoperative analgesia included subcutaneous butorphanol 0.5 mg/kg every 4–6 hours and subcutaneous buprenorphine 0.01–0.05 mg/kg every 8–12 hours for 2 days. Immunosuppressive and preventative treatment consisted of topical antibiotics (ofloxacin 0.3% ophthalmic solution every 6 hours), topical steroids (0.1% dexamethasone every 6 hours), and topical CSA (0.5% every 6 hours) on the subject's eye throughout the study. Experimental animals also received enrofloxacin (5 mg/kg subcutaneously twice daily) for 7 days and subcutaneous CSA (5 mg/kg/day) for 1 week and then at half dose for the following 3 weeks. Surgical procedures were in accordance with the Association for Research in Vision and Ophthalmology Statement for Use of Animals in Ophthalmic and Vision Research and approved by the University of Georgia Institutional Animal Care and Use Committee. The University of Georgia University Research Animal Resources section is accredited by the Association for Assessment and Accreditation of Laboratory Animal Care, International.
Twenty-two days after ocular surgery and indicated medical treatment, the first cohort of 6 rabbits (1 male, 5 females) were noted to have multiple enlarged mammary glands. The enlarged mammary tissue from 1 female rabbit was aspirated (22-gauge needle, 3-ml syringe), and cytologic aspirate preparations were made. The slides were routinely stained with modified Wright's stain. On examination, there were variably preserved small epithelial clusters scattered throughout the slides (Fig. 1). Cells were mildly jumbled and had moderate pale cytoplasm with indistinct borders and few small clear punctate vacuoles. Nuclei were rounded to slightly oval and central with coarsely granular chromatin and inconspicuous nucleoli. The background of many cytology aspirates had a few scattered foamy macrophages with digested debris and serous to proteinaceous eosinophilic fluid (Fig. 2). There was no evidence of inflammation or sepsis.
A different affected female rabbit from the same cohort was necropsied the following day. Mammary tissues were formalin fixed and paraffin embedded, and 3-μm sections were prepared and stained routinely with hematoxylin and eosin. On histologic examination, there were loosely demarcated lobules composed of mammary gland tubules surrounded and separated by an abundant hypercellular stroma of spindle cells (Figs. 3, 4). In the areas with most abundant stroma, the mammary tubules were larger, variably ectatic, and more widely separated. The epithelium lining the tubules had smaller basophilic cells. Isolated dilated lymphatic vessels were present and were more prominent in the latter areas.
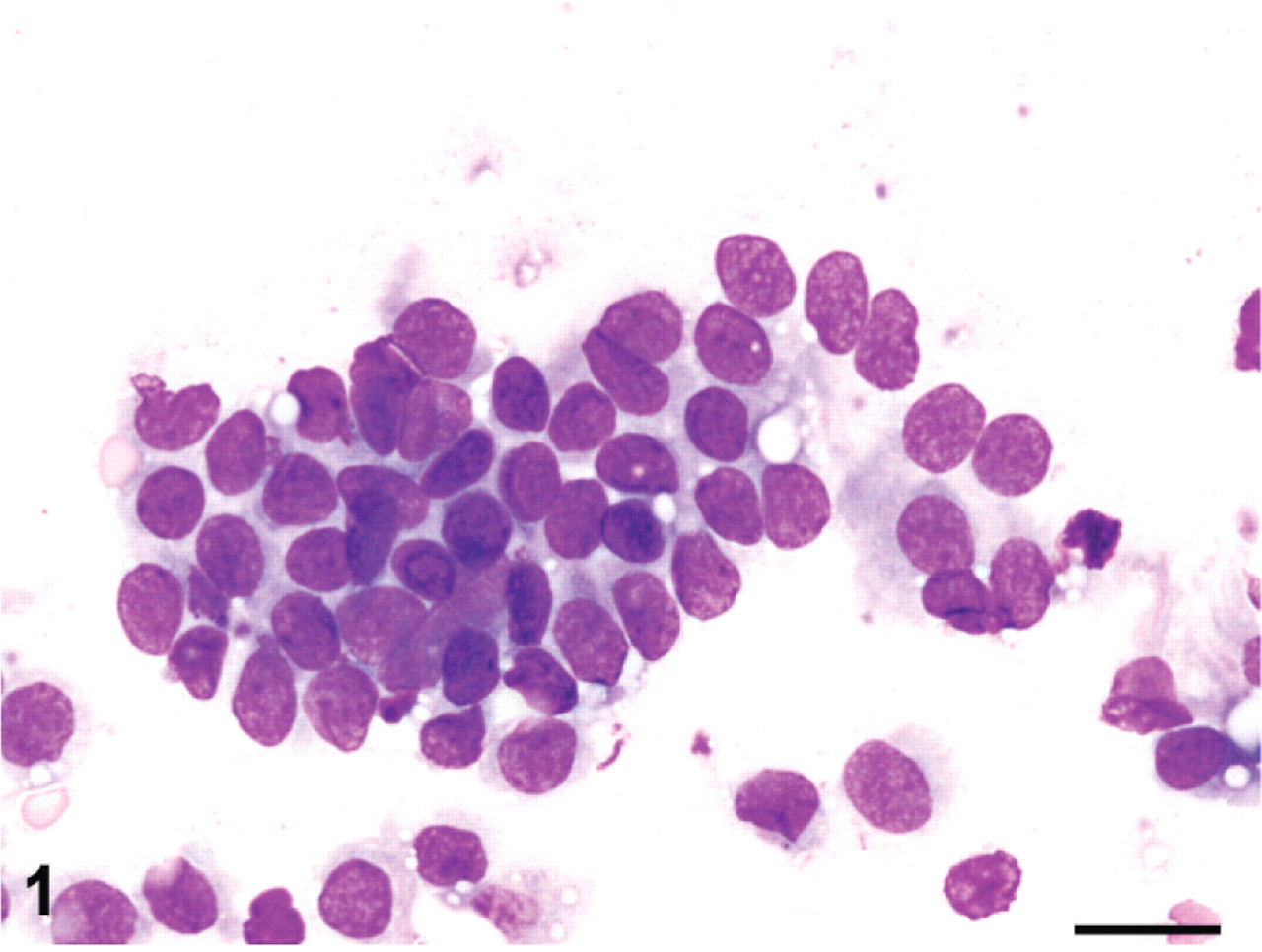
Mammary tissue from cytologic aspirate; rabbit, case 1. Clusters of epithelial cells with minimal anisocytosis, anisokaryosis, clumped chromatin, and inconspicuous nucleoli. Modified Wright's stain. Bar = 50 μm.
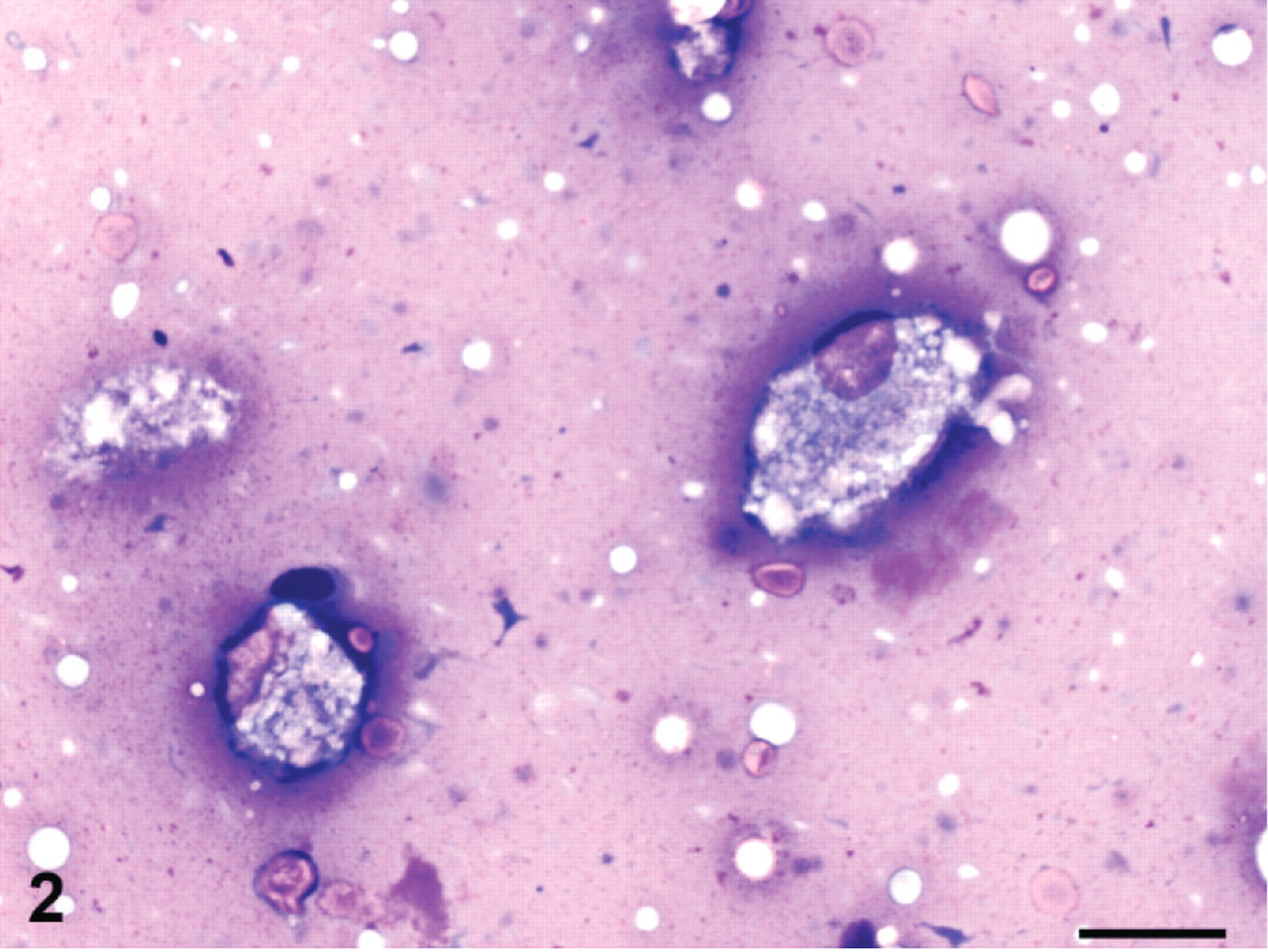
Mammary tissue from cytologic aspirate; rabbit, case 1. Scattered foamy macrophages with digested debris in a granular eosinophilic proteinaceous background were present on most cytology aspirates. Modified Wright's stain. Bar = 10 μm.
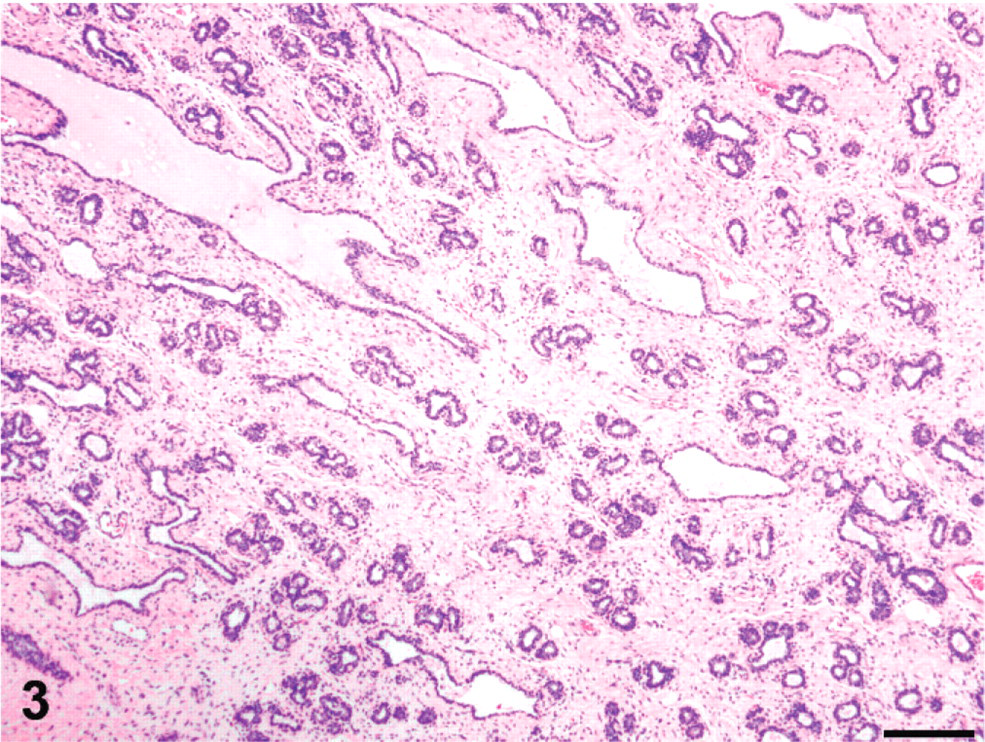
Mammary tissue on histologic biopsy; rabbit, case 2. Prominent hyperplastic stromal tissue separates variably ectatic mammary glands, which sometimes contain homogeneous palely eosinophilic serous fluid. HE. Bar = 200 μm.
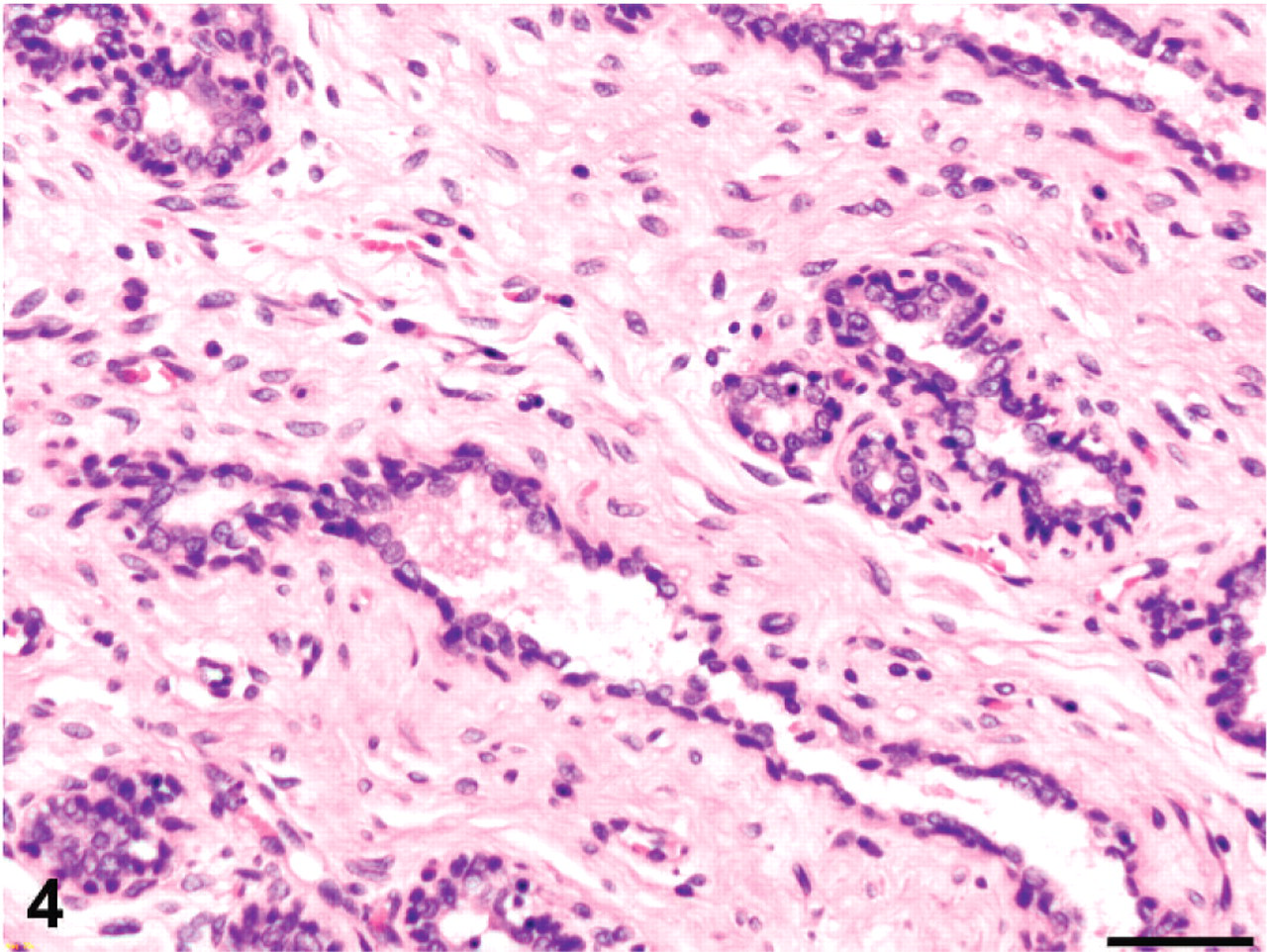
Mammary tissue on histologic biopsy; rabbit, case 2. The stroma has increased cellularity without cellular atypia, and mammary gland epithelium has minimal pleomorphism. HE. Bar = 50 μm.
Topical CSA was discontinued at day 28, and palpable mammary gland hyperplasia completely resolved in all rabbits within 14 days of withdrawal of the CSA. All 20 rabbits in the study developed mammary hyperplasia. Postmortem examination of the remaining 19 rabbits at termination of the study, 45–48 days after surgical manipulation and 17–26 days after cessation of CSA treatments, did not reveal any grossly identifiable mammary masses in any animal.
Cyclosporine-induced reversible mammary hyperplasia has been previously reported in female New Zealand White rabbits but not in males.21 In the prior study, CSA was administered through continuous intravenous drip at a rate of 2 mg/kg/minute for 14 days, equivalent to 10 mg/kg/day, and some rabbits also received concurrent methylprednisolone. In that study, rabbits receiving concurrent CSA and methylprednisolone immunosuppressive treatment had larger mammary gland hyperplasia than did those on CSA alone. Such gland enlargement correlated well with increased serum prolactin and 17 beta-estradiol and decreased serum progesterone.21 In women, only 1 case with unequivocal elevation in prolactin level has been found, and that patient was also receiving a calcium channel blocker.20
The precise mechanism for CSA-induced mammary changes has not been determined. Cyclosporine does prevent the binding of prolactin to receptors that results in hyperprolactinemia, and this is presumed to be at least a contributor to the mammary hyperplasia.5, 10 Prolactin has actions that are generally categorized as 1) water and electrolyte balance, 2) growth and development, 3) endocrinology and metabolism, 4) brain and behavior, 5) reproduction, and 6) immunoregulation and protection.6 The prolactin receptor is a type-I cytokine-type receptor with 4 isoforms and multiple signaling pathways, including Janus kinase–signal transducer and activator of transcription, mitogen-activiated protein kinase, and phosphoinositide 3 kinase.4 Due to its diverse physiologic functions, the prolactin receptor is expressed in most tissues, with the ratios of particular isoforms varying by tissue, as well as by developmental and reproductive stages.4
The combination of varying isoforms and multiple signaling pathways for the prolactin receptor provides room for speculation on the mechanisms of cyclosporine induction of mammary hyperplasia. Selective blockage of only certain isoforms of the receptor by cyclosporine (especially those involved in immune functioning, such as in leukocytes) would still cause a compensatory hyperprolactinemia. However, the isoforms that predominate in the mammary gland would be unaffected and respond normally to the increase in circulating prolactin by causing mammary hyperplasia. Alternatively, generalized interference with all prolactin receptors would cause a compensatory hyperprolactinemia, but the relatively high proportion of receptors in the mammary tissues would result in some receptor activation and mammary hyperplasia.
In support of the latter hypothesis, rabbits appear to have an increased number of prolactin-binding sites on mammary gland cells relative to other species and as such may be more susceptible to this effect.26 Pharmacokinetic studies of CSA in pregnant rabbits (in which mammary gland tissue is abundant and readily assayed) show that although mammary concentration of CSA is notable, it is less than in spleen, fat, and kidney, and that proportionally the liver, fat, and muscle stored the most drug.23 Hence, mammary hyperplasia is not related to preferential distribution to this organ. There are differences in CSA hepatic metabolism between species,27 and the consequent variation in metabolite concentrations could also play a role in species-specific adverse reactions.
Concurrent use of methylprednisolone in combination with CSA suggests that this corticosteroid may contribute to the development of mammary hyperplasia in the rabbit.21 The interaction between different steroids and CSA is complex, with conflicting study results.15 Some investigators postulate that corticosteroids could inhibit hepatic metabolism of CSA.15 This would increase circulating levels or induce the cytochromes necessary for its metabolism, which would lower circulating levels. Both mechanisms have been reported with methylprednisolone, although with dexamethasone only a decrease in circulating CSA has been reported.15 In general, methylprednisolone is considered a more potent immunosuppressive and anti-inflammatory agent than dexamethasone at similar doses,12 and therefore the dexamethasone administered to our rabbits is unlikely to have been a critical factor in their mammary hyperplasia.
Although the systemic levels of exogenous corticosteroids in this study were not determined, multiple studies have shown that topical ophthalmic steroids absorb systemically with quantifiable systemic effects, including reduced plasma cortisol, detectable urine dexamethasone, hepatic vacuolar change, and adrenal cortical atrophy.7 Furthermore, although some topically applied ocular CSA may have been absorbed, it is unlikely to have raised blood levels to an equivalent of 10 mg/kg/day. Ocular penetration of ofloxacin is low in people, and systemic absorption is unlikely.9 Ofloxacin and enrofloxacin are fluoroquinolone antibiotics; hormonal alterations or mammary gland changes have not been reported with any fluoroquinolone, and they were unlikely to have played a direct role in the mammary hyperplasia of these rabbits. However, other fluoroquinolones have been reported to increase circulating levels of CSA and alter CSA efficacy. Ciprofloxacin and norfloxacin have been shown to inhibit cytochrome p450–mediated microsomal drug metabolism in rats and people,17 and CSA-dependent inhibition of interleukin 2 and interferon gamma expression is counteracted by ciprofloxacin,22 whereas levofloxacin does not appear to interact with CSA.13 Specific studies with ofloxacin and enrofloxacin were not evident in the literature.
Although gingival hyperplasia has been reported as a common complication to CSA administration in humans, none of these rabbits developed oral lesions. In humans, up to 35% of renal transplant patients develop gingival hyperplasia, which resolves after cessation of CSA therapy.11 There are also multiple reports of gingival hyperplasia associated with CSA administration in dogs.1, 19, 24 Although a specific mechanism has not been determined for CSA-induced gingival hyperplasia, it is likely a result of individualized drug effects on gingival fibroblasts.8, 11 Because CSA-associated gingival hyperplasia and mammary hyperplasia have a significant stromal component, a similar fibroblast-related mechanism might be present. If this were the case, an association between mammary hyperplasia and gingival hyperplasia would be present. However, an association has not been found, and a generalized or multifocal fibroblast effect is unlikely.2 Selective influence on fibroblasts surrounding mammary glands, possibly due to specific receptors, cannot be excluded.
Mammary hyperplasia has also been reported in rabbits with prolactin-secreting pituitary adenomas.16 However, mammary neoplasms in rabbits are uncommon, and case reports are scarce. In both conditions, the changes are not reversible, and the mammary gland enlargement does not regress with withdrawal of medications. Cyclosporine-induced mammary hyperplasia is a reversible change that should be considered as a primary differential diagnosis when evaluating mammary masses in male or female rabbits exposed to CSA levels as low as 5 mg/kg/day.
Footnotes
Acknowledgements
Funding for this project was provided by the Children's Glaucoma Foundation and University of Georgia Veterinary Ophthalmology Fund. We thank Lynn Reece for technical assistance and the staff of University Research Animal Resources for their dedicated care of the laboratory animals.