
Abstract
An 11-year-old female American Cocker Spaniel was presented with a rectal mass that protruded through the anus. Cytologically, the mass was composed of neoplastic round cells consistent with an extramedullary plasmacytoma. Histiocytic sarcoma, carcinoid tumor, and melanoma were also considered because of the presence of golden-brown cytoplasmic granules. Histopathologic findings and immunohistochemical reactivity for lambda light chains confirmed the cytologic diagnosis of plasmacytoma. Prussian blue staining identified the cytoplasmic granules as hemosiderin. The granules were negative by Fontana Masson and Grimelius histochemistry. To our knowledge, this is the first report of an extramedullary plasmacytoma containing hemosiderin in a dog.
Extramedullary plasmacytoma is a relatively common tumor in older dogs, and, in a recent compilation of cases, accounted for 2.4% of all canine tumors.9 The American Cocker Spaniel, English Cocker Spaniel, and West Highland White Terrier are at a higher risk of developing this tumor.13 Plasmacytoma occurs most frequently on the skin and mucous membranes but has been reported in other areas such as the brain stem, spinal cord, lymph nodes, and abdominal viscera.7, 13 Canine rectal and colonic plasmacytomas have been reported to represent only 4% of all extramedullary plasmacytomas.1, 9, 12 We report a case of rectal plasmacytoma in a dog, diagnosed cytologically, and confirmed by histopathology as well as immunohistochemistry. In addition to the usual characteristics of plasma cell tumors, some neoplastic cells had Prussian blue–positive cytoplasmic granules, consistent with hemosiderin, a unique cytologic feature not previously described in canine plasmacytomas.
Case History
An 11-year-old spayed female American Cocker Spaniel was presented to the Oncology Service of the Centre Hospitalier Universitaire Vétérinaire (CHUV) de l'Université de Montréal for evaluation of a mass located in the rectal wall and protruding through the anus. The mass had been noticed approximately 2 months before presentation. Upon examination, the mass was 2 cm in diameter, firm, pedunculated, and reddish, but non-ulcerated. According to the owner, the mass did not appear to have grown since it was first observed, and it did not bother the animal. Physical examination was otherwise unremarkable. Results of a complete blood count, serum biochemistry panel, and urinalysis were within reference intervals, and abdominal ultrasound revealed no abnormalities except for the presence of the rectal mass. Colonoscopy was recommended to detect any other masses in the rectum or colon, but this option was declined by the owner.
Results
Cytologic findings
Cytologic preparations, obtained by fine-needle aspiration of the rectal mass and stained with a 2-part Romanowski stain (Wescor Inc., Logan, UT), were densely cellular with only mild blood contamination (Fig. 1). The cell population was composed of individualized round to oval cells, measuring 15 to 30 μm in diameter, with moderate to large amount of finely granular and pale basophilic cytoplasm, and a single, round to oval, eccentric nucleus with clumped to reticular chromatin. Few cells had eosinophilic cytoplasm, typical of flame cells. Several binucleated cells were also observed. Some neoplastic cells contained a moderate number of golden-brown cytoplasmic granules. No mitotic figures were seen, but moderate anisocytosis and anisokaryosis were present. Based on cytologic evaluation, a diagnosis of a round cell tumor, most consistent with an extramedullary plasmacytoma, was established. A melanoma was included in the differential diagnosis due to the presence of brown cytoplasmic granules. A diagnosis of carcinoid was also considered, but thought to be less likely due to the lack of cytologic features of epithelial cells. Because of the round cell characteristics of the neoplastic cells, histiocytic sarcoma was also included in the differential diagnosis.
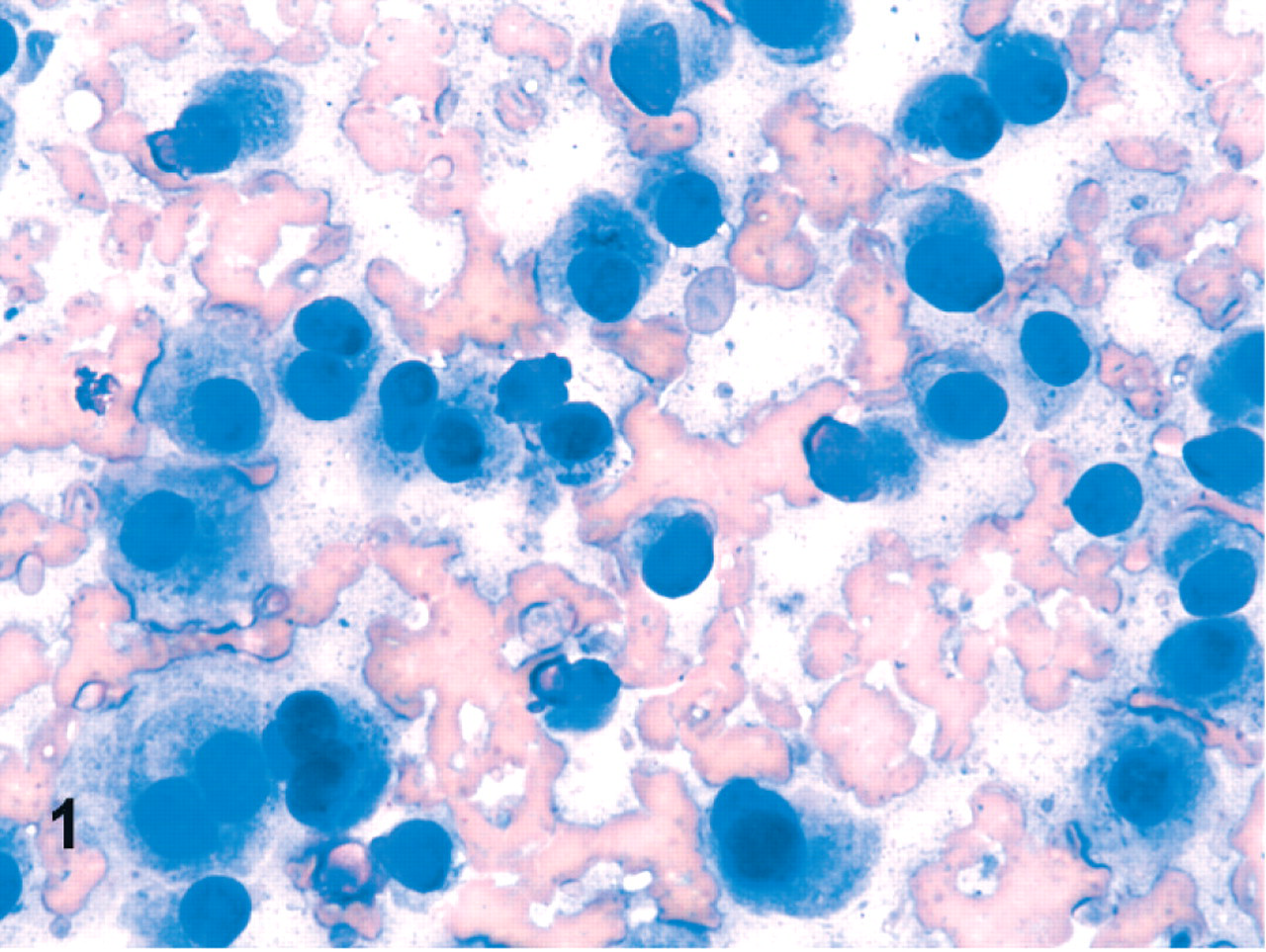
Rectal mass aspirate; dog. The neoplastic cells have plasmacytoid cytologic features. Some contain a moderate amount of brown cytoplasmic granules. Wright's-Giemsa.
Because the prognosis and treatment of colorectal plasmacytomas, melanomas, and carcinoids are different, definitive diagnosis is essential for clinical management. Colorectal plasmacytomas are considered slow growing, benign tumors with no recurrence after complete excision, whereas visceral carcinoids and melanomas are considered to be highly aggressive tumors with frequent metastasis by the time of diagnosis. To determine the origin of the neoplastic cells and the nature of the cytoplasmic granules, 3 special stains were performed on the cytologic preparations. The neoplastic cells were negative for argentaffin granules using the Fontana-Masson reaction, but the granules were argyrophilic with the Grimelius stain (Fig. 2). The granules were also strongly positive for iron with a Prussian blue stain (Fig. 3). The lack of argentaffin granules with Fontana-Masson reaction enabled us to rule out a melanoma. The positive results with the Grimelius and Prussian blue stains were both surprising and conflicting as they suggested a round cell tumor with intracytoplasmic iron granules or a carcinoid with neuroendocrine granules. Typically, Prussian blue stain reacts with ferric iron but not with argyrophilic granules, whereas Grimelius staining is positive for argyrophilic granules but negative for iron.
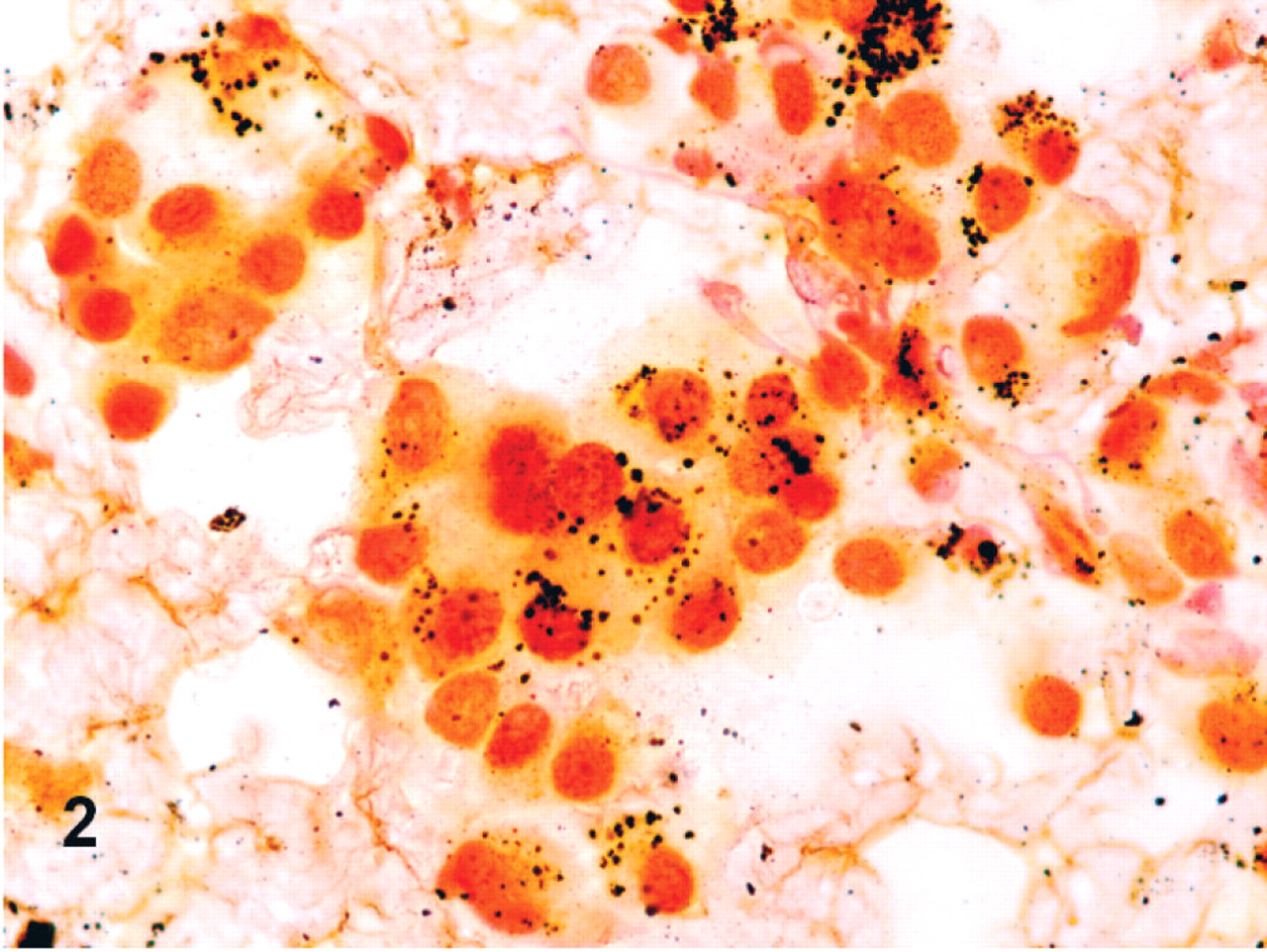
Rectal mass aspirate; dog. The cytoplasmic granules of neoplastic cells are mildly positive, consistent with argyrophilic granules. Grimelius' stain.
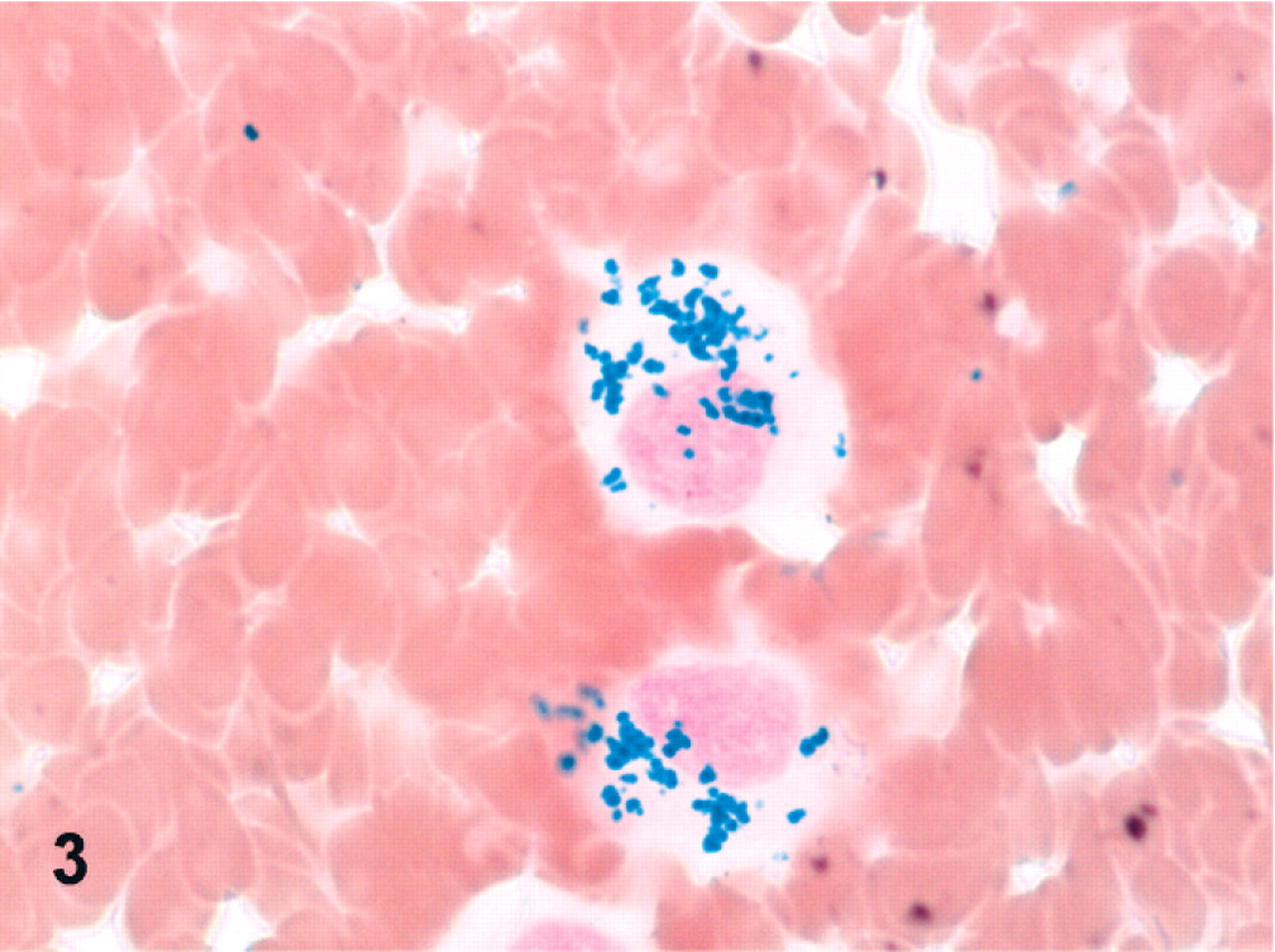
Rectal mass aspirate; dog. The cytoplasmic granules are also strongly positive for ferric iron. Prussian blue.
Histopathologic findings
The mass was surgically excised, fixed in 10% buffered neutral formalin, and stained with hematoxylin-phloxin-saffron (HPS) and methyl green-pyronin. Histologically, the mass was a well-demarcated, nonencapsulated, and densely cellular neoplasm located mainly in the submucosa, but extending multifocally into the rectal mucosa (Fig. 4). Multifocal hemorrhages were present throughout the mass. Neoplastic cells were pleomorphic (round to oval) and arranged in packets and small nests, separated by a delicate fibrovascular stroma. Neoplastic cells had ample to abundant amphophilic and pyroninophilic cytoplasm with variably distinct cytoplasmic margins, and occasionally prominent paranuclear pallor. In a few cells, the cytoplasm was distended by pale acidophilic globules. The nucleus was round, eccentric, and hyperchromatic; anisocytosis and anisokaryosis were moderate. There was 0–1 mitotic figure/high power field. Scattered cells had 2 or 3 nuclei. Numerous Prussian blue–positive granules (hemosiderin) were present in macrophages as well as in scattered neoplastic cells (Fig. 5). The Grimelius stain was negative. Immunohistochemistry for kappa/lambda light chains was performed with strongly positive reaction for lambda light chains, consistent with a plasmacytoma (Fig. 6). The histologic diagnosis was rectal plasmacytoma with chronic hemorrhage.
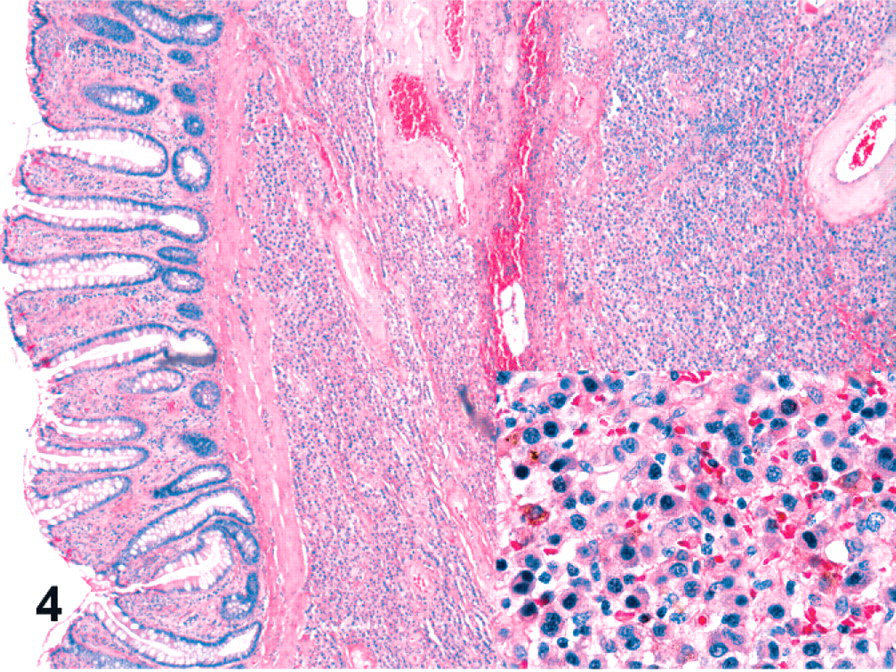
Rectal mass; dog. The tumor is composed of sheets of pleomorphic neoplastic round cells. Inset: Several neoplastic cells contain golden-brown granules. Numerous hemosiderophages are present through the section. HPS.
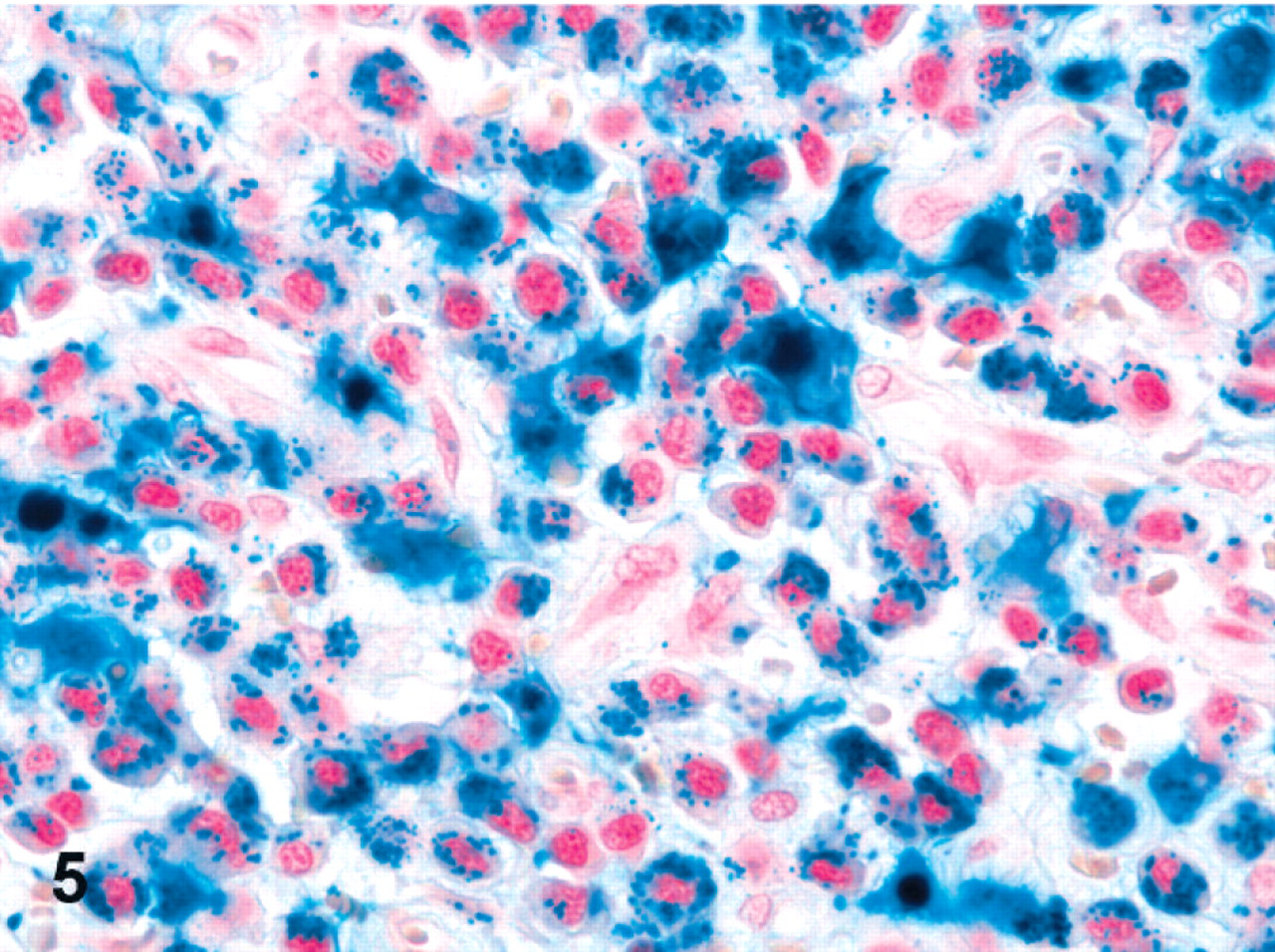
Rectal mass; dog. The neoplastic cells are strongly positive for Prussian blue stain. Hemosiderophages are also present. Prussian blue.
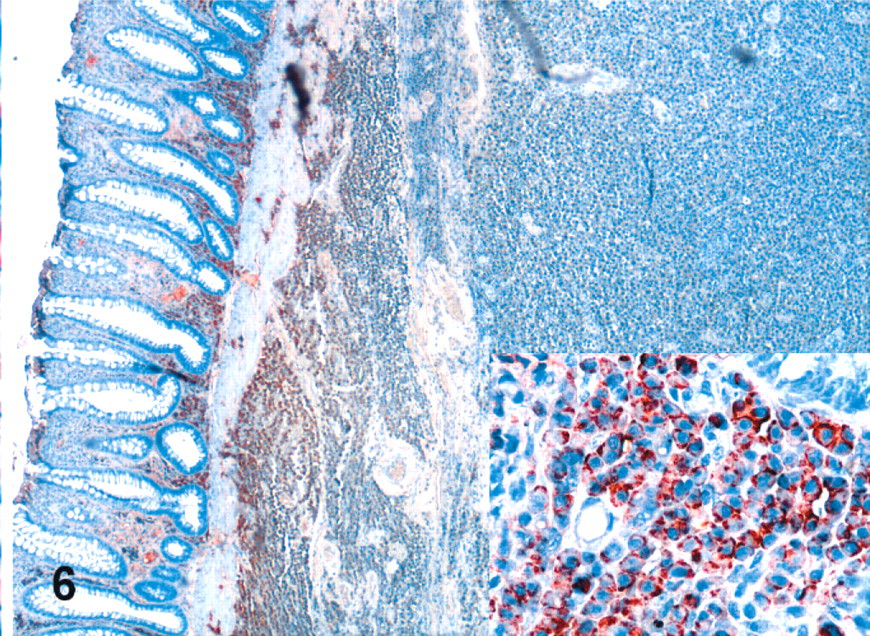
Rectal mass; dog. Neoplastic cells are immunohistochemically positive for lambda light chains. Inset: Higher magnification of neoplastic cells.
Discussion
The cytologic and histologic appearances of this rectal mass were compatible with an extramedullary plasmacytoma. However, the presence of iron-containing granules within the cytoplasm of the neoplastic cells was atypical. To the authors' knowledge, no case of plasmacytoma with cytoplasmic hemosiderin granules has been reported in veterinary species. Extramedullary plasmacytomas commonly occur at cutaneous sites (86%), mostly on the skin of the limbs, head, and at mucocutaneous areas including the mouth and lips (9%), as well as the rectum and colon (4%). All others sites account for only 1% of cases. Grossly, extramedullary plasmacytomas appear as solitary, red, raised and smooth nodules that grow rapidly. Multiple colonic plasmacytomas were reported in 1 dog.9 Cutaneous and oral plasmacytomas usually have a benign course with no related clinical signs.13 Complete excision is usually curative. In contrast, dogs with colorectal plasmacytomas often present with hematochezia, tenesmus, and rectal prolapse. However, the prognosis for colorectal plasmacytoma is generally good with complete excision. Of 9 dogs with colorectal plasmacytomas, 2 had local recurrence at 5 and 8 months after incomplete resection, and only 1 dog was euthanatized because of clinical signs related to bleeding from the tumor.9 That dog had multiple colonic masses that had not been completely removed. In that study, the overall median survival time was 15 months (range, 5 to 33 months). Two dogs were alive at the end of the study with no recurrences at 20 and 33 months.
The presence of iron granules in marrow plasma cells has been reported in human patients.3, 4 However, it is an unusual finding and mainly reported in alcoholics. These patients are presented with no primary plasma cell abnormalities, but have evidence of abnormal iron metabolism, notably ring and non-ring sideroblast formation. They also frequently present with megaloblastic anemia secondary to folic acid deficiency. All these features suggested that the common factor in these patients was ineffective iron utilization and mobilization. This is a relatively frequent finding in alcoholics, as they usually suffer from folic acid deficiency and secondary sideroblastic anemia, along with increased iron absorption. Ultrastructural studies revealed that the iron granules were present within the mitochondria of the plasma cells. Based on these observations, Cook and colleagues proposed that excessive iron accumulation takes place in the mitochondria of marrow plasma cells in alcoholic patients.3 The mechanism is similar to that observed in ring sideroblast formation in alcohol-induced sideroblastic disease. Alcoholic patients usually have reduced plasma levels and accelerated hydrolysis of pyridoxal-5-phosphate. Ferrochelatase activity is also reduced by alcohol. These 2 enzymes normally catalyze 2 reactions in mitochondrial heme synthesis. Inadequate heme formation leads to increased iron entry. Thus, in sideroblasts, as iron fails to be incorporated into heme, it accumulates within the cytoplasm as hemosiderin. Likewise, because mitochondria contain heme mostly in cytochromes, it was postulated that the same mechanism could take place in all cells that contain mitochondria, including plasma cells.
The cause of iron accumulation in the neoplastic plasma cells of the dog in this case is unknown. One hypothesis is that a mutation occurred in one of the heme-containing enzymes involved in the respiratory chain leading to the accumulation of iron by the mechanism proposed by Cook and colleagues. The presence of chronic bleeding within the mass could predispose to iron uptake by creating an iron-rich environment around the neoplastic plasma cells. The other possibility is that the neoplastic plasma cells acquired the possibility to phagocytize erythrocytes. However, only hemosiderin granules were observed, without cytologic or histopathologic evidence of erythrophagocytosis. Phagocytosis by neoplastic plasma cells is a rare but well-recognized feature that has been described in several articles in the medical literature.5, 6, 8, 14 This phenomenon has also been described in 2 dogs, 1 with a nonsecretory multiple myeloma10 and the other, with an extramedullary plasmacytoma.15 The plasmacytoma in the latter case was in skin of the forelimb and was composed of round neoplastic cells that demonstrated phagocytosis of both erythrocytes and neutrophils. However, no cytoplasmic accumulation of hemosiderin was reported.
Transmission electron microscopy can help differentiate among melanin granules, hemosiderin, and neuroendocrine granules. Melanosomes appear as ellipsoid bodies, about 5 nm in diameter, with intralumenal fine fibrils, giving a striated appearance, whereas hemosiderin appears as variably sized electron-dense aggregates localized within siderosomes.2 However, it can be very difficult to differentiate highly electron-dense siderosomes from mature melanosomes (stage IV melanosomes), which also are electron dense. Endocrine granules in carcinoid tumors are round to rod-shaped with variable size, electron density, and texture.11 Electron microscopy was not performed in this case.
It is unclear why the granules were mildly positive with Grimelius stain in cytologic specimens. One possible explanation for this discrepancy is that the Grimelius stain protocol was adapted from a histopathologic technique, and the positive control was a histologic specimen of a carcinoid. This highlights the difficulty in interpreting cytologic samples when protocols and controls are not adapted for cytology as well as the need to use specific cytologic protocols.
The cytologic and histopathologic diagnosis of extramedullary plasmacytoma is usually straightforward even though neoplastic plasma cells may have variable cytologic features and degrees of differentiation. Occasionally, immunohistochemical detection of immunoglobulin or light chains may be necessary for a definitive diagnosis.13 In this dog, the cytologic features of the neoplastic cells, the presence of flame cells, and the lambda-positive immunohistochemistry confirmed the cytologic diagnosis of extramedullary plasmacytoma. The brown cytoplasmic granules were identified as iron-containing granules by positive Prussian blue staining.
Footnotes
Acknowledgements
We thank Dr. Manon Girard for submission of this case and for providing clinical information, and Drs. Carolyn Gara-Boivin and Charlotte Thorneloe for their useful comments on the manuscript.