
Abstract
Abstract
Malignant bone tumours of the lower limb represent the majority of cases in both osteosarcoma and Ewing sarcoma in the growth period. Surgical treatment represents a key element of treatment. Different localizations and age groups require a differentiated surgical approach. Life and limb salvage are first on the list of treatment goals, followed by functional and cosmetic considerations. This review article delivers and discusses current surgical treatment strategies and outcomes for lower limb malignant bone tumours in children.
Introduction
Osteosarcoma and Ewing sarcoma are the two most common malignant bone tumours in childhood and adolescence that require surgical orthopaedic management as a part of the internationally accepted and guided treatment protocols. Their localization in the lower limb varies between the two and is shown in Figure 1.
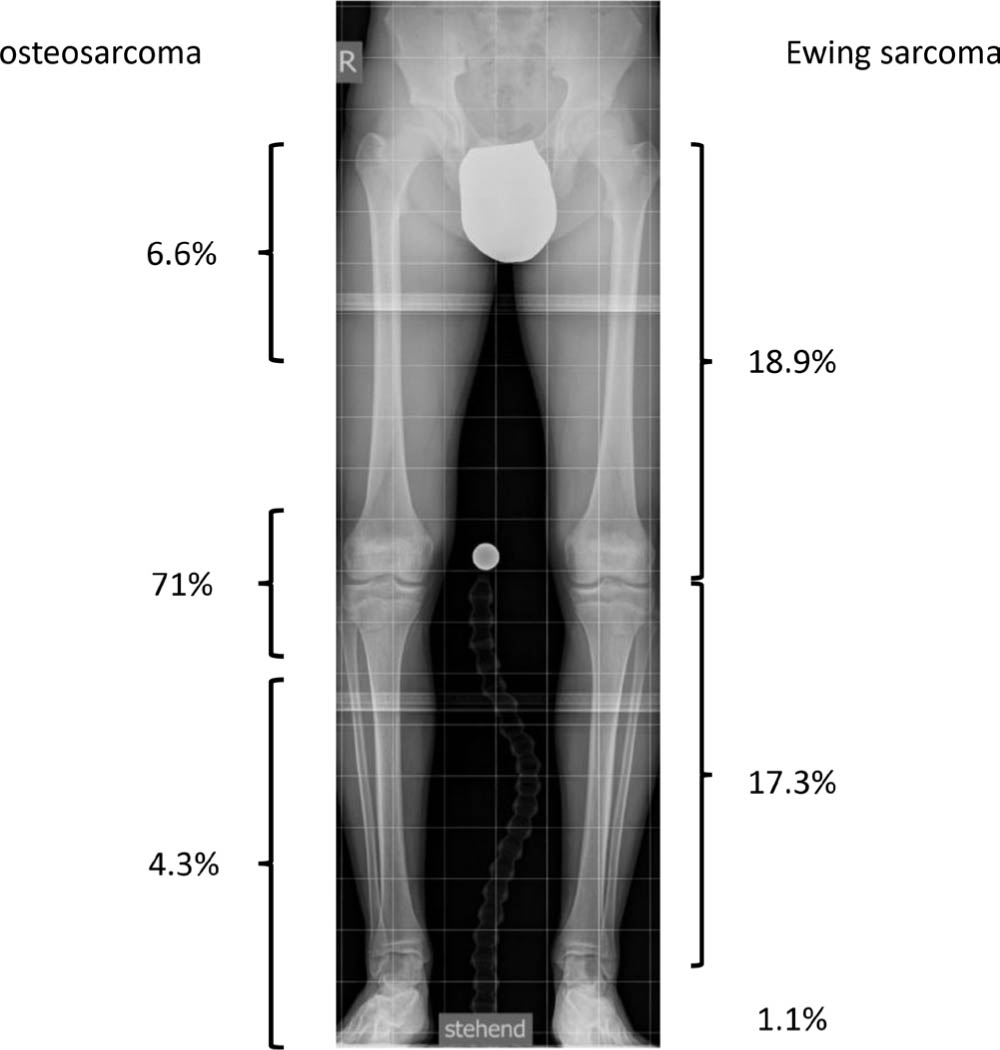
In a continuous series of 528 young patients aged below 15 years (339 osteosarcoma (OS) and 119 Ewing family tumours (EFT), treated in a 20-year period (1997 to 2016) at Istituto Ortopedico Rizzoli, 250 cases (47%) arose in the distal half of the femur and 119 (23%) in the proximal half of the tibia. Proximal femur and hip are the second most frequent and distal tibia and foot uncommon locations of bone sarcomas in children.
Local tumour management comes second after neo-adjuvant and prior to adjuvant polychemotherapy. It consists of surgical intervention by wide resection in both sarcoma variants with radiotherapy being discussed in some cases of Ewing sarcoma. Defect reconstruction can be accomplished by using ablative procedures, tumour endoprostheses and various techniques of biological reconstructions. This comprehensive review discusses the most widely used options with great emphasis to the region the malignancy is localized at.
Tumour resection
The basic principles of surgical resection of all bone sarcomas do not differ: the cornerstone of local treatment is wide surgical resection. Accurate surgical planning is strongly advised, and in all the available imaging studies it may be useful to include a high-definition MRI of the whole affected bone to define the surgical margins both in the bone and surrounding soft tissue.
Depending on the anatomical region, specific particularities have to be respected such as tumour dimensions, specific anatomical considerations and soft-tissue involvement, which always leads to an individualized surgical intervention, i.e. in the distal lower limb and in the foot there is frequently lack of soft-tissue coverage. With regards to the foot, Yang et al 3 stated, that “these tumours are less amenable to limb sparing surgery because of poor tumour compartmentalization in the foot and difficulty in achieving adequate resection margins”. In case of articular involvement an extra articular resection is performed without opening the joint involved.
Despite the advent of limb-salvage surgery, in very large high-grade sarcomas involving more than two anatomical compartments and main neurovascular structures, and if there is a doubtful effect of preoperative chemotherapy, amputations may still represent the best surgical choice in about 5% to 10% of children.
Ablative surgery
For the vast majority of families and children, the indication for an amputation is a big trauma and means failure of treatment. Nevertheless, the fast adaptation of a child to an external prosthesis is amazing and the patients may reach nice functional results in a few months, particularly in distal amputations with a good stump. In order to better accept the aesthetic impairment of any form of ablative therapy, children and family should be involved early in meetings with previously treated patients and families. 4
Amputation
Tumours of the distal half of the femur and confined to the lower third of the diaphysis, as well as proximal tibia sarcomas, may be candidates for amputation. Depending on the localization and relation to the knee joint, a transfemoral amputation with an acceptable bone margin and a good soft-tissue coverage of the femur stump can be done. A knee disarticulation with the patella fixed to the trans-metaphyseal distal femur osteotomy could allow whole quadriceps preservation and a robust stump. 5
If the tumour involves the upper third of the diaphysis, hip disarticulation should be considered.
Amputation has a higher priority in malignant tumours of the distal tibia and foot. Functional limb sparing surgeries with wide resections and clear margins are often impossible or need additional flaps to achieve wound closure which may affect the function of the foot and compromise the outcome significantly. Further, there is a higher risk of local recurrence if the surgical strategy accepts smaller margins to avoid unnecessary soft-tissue loss (Fig. 2). On the other side the functional outcome after partial or complete foot or below knee amputation is reported to be so favourable that many patients prefer this option.
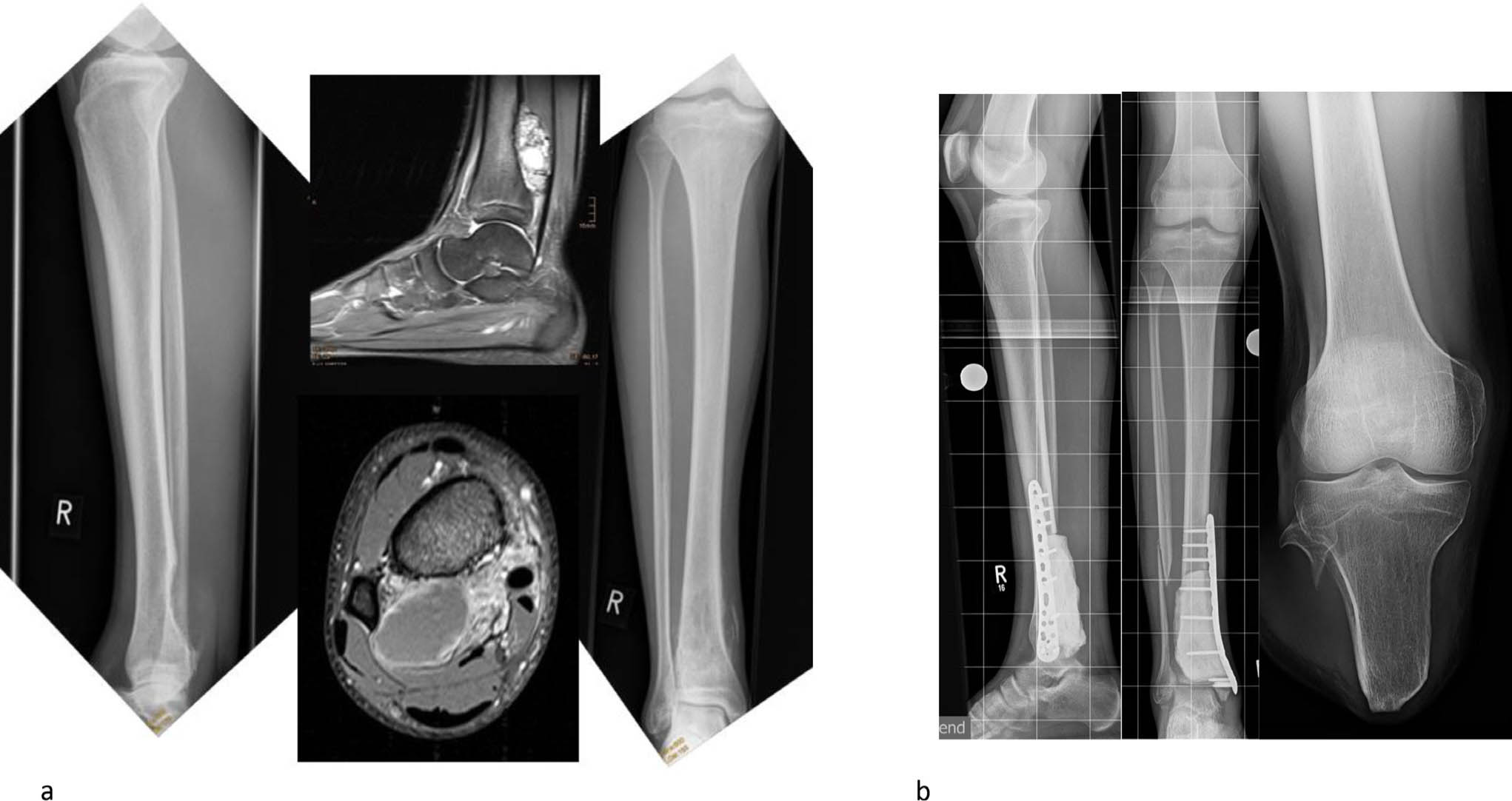
Parosteal osteosarcoma of the distal tibia (a). Resection within narrow limits, limb sparing surgery and attempt of biological reconstruction using intermediate bone cement spacer. Only R1-resection achieved; subsequent below-knee amputation agreed with the patient and family (b).
Depending on the localization and extent of the tumour and contamination of compartments below knee amputations, ray amputation, forefoot, midfoot or hindfoot level amputations are possible options (Fig. 3). The time delay of diagnosis of malignant bone tumours of the foot is greater than in other areas, 3 which further explains the higher amputation rate of malignant bone tumours of the foot.

Recurrence of Ewing sarcoma of the left first metatarsal (a). Midfoot amputation through the Chopart joint – four years follow-up with very good functional result (b).
In all patients noneligible for limb salvage for a knee bone sarcoma, the surgeon should evaluate the sciatic nerve relationship with the tumour and neurovascular condition of the ankle and foot. Whenever the sciatic nerve can be preserved, a rotationplasty might offer the patient a clear functional advantage over an amputation or a hip disarticulation.
Rotationplasty
This technique uses en bloc excision of the original tumour site, i.e. the knee or hip joint, with the vascular structures spared or removed and reconstructed in a termino-terminal fashion while the sciatic nerve must be preserved and looped. The leg is rotated 180° and the bony stump is fused to the adjacent bony structure according to the type of rotationplasty. The reversed knee joint acts as the hip, the reversed ankle as the knee with the foot fitting into a below-knee prosthesis.
This technique was popularized for the treatment of children with sarcomas around the knee in the 1980s, and Winkelmann 6 described an A1 type for distal femur sarcomas and an A2 variant for proximal tibia neoplasms. 7 Type IIB rotationplasty could avoid a proximal disarticulation in very small children in either intra- or transarticular proximal femur resection for bone sarcomas or in cases with very severe soft-tissue involvement and unaffected sciatic nerve.
In Rizzoli, A1 rotationplasty has been performed in 50 children (mean age eight years (3 to 15)) since 1986, with no case of an A2 type. 8
There are well-demonstrated functional advantages of A1 rotationplasty over an above-knee amputation: thanks to the new ‘knee joint’ the young patients may reach very high functional levels, similar to patients with below-knee amputations and superior to long-term functional results of distal femur megaprostheses. 9
Therefore, A1 and B2 rotationplasty remain our first choice in a selected group of very young patients, where the resected femur is too short and small for accepting any prosthetic implant.
The biggest controversy for this procedure remains the cosmetic appearance with all the psychologically related issues that have to be addressed in advance by the multidisciplinary team (surgeon, paediatric oncologist, psychologist and physiotherapist).
Reconstructive surgery
Reconstructive procedures have changed significantly in the last 40 years and some options such as arthrodesis, very popular in the 1980s or 1990s, have been abandoned in favour of some new procedures.
Modular prostheses
Several modular endoprosthetic reconstructions are available for patients who undergo distal femur and proximal tibial resections. Functional outcome and implant survival have gradually improved through the years and nowadays most patients obtain good to excellent function with implant survival that exceeds 80% at ten years. In growing patients of course, the surgeon must evaluate the rate of residual growth length expected in the contralateral knee, both in the distal femur and in the proximal tibia, in order to foresee the lower-limb discrepancy at skeletal maturity.
If the expected inequality related to distal femoral or proximal tibial physis loss stays below 3 cm to 4 cm, a modular distal femur megaprosthesis may be used with a custom femoral or tibial component and a polished uncemented stem to allow further growth. In proximal tibial sarcomas this philosophy bears limitations. The preservation of the distal femoral physis is more unreliable, the complication rate is higher and there is regular need for good soft-tissue coverage and the use of a pedicled gastrocnemius flap.
Modular tumour endoprostheses or megaendoprostheses have become the benchmark of reconstructive limb salvage surgery in the knee area in teenagers, adolescents and young adults. In the proximal femur and distal tibia their use is subject to much more specified indications.
In the proximal femur, hemiarthroplasty with a bipolar femoral head to preserve acetabular bone stock and to improve stability 10 is superior to total hip replacement in the younger still growing patient. Here, the reattachment of the greater trochanter, if preserved, or the hip abductors and other saved muscles, can be crucial for optimal functional results. They can be fixed to the coated hydroxyapatite surface of the prosthesis or a Trevira tube surrounding the implant. Postoperatively a hip spica cast or orthosis supports healing of the abductor mechanism and decreases the risk of immediate dislocation.
Growth arrest of the acetabulum and secondary acetabular dysplasia or even dislocation is a regular complication after endoprosthetic replacement (Fig. 4). 11
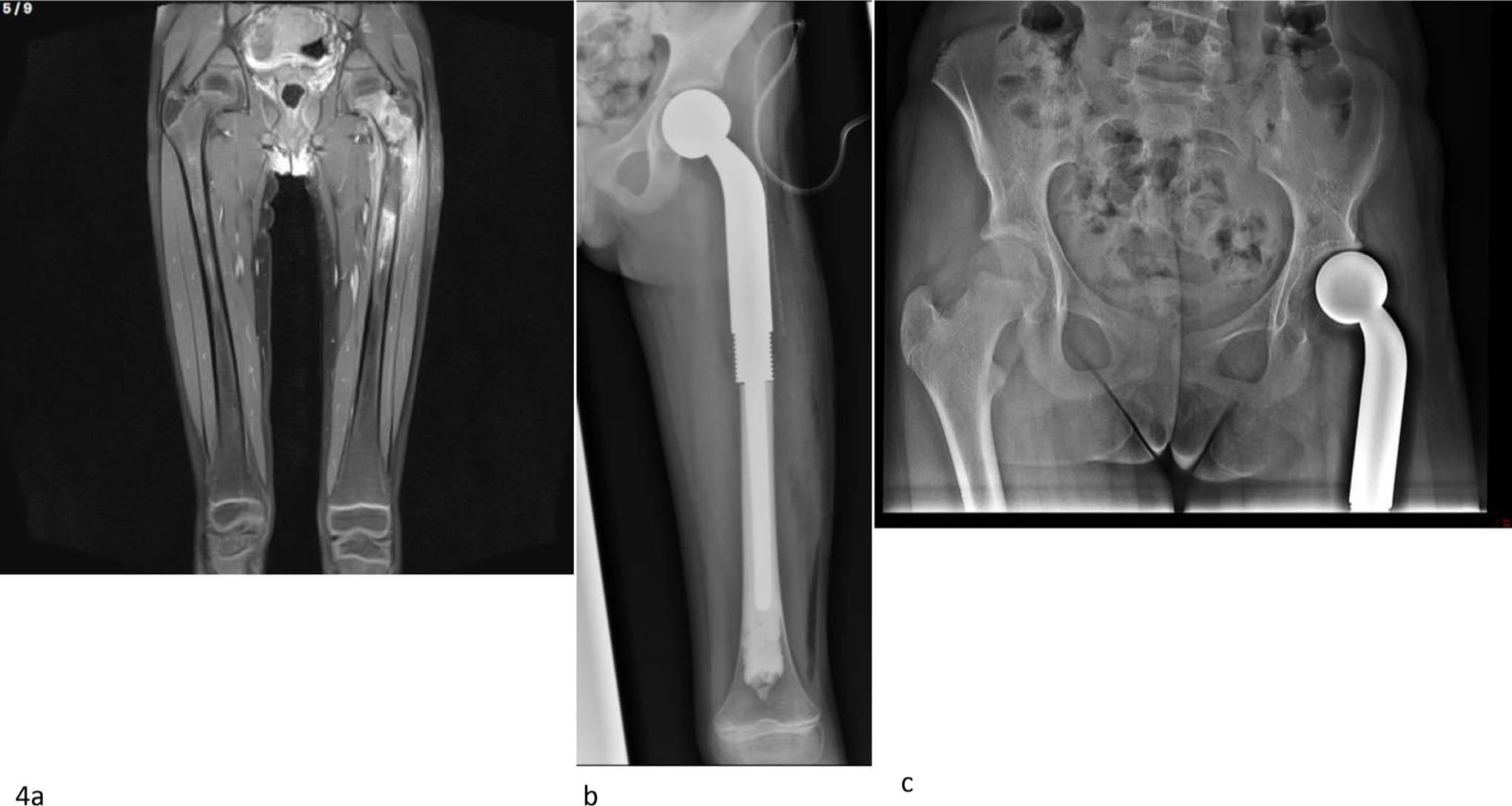
Proximal left femur Ewing's sarcoma in a girl aged eight years. Preoperative MRI (a). Postoperative radiograph (b). Final radiograph in 2020 six years after surgery showing a progressive dislocation of the femoral head and a secondary acetabular dysplasia (c).
Bone defect reconstruction following wide en bloc resection of the distal tibia can be done by implantation of a tumour endoprosthesis (Fig. 5). This allows some ankle movement and also may preserve the subtalar joint function. The major difficulty remains the coverage of the large prosthesis by soft tissue, still permitting wound closure. In cases with ankle joint involvement extraarticular distal tibia/ankle resection and implantation of the tumour prosthesis is possible (Fig. 5). The complication rate of such megaprostheses is quite high with tibial and talar component loosening and deep infections being the most relevant ones. 12 Due to muscular imbalances of the foot as a result of muscle resection secondary tendon transfers or hindfoot realignment procedures may be necessary like in the case pictured in Figure 5a. In our limited series of three cases, one ended in a below knee amputation following deep infection. 12
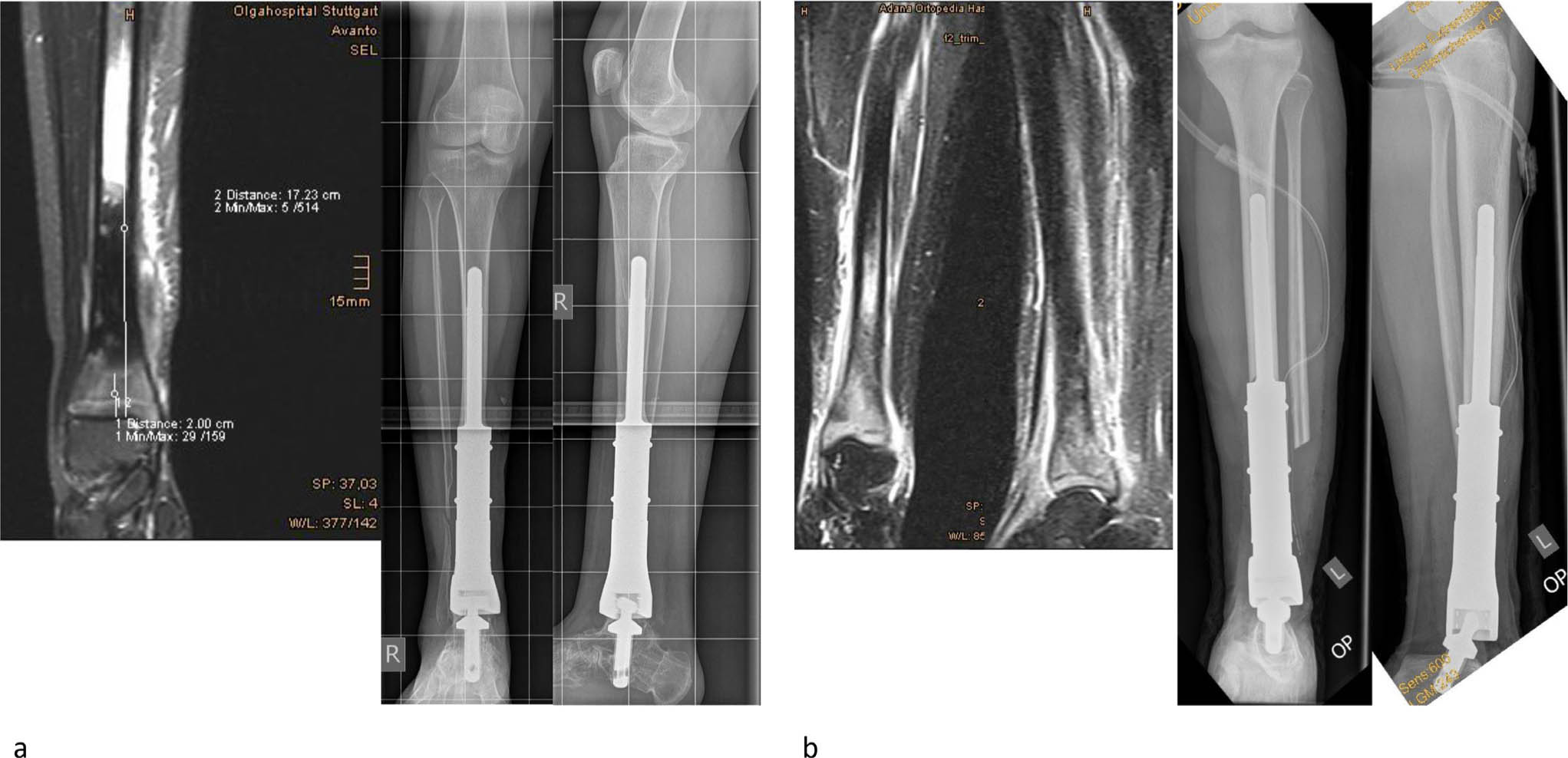
Osteosarcoma of the right distal tibia. The tumour dimension permits distal talar fixation. Wide resection and distal tibia replacement by tumour endoprosthesis, long-term follow-up: ten years (a). Ewing sarcoma left distal tibia. The tumour extent requires ankle resection, calcaneal fixation of the tumour endoprosthesis performed (b).
Expandable prosthesis (EP)
The distal femoral physis accounts for about 40% and the proximal tibial growth plate for about 30% of lower limb length. Their removal in childhood causes a potential significant loss of the affected limb length at skeletal maturity.
A predicted significant leg-length discrepancy prepares the ground for EP.
There is no complete consensus about the minimum age of patients eligible for expandable implant reconstruction. A survey among orthopaedic surgeons of the European Musculoskeletal Oncology Society (EMSOS) recommended a minimum age of 6.5 years and an expected limb-length discrepancy of 3 cm to 4 cm.13,14 At Istituto Rizzoli, we used EP from the age of five years. Two types are available:
magnetic or electro-magnetic type EPs allow non-invasive lengthening procedures by
a rotating magnetic field, that is captured by a magnet within the implant, and transferred to an internal gearbox (Fig. 6), or by; a motorized device, activated by an external electromagnetic field that uses a subcutaneous antenna as transmitter;
biologically lengthening tumour endoprostheses by elongating the original femoral or tibial shaft through callostasis. A lengthening nail fixed to the tumour endoprostheses is being used. This method is recommended in particularly young children and creates new bone stock.
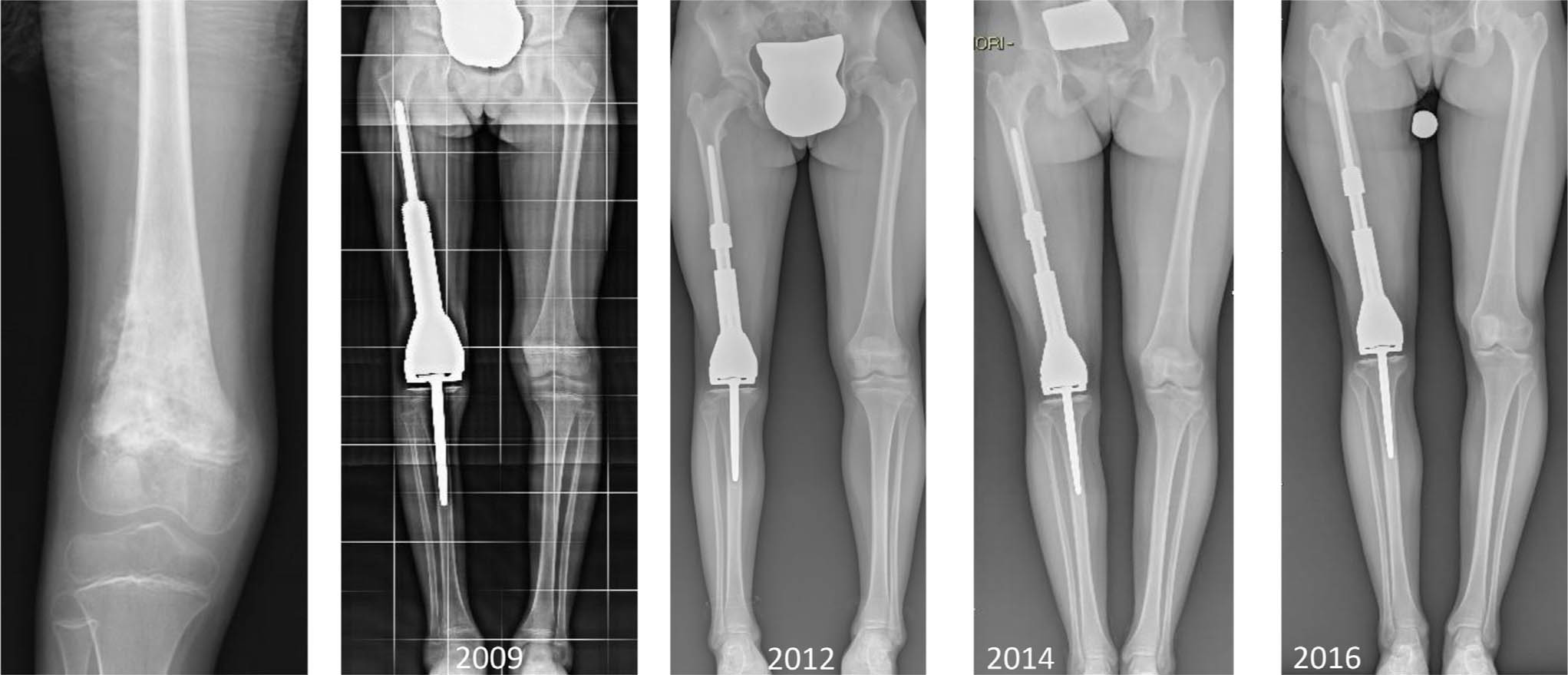
Nine-year-old girl, osteogenic sarcoma, reconstruction by a magnetic EP (April 2009) with potential expansion 50 mm. From 2009, she had nine noninvasive lengthening procedures and no further surgical procedures.
In tumours of the proximal femur non-invasively extendable prostheses are being indicated very rarely for patients with larger predicted leg-length inequalities, and contralateral epiphyseodesis of the longer leg is preferred for differences up to 3 cm. 15 There were reports on very relevant complications during the elongation procedure, such as progressive acetabular dysplasia or even hip dislocations.
Osteoarticular allograft and allo-endoprosthetic composite
The domain of osteoarticular allograft and allo-endoprosthetic composite constructs in bony tumour surgery of the lower limb is the proximal femur. Patients of adequate bone sizes to implant conventional long-stem endoprostheses placed in bony allografts offering sufficient bone stock and soft-tissue coverage of implants of greater thickness and volume are the best indications. This technique allows abductor muscles reinsertion for better function, which makes it our favourite reconstruction technique in older children and adolescents. The diameter of the femoral head should be planned on the MRI and sometimes custom-made. We regard this method superior to using a dedicated tumour megaprosthesis because of better long-term function of the abductor mechanism.16–20
At the knee level osteoarticular allografts and allo-endoprosthetic composites are an alternative surgical option as they preserve the adjacent physis and decrease the impact of final limb-length discrepancy. 16
The indication to carry out a distal femoral hemiarticular reconstruction by the use of an osteoarticular fresh frozen massive bone allograft (MBA) is related to the oncological indication of intraarticular resection that allows the maintenance of the capsular tissue including the menisci. 17 Osteoarticular tibial allografts have been reported in children with proximal tibia sarcomas since the late 1980s. They preserve the distal femur and allow host-graft fixation with load transfer at the osteotomy site.18,19 Enforcing the proximal allograft by an unconstrained femoral or tibial component of a total knee replacement system has been promoted from us since many years (Fig. 7).
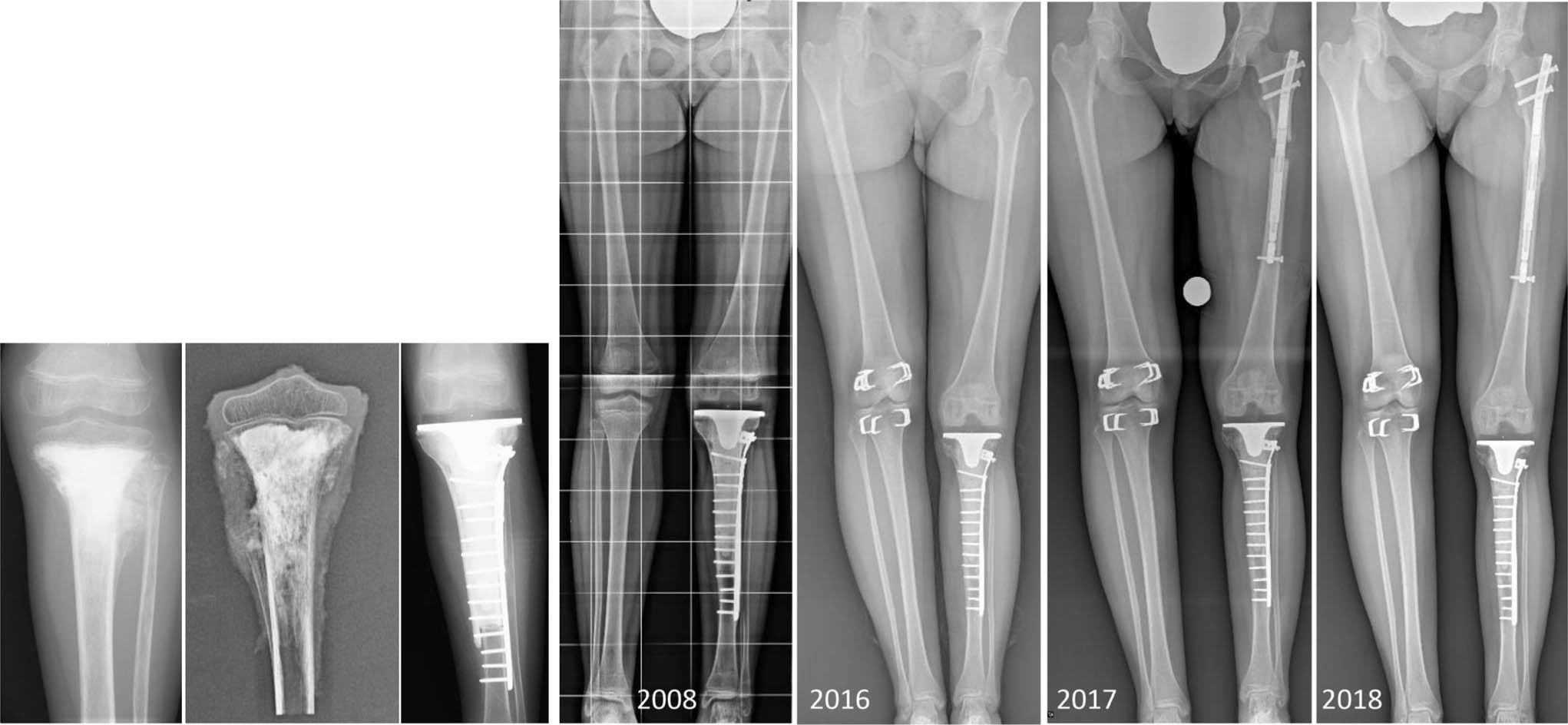
Seven-year-old girl, osteogenic sarcoma, reconstruction by allo-endoprosthetic composite (2006). In 2017 lengthening procedure (5 cm) of the proximal femur by intramedullary magnetic expandable rod.
Again, the main difficulty in the use of osteoarticular allografts in the knee reconstruction of paediatric patients is the small size of the skeletal segment and the limited availability of an acceptable graft size-matching the child's knee. This is almost impossible in children below the age of ten years.
Biological reconstruction
Biological reconstruction of metaphyseally located bone sarcomas
Vascularized epiphyseal transplant
This technique was first described in the proximal femur by Manfrini et al. 20 He tried to reproduce the ‘normal’ anatomy of the proximal femur by reconstructing the femoral neck angle by a combination of allograft for the metaphysis and the epiphyseal transfer for the neck and the femoral head. The very beautiful short-term results could rarely be maintained. Proximal femur reconstruction without femoral neck formation can be successful at allowing the diaphysis to grow in length and the femoral head in diameter. 21 The technique is technically very demanding and the success dependent from the quality of the vascularization of the bony transplants (Fig. 8).

Proximal femur telangiectatic osteosarcoma in a boy aged four years. Reconstruction with a vascularized epiphyseal transfer. Preoperative radiograph (a); MRI (b); postoperative radiograph (c); standing radiograph 13 years after surgery (d).
Arthrodesis
Hip arthrodesis is possible in all patients requiring transarticular and extra-articular resection of the proximal femur. The resected bone could be reconstructed using a composite allograft and vascularized fibula transfer or with non-vascularized tibial strut grafts and fixed with a Cobra plate. Functionally the limb is usually very good with less complications and revisions than after prosthetic replacement. However, this technique is no longer ‘fashionable’ in Western Europe but should be considered as a valuable solution. 22
In the distal tibia, maintaining the ankle joint is almost always impossible and resection arthrodesis the method of choice if biological reconstruction is being selected for treatment. Several methods can be successfully used: 1) en bloc resection, intermediate bone cement spacer, vascularized fibula plus tibial strut graft; 23 2) en bloc resection, non-vascularized fibula plus autologous or allogeneic bone graft without using an intermediate cement spacer; 24 and 3) en bloc resection and bone transport. 25
Biological reconstruction of diaphyseally located bone sarcomas
Intercalary reconstruction
Diaphyseal bone tumours of the femur and tibia are very suitable for intercalary resections, as detailed below. These methods are exemplarily discussed for intercalary reconstruction of the femur. Publications upon recent techniques and case reports are often enthusiastic but late results show a lot of late mechanical complications.
Reconstruction of the femur diaphysis
Allografts alone
Allografts have been and still are a popular and easily applicable technique. With some variability to the fixation used there are complications like late fractures (15% to 45%) and pseudarthroses (15% to 40%), leading up to 70% revisions. Infections would occur in about 15% of cases. The EMSOS multicentric study revealed much better long-term results in children than in adults with more than 90% probability of graft survival in children after 10 years. 26
Vascularized fibula transfer
This technique has been widely used for biological reconstruction in tumour surgery. Despite the remodelling and thickening potential of this bone the big diameter discrepancy between the fibula and the femur promises a high rate of mechanical failure to the transferred bone and the hardware. 27 In addition, there are donor site complications such as transient neurological impairment of the common fibular nerve, claw toes and progressive valgus of the ankle. 28 Healing to the recipient bone is more likely to occur than with non-vascularized grafts or allografts alone. In femur reconstruction we recommend associating the vascularized fibula transfer to an allograft but nonvascularized graft could also be effective in patients with no radiotherapy. 29 The use of biological reconstructive surgical procedures after wide resection of a malignant bone tumour of the foot is restricted to single cases with ideal tumour localization and favourable extent (Fig. 9). Vascularized osteo-cutaneous flaps are recommended to be used for reconstruction.
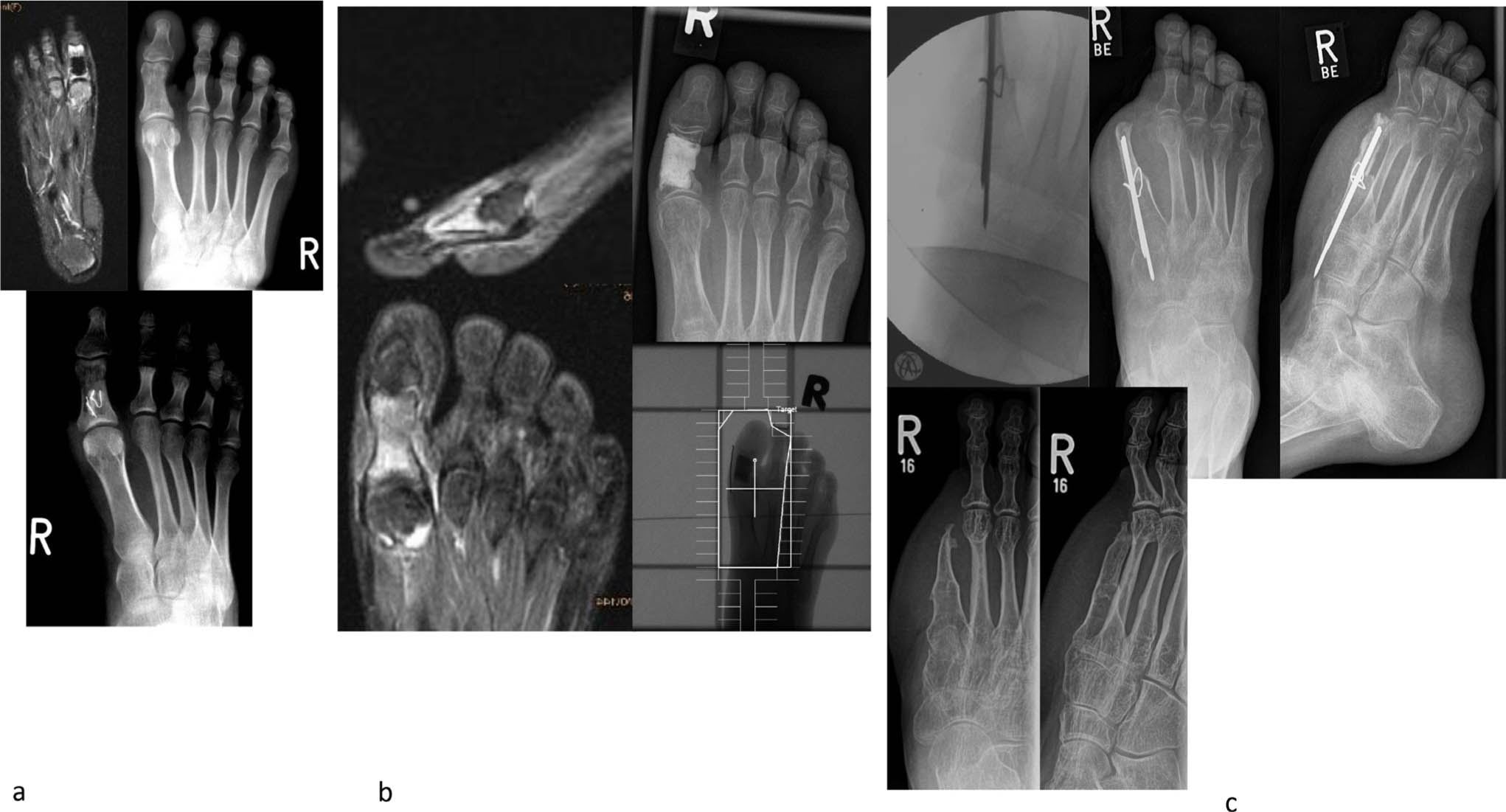
An 18-year-old girl; bony lesion of the great toe, treated as osteomyelitis (a). No healing trend, referral to our department; second biopsy = Ewing sarcoma, local resection and cement spacer; polychemotherapy, local radiation (b). Final treatment by partial first ray resection and reconstruction with vascularized osteo-cutaneous scapula flap (c).
Allografts combined with vascularized autologous fibula (composite allograft)
This technique is supposed to combine the benefits of a ‘real biological’ reconstruction, the vascularized fibula, with the immediate mechanical properties of a massive allograft. 30 The vascularized fibula can be placed inside a femoral allograft or by using the so called ‘hot dog’ technique. Osteosynthesis is performed by a lateral plate bridging the allograft. With time, if properly vascularized, the fibula is supposed to thicken and fuse with the allograft (Fig 10).
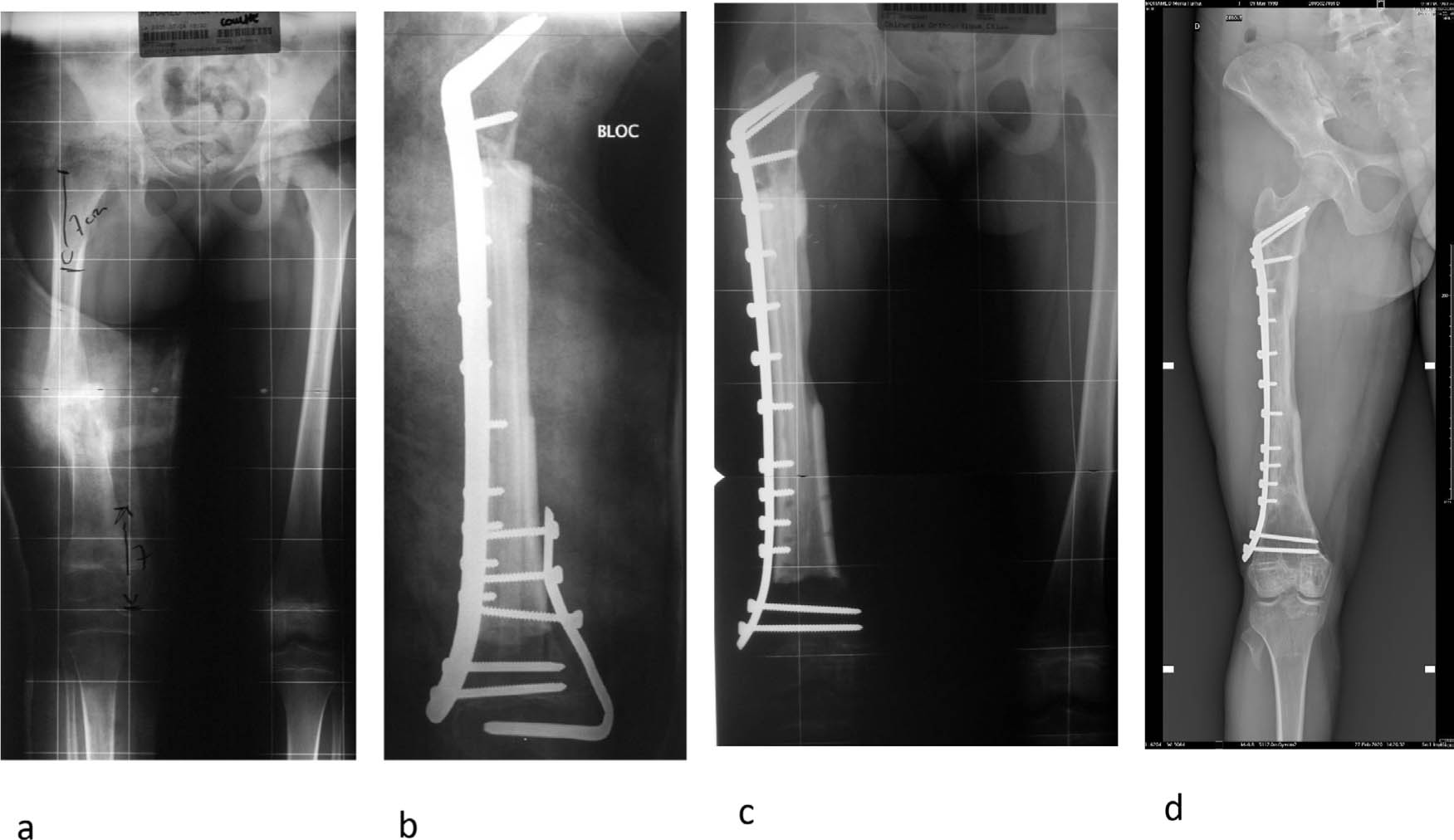
Fractured diaphyseal osteosarcoma in a girl aged seven years. Intercalary reconstruction with an allograft and a vascularized fibula. Preoperative radiograph (a); postoperative radiograph (b); radiograph one-year postoperative and partial hardware removal (c); standing radiograph 15 years after surgery (d).
Although Errani et al 31 and Manfrini et al 32 published that vascularized fibula transfer with allograft did not allow significantly better results than allograft alone Manfrini himself and other authors observed that most complications after allograft with vascularized fibula intercalary reconstructions occurred in the first five postoperative years, indicating that the mechanical properties of the reconstruction will improve with time 33 whereas late fractures in allograft-alone reconstructions can occur.
In a selected group of patients with distal femoral or proximal tibial sarcomas, the metaphyseal location of the tumour in the presence of an intact physis may allow the surgeon to plan an intercalary resection preserving the native distal femur or proximal tibial articular surface by a transepiphyseal distal femur resection. In these cases, the removed specimen includes the growth plate and the residual epiphyseal segment may be very short and thin. 34
The reconstruction in children is usually biological by an intercalary MBA or by the association of MBA with vascularized fibula autograft (VFA). The choice depends on the age of the patient and on the length of the resection (Fig. 11).
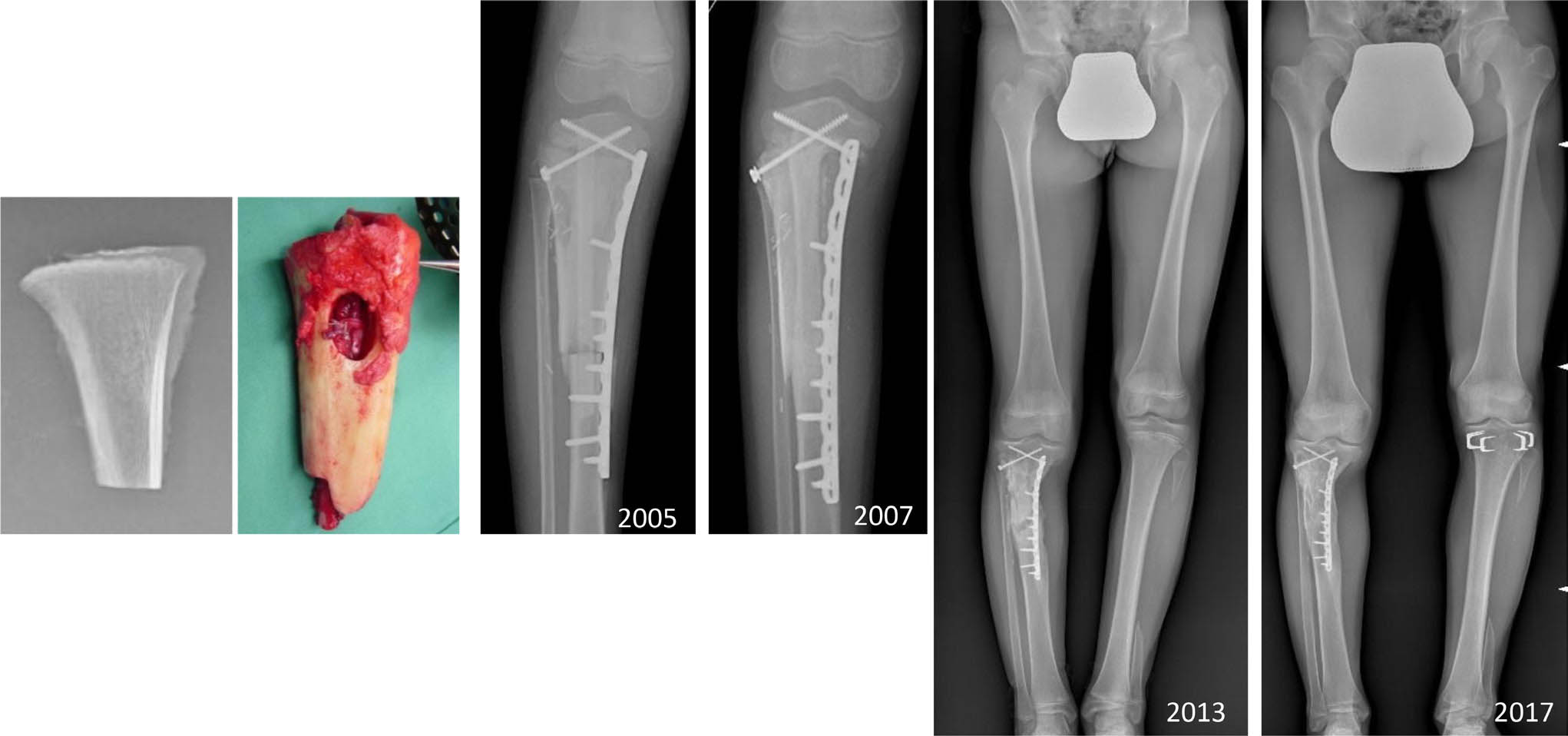
An 11 year-old boy, Ewing family tumour, proximal tibia reconstruction by intercalary intraepiphyseal bone allograft with associate vascularized fibula autograft (2005). In 2013, contralateral proximal tibia epiphysiodesis was performed.
The issue of future limb discrepancy due to the loss of the distal femur physis may be addressed with contralateral distal femur epiphysiodesis or with the plan of lengthening procedures of the femur at the end of growth, nowadays possible by expandable magnetic intramedullary devices.35,36 Due to the intense and everlasting remodelling of the biological implant, increasing the long-term viable bone stock, crucial for the subsequent lengthening procedures, we prefer this method in all diaphysis and also young children.
VFA may be associated with MBA as free flap harvesting the fibula in the contralateral leg or as pedicled flap avoiding the vascular anastomoses. A preoperative evaluation by a CT angiogram of both legs is necessary to indicate which type of VFA to be used.
Sterilized tumour reimplantation
Sterilized tumour reimplantation is an interesting technique when allografts are not available for technical or cultural reasons. Different methods can be used, like irradiation (30 Gy to 80 Gy), pasteurization or cryogenization. Obviously, the graft will perfectly match with the recipient bone, making the reconstruction easy to perform. The disadvantage is to miss the opportunity to assess the margins of resection and response to chemotherapy. The reimplanted tumour will work like an allograft with many late complications. It seems useful to augment it with an autologous bone graft or even with a vascularized fibula. 37 Apparently, there are less pseudarthroses but more late fractures than in allografts. 38
Bone transport
Bone transport was used in the past for secondary diaphyseal reconstruction and correction of limb-length discrepancy after tumour resection. In the past an external fixation was used, but motorized lengthening nails made this technique more simple, reliable and attractive. The size of the resection should be limited to allow a stable fixation of the lengthening device in the remaining bone. 39
Masquelet's induced membrane technique
The induced membrane has been described by Masquelet in traumatic bone loss reconstruction. After tumour resection the technique is a staged procedure. The custom-made bone cement spacer-plate construct will be replaced by autologous and/or autologous bone grafting. The technique is easy, fast and inexpensive and the biological reconstruction is to be postponed after the end of cytotoxic treatments. It has some pitfalls as mandating at least two surgeries. The osteosynthesis should be stable initially to allow healing of the graft but not too rigid, to allow thickening and revascularization. 40 Recent publications showed the effectiveness of using bone substitutes and bone marrow concentrate to enhance the reconstruction.
Prosthetic diaphysis
The reconstruction of the diaphysis with a prosthesis is very easy and will decrease the operating time compared with biological reconstructions. The patients will be allowed immediate rehabilitation and weight bearing. Albergo et al 41 compared the results of allograft and prosthesis in intercalary reconstruction of the femur, showing no statistical differences but a tendency towards more mechanical complications, fractures and loosening after prosthetic reconstructions. Prosthetic reconstruction is possible but more often indicated in patients with a short life expectancy or in adults. In children and adolescents this technique should be reserved for palliative cases or as provisional solution waiting for a biological reconstruction.
New techniques?
Many techniques to improve biological bone reconstruction have been developed for post-traumatic or infectious bone loss; unfortunately many are not allowed in tumour surgery. 42 Tissue engineering is perhaps the future but it remains purely experimental for now. 43
The experts’ choice
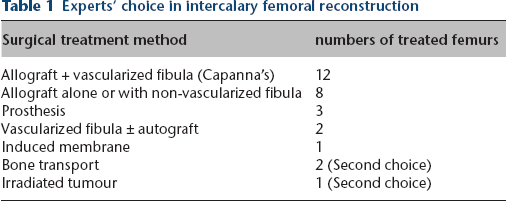
In preparation of the 2017 EMSOS meeting a survey among 28 expert tumour surgeons about their preferred technique in intercalary reconstruction of the femur in children and adult patients was made. Most surgeons prefer biological reconstructions and many used allografts. The most favoured one was the composite allograft technique as described by Capanna (Table 1).
Experts’ choice in intercalary femoral reconstruction
Our experience
In our department, between 1984 and 2015 4 modalities of ‘biological’ intercalary reconstruction were used after resection of a bone tumour of the femur in 62 patients. Length of resection ranged from 24% to 88% (mean 52%) of the total bone and are summarized in Table 2.
Techniques of reconstruction in 62 femoral intercalary resection
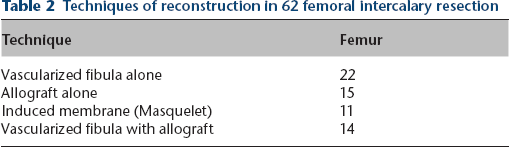
The results were assessed after a mean follow-up of 10.5 years (2 to 30). Primary healing to host-bone was achieved in 35 out 62 cases and after revision in 59/62. Three reconstructions did not heal in non-surviving patients. Allografts healed primarily in only 31% in contrast with induced membrane cases (61%), vascularized fibula alone (62.5%) and vascularized fibula with allograft (71.4%; p = 0.055). Many mechanical complications occurred requiring numerous revisions with the least number of reoperations in vascularized fibula augmented with allograft. 30
Conclusion
What is the best reconstruction after malignant tumour resection of the lower limb? The answer is tough. Tumour dimension, location, age and prognosis of the patient, safety of the procedure, functional demands and individual choices of patient and parents are the main factors to select the most suitable local therapy.
Our indications are summarized below. In children below the age of five years, and with need of sacrificing the joint, rotationplasty is recommended. In children aged five years to 13 years, with need of removal of the joint, EP and allo-endoprosthetic composite constructs are favoured. In children beyond 13 years modular megaprostheses are regarded as the main surgical options.
In all age groups and in particular localizations, intraepiphyseal intercalary reconstructions can be considered.
Diaphyseally localized malignant bone tumours are best treated by wide resection and a variety of biological reconstructions. The composite allograft construct with vascularized fibula augmentation seems to produce the most reliable results.
Large tumours that do not respect compartmental borders, patients who wish it after thorough counselling and patients with local recurrences or complications of endoprostheses are candidates for any suitable form of ablative surgery.
In all distal femur and proximal tibial reconstructions, the expected limb-length discrepancy may be treated during follow-up by contralateral knee epiphysiodeses. In all biological reconstructions a strategy for a final lengthening of the affected bone by intramedullary expandable devices should be offered.
Footnotes
MM: Wrote section on the knee (distal femur and proximal tibia), Performed second round of editing.
TW: Wrote section on the distal tibia and foot, Combined all three parts and finalised the manuscript, Performed second round of editing.