
Abstract
Abstract
Purpose
Several hexapod external fixators are used in the treatment of bone fracture and deformity corrections. One characteristic of all of them is the requirement for manual adjustment of the fixator struts. The purpose of this study was to introduce a novel robotic system that executes automatic adjustment of the struts.
Methods
Ten patients were treated for various bone deformities using a hexapod external fixator with the Auto Strut system. This new system automatically adjusts the fixator struts according to a hexapod computer-assisted correction plan. During each visit, the progress of the correction was assessed (clinically and radiographically) and reading of the strut scale numbers was performed and compared with the original treatment plan.
Results
All patients completed treatment during the follow-up period, achieving all planned correction goals, except from one patient who switched to manual struts due to personal preference. The device alarm system was activated once with no device-related adverse events. Duration of distraction ranged between ten and 90 days with a distraction index ranging between eight and 15 days/cm. Regenerate consolidation time between one and seven months. In total, 48 struts of eight patients were recorded and analyzed. In all, 94% of the final strut number readings presented a discrepancy of 0 mm to 1 mm between planned and actual readings, indicating high precision of the automatic adjustment.
Conclusion
This study presents preliminary results, showing that Auto Strut can successfully replace the manual strut adjustment providing important advantages that benefit the patient, the caregiver and the surgeon.
Level of Evidence
Level II
Introduction
The Ilizarov surgical method was developed in the 1950s and was introduced to the Western world 30 years later, and has been used to achieve gradual correction of deformities, both congenital and acquired.1–4 The use of Ilizarov circular external fixators for lengthening and axial correction requires mechanical hinges and translation mechanisms for constructing a custom-made frame for each patient. 5 The method is principally based on the application of circular frames followed by osteotomy and gradual distraction or compression in three dimensions to attain the biomechanical environment for bone healing.6–8 Correcting a deformity in all planes requires multiple sequential adjustments during treatment. Such mechanical corrections may impose difficulties that have shown to decrease the accuracy of correction. 9
Several technological improvements were developed and are in use today. A powerful tool for obtaining precise correction of limb deformities is the hexapod frame; a substitution of the threaded rods and hinges of the traditional Ilizarov frame with a hexapod system of six telescopic struts at the focal level. The first hexapod fixator that has been in use for more than 25 years is the Taylor Spatial Frame (Smith and Nephew, Memphis, TN) (TSF). The TSF, introduced by Charles Taylor in 1994, is a stable external fixation device with six-axis deformity apparatus.6,7,9,10 It has at least two circular rings connected by six telescopic crossing struts that allow external control in six degrees of freedom. 11 It does not require construction of mechanical hinges and precise mounting of the ring fixator, and relies on the adjustment of the strut lengths. 12 The surgeon assembles the computerized correction plan via a frame software algorithm. It provides an initial and final set of struts lengths aiming to achieve the planned correction of a deformity. 6 The patients and caregivers are provided with the treatment plan and manually adjust the struts to implement a multiplane simultaneous correction plan.6,10,13,14
The MaxFrame (DePuy Synthes USA, LLC) device, which was introduced later, is designed as a multi-axial correction system to reduce procedure complexity by streamlining the surgical and software workflows.15,16 The TSF and MaxFrame fixators require manual adjustment of the struts several times a day. The duration of treatment is defined by the deformity and the intended change and could range between 30 days and several months, increasing the burden on the patients and their caregivers. 17
Bright and colleagues 18 described a prototype of motorized distraction fixator based on the Ilizarov method. They reported tibial lengthening with motorized distraction at a rate of 1 mm per day in 1440 steps. Eren et al 19 used the Smart Correction fixator in a clinical study and demonstrated higher deformity correction accuracy than the Ilizarov external fixator.
OrthoSpin Ltd (Israel, Misgav) has developed the Auto Strut system which is intended to replace the manually controlled struts in a hexapod fixator. Auto Strut includes control units that are mounted on the fixator and are then connected to the six motorized robotic struts. The control unit in accordance with a pre-programmed treatment plan performs the execution of the strut adjustments automatically.
The Auto Strut system received a Food and Drug Adminstration approval (K191241) for utilization in combination with the MaxFrame fixator. In accordance with the approval, Auto Strut can be used for fracture fixation (open and closed), pseudoarthrosis of long bones, limb lengthening, joint arthrodesis, infected fractures or nonunion, correction of bony or soft-tissue deformities and correction of segmental defects.
In this study we present our experience with ten patients who underwent deformity correction using the Auto Strut system.
Materials and methods
The study protocol and modifications for utilization of the Auto Strut system in combination with the hexapod fixator (TSF or MaxFrame) were approved by the Helsinki Committee of our medical centre.
Device
The Auto Strut device is presented in Figure 1. The device is comprised of one central control box connected to two lateral control boxes.

Auto Strut device assembled on a circular fixator: a) Auto Strut device; b) assembled on patient's leg.
After being mounted onto the fixator, each box is connected to two adjacent struts via an electrical cable. The addition of the Auto Strut components makes the fixator approximately 760 g heavier than the manually adjustable one.
System components
Motored strut: the mechanics of the motored strut are based on a threaded tube that is extended by a rotating screw element. The struts are connected to the pair of external rings in a similar way to the mechanical strut (i.e. same interface and locking bolt).
Motor and gear: the motor and gear lengthen or shorten the strut according to the treatment plan. Each motor is connected to an encoder that senses its rotational positioning and enables the controller to close the control loop.
Electronic controller: the controller is in command of the motor's speed and direction according to the treatment plan. It provides hardware and software protections that prevent any deviation from the treatment plan and alert in case of any malfunctions.
Power supply: three standard 9 V lithium batteries supply energy to the system. The alarm system is activated (red light) when the battery is running low.
Alarm system: activated automatically when a device malfunction or connector assembly problem is detected by the electronic controller.
Following a standard surgical procedure, a portable document format (PDF) file of the treatment plan is produced by the MaxFrame or TSF software.
The PDF file is imported into OrthoSpin software and uploaded to the central control box (Fig. 2) from the external computer via a Universal Serial Bus (USB) cable. The central control box controls the strut adjustments in accordance with the plan without any involvement from the patients/caregivers.
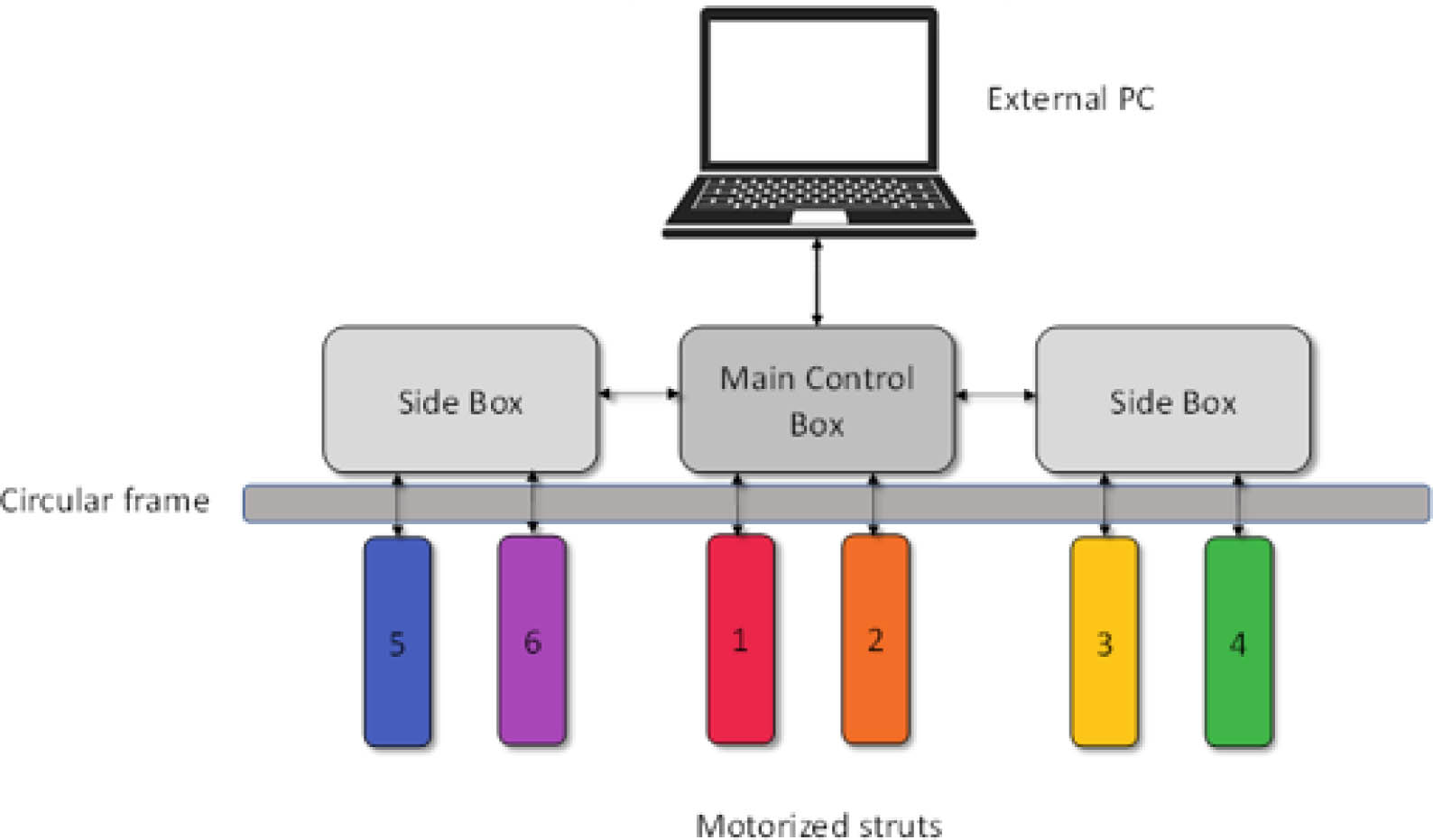
Schematic diagram of the Auto Strut system. A control unit is placed onto the frame of the fixator. It is connected by a Universal Serial Bus cable to the external computer for downloading the treatment plan, prior to treatment initiation.
Patients and treatment procedure
Patients were assessed for suitability to be treated with the hexapod external fixator.
Patients between three and 20 years old were eligible to participate in the study. Exclusion criteria included an allergy to any of the device components, active systemic disease, malignancy or active infection. Prior to treatment initiation, adult patients/parents of the minor patients provided informed consent to being treated with the novel device.
Following confirmation, a surgery was scheduled to place the fixator. The Auto Strut control boxes were mounted on the circular frames after the surgical procedure. A treatment plan for the strut adjustment was generated based on the characteristics of the limb deformity and hexapod external fixator mounting and then downloaded into the Auto Strut central control box. When activated, the control boxes carried out the strut adjustment automatically, in accordance with the treatment plan, with no intervention required from the patient or the caregiver. Patients arrived at the clinic for follow-up during the correction period until treatment completion.
Results
A treatment with a hexapod external fixator, in which the manual struts were substituted with the Auto Strut automatic device, has been initiated in ten 12- to 20-year-old patients (five girls). All patients completed the treatment plan. The alarm system was activated twice in one patient (patient 02), indicating a device malfunction (connector assembly problem). Although the malfunction was solved, the Auto Strut device was replaced with manual struts as the patient preferred not to go back to the Auto Strut.
Patients’ demographic characteristics and the aetiology of their orthopaedic impairment are presented in Table 1.
Demographics
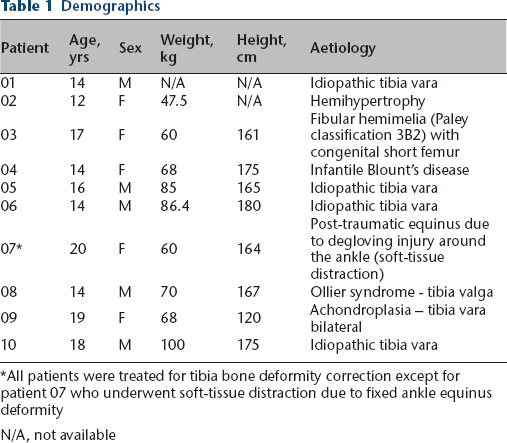
All patients were treated for tibia bone deformity correction except for patient 07 who underwent soft-tissue distraction due to fixed ankle equinus deformity
N/A, not available
Four of the ten patients had pre-existing medical conditions, which included fatty liver disease (patient 02), pervasive developmental disorder (patient 05), anxiety disorder (patient 07) and obstructive sleep apnea due to achondroplasia (patient 09). Out of the ten patients, only patient 07 reported concomitant medication use, treated with Olanzapine 10 mg once daily.
Details on the planned corrections, distraction and consolidation parameters and treatment duration are presented in Table 2. Nine patients received unilateral treatment (seven left limbs and two right limbs) and patient 09 was treated bilaterally. The corrections involved axial lengthening for all patients, axial angulation for five patients, anteroposterior angulation (varus/valgus) for eight patients and lateral angulation (posterior/anterior) for three patients. Time to recovery, defined as the time between the placement of the device (date of operation) and the imaging results indicating three cortex regenerate consolidation, ranged between one and seven months. Duration of distraction ranged between ten and 90 days. The distraction index, defined as the period (in days) required per cm of change (lengthening/angulation), ranged between 8 days/cm and 15 days/cm. The length of distraction varied between 1 cm and 6 cm.
Planned treatment and outcomes
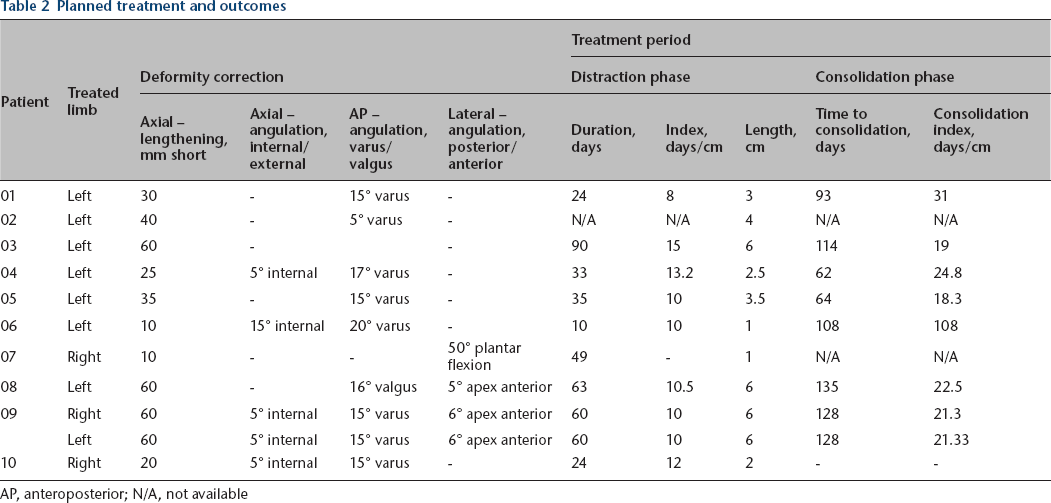
AP, anteroposterior; N/A, not available
The planned corrections were fully attained in all patients who completed the treatment and no device-related adverse events were reported.
The precision of the automatic adjustment of the struts was assessed by calculating the absolute discrepancy of the final reading on each strut relative to the planned final number. Data from 48 struts (eight patients) was collected for precision analysis. Patient 01's actual numbers on the struts were not recorded every office visit and patient 2 switched into manual struts during the treatment period. Of those 48 struts, 94% (45/48) of the final strut number readings presented a discrepancy of 0 mm to 1 mm. Final strut number readings from three struts (6%) presented a discrepancy of 2 mm to 3 mm. These differences probably stem from errors in strut readings as they are mainly associated with the struts that were located more internally (between the legs) or posteriorly, precluding comfortable visual access thus making the accurate reading more challenging. The discrepancy of 2 mm to 3 mm is clinically insignificant. The automatic adjustment readings of the six struts taken during the treatment course of a representative patient (patient 08) are presented in Figure 3, together with the planned adjustment.
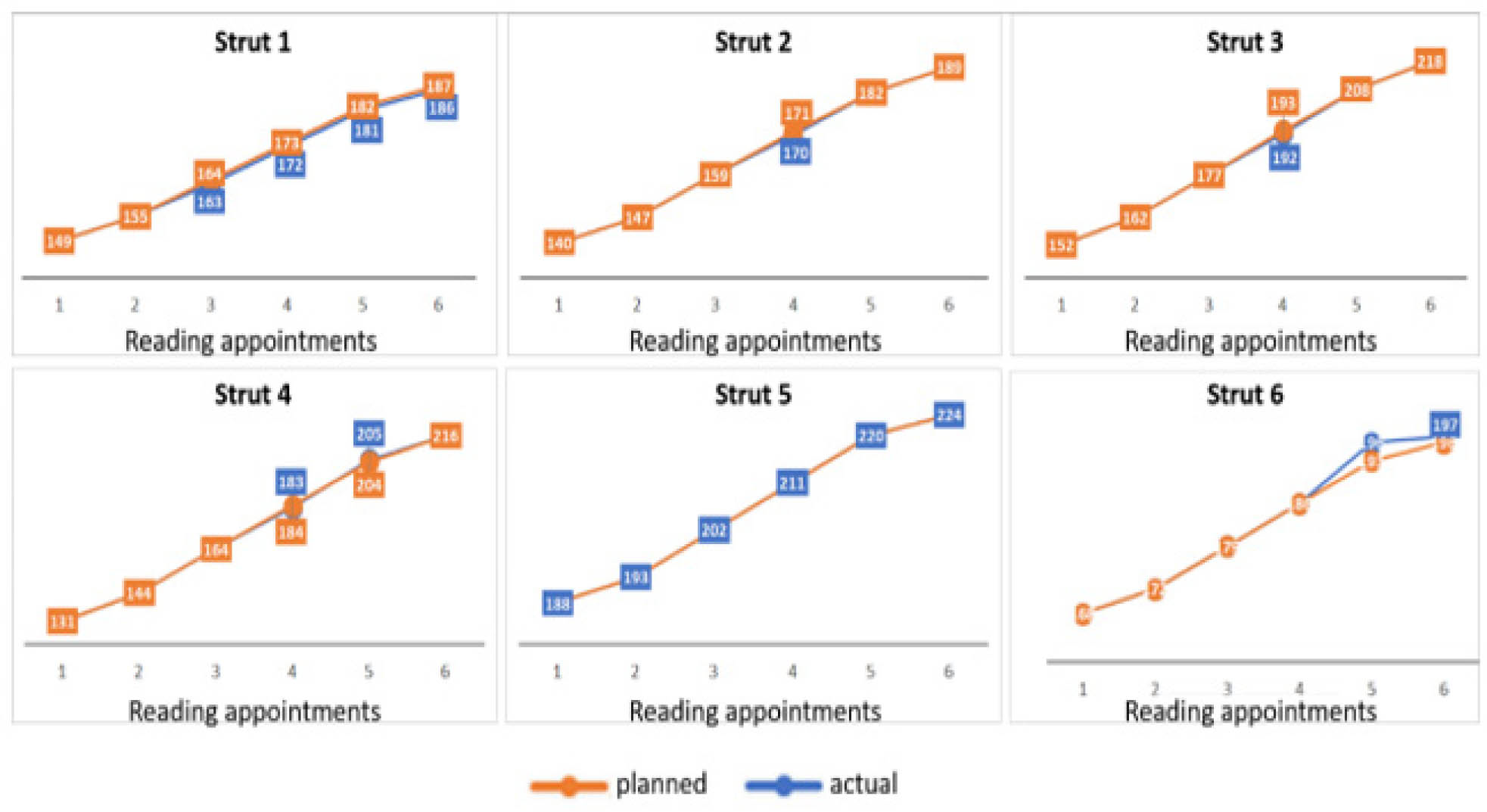
Automatic strut adjustment versus planned readings of a representative patient (patient 08). The actual automatic adjustment (blue) is presented against the office visits readings (orange) for each of the six struts of the hexapod external fixator. Readings of the scale numbers of the struts were carried out on six time points during the treatment course (x-axis). Y-axis represents number on the struts.
Out of 36 readings (six reading per strut) obtained during the course of treatment, 26 showed 100% accuracy of adjustment, nine readings indicated discrepancy of 1 mm and a single reading showed 3 mm discrepancy, which is clinically insignificant.
Radiographic images of a representative patient (patient 09) three months after fixator installation surgery and six months after fixator removal surgery, are presented in Figure 4.
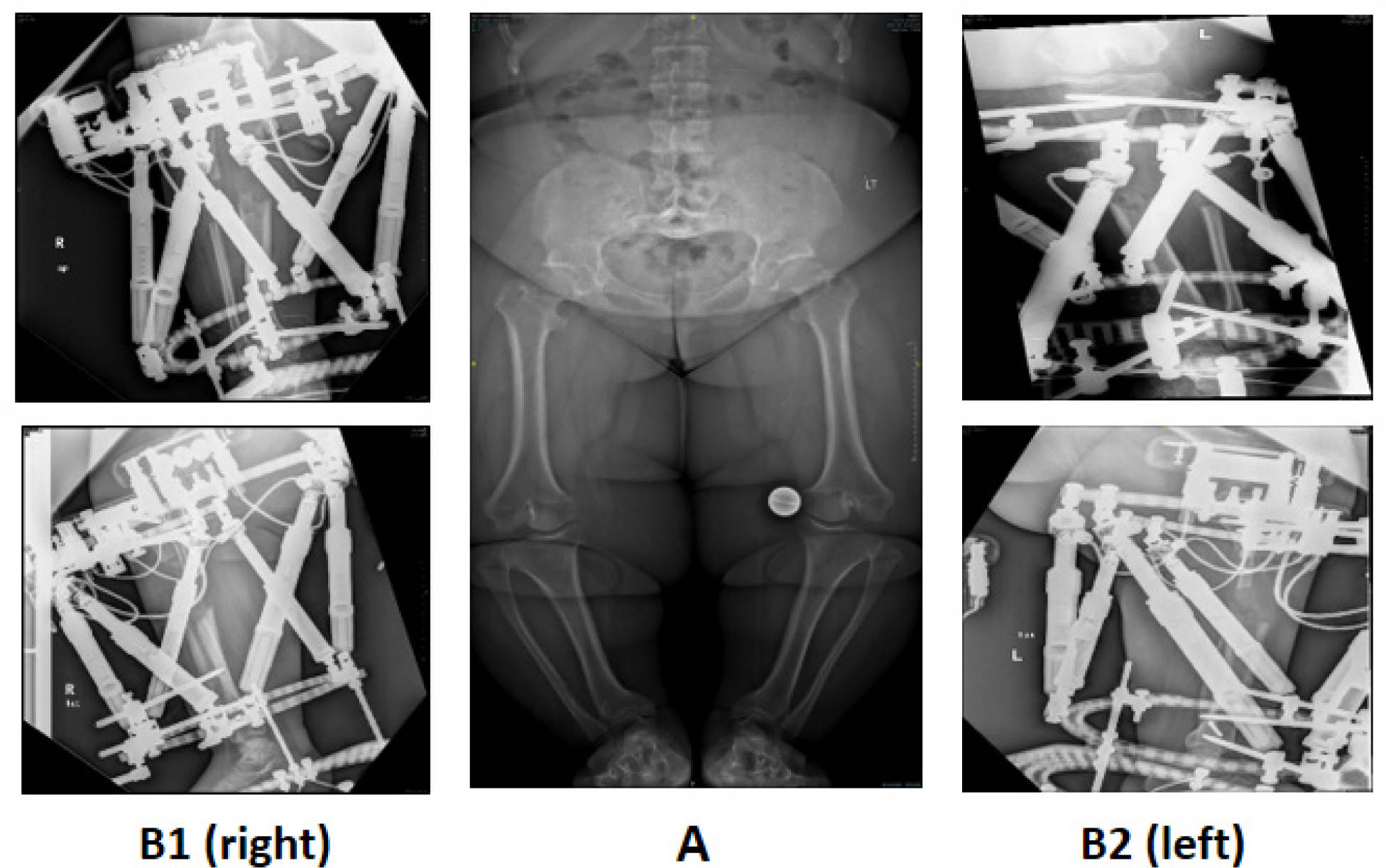
Radiographs before surgery and during distraction of bilateral tibia vara with Auto Strut Hexapod external fixation system in 19-year-old achondroplasia patient: a) preoperative leg-length radiograph of 19-year-old achondroplasia patient for deformity correction and lengthening procedure; b) radiograph after 60 days of distraction for bilateral tibial genuvarum correction and lengthening, using Auto Struts over an circular cexapod external fixator system.
Discussion
We have presented the successful utilization of an automated hexapod external fixator in the treatment of bone deformities.
The treatment duration, correction success and adverse events observed in our study indicate that utilizing the Auto Strut device with the hexapod external fixator for automatic gradual deformity correction is safe and as accurate as manually adjusted struts.6,11,14,20 Manual strut adjustment is dependent on patient/patient family collaboration and is prone to errors. Errors may rise as the numbers of daily manual operations increase. The results showed that the Auto Strut system is highly accurate (94%) indicating high precision of the automatic adjustment ensuing full compliance with the preplanned schedule.
An additional advantage of Auto Strut utilization is the elimination of the burden associated with the manual adjustments. This, in turn, enables a more independent life during treatment and reduction in the loss of working days lost for both the patients and caregivers.
Auto Strut is easy to use. No alteration of the standard surgical procedures is required. The mounting of the device onto a fixator is intuitive and does not require any additional training. Uploading the treatment plan to the device can be easily done, using a computer with a USB-cable-mediated connection to the central control box.
Auto Strut provides numerous technical possibilities. As a programmable multi-purpose device, it allows the implementation of diverse treatment schedules and, therefore, is applicable to the treatment of diverse bone impairments, including, nonunion, correction of bone deformities and segmental defects.
Further treatment schedules will be based on smaller increments, which will be implemented more frequently, from four to 20 or more steps. This could improve the quality and speed of bone formation during correction. The system can be adjusted to perform a continuous distraction compression schedule, the ‘accordion’ motion (an accepted technique to speed bone healing in cases delayed or nonunion), as well as any other appropriate schedules.
Future developments will increase its modularity, allow the collection of information associated with bone healing, such as the parameters of bone resistance during various treatment stages, which may be indicative of the maturity/strength of the newly formed bone. The availability of such information, recorded online, during the treatment, could advance research of bone formation and shed light on the clinically significant details of bone healing. This knowledge will lead to the construction of improved and personalized treatment plans.
We believe that Auto Strut can successfully replace the manual strut adjustment method and provide several important advantages that benefit the patient, the caregiver, the surgeon and may have important future research implications.
Footnotes
Dr Eitan Segev reports he is Chief Medical Consultant to Orthospin company.
All other authors declare that they have no conflict of interest.
JM: Manuscript writing and revision.
IL: Data acquisition, Interpretation of data, Revision of manuscript.
DO: Interpretation of data, Manuscript writing and revision.
ES: Study design, Data acquisition and analysis, Interpretation of data, Manuscript writing and revision.