
Abstract
Abstract
Purpose
Late-diagnosed dislocated hips underwent open reduction, Dega osteotomy, and proximal femoral osteotomy between 1968 and 1988. The objectives of this study are to assess the survival of hips into adulthood, clinical and radiological outcome, patients’ life perspectives and the risk factors of failure.
Methods
An assessment of 67 hips treated when younger than five years (<age 5yr. group) and 71 hips in the group aged older than five years (+age 5yr.) was performed. All cases were evaluated clinically and radiographically, and survival was assessed, considering hip replacement as endpoints for failure (abbreviation HR+ refers to hips that underwent hip replacement surgery; HR- refers to hips that have not been replaced at the follow-up). The fertility rate and the social security disability benefits (SSDB) recipiency percentage were calculated.
Results
The 40-year survival rates were 73% (95% confidence (CI) 71% to 76%) in the <age 5yr. group, 54% (95% CI 51% to 57%) in the +age 5yr. group, 70% (95% CI 67% to 73%) in one-sided dislocations and 57% (95% CI 54% to 60%) in bilateral dislocations. At follow-up, the median Harris hip and Western Ontario and McMaster Universities Osteoarthritis scores were 90.0 and 13.0 (<age 5yr. group, HR-), 74.0 and 28.0 (+age 5yr. group, HR-), 90.0 and 16.0 (<age 5yr. group, HR+) and 84.5 and 11.5 (+age 5yr. group, HR+), respectively. The operation normalized the radiological parameters. The correlation between the grade of femoral head avascular necrosis (AVN) at a median 2.6 years after the operation and the grade of osteoarthritis at follow-up was 0.38 (p < 0.001). The fertility rate was 1.54. In total, 16.0% (aged under five years) and 38.5% (aged over five years) of patients were receiving SSDB (p = 0.003).
Conclusion
Early failure risk factors are older age at the surgical procedure, high AVN grade and bilateral hip involvement. Still, the results facilitate hip reposition whenever technically manageable, even in teenagers.
Level of evidence
III
Keywords
Introduction
Developmental dysplasia of the hip (DDH) is the most common neonatal hip disorder and is characterized by an abnormal relationship between the femoral head and acetabulum of otherwise healthy children. 1 Since the introduction of universal ultrasound screening to clinical practice in some European countries (e. g. Austria, Germany, Poland), the number of DDH patients who require surgical treatment has significantly dropped. 2 Nevertheless, late-diagnosed hip dislocations are still reported and provokes a question about the upper age limit at which surgery provides a superior outcome to the natural history of the disease and about the most suitable technique for delayed DDH diagnosis. 3
In 1969 Wiktor Dega described the surgical technique of the pelvic osteotomy in Polish.4,5 In 2001, the description of the Dega osteotomy (DO) in English 6 caused interest in the technique to gradually increase. The longest published follow-up for this method is 16.6 years, with favourable results in 75.9% of patients.7,8
Historically, the hip acetabulum's remodelling potential was considered to be present until the age of 12 years if the concentric reduction had been obtained before the age of four years. 9 In the 1970s, in Poland, an age of three to five years was considered optimal for surgical treatment with open reduction (OR) and DO (OR+DO). 10 More recently, Herring 11 suggested not treating hips in patients older than eight years (when bilaterally dislocated) and nine to ten years (when unilaterally dislocated). Other authors have supported performing surgical hip reconstruction up to the age of six 12 or seven years, 13 while others have described satisfactory results even in children older than eight years.14–16 Unfortunately, only a limited number of papers have assessed the outcome of untreated hip dislocations into adulthood, providing inconsistent results.17–19
This study aims to assess the survivorship of hips into adulthood after OR+DO and proximal femoral osteotomy (PFO), functional and radiological outcome, the life perspectives of treated patients (fertility rates in women, social security benefits recipiency) and the risk factors of failure.
Materials and methods
The study is a retrospective review of a prospectively assembled cohort. The approval of our institutional review board (No. 666/17) and written patient consents were obtained.
The study compares the outcome of treatment in the group of children who underwent the surgical procedure when younger than five years (<age 5yr. group) with those treated at the age of five years or older (+age 5yr. group) to confront the historical guidelines of treatment that assumed age over five years would worsen the outcome. 10
The inclusion criteria were: DDH, with no other chronic diseases, e.g. genetic syndromes; dislocated hip joint (grade III to IV in the Tönnis classification) 20 ; treatment protocol including OR+DO; operation between 1968 and 1988.
In our hospital archives, 112 medical records were identified that fulfilled the inclusion criteria for the +age 5yr. group. Selection of the <age 5yr. group was based on the randomization of 867 medical records of patients who underwent DO+OR. The statistician (IM) drew 223 out of 867 medical records taking into account the primary group's age distribution. A manual search through those according to the inclusion criteria left us with 133 medical records.
The patients were tracked down, despite the length of time since surgery posing many obstacles (out-of-date addresses, changes in surnames).
In all, 50 patients (45 female and five male; 67 hips) responded positively in the <age 5yr. group (37.6% response rate) and 52 (46 female and six male; 71 hips) in the +age 5yr. group (46.4% response rate). In the <age 5yr. group, the final age distribution did not differ from the distribution in the randomized group of 223 patients (p = 0.08, chi-squared test). A total of 91 patients accepted an invitation to the outpatient clinic and 11 were assessed in their home facilities (the general practitioner ordered pelvic anteroposterior radiograph). The data were collected between March 2017 and November 2019.
In all, 52.2% of hips in the <age 5yr. group and 56.3% in the +age 5yr. group had received some treatment before the primary surgical procedure (see Appendix).
In the <age 5yr. group, 95.5% hips (64/67) had DO+OR and shortening PFO performed. In 1.5% of hips (1/67), DO+OR and derotation PFO was performed. In total, 3.0% of hips (2/67) hadn't any accompanying procedures added to DO+OR (one patient was treated before the age of two years bilaterally and did not need PFO). In the +age 5yr. group, 95.8% of hips (68/71) had DO+OR and shortening PFO performed. In 4.2% of hips (3/71), DO+OR and derotation PFO were performed (the femoral pressure was relieved by iliopsoas muscle transposition). In every hip, OR+DO was performed as described by Dega 21 and Grudziak and Ward. 6 Detailed characteristics of procedures accompanying OR+DO are listed in the Appendix.
Pelvis anteroposterior radiographs were taken at a median time of 23 days (interquartile range (IQR) 11 to 63) before the primary operation and assessed by the grade of hip dysplasia 20 and acetabular index (AI). 11
The radiograph taken at least one year after the primary operation (median 2.6 years; IQR 1.9 to 3.3) was available for 136 hips to assess the grade of the femoral head avascular necrosis (AVN) according to the Kalamchi-MacEwen (K&M) classification system (the radiographs for two hips were not available in medical archives). 22 The division of all hips (<age 5yr. and +age 5yr. together) into groups without AVN and with AVN scored 1 to 4 was done to estimate the classification system's long-term predictive value. The correlation between the patient's age at the primary operation and the AVN grade was calculated. AI values and migration percentage (MP) 23 were measured in every radiograph.
At the follow-up, radiographs taken at a median time of 0 days before the visit (IQR 0 to 11) were assessed. All but four radiographs were taken no longer than one year before the visit (four patients did not grant permission for the radiographic examination; the most recent radiographs were assessed). Radiographs of hips that had not been replaced were graded by comparison with the atlas standards of the Kellgren-Lawrence (K&L) osteoarthritis (OA) classification system. 24 The <age 5yr. and +age 5yr. groups were compared by the length of follow-up, patient's body mass index (BMI), fertility rate (births per woman), the percentage of patients receiving social security disability benefits (SSDB) and the primary surgery reoperation rate (see Appendix). Every patient was assessed clinically based on the modified Harris hip score (HHS), and fulfilled the HHS 19 and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) 25 questionnaires. The rate of hip replacement (HR) surgical procedures was calculated. Throughout the text, the abbreviation HR+ refers to hips that underwent HR surgery; HR- refers to hips that have not been replaced at the follow-up. In the HR+ group, the time between primary surgery and HR operation was calculated. The HHS and WOMAC scores were calculated in the <age 5yr. HR+ and +age 5yr. HR+ groups. Survival was assessed using Kaplan-Meier curves and compared statistically between the <age 5yr. and +age 5yr. groups. The end of follow-up or the HR operation date (for replaced hips) was considered the endpoint. The analogous analysis was performed for <age 5yr. and +age 5yr. hips (together) with division into one-sided and bilaterally dislocated hips. The data become unreliable when there are fewer than ten hips in the tail of the survival curve. 26 Moreover, the correlations between the AVN grade and OA grade at follow-up, between the AVN grade and HHS, and between AVN grade and WOMAC score were calculated.
Every radiograph was converted to a digital format. Scoring of radiographs and angle measurements were performed in ImageJ Software ver. 1.51 (NIH, Bethesda, Maryland, USA) by the first author (ŁW), blinded to other parts of the assessment.
Normally distributed data were presented by the mean with standard deviation and compared between the <age 5yr. and +age 5yr. groups by the Student's t-test. The not normally distributed data were presented as the median with IQR and assessed by the non-parametric Mann-Whitney U test. The percentage of patients receiving SSDB, the reoperation rate and the HR operation rate were compared between groups by the Pearson chi-squared test. Spearman rank correlation coefficient was used. The Tarone-Ware test compared the Kaplan-Meier curves. A p-value < 0.05 was considered significant.
Results
Before the primary operation
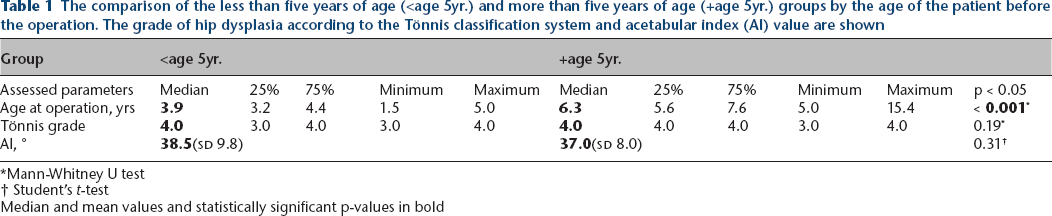
There were no differences between the <age 5yr. and +age 5yr. groups in terms of grade of hip dysplasia and AI values (Table 1). In <age 5yr. group, there were 20 hips of Tönnis grade III and 47 hips of grade IV. In the +age 5yr. group, there were 15 hips of grade III and 56 hips of grade IV.
The comparison of the less than five years of age (<age 5yr.) and more than five years of age (+age 5yr.) groups by the age of the patient before the operation. The grade of hip dysplasia according to the Tönnis classification system and acetabular index (AI) value are shown
Mann-Whitney U test
Student's t-test
Median and mean values and statistically significant p-values in bold
At the primary operation
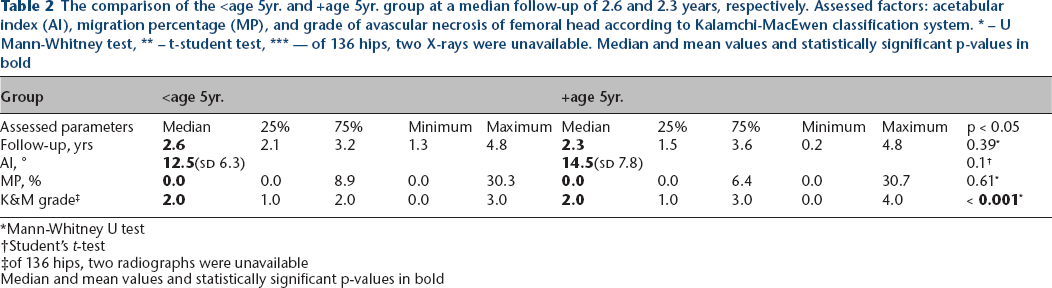
There were no differences between groups in terms of AI and MP at a median follow-up of 2.6 years (IQR, 2.1—3.2) in <age 5yr. and 2.3 years (IQR, 1.5—3.6) in +age 5yr. group. The grade of AVN was significantly higher in the +age 5yr. group (Table 2).
The comparison of the <age 5yr. and +age 5yr. group at a median follow-up of 2.6 and 2.3 years, respectively. Assessed factors: acetabular index (AI), migration percentage (MP), and grade of avascular necrosis of femoral head according to Kalamchi-MacEwen classification system. * – U Mann-Whitney test, ** – t-student test, *** — of 136 hips, two X-rays were unavailable. Median and mean values and statistically significant p-values in bold
Mann-Whitney U test
Student's t-test
of 136 hips, two radiographs were unavailable
Median and mean values and statistically significant p-values in bold
Radiographs showed no AVN signs in 15 hips, AVN grade 1 in 35 hips, grade 2 in 58, 3 in 23 and 4 in five joints. The correlation coefficient between the patients’ age at the primary surgical procedure and the AVN grade was 0.47 (p < 0.001). Joints that showed no signs of AVN underwent operation at a mean age of 3.6 (sd 1.1). Those with AVN grades 1 to 4 were treated at the mean age of 5.0 years (sd 1.9), 5.0 years (sd 1.4) and 6.9 years (sd 2.0) and 10.0 years (sd 3.5), respectively.
At the follow-up
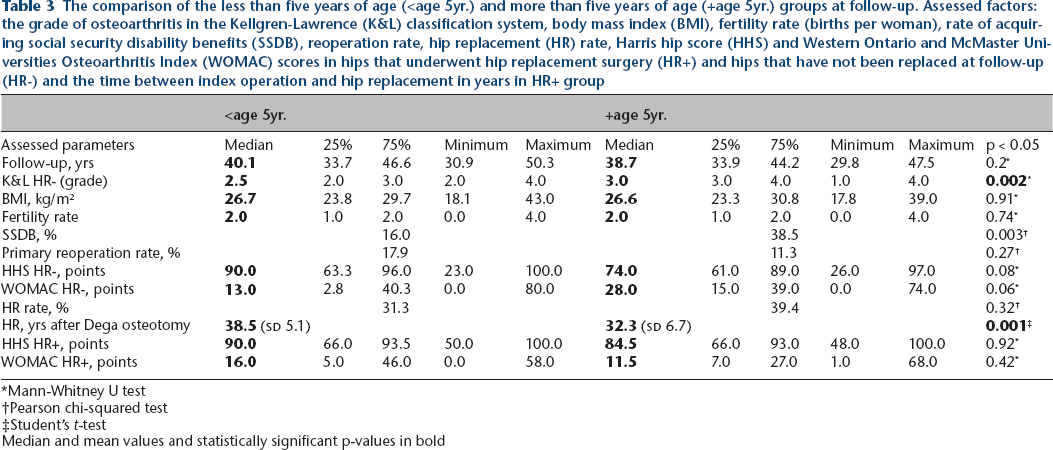
There were no differences in patient BMI, fertility rate, primary reoperation rate, HHS and WOMAC scores. The K&L grade was significantly higher in the +age 5yr. group, the same as the percentage of patients who required SSDB. HR rate was comparable in both groups, but patients who underwent primary surgical procedure when five years or older required arthroplasty earlier. HR+ patients scored comparably in HHS and WOMAC scales in the <age 5yr. and +age 5yr. groups (Table 3).
The comparison of the less than five years of age (<age 5yr.) and more than five years of age (+age 5yr.) groups at follow-up. Assessed factors: the grade of osteoarthritis in the Kellgren-Lawrence (K&L) classification system, body mass index (BMI), fertility rate (births per woman), rate of acquiring social security disability benefits (SSDB), reoperation rate, hip replacement (HR) rate, Harris hip score (HHS) and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores in hips that underwent hip replacement surgery (HR+) and hips that have not been replaced at follow-up (HR-) and the time between index operation and hip replacement in years in HR+ group
Mann-Whitney U test
Pearson chi-squared test
Student's t-test
Median and mean values and statistically significant p-values in bold
The hips’ survival in the <age 5yr. group was better than in the +age 5yr. group (p = 0.02). The data become unreliable after 43.5 years. The survival rates at 30 years after hip reduction are 100% in the <age 5yr. group and 86% (95% confidence interval (CI) 85% to 87%) in the +age 5yr. group. At 35 years it was 88% (95% CI 86% to 89%) in the <age 5yr. group and 74% (95% CI 73% to 76%) in the +age 5yr. group. At 40 years it was 73% (95% CI 71% to 76%) in the <age 5yr. group and 54% (95% CI 51% to 57%) in the +age 5yr. group. At 43 years it was 64% (95% CI 60% to 67%) in the <age 5yr.group and 50% (95% CI 45% to 54%) in the +age 5yr. group (Fig. 1).
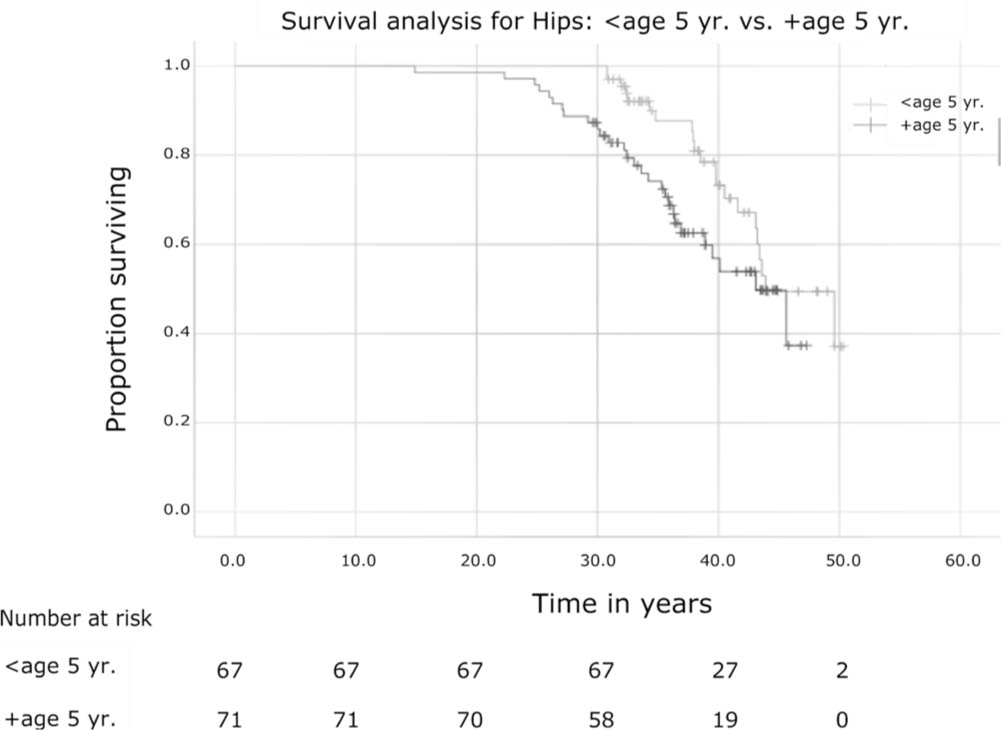
The Kaplan-Meier survival curve for the less than five years of age group (<age 5 yr.) (grey line) and more than five years of age group (+age 5 yr.) (black line), with hip replacement as the endpoint. Number of hips at risk at the timeline below the graph. The difference in curves statistically significant (p = 0.02 in the Tarone-Ware test).
The hips’ survival was better in one-sided than in bilateral dislocations (p = 0.048). The data become unreliable after 43.2 years. The survival rate at 30 years after reduction is 94% (95% CI 93% to 95%) in one-sided and 90% (95% CI 89% to 91%) in bilaterally involved hips. At 35 years it was 85% (95% CI 83% to 86%) in one-sided and 75% (95% CI 74% to 77%) in bilateral cases and at 40 years it was 70% (95% CI 67% to 73%) and 57% (95% CI 54% to 60%), respectively (Fig. 2).
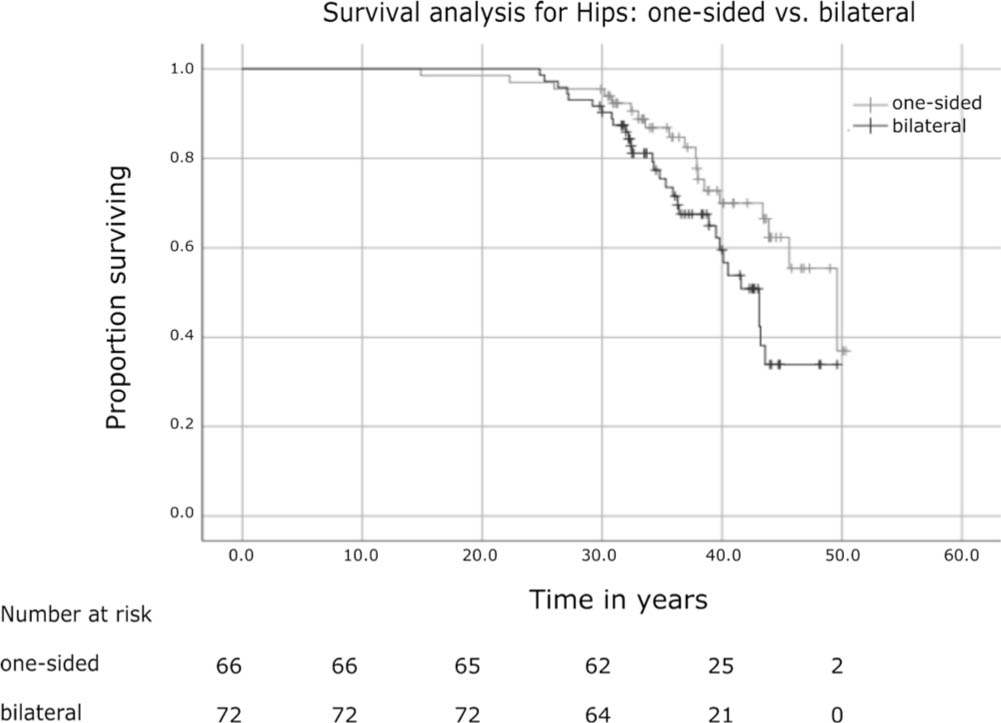
The Kaplan-Meier survival curve for one-sided (grey line) and bilateral hip dislocations (black line), with hip replacement as the endpoint. Number of hips at risk at the timeline below the graph. The difference in curves statistically significant (p = 0.048 in the Tarone-Ware test).
The correlation coefficients between the AVN grade and the OA grade, the HHS and the WOMAC score were 0.38 (p < 0.001), -0.23 (p = 0.03) and 0.25 (p = 0.02), respectively.
Discussion
The present study was designed to assess the influence of DDH surgical treatment (OR+DO+PFO) on patients’ life perspectives into adulthood. It focused not only on functional and radiological assessment but attempted to investigate the social and demographic impact of the disease. The 40-year follow-up allowed for a multilayer assessment that is uncommon in papers presenting surgical treatment results.
We believe that a delayed DDH diagnosis is not only of historical concern, as the study of Broadhurst et al 3 proved that it is still being diagnosed late in England. The selective screening programme introduced there in 1986 has not seemed to reduce the incidence of late-diagnosed DDH. 27
This study implicates that HR had been performed earlier after DO in the +age 5yr. group than in the <age 5yr. group. Despite this fact, 60.6% of hips had not been replaced in the +age 5yr. group. Among 28 joints that had needed HR, the mean time between the DO and HR of 32.3 years (sd 6.7) prolonged living with a preserved joint into patients’ late 30s or early 40s. Moreover, every joint that needed HR in the present study underwent arthroplasty without the subtrochanteric shortening osteotomy. It eliminated the additional risk of nonunion on the operative side, reported as 4.2% to 20.0%. 28 Moreover, the clinical examination revealed no patient presenting with hip flexion contracture and subsequent hyperlordosis of the lumbar spine after the primary procedure (based on the medical records) what seems inevitable in untreated patients with bilaterally dislocated joints. 1
This paper's advantage is the accessibility of pre-operative radiographs and radiographs taken after the procedure in short-term follow-up. It allowed for the measurement of the radiological parameters before, at the operation and at the follow-up. Postoperative radiograph analysis proved the value of DO in correcting the AI and MP to normative values. 11 The assessment of radiographs by the K&M classification showed a moderate positive correlation between the patient's age at primary surgical procedure and the AVN grade at short-term follow-up. The latter showed a weak positive correlation with OA grade and WOMAC scores and a weak negative correlation with the HHS score. The general tendency towards the worsening of radiological and clinical outcomes with a higher AVN grade leads to the conclusion that the K&M classification helps predict the long-term outcome of late-diagnosed DDH. High inter- and intraobserver reliability recommend it as the assessment tool in late-presenting DDH. 29
According to Statistics Poland, 4.1% of the Polish population at working-age received SSDB because of their incapability to work in 2019.30,31 In the present study, the percentage of SSDB beneficiaries was much higher, especially in the +age 5yr. group. It indicates that early DDH diagnosis might lower not only the cost of treatment but indirect state expenses. The study of Thallinger et al 2 reported a 46.0% decrease in the OR number since the introduction of a nationwide ultrasonographic DDH screening programme in Austria. Another point of discussion relates to the cost-effectiveness of selective versus universal DDH screening programmes, that may warrant the latter.2,27 The material fertility rate was 1.54 compared with 1.46 in the Polish population in 2018. 32 Despite female patients’ concern regarding pelvic osteotomy's negative effect on childbearing, our results show no difference in fertility rates between the general population and women diagnosed with late-presenting DDH.
Studies presenting short-term outcomes of different surgical techniques in DDH support the hypothesis that performing OR with femoral and pelvic osteotomy is beneficial even when a child is older than eight years.14–16 On the other hand, a limited number of publications assessed the natural history in DDH. Wedge and Wasylenko 19 reported that only 41% of 42 untreated dislocated hips had good rates of HHS (> 71 points) at 16 to 86 years of age. In the present study, in the HR- group, 59.6% of 89 hips had good rates of HHS at the median age of 42.3 years (IQR 37.8 to 47.5), but when considering hips after HR as a failure of treatment, it would leave us with only 38.4% favourable results. In contrast to that, in Crawford et al's 17 study, a good clinical and radiological outcome was obtained in 20 untreated hips at the average age of 40 years, with only one hip (5.0%) requiring HR. The lack of prospective randomized studies makes it impossible to compare surgical treatment with the disease's natural course.
To our knowledge, only three studies33–35 have assessed the treatment outcome of DDH patients with comparable follow-up length (Table 4). Our material hips survivorship is worse at 40-years than in Terjesen 33 or Thomas et al's 34 studies by 32% and 23%, respectively. Higher median patient age at operation in this study might drive this difference and influence much higher AVN rates than in other studies. Even excluding mild AVN cases (AVN grade 1), our study's AVN rate is 63.2%, despite performing shortening PFO in 96% of treated joints to lower the acetabulum pressure on the femoral head. Terjesen 33 reported an AVN rate of 8.1% and Thomas et al 35 of 5.7%, while not performing shortening PFO. It might suggest that the natural history of untreated DDH is more responsible for AVN development than excessive femoral head pressure. Still, we agree with Herring's 11 recommendation to perform shortening PFO in every dislocated hip in children older than two years and consider it even in younger children if excessive pressure is placed on the reduced femoral head. In this material, median AVN grade was higher in the +age 5yr. group than in the <age 5yr. group. The data seem to confirm that the younger the child at DDH operative treatment, the lower the AVN risk and potentially the higher the long-term hip survival rate. Nevertheless, it should be underlined that no significant difference in the clinical outcome between the <age 5yr. (median age 3.9 years) and +age 5yr. (median age 6.3 years) groups seems to justify OR+DO+PFO operation at the age >5yr. or even in teenagers in late-diagnosed cases. We should still have in mind that better results are expected in children younger than included in this analysis.
Comparison of the results of developmental hip dysplasia treatment with other studies at 30-years and 40-years follow-up

CI, confidence interval; CR, closed reduction; OR, open reduction; NA, not available; DO, Dega osteotomy; PFO, proximal femur osteotomy
The limitation of this study is its retrospective character with no DDH natural history control group. Unfortunately, the number of joints that underwent surgery at an age older than eight years was too low to perform the analysis. Therefore, this study has no justification in denying surgical treatment at that age of dislocated joints. The variety of procedures accompanying DO may raise the question about the importance of DO in the surgical technique (see Appendix). Every patient who presented with radiographic signs of hip dislocation (Tönnis grade III to IV) was included in the analysis despite previous medical interventions. 20 This approach is different from that of Thomas et al, 34 who excluded patients who received any treatment before the surgical procedure. This study assessed patients with very late presenting DDH (median 5.0 years; IQR 4.0 to 6.3), making it one of the oldest series of DDH patients. Many late presenting DDH patients were initially referred to the outpatient clinic in our centre, where they received non-surgical treatment between the 1960 and 1980s. Nowadays, those children would be treated primarily surgically. It might have raised the percentage of non-surgically treated patients before the primary operation.
In conclusion, OR+DO+PFO facilitates the correction of the anatomical pelvis parameters in delayed DDH diagnosis. This study proves its value in prolonging patient's living with a native reduced hip into adulthood. Nevertheless, the late DDH diagnosis affects the quality of living, raises social costs and facilitates early OA development. The risk factors of early failure of treatment are older age at operation, high AVN grade and bilateral hip involvement. Still, we recommend OR+DO+PFO whenever technically manageable and to not leave the patient with a dislocated hip joint even in teenagers.
Footnotes
Acknowledgements
We thank Dr. Julieanne P. Sees, DO, from Nemours Alfred I. duPont Hospital for Children in Wilmington, USA, for this manuscript's language editing.
We thank Izabela Miechowicz, Ph.D., from Poznan University of Medical Sciences, Poland, for the statistical analysis of data.
MI: Study design, Analysis and interpretation of data, Manuscript preparation.
MJ: Study design, Analysis and interpretation of data, Manuscript preparation.