
Abstract
Abstract
Purpose
Addressing the psychosocial needs of adolescents can improve surgical outcomes. The aim of this retrospective comparative study was to understand the core psychosocial factors that shaped the experiences of adolescents who underwent multiple limb lengthening/reconstruction surgeries (LLRS).
Methods
A novel 62-question survey was developed and administered to 31 patients from the study institution. Data was obtained using a self-report inventory assessing medical care, communication/connection to doctor, peer relations, physical space, self-esteem, counselling/clergy, physical/emotional support, school issues and concerns about future. This survey and demographic questions were administered to young adults (now aged 18 to 30 years) who underwent LLRS treatment between the ages of 11 to 20 years.
Results
Psychosocial needs were determined to be within the categories of body image/self-esteem, subjective perception of treatment, patient-physician relationship, role of parents, peer interactions, academic performance and hospital experience. Patients valued parental involvement while also wanting their surgeon to speak directly to them. They preferred to be in private rooms on the paediatric floor and to not socialize while in the hospital. They were indifferent to keeping up with friends, speaking to a counsellor and having their surgeon inquire about their emotions. They expressed concern about pain, carrying out activities and the financial impact of surgery.
Conclusions
Adolescent LLRS patients value focused psychosocial support from their surgeon and caregivers. This perceived level of support influences their ability to cope with their condition. These findings helped us understand the psychological issues and preferences of adolescents who underwent LLRS and can assist orthopaedic surgeons in providing holistic care.
Level of Evidence
IV
Keywords
Introduction
Adolescence is a critical time period for emotional, cognitive and psychosocial development marking the transition from childhood into adulthood. Psychosocial, a term first introduced and later refined by Erik Erikson (1950, 1968),1,2 describes human development as it pertains to the mind and social relationships. Erikson's theory detailed the conflicts encountered at each of eight stages of development. This study focuses on the adolescent stage, also known as ‘identity versus role confusion’. Adolescents begin to form their identity, gain independence, focus on peer relationships and become aware of body image. 3 Unmet or traumatic health needs during this period may impair neurological development, puberty and future quality of life and may present challenges in transitioning into later developmental stages. Orthopaedic surgery, in particular, may leave adolescents with increased vulnerability both physically and emotionally. Whether they seek a return to sports, correction of deformity or congenital abnormality treatment, adolescents undergoing extensive orthopaedic surgery may experience long-term psychosocial vulnerability. 4
Psychosocial factors are known to be important in healthcare, especially with regard to symptoms, outcomes and patient experience.3,4 However, little is known about the psychosocial issues of children and adolescents in the context of limb lengthening and reconstruction surgery (LLRS). This pilot study sought to uncover the core psychosocial issues and challenges experienced by children and adolescent patients while undergoing orthopaedic treatment in the area of LLRS. The knowledge gained is intended to improve best practices. With a better understanding of the issues and challenges, the healthcare team then may become aware of opportunities for further study and improved healthcare delivery. Experience from this study will help refine and validate the survey for future use. Subsequent phases of the study will address a wider sample of children and adolescent patients in a prospective manner. This knowledge may be relevant, useful and generalizable for medical practitioners across multiple subspecialties. With such insight, the medical community can understand and implement age specific psychosocial considerations more effectively in caring for patients.
The primary goal of this study was to perform a qualitative assessment of the data. The secondary goal was to determine if there were patterns for particular demographic groups such as sex and age of surgery.
Patients and methods
Upon institutional review board approval, a novel survey (Tables 1 and 2) was developed with input from focused discussions and interviews among a paediatric orthopaedic surgeon (PDF), paediatric/adult limb deformity orthopaedic surgeons (ATF, SRR), an orthopaedic psychologist, a child psychologist (BSE), a social worker, several patients, several parents and an epidemiologist. The survey utilized Likert scale responses to questions about medical care, communication/connection to doctor, peer issues, physical space, self-esteem, counselling/clergy, emotional support, school issues and concerns about future.5,6 This survey and other demographic questions were administered retrospectively to study participants.
Likert Scale questions

surgeons’ names removed
Likert Scale responses. Responses’ expressed as number of responses for question with percentage of total responses for that question in parenthesis

Patients were recruited for the study through telephone contact and via email. Inclusion criteria were young adults (now aged 18 to 30 years) who underwent LLRS treatment at the study institution between ages 11 to 20 years and who had undergone more than one lifetime orthopaedic surgery. Details regarding number of surgeries, age at first surgery, current age and sex were collected (Table 3). A total of 38 patients were successfully contacted, consented and enrolled in the study. A total of 31 of these patients completed the survey in its entirety. There were 17 female and 14 male patients. The responses from participants who completed the survey were assessed and grouped into seven broad categories that may characterize the needs of this patient population.
Patient demographic data

Statistical analysis
The Likert scale responses for questions under the ‘peer interaction’ domain were converted to a ‘peer interaction’ Likert scale score. These scores were calculated by assigning numeric values to each question's responses. The numeric values were assigned to responses as follows: ‘very unimportant’ = 0, ‘unimportant’ = 1, ‘neutral’ = 2, ‘important’ = 3 and ‘very important’ = 4. Likert response scores were summed for each ‘peer interaction’ question.
This score was reviewed for potential association with sex and age at surgery using a simple linear regression. For age category analysis, patients with age categories ‘11-12 years old’ and ‘13-14 years old’ were categorized as Group 1 (n = 13). Patients with age categories ‘15-16 years old,’ ’17-18 years old’ and ‘19+ years old’ were categorized as Group 2. Additionally, chi-squared tests or Fisher's exact tests were conducted to ascertain the relationship between sex/age category and individual Likert responses under the ‘peer interaction’ domain.
Association between sex/age category and ‘perception of how complicated the problem and treatment were’ was assessed using the chi-squared test or Fisher's exact test. SAS 9.4 (SAS Institute Inc., Cary, North Carolina) was used for statistical analysis. Only p-values < 0.05 were considered statistically significant.
Results
Overall, trends are reported that appear to be subjectively significant in this patient population. The needs of adolescents undergoing orthopaedic surgery were found to be in the following seven categories.
Body image and self-esteem
Patients were indifferent to the impact of their orthopaedic problem on their body image and self-esteem prior to surgery. They had similar responses when asked about its current impact. Patients were indifferent to having their scars lightened or removed.
Subjective perception of medical condition and treatment plan
Most patients reported that their orthopaedic conditions and subsequent treatment plans were complicated to some degree. They expressed worry about the level of pain they would experience and their ability to carry out activities of daily living such as getting out of bed, showering, and dressing self (Fig. 1). Ultimately, all patients reported the final result of their orthopeadic treatment as positive with 52% of patients (16 of 31) reporting it to be ‘excellent’. The majority of patients were neutral about wanting to speak to a counsellor about what they were experiencing (Fig. 2).

Patients were asked ‘were you worried about the level of pain you would experience with your treatment’ and ‘were you worried about being able to carry out your daily routine after surgery?’. The answer choices were ‘not worried at all’, ‘not worried much’, ‘a little worried’, ‘worried a lot’ and ‘extremely worried’ (n = 31). Numbers over bars indicate the number of patients who chose that specific answer choice for the question.

Patients were asked ‘how important was it that you could speak to a counselor about what you were going through?’. Answer choices were ‘very unimportant’, ‘unimportant’, ‘neutral’, ‘important’ and ‘very important’ (n = 31). Numbers over bars indicate the number of patients who chose that specific answer choice for the question.
Patient-physician relationship
Respondents valued physician transparency regarding information about their surgery. It was found that 87% of patients (27 of 31) responded ‘very important’ when asked if they wanted their doctor to be experienced with their surgery. The majority of respondents found it ‘very important’ to have their questions answered by their surgeon and to have their surgeon speak directly to them instead of to their parents only (Fig. 3). Patients wanted their surgeon to communicate directly with their paediatricians and other physicians involved in their care instead of having to communicate their own medical history. They emphasized being able to reach members of their medical team outside of scheduled appointment times and particularly appreciated being able to contact their surgeon directly. Respondents were less interested in having their surgeon inquire about the emotional and psychological effects of their surgery (Fig. 3).

Patients were asked ‘how important was it that your surgeon had experience with your treatment plan’, ‘how important was it to have your surgeon speak directly to you rather than your parents only’ and ‘how important was it that your surgeon asked you about the emotional and psychological effects of the surgery?’. The answer choices were ‘very unimportant’, ‘unimportant’, ‘neutral’, ‘important’ and ‘very important’ (n = 31). Numbers over bars indicate the number of patients who chose that specific answer choice for the question.
Patients appreciated the availability of information including patient stories and before and after images on their surgeon's website. The majority of patients were interested in following their surgeon on social media. While some patients enjoyed communicating with their medical team via text message, email and phone, most respondents preferred in-person communication.
Role of parents
All responses regarding the role of parents were weighted toward maximizing parent involvement. The majority of patients responded ‘very important’ when asked if they wanted a parent or guardian present for emotional support, to help understand their treatment plan and to ask additional questions (Fig. 4).

Patients were asked ‘how important was it that you had a parent or guardian present for emotional support’, ‘how important was it that you had a parent or guardian present to help you understand your treatment plan’ and ‘how important was it that you had a parent or guardian present to ask additional questions?’. Answer choices included ‘very unimportant’, ‘unimportant’, ‘neutral’, ‘important’ and ‘very important’ (n = 31). Numbers over bars indicate the number of patients who chose that specific answer choice for the question.
All patients responded positively when asked about the level of physical support they had at home after surgery. Patients also responded positively when asked about the level of emotional support they had at home following surgery but to a slightly lesser degree. Patients felt that their surgery and recovery impacted the daily lives of those in their households. In total 84% (26 of 31) responded that their surgery was to some degree a financial burden on their families (Fig. 5). In all, 97% of respondents (30 of 31) are currently comfortable living independently to some degree.

Patients were asked ‘to what extent did you feel that your surgery was a financial burden on your family?’. Answer choices were ‘not at all’, ‘slightly’, ‘moderately’, ‘considerably’ and ‘extremely’ (n = 31). Numbers over bars indicate the number of patients who chose that specific answer choice for the question.
Peer interactions
The majority of patients were indifferent to speaking with peers who underwent or who were undergoing similar treatment. Most patients felt neutral about socializing with other adolescents during their hospital stay and about there being a place for them to spend time outside of their hospital room to do schoolwork (Fig. 6). Most patients did not want a roommate while in the hospital. In total, 81% of patients (25 of 31) responded ‘definitely yes’ when asked if they wanted a private room without a roommate (Fig. 7).

Patients were asked ‘how important was it that you could socialize with other kids your age while you were in the hospital’, ‘how important was it that there be a space in the hospital outside of your room to hang out’ and ‘how important was it that there was a quiet study area where you could do your school work during your stay at the hospital?’. Answer choices were ‘very unimportant’, ‘unimportant’, ‘neutral’, ‘important’ and ‘very important’ (n = 31). Numbers over bars indicate the number of patients who chose that specific answer choice for the question.

Patients were asked ‘did you prefer a private room without a room?’. Answer choices were ‘definitely no’, ‘not so much’, ‘neutral’, ‘yes, a little’ and ‘definitely yes’ (n = 31). Numbers over bars indicate the number of patients who chose that specific answer choice for the question.
Respondents did not feel that their orthopaedic conditions affected their relationship with their peers prior to treatment, and they were able to enjoy being both at home and in school. Keeping up with friends prior to treatment was important to most respondents. Patients were more indifferent to keeping up with friends during their treatment.
Academic performance
The majority of patients wanted their schools to be made aware of their upcoming surgery. They felt indifferent to bringing schoolwork with them so they did not fall behind academically. They also were indifferent to having a designated area to do schoolwork while in the hospital. With regard to university and college choices, most patients were not influenced by their medical conditions (Fig. 8). For those to whom this question applied, respondents did not feel that their orthopaedic conditions limited them in their ability to find work or in future career choices.
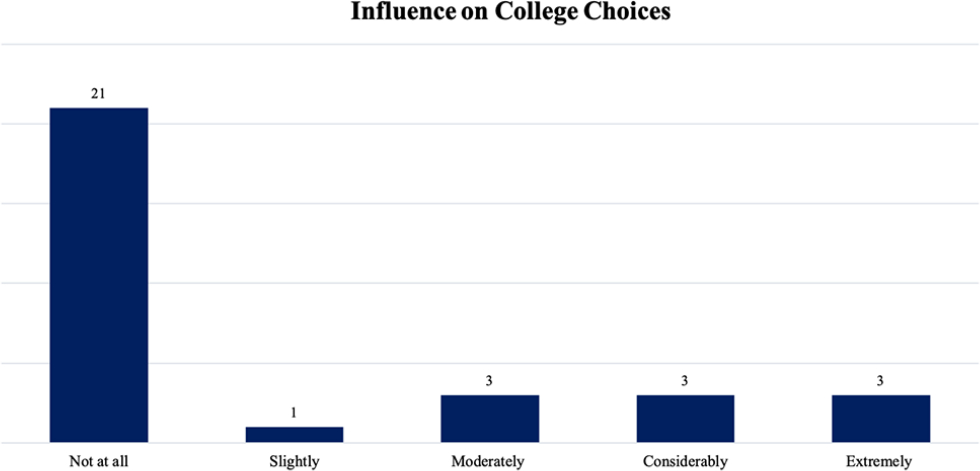
Patients were asked ‘how much did your medical condition affect your college choices?’. Answer choices were ‘not at all’, ‘slightly’, ‘moderately’, ‘considerably’ and ‘extremely’ (n = 31). Numbers over bars indicate the number of patients who chose that specific answer choice for the question.
Hospital/office experience
Respondents were indifferent to having age-appropriate activities be available to them to pass time in the waiting area during office visits. The majority of patients preferred to be admitted to the paediatric floor of the hospital postoperatively (Fig. 9).

Patients were asked ‘did you prefer to be on the pediatric floor of the hospital?’. Answer choices were ‘definitely no’, ‘not so much’, ‘neutral’, ‘yes, a little’ and ‘definitely yes’ (n = 31). Numbers over bars indicate the number of patients who chose that specific answer choice for the question.
Quantitative analysis
Regarding questions about the importance of peer interaction, the mean score of the Likert scale was noted to be lower for male than female patients (6.46 versus 7.06) suggesting that peer interaction is somewhat less important for male patients than it is for female patients, though the association was not significant (p = 0.45). There was no association noted between sex and overall responses (p = 0.72) nor between sex and the perception of how complicated the treatment and medical problems were (p = 0.60)
The mean peer interaction score for patients having surgery between the ages of 11 and 14 years was lower than that for patients having surgery between the ages of 15 and 20 years (6.15 versus 7.23) suggesting that younger patients are less likely to desire peer interaction while undergoing LLRS treatment, though the association was not significant (p = 0.171). No association was found between ‘perception of how complicated the problem and treatment were’ and age group (p = 0.306).
Discussion
Given the vulnerability of this patient population, adolescents require attentive care during all stages of the perioperative period. These findings support the importance of preoperative psychosocial assessment and continuity of emotional support throughout healing and rehabilitation. The most efficacious way for orthopaedic surgeons to improve patients’ physical condition and quality of life is to incorporate a psychosocial-focused approach into their treatment plans.
According to survey responses, concerns about pain, social stressors, disruptions in academic performance and body image arise during early interactions with the orthopaedic surgeon. Patients also worried about the outcome of surgery and potential impact on activities of daily living. Orthopaedic surgeons should establish trust and open communication, allowing patients and their caregivers to feel safe and supported enough to voice these concerns. This can be accomplished by strengthening the surgeon's interpersonal and communication skills and focusing specifically on matters of importance to this age group. According to a study done by Tongue et al, 7 75% of surveyed orthopaedic surgeons felt their communication with patients was satisfactory, while only 21% of orthopaedic patients report satisfactory communication with their surgeon.
Patients expressed desire for their surgeon to be knowledgeable, invested and willing to do all that is necessary to understand fully their health condition. They wanted to be able to reach their surgeon directly and have their surgeon speak to them as opposed to their parents. The majority of patients were interested in interacting with their surgeons on social media. In this age of technology, adolescents obtain information and interact with others using online platforms. Research in this area has considered the impact social media has had on adolescent health, but further exploration into the use of social media as a health intervention is indicated. 8
Adolescents are in a developmental period during which their sense of self and independence are maturing. When this path is complicated by the need to navigate the healthcare system, they are tasked with coming into their own while simultaneously having to increase dependence on their parents.9,10 Based on the responses to the survey, adolescents relied heavily on their parents for physical, emotional and financial support. This dependency may contribute to disruption of normal psychological growth and impede progression into the next stage of development. It would be prudent for orthopaedic surgeons to consider a patient's medical needs against a backdrop of working with families to mediate conflictual behaviours that may emerge. Adolescents need to be educated about how to take control of their care, ask questions and understand their health condition, while parents likely would benefit from being counselled as to how to navigate the teenager's health concerns while fostering autonomy.
Though research has shown that adolescents living with a chronic physical condition tend to be more susceptible to developing psychological problems such as depression, anxiety and post-traumatic stress disorder, no formal screening tool for psychosocial challenges among adolescent patients exists. 4 Further inquiry is needed to develop an age appropriate instrument which can offer a more accurate assessment of the needs of this patient population, thereby leading to more applicable interventions. Meanwhile, orthopaedic surgeons are encouraged to educate patients and families as to the benefits of early detection and intervention. According to a study done by Vranceanu et al, 11 orthopaedic surgeons are likely to recognize psychological factors. However, they tend to refrain from referring their patients for psychological treatment due to time constraints, stigma and discomfort in doing so. This further underscores the necessity of incorporating psychosocial screening of patients as well as physician training in orthopaedic surgery programmes.
Most patients in this study expressed pain as a postoperative concern. Studies have found that overall patient satisfaction is positively associated with lower pain scores and low levels of anxiety throughout treatment. 12 Therefore, careful consideration of pain and proper pain management can lead to better outcomes.
Ability to participate in sports is an especially prominent concern for adolescents. 13 The survey developed for this study did not address specifically patients’ concern about returning to sports, thereby constituting a limitation of the study. In the subsequent prospective investigation, questions relating to participation in athletics, both competitive and recreational, will be included. Other limitations of this study are noted in that it was retrospective with inherent recall bias and that it surveyed a relatively small group of patients. Furthermore, the patient group is homogenous, based on the fact that all are LLRS patients. The small sample size made it difficult to demonstrate differences in the importance of psychosocial issues for various subgroups of patients. This impeded the conduction meaningful statistical analysis.
Future investigation will seek to utilize and expand upon current findings with the goal of establishing a reliable and valid instrument. Modifications of the current survey will be used in a prospective manner with a larger sample size of various paediatric orthopaedic conditions including trauma, sports medicine and spine. Additionally, there will be future plans to include more diverse medical and surgical treatments. Subsequent studies are expected to uncover an enhanced understanding of core psychosocial issues for children and adolescents which may be unique to age, sex, complexity of treatment and socioeconomic background. The information learned from current and future studies is expected to assist the healthcare community to take into account the psychosocial needs of children undergoing protracted medical treatment as they transition through adolescence and on toward adulthood. It is the expectation that such empirical knowledge will lead to a more holistic approach, which in turn will foster improved care and outcomes.
Conclusion
Adolescent LLRS patients value focused psychosocial support from their surgeon and caregivers. This perceived level of support influences their ability to cope with their condition. These findings helped us understand the psychological issues and preferences of adolescents who underwent LLRS and can assist orthopaedic surgeons in providing holistic care.
Footnotes
Author SRR reports grants from I Am Not Done Yet Foundation and personal fees from Nuvasive and Orthospin outside the submitted work.
The other authors declare no conflict of interest relevant to this work.
RM: Organize questionnaire in online survey program, contacted and consented patients, collected and performed analysis of data.
BSE: Conceive and design project, developed survey, performed analysis of data, edit manuscript.
PDF: Conceive and design project, developed survey, performed analysis of data, edit manuscript.
ATF: Conceive and design project, developed survey, performed analysis of data, edit manuscript.
SRR: Conceive and design project, developed survey, performed analysis of data, edit manuscript.