
Abstract
Abstract
Purpose
The EOS-imaging system is increasingly adopted for clinical follow-up in scoliosis with the advantages of simultaneous biplanar imaging of the spine in an erect position. Skeletal maturity assessment using a hand radiograph is an essential adjunct to spinal radiography in scoliosis follow-up. This study aims at testing the feasibility and validity of a newly proposed EOS workflow with sequential spine-hand radiography for skeletal maturity assessment and bracing recommendation.
Methods
EOS spine-hand radiographs from patients with diagnosis of idiopathic scoliosis, including both sexes and an age range of ten to 14 years, were scored using the Thumb Ossification Composite Index (TOCI), Sanders and Risser methods. Intraclass correlation coefficients (ICCs) were calculated for inter/intraobserver agreement and were tested with Cronbach's alpha values.
Results
In all, 60 EOS-spine hand radiographs selected from subjects with diagnosis of adolescent idiopathic scoliosis (AIS), including 32 male patients (mean age 11.53 years; 10 to 14) and 28 female patients (mean age 11.50 years; 10 to 13) who underwent sequential spine-hand low dose EOS imaging were generated for analysis. The overall interobserver (ICC = 0.997) and intraobserver agreement (α > 0.9) demonstrated excellent agreement for TOCI staging; ICC > 0.994 for both TOCI and Sanders staging comparing traditional digital versus EOS hand radiography; ICC ≥ 0.841 for agreement on bracing recommendation among TOCI versus the Risser and Sanders system.
Conclusion
With the proposed new EOS workflow it was feasible to produce high image quality for skeletal maturity assessment with excellent reliability and validity to inform consistent bracing recommendation in AIS. The workflow is applicable for busy daily clinic settings in tertiary scoliosis centres with reduced time cost, improved efficiency and throughput of the radiology department.
Level of evidence
III
Keywords
Introduction
Adolescents with idiopathic scoliosis (AIS) have been regularly subjected to repeated x-ray exposure to the growing spine as part of clinical follow-up; this has raised major concerns of increased cancer risks. 1 The EOS slot-scanning 2D/3D system (EOS Imaging, Paris, France) has gained increasing popularity for the assessment of spinal and lower limb alignment with a much lower radiation dose (50% to 80% lower than conventional radiography) and additional advantages such as true-to-size images and the acquisition of bi-planar simultaneous images that also enable 3D reconstruction. 2
In addition to the spine radiographs, hand radiographs to assess skeletal maturity are essential for important decision-making such as bracing treatment for the clinical follow-up.3,4 The current hand skeletal age assessment methods are mostly derived from the Tanner-Whitehouse III (TW3) 5 method and further simplified staging system, e.g. the simplified Skeletal Maturity Scoring (SSMS) 3 and the recently reported Thumb Ossification Composite Index (TOCI).6,7 Conventionally, these hand radiographs are taken in the sitting position following the TW3 imaging protocol 5 using standard digital radiography, which is taken in a separate x-ray room away from the EOS spinal radiography procedure.
We proposed a new practical imaging workflow with the standard low-dose hand radiography taken sequentially immediately after the spinal radiographs in the same EOS imaging setting (Fig. 1). We hypothesized that the image quality of the low-dose EOS hand radiograph can allow reliable assessment of skeletal maturity in AIS patients to inform valid bracing treatment decisions as compared with the classic Risser 8 and Sanders 9 SSMS systems.
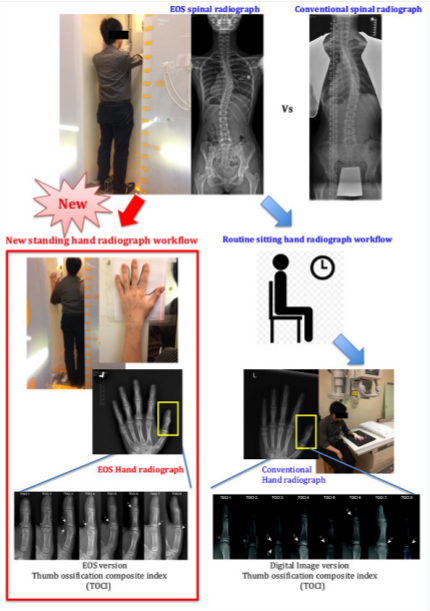
Lefthand image shows the new workflow with the hand radiography taken using the EOS standard low dose followed immediately after the spinal radiographs in the same EOS system. The righthand image shows the conventional workflow with hand radiographs taken using traditional x-ray machines after spinal radiographs are taken with the EOS system.
The objectives of this study were: 1) to test the feasibility of the current new EOS spine-hand radiographs workflow and to determine the inter- and intrareliability of skeletal maturity assessment with the low dose EOS-hand radiograph using the modified TW3 staging of the thumb epiphyses and the TOCI staging system; 2) to conduct a validation testing for EOS hand radiographs versus standard digital hand radiography; 3) to compare TOCI staging based on EOS hand radiograph in brace treatment recommendation versus the Risser and Sanders scoring systems.
Materials and methods
The sequential EOS hand radiographs obtained from patients with clinical diagnosis of AIS were retrospectively reviewed. Inclusion criteria of subjects included: 1) both sexes; 2) age between ten and 14 years at initial visit; 3) clinically and radiologically confirmed diagnosis of idiopathic scoliosis. Ethical approval was obtained from the ethics review board of the Joint New Territories East Cluster/Chinese University of Hong Kong (NTEC/CUHK) Ethics Committee (reference number: 2016.045).
EOS spine and hand imaging protocol
All AIS subjects underwent imaging assessment according to a new EOS protocol during both initial and follow-up visits. The imaging protocol included first a low-dose EOS spine radiograph taken in a posteroanterior standing position, immediately followed by an EOS hand radiograph by the same machine in the same setting. Subjects were asked to place their left hands at a designated region over the surface of the EOS slot-scanning system. An image covering only the hand and wrist was taken at the lowest achievable dose of 18.6 mGycm 2 that can produce an image of acceptable quality (Fig. 1).
The most experienced author (ALHH) first graded all EOS hand radiographs using the TOCI staging system (Fig. 2).6,7 Another investigator (WWC) not involved in this study helped to randomize the radiographs into a full spectrum of TOCI staging from 1 to 8. Four junior non-orthopaedic residents (Dr. Cheuk-Yin Tam, Dr. Kathy Yun-Yee Chan, Dr. Aaron See-Long Hung and Dr. Hebe Wai-Yee Fung) and one orthopaedic resident (LCML) with no prior experience in staging hand skeletal maturity were invited as voluntary novice raters for this study. After a special training session, each rater was requested to grade blindly and independently the thumb ossification pattern for each hand radiograph using the modified TW3 descriptors (Table 1): uncovered (Stage E), covered (Stage F), capped (Stage G), partial fused (Stage H) and fused (Stage I) status for thumb proximal phalanx; stage I or non I for thumb distal phalanx. In addition, the thumb adductor sesamoid bone ossification was also rated as absent (A) or present (O). The TOCI staging was scored at the same setting. The raters then regraded the same set of images four weeks apart to test for intraobserver reliability. The investigator (WWC) collected and tabulated all the inter- and intra-rater scoring and analyzed the results independently.
Conversion table from Tanner Whitehouse III (TW3) descriptors to Thumb Ossification Composite Index (TOCI)
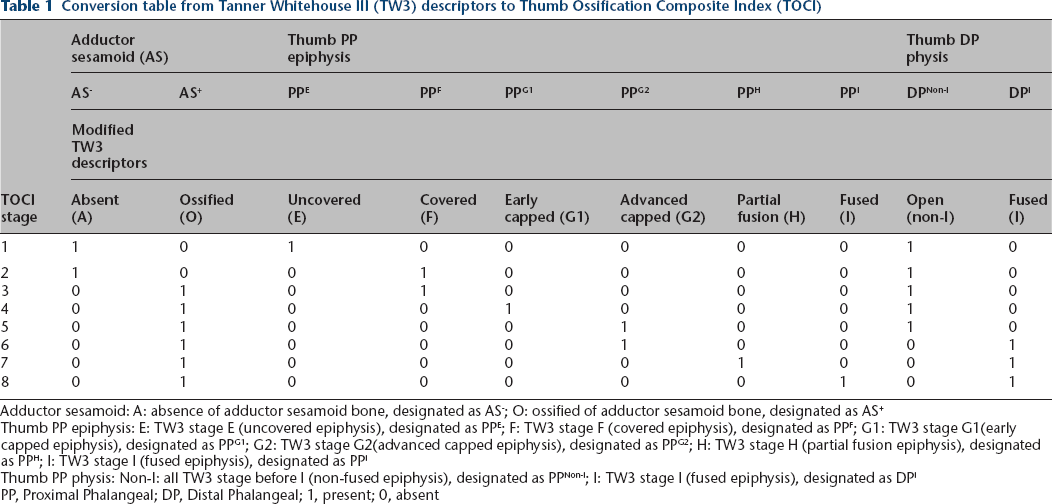
Adductor sesamoid: A: absence of adductor sesamoid bone, designated as AS−; O: ossified of adductor sesamoid bone, designated as AS+
Thumb PP epiphysis: E: TW3 stage E (uncovered epiphysis), designated as PPE; F: TW3 stage F (covered epiphysis), designated as PPF; G1: TW3 stage G1(early capped epiphysis), designated as PPG1; G2: TW3 stage G2(advanced capped epiphysis), designated as PPG2; H: TW3 stage H (partial fusion epiphysis), designated as PPH; I: TW3 stage I (fused epiphysis), designated as PPI
Thumb PP physis: Non-I: all TW3 stage before I (non-fused epiphysis), designated as PPNon-I; I: TW3 stage I (fused epiphysis), designated as DPI
PP, Proximal Phalangeal; DP, Distal Phalangeal; 1, present; 0, absent

EOS version for Thumb Ossification Composite Index (TOCI):
Validity testing for EOS hand radiographs
AIS subjects who were followed up at the scoliosis clinic during the transition period experiencing the usage of both new and original method for hand radiography were identified for this validity testing. During this special transition period, all subjects had their initial hand radiographs taken using the original digital radiographic method at their first consultation visit. Their immediate subsequent follow-up assessment for hand maturity was determined using the newly proposed EOS hand radiography. The two sequential hand radiographs were then assessed with both the TOCI and Sanders SSMS methods and compared. The key assumption in this validity testing was that there was no change in hand maturity during these close follow-up intervals.
Consistency of bracing decision
The current Scoliosis Research Society (SRS) criteria for bracing decision are Cobb angle ≥ 25° with Risser stage less than or equal to stage 2; 10 which is equivalent to Sanders scores of less than or equal to stage 6; and equivalent to TOCI scores less than or equal to stage 7. The bracing recommendation of the new referred AIS subjects were decided separately for Risser, Sanders SSMS and TOCI systems with their results compared.
Statistical analysis
Intraclass correlation coefficients (ICCs) were calculated for interobserver agreement using an absolute agreement, two-way random effect model with 95% confidence interval (95% CI) for reproducibility of the differentiation between TOCI stages and TW3 descriptors. ICC values were interpreted as 0.00 to 0.20 indicating ‘slight agreement’; 0.21 to 0.40 ‘fair agreement’; 0.41 to 0.60 ‘moderate agreement’; 0.61 to 0.80 ‘substantial agreement’; and 0.81 and 1.00 ‘almost perfect agreement’.11,12 Continuous variables were expressed as mean and sd, whereas ordinal and categorical variables as frequencies, ratios or percentages. Internal consistency of individuals was tested by Cronbach's alpha values. Statistical analyses was done with IBM SPSS version 24.0 (Armonk, New York). Statistical significance was taken at p < 0.05.
The decision to start bracing referencing with the three scoring methods was represented by either ‘Yes’ (bracing recommended) or ‘No’ (not required). Inter-scoring system reliability against the bracing decision was calculated using ICC. Both EOS scans and digital radiographs were also scored by the TOCI and Sanders systems with their scoring agreement between EOS and radiograph also carried out by inter-rater reliability using ICC.
Results
Inter- and intra-rater reliability testing
A total of 60 EOS hand radiographs were selected randomly from all newly diagnosed AIS subjects with sequential spine-hand low-dose EOS imaging. These radiographs from 32 male patients (mean age 11.53 years; 10 to 14) and 28 female patients (mean age 11.50 years; 10 to 13) were used for the intra- and inter-rater validation and reliability tests, with a total of 600 modified TW3 and TOCI scores for analysis.
The inter- and intraobserver agreement for each rater with corresponding 95% CIs among trial 1 and 2 are shown in Tables 2 and 3, respectively. The overall agreement was found to be excellent between the novice raters for the different TW3 and TOCI staging.
Intraobserver reliability with trial 1 versus trial 2 analysis (Cronbach alpha, bracket showing 95% confidence interval).
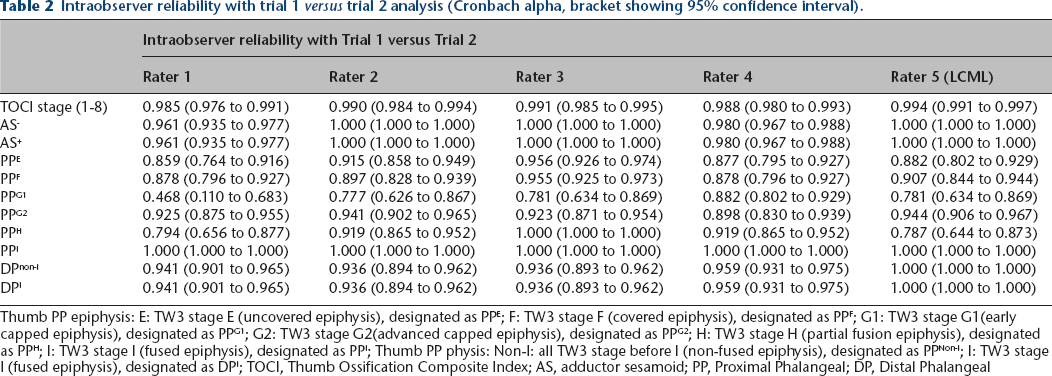
Thumb PP epiphysis: E: TW3 stage E (uncovered epiphysis), designated as PPE; F: TW3 stage F (covered epiphysis), designated as PPF; G1: TW3 stage G1(early capped epiphysis), designated as PPG1; G2: TW3 stage G2(advanced capped epiphysis), designated as PPG2; H: TW3 stage H (partial fusion epiphysis), designated as PPH; I: TW3 stage I (fused epiphysis), designated as PPI; Thumb PP physis: Non-I: all TW3 stage before I (non-fused epiphysis), designated as PPNon-I; I: TW3 stage I (fused epiphysis), designated as DPI; TOCI, Thumb Ossification Composite Index; AS, adductor sesamoid; PP, Proximal Phalangeal; DP, Distal Phalangeal
Inter-observer reliability for trial 1 and trial 2 (brackets showing 95% confidence intervals)
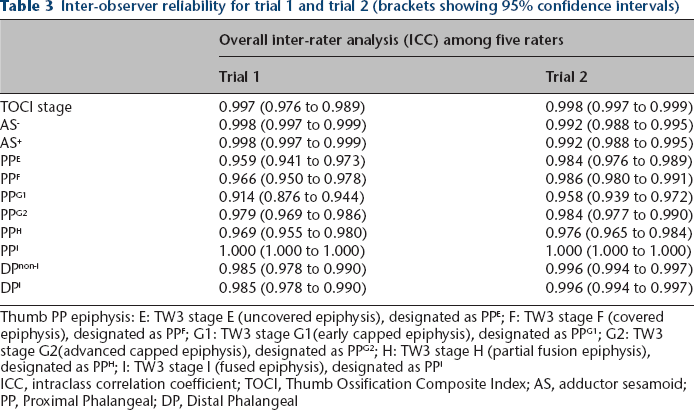
Thumb PP epiphysis: E: TW3 stage E (uncovered epiphysis), designated as PPE; F: TW3 stage F (covered epiphysis), designated as PPF; G1: TW3 stage G1(early capped epiphysis), designated as PPG1; G2: TW3 stage G2(advanced capped epiphysis), designated as PPG2; H: TW3 stage H (partial fusion epiphysis), designated as PPH; I: TW3 stage I (fused epiphysis), designated as PPI
ICC, intraclass correlation coefficient; TOCI, Thumb Ossification Composite Index; AS, adductor sesamoid; PP, Proximal Phalangeal; DP, Distal Phalangeal
Validity testing for EOS hand radiography
A total of 22 AIS subjects with their sequential hand radiographs (first visit digital and immediate follow-up visit as EOS hand radiography) taken at mean 14.8-week intervals (2 to 25) were available for analysis. In all, 20 out of 22 subjects were found to have consistent Sanders SSMS and TOCI scores. The agreement of TOCI scores for EOS and digital radiographs was highly significant (ICC = 0.994; 0.986 to 0.998) and similarly with the Sanders score (ICC = 0.995; 0.988 to 0.998). All comparisons were statistically significant (p < 0.01).
Consistency in bracing decision
All initial EOS spine-hand radiography taken at the first clinic visit from these 60 newly referred AIS subjects was analyzed for bracing decision based on TOCI, Sanders SSMS and Risser systems. The correlation in bracing decision between TOCI and Sanders scoring systems was perfectly agreed (ICC = 1.000), and excellent agreement was observed between the TOCI and Risser systems, as well as between Sanders and Risser systems (ICC = 0.841; 95% CI 0.657 to 0.927).
Discussion
Skeletal maturity assessment is an integral part of the clinical assessment of AIS apart from monitoring of the spinal curve progression. The Risser sign 8 is the most common method for maturity assessment in AIS and had been included for the SRS bracing criteria 10 despite reports on significant interobserver variations. In addition, it is also associated with other major limitations 13 including insensitivity to predict the timing of the crucial peak height velocity, high variability among Risser stages 1 to 4 and low inter- and intra-rater reliability. 14 Recently it has been reported that the Risser stage is also a poor predictor 15 compared with the more accurate SSMS 3 proposed by Sanders, with the chance of having mismatched stages leading to potential incorrect brace treatment decisions. 16 The SSMS system with a thorough assessment of all digital epiphyses in the hand radiograph, which is derived from the most accurate but complex TW3 method, 5 has the best correlation to the crucial curve acceleration phase 9 and prediction of skeletal maturity. 3
The TOCI6,7 validated in this study, also derived from the TW3 method, a simplified version of the SSMS system assessing only to the two thumb digital epiphyses and one adductor sesamoid bone, has been shown to have comparable accuracy and excellent reliability compared with the SSMS system for skeletal maturity prediction. 6 It is shown that TOCI stages have a high concordance rate (up to 71%) to predict similar TW3 stages in remaining ulnar four digital epiphyses 17 and most key pubertal stages among TOCI and SSMS systems are highly correlated and interchangeable 18 as well. This validation study hence opens the door for the EOS system to apply to all skeletal maturity assessment methods involving digital epiphyses grading in the hand.
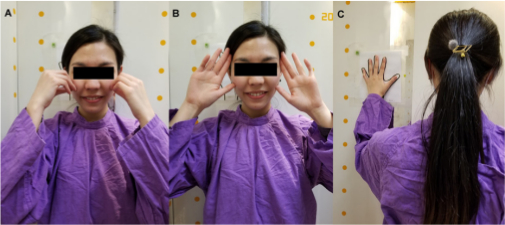
The original EOS scanning protocol of the spine in the anteroposterior position and the recommended ‘hand on cheek posture’ with all digits in flexed position does not allow any detailed morphological assessment of the digital and wrist epiphyses (Fig. 3a). 2 A modified scanning method was subsequently tested at our institution by incorporating the hand in full pronation with all fingers extended when the spine was simultaneously scanned (Fig. 3b). The image quality was found inadequate for accurate assessment of the skeletal maturity due to the inconsistent hand orientation and movement artifact as the hand was not firmly supported on a fixed surface. Another alternative method of positioning the hand near the trunk level on the wall of the EOS scanner with a posteroanterior position of the spine was also far from ideal as part of spinal anatomy was obscured by the hand while the natural standing alignment was also compromised; while placement of patients’ hands with wrist just above the shoulder 19 raised concern about simultaneous exposure to adolescents’ growing brain with unknown harmful effect. After some pilot testing, the current scanning protocol was implemented in our institution (Fig. 3c) by taking the sequential low-dose hand radiograph over a designated stable position immediately following the posteroanterior spinal radiography (scanned up to jaw level without exposing the skull) in the same EOS imaging setting. Our results have demonstrated that the new protocol was able to provide a good quality image that can allow reliable assessment of skeletal maturity in AIS patients with excellent inter- and intraobserver reliability through validation with both the TW3 and the TOCI staging systems.
The validity testing on EOS hand radiographs by comparing the results of conventional digital hand radiography taken on the same day from the same patient was not feasible to conduct in this study. The main concern related to the additional radiation; we found it ethically unjustified to conduct this part of the study after discussion among our local ethics committee, since the high image quality of EOS hand radiography had already attained an excellent reliability result even among novice users. We attempt to address this indirectly through the expanded objectives of including additional validity and reliability testing of a separate cohort of patients with both EOS and traditional digital hand radiography taken within a short mean duration of < 14.8 weeks. The agreement of both the TOCI and Sanders scores for EOS and digital radiograph were excellent with an ICC > 0.994, which was statistically significant (p < 0.01). This implies an expectant result of achieving a nearly perfect agreement if the images were taken within the same day.
The EOS system was originally tailored for spinal and limb alignment assessment.1,2,20–23 To our knowledge, this is the first report on the use of the EOS system for detailed skeletal maturity assessment that relied on precise identification of the three different epiphyseal morphologies of the thumb, with validity testing on its clinical role for bracing recommendation as compared with the Risser and Sanders SSMS systems. The current effective radiation dose used in this validation study was as low as 1.17 uSv without imposing extra radiation risk for the growing children. The main additional advantages of this new EOS workflow are the great reduction in time cost for both patient and radiography staff and increased efficiency and throughput of the radiology department. At our institution, the average time for taking EOS spine and hand radiographs for each patient is seven minutes as compared with 20 minutes for taking EOS spine and separate conventional digital hand radiographs that requires extra time for patient transit and identity checking logistical procedures at different working locations.
Conclusions
The current proposed new sequential spine-hand radiograph with low-dose EOS workflow is feasible and the image quality allows assessment of the skeletal maturity in AIS patients. The reliability and validity based on EOS hand radiographs using TOCI staging for recommending brace treatment was highly comparable with the the Risser sign and Sanders SSMS system. The efficient workflow and reliability can assist the clinician in making effective informed decisions on the prognosis and bracing treatment for AIS in the busy clinic setting. Further validation with larger samples across different centres would be helpful to support wider clinical applicability.
Footnotes
Acknowledgements
The authors wish to acknowledge the following workgroup and members:
The EOS workgroup
Leaders: Mr. Ricky Chan, Miss Melinda Choi
Members: Miss Judy Wong, Mr. Victor Lo, Mr. Derek Leung, Mr. Law Ying Yeung, Miss Carmen Chan, Miss Zora Sze, Miss Athena Lam, Mr. Henry Tse, Mr. Tsang Sze Yeung, Miss Janice Luk, Miss Jasmine Cha
Medical professional for reliability testing and figure production: Dr. Aaron See Long Hung, Dr. Cheuk Yin Tam, Dr. Hebe Wai Yee Fung, Dr. Kathy Yun Yee Chan, Dr. Li Charles
ALHH: Conception or design of the work, Acquisition, analysis, or interpretation of data for the work, Data analysis and/or data interpretation, Drafting of the manuscript, Drafting the work or revising it critically for important intellectual content, Final approval of the version to be published.
WWC: Acquisition, analysis, or interpretation of data for the work, Statistical analysis, Figure/Graph production, Drafting the work or revising it critically for important intellectual content.
ZH: Acquisition, analysis, or interpretation of data for the work, Drafting the work or revising it critically for important intellectual content.
AK: Acquisition, analysis, or interpretation of data for the work, Drafting the work or revising it critically for important intellectual content.
TPL: Drafting of the manuscript, Drafting the work or revising it critically for important intellectual content.
WCWC: Drafting the work or revising it critically for important intellectual content, Final approval of the version to be published.
JCYC: Drafting the work or revising it critically for important intellectual content, Final approval of the version to be published.