
Abstract
Abstract
Purpose
Reports on heterogenous groups of patients have indicated that pedicle screw insertion guided by navigation (PIN) leads to, for the patient, higher doses of radiation compared with pedicle screw insertion guided by fluoroscopy (PIF). This would be a major concern, especially in paediatric deformity correction.
Methods
After a power analysis (aiming at > 0.8) 293 pedicle screws which were inserted in patients with adolescent idiopathic scoliosis were analyzed by comparing effective dose and fluoroscopy time per screw for three different techniques. Groups 2 and 3 were matched to Group 1 by Lenke type of scoliosis. Group 1 were prospectively enrolled consecutive patients that have been operated on by PIN with image acquisition by preoperative CT scan (CTS). Group 2 were consecutive retrospectively matched patients who have been operated on by PIN with image acquisition by an intraoperative 3D scan (3DS). Group 3 were consecutive retrospectively matched patients who have been operated on by PIF.
Results
Mean dose of radiation per screw was 1.0 mSv (sd 0.8) per screw in CTS patients, 0.025 mSv (sd 0.001) per screw in 3DS patients and 0.781 mSv (sd 0.12) per screw in PIF patients. The difference was significant (p < 0.0001).
Conclusion
When we compared different techniques of navigation, navigation by image acquisition with CTS showed a significantly higher (by 97.5%) dose of radiation per screw for the patient than navigation by image acquisition by a 3DS. Navigation by 3DS showed significantly lower effective dose per screw for the adolescent patients than the fluoroscopic technique.
Level of Evidence
II
Keywords
Introduction
Pedicle screw insertion guided by navigation (PIN) has been reported to be superior to pedicle screw insertion guided by fluoroscopy (PIF) with regard to accuracy of pedicle screw insertion. Especially in thoracic vertebrae, where the accuracy of PIN is reported to be up to five times higher than that of PIF.1–5 Additionally, PIN has been reported to significantly reduce exposure of the surgical team to radiation,6–8 which is highly relevant, especially for high-volume deformity surgeons.
On the other hand, there are reports of higher overall doses, for the patient, of radiation with PIN versus PIF7,9–12 which is a major concern especially in the surgery of paediatric deformities. Doody et al 13 reported that the incidence of breast cancer correlates with dose of radiation and is significantly higher in scoliosis patients than in the normal population.
However, the former reports which state higher doses of radiation in PIN compared with PIF7,9–12 investigated mainly short segment fusions and enrolled patients with heterogenous indications for surgery, heterogenous surgical levels and heterogenous techniques including minimally invasive surgery (MIS) and standard open surgery, with and without interbody spacers. To the best of our knowledge, there is no data available comparing the dose of radiation of PIN versus PIF in instrumented posterior fusion of spinal deformities.
PIN can be performed by different techniques of image acquisition, among them intraoperative 3D scan (3DS) and preoperative CT scan (CTS). We do not know which technique allows for lower exposure to radiation; former investigations recorded radiation exposure in non-comparable units (mGy, mGy*cm, cGy*cm2, mSv/pt, nSv/pt and others) and compared heterogenous groups of patients 11 which did not lead to sufficient data to compare dose of radiation after 3DS with that of CTS. Furthermore, there are no reports that compare these different techniques of image acquisition for navigation with regard to dose of radiation in surgery of spinal deformities. The complexity of the calculation of dose of radiation to compare 3DS and CTS may be one reason why there are no reports on this comparison:
For CTS the dose of radiation that results from the CTS has to be added to the dose of radiation that results from intraoperative fluoroscopic images by C-arm which are performed to control the position of the inserted screws and the result of the deformity correction. This addition is a complex calculation since radiation exposure of CT scans is recorded as dose-length-product (DLP, mGy*cm) and radiation exposure of fluoroscopy is recorded as dose-area-product (DAP, cGy*cm2).
For 3DS the DAP that results from the 3DS has to be added to the DAP that results from intraoperative fluoroscopic images by C-arm which are performed to control the position of the inserted screws and the result of the deformity correction.
Since the parameters DAP and DLP cannot be compared (cGy*cm2 versus mGy*cm), they both have to be converted to the effective dose in mSv to allow for comparison of dose of radiation of 3DS with dose of radiation of CTS.
Radiation exposure and conversion factors from DAP or DLP to effective dose are hardware- and body mass index (BMI)-dependent. Therefore, conversion factors have to be adapted to the exposed region (thoracic or lumbar spine), as other investigators have described.14,15
There is no report that compares the overall dose of radiation (intra- and preoperative) for the patient by navigation with image acquisition by CTS to the dose of radiation of navigation by image acquisition with a 3DS in spinal deformity surgery.
In this study, we investigated which technique of navigation (image acquisition by CTS or image acquisition by 3DS) exposes adolescent patients undergoing surgical correction of idiopathic scoliosis to higher doses of radiation during the insertion of pedicle screws. Furthermore, we tested the hypothesis that PIN leads to lower doses of radiation for the patient than PIF in patients with idiopathic scoliosis.
Patients and methods
We conducted matched pair analysis of consecutive patients. Sample size was determined by a prior power analysis based on a former investigation; 6 293 screws were analyzed.
Group A: Prospective data collection
We prospectively collected data of ten consecutive patients with adolescent idiopathic scoliosis (AIS) that were operated on in a 12-month period by posterior stabilization with a pedicle screw rod construct and PIN with image acquisition by CTS of the relevant spinal segments (group A). Lenke type of scoliosis, 16 number of screws implanted, level of implantation of screw and time of operation were recorded.
Groups B and C: Retrospective data collection
We retrospectively included ten consecutive matched patients who were operated on by PIN with image acquisition by 3DS (group B) and ten consecutive matched patients who were operated on by PIF (intraoperative fluoroscopy without navigation) (group C).
Matching procedure
After inclusion of the ten prospective CTS patients (group A), we identified all patients with AIS that were operated on by posterior stabilization with a pedicle screw rod construct in our institution by diagnostic code. Matching patients were allocated, backwards in order of date of surgery, to CTS patients. The first CTS patient that was operated on was matched with the latest patients (one 3DS and one PIF) of the retrospective database that showed identical Lenke type of scoliosis and fused segments. The matching process was conducted accordingly for the remaining nine CTS patients. Patients with incomplete sets of data, previous spinal surgery, BMI > 25 and spinal anomalies were excluded.
All patients operated on by CTS and 3DS were operated on by the first author (MRK), whilst the patients operated on by PIF were operated on by three different surgeons. All surgeons had at least eight years of experience in surgical correction of spinal deformity.
Imaging and technique of pedicle screw insertion: Pre-operative CT (group A)
Preoperative CT scans were acquired with a Somatom Definition Flash CT-scanner (Siemens Healthineers, Forchheim, Germany). The scan range included the thoracic and lumbar spine. Scans were performed at a tube potential of either 100 kVp or 120 kVp.
Imaging and technique of pedicle screw insertion: Navigation (group A and B)
For CTS and 3DS the same C-arm (Arcadis; Siemens Healthineers, Forchheim, Germany) was used in all cases for intraoperative fluoroscopy, which was exclusively applied to control the position of the pedicle screws and the correction of the deformity in CTS patients and additionally for 3D scan in 3DS patients.
The Navigation System ‘Kick’ (Brainlab, Munich, Germany) was applied in CTS and 3DS. Reference clamp for spinous process was applied and attached to the segment which was instrumented. Preparation of pedicle and insertion of pedicle screws was performed with navigation. In 3DS the operative team left the operating room during fluoroscopy acquisitions.
Imaging and technique of pedicle screw insertion: Fluoroscopy (group C)
For PIF a different C-arm (a flat panel detector, Exposcop 8000; Ziehm Imaging, Nürnberg, Germany) was used. Fluoroscopy was exclusively applied for insertion of the pedicle screws and to control the correction of the deformity. Hence, the operative team did not leave the operating room during these fluoroscopic acquisitions. The pedicle screws were inserted similarly to the technique described by Kim et al. 17 Entry points were exposed and identified, then a cortical breach of approximately 5 mm depth was created. Subsequently, a slightly curved gear shift was used to probe the pedicle. It was pointed laterally at first. When the posterior border of the vertebral body should have been reached, according to the inserted length of the probe, it was taken out, the pedicle was palpated to exclude a soft-tissue breach, and reinserted pointing medially. An anteroposterior fluoroscopic control was then made to ensure correct positioning of the probe before it was inserted into the vertebral body. Following this, the entire created canal was palpated to exclude a soft-tissue breach. After screw insertion fluoroscopic control was performed in two planes (anteroposterior and lateral), three to four segments at the same time were checked.
Instrumentation: Navigation (groups A and B)
The 3DS and CTS patients were operated on using the same technique. Caudally three to four segments were instrumented by pedicle screws, and the upper instrumented vertebra (UIV) and the vertebra below the UIP (UIV + 1) were instrumented by pedicle hooks. The other vertebra were instrumented by (lamina -) tapes.
Instrumentation: Fluoroscopy (group C)
In PIF patients pedicle screws were used in all instrumented vertebra.
Monitoring of the dose of exposure to radiation and calculation of the effective dose
The doses of exposure to radiation were recorded automatically by the different devices (CT scanner or flat panel detectors) and were monitored for all patients.
For group A, the dose of exposure to radiation was recorded by adding the dose of exposure to radiation of the preoperative CT to that of the intraoperative fluoroscopy. The dose of exposure to radiation of group A was compared with the dose of exposure to radiation of groups B and C.
For this purpose, the overall dose of radiation (addition of pre- and intraoperative dose of radiation) that patients operated on by navigation were exposed to was converted to the effective dose (mSv).
3DS
No direct conversion factor was available for the system used in our study (Arcadis). In spite of similarities in the hardware, a direct application of the conversion factors used by Suzuki et al 14 was not possible, since the tube potential for their phantom acquisitions was considerably lower (72 kVp to 79 kVp, depending on phantom size). For each patient's image acquisition, the effective dose was calculated by multiplication of the examination's DAP with the thus determined BMI-specific conversion factor. The conversion factors are 0.19 mSv/Gy·cm2 for the thoracic spine and 0.21 mSv/Gy·cm2 for the lumbar spine.
PIF
Effective dose was calculated in the same technique as for 3DS.
Since a different C-arm (Exposcop 8000) (which might have led to different doses of radiation for comparable images) was used for PIF patients, we additionally compared time of fluoroscopy of these patients with time of fluoroscopy of 3DS patients to enhance the validity of the results.
CTS
For CT examinations, the International Commission on Radiological Protection (ICRP)103 conversion factors from DLP to effective dose for scans of thoracic and lumbar spine were taken from the recent publication by Huda et al. 18 The conversion factors are 0.0204 mSv/mGy·cm for the thoracic spine (chest region) and 0.0163 mSv/mGy·cm for the lumbar spine (abdominal region).
Effective dose of 3DS and CTS matched patients was compared.
Statistical analysis
In a matched pair analysis, we investigated if PIN (3DS) was different in CTS, 3DS and PIF with regard to overall dose of exposure to radiation (for the patient). Since dose and time of exposure to radiation did not show normal distribution in a Kolmogorow-Smirnow test, we performed Mann-Whitney U Tests. We first determined which technique of navigation (3DS or CTS) led to the lowest dose of exposure to radiation per screw and then compared this technique with PIF.
Power analysis was performed by G-Power (Heinrich Heine University, Institute for industrial and cognitive psychology, Düsseldorf, Germany)19,20 based on results of former reports. 6 To achieve a high statistical power (> 0.8) at least 80 screws per group were needed.
Since cancer induction and radiation induced hereditary effects are stochastic effects, there is no ‘minimal clinically important difference’; we, therefore, reported the statistical power of our tests.
Statistical analysis was performed by SPSS 25 (IBM, Armonk, New York). Descriptive data are reported as mean and sem.
Results
Patient cohort
The mean age of the CTS patients was 15.9 years (sem 0.9) (group A); 16.0 years (sem 1.6) for 3DS patients (group B); and 15.6 years (sem 0.8) for PIF patients (group C).
Lenke type was 1A in three pairs, 1B in three pairs, 1C in one pair, 2A in one pair, 2B in one pair and 5C in one pair.
In CTS patients, 81 screws were inserted (8.1 screws per patient), 81 screws in 3DS patients (8.1 screws per patient) and 131 in PIF patients (13.1 screws per patient).
Dose of exposure to radiation
Mean dose of exposure to radiation per screw was 1.0 mSv (sem 0.8) per screw in CTS patients; 0.025 mSv (sem 0.001) per screw in 3DS patients; and 0.78.1 mSv (sem 0.12) per screw in PIF patients (Fig. 1).
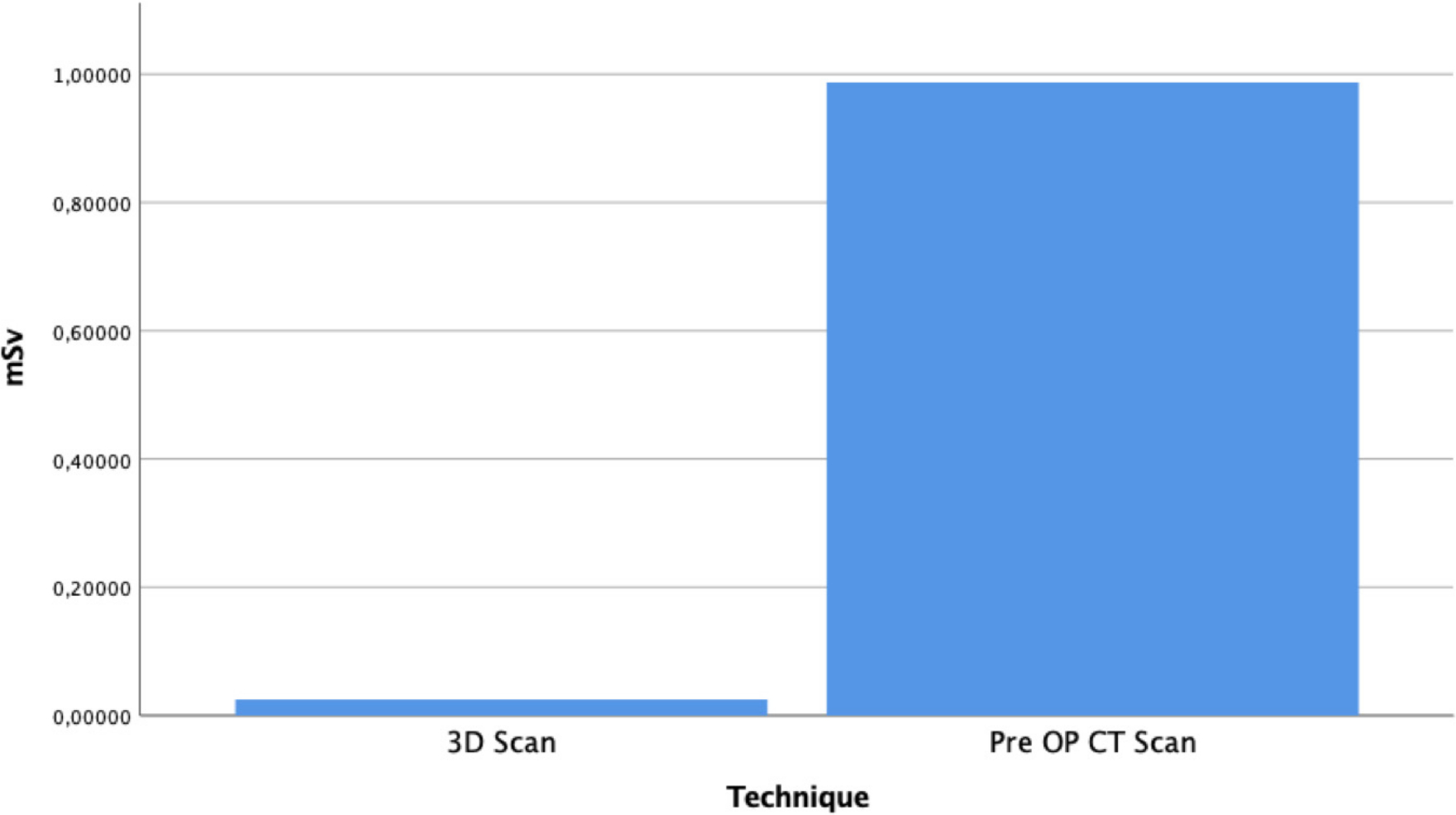
Effective dose of radiation of pedicle screw insertion guided by navigation. Image acquisition by intraoperative 3D scan versus image acquisition by preoperative CT scan.
The difference between CTS and 3DS was significant (p < 0.0001) with a high statistical power (0.95).
The difference between 3DS and PIF was significant (p < 0.001) with a high statistical power (0.80).
Fluoroscopy time
Mean fluoroscopy time per screw was 15.0 seconds (sem 0.8) in all patients; 13.5 seconds (sem 0.3) per screw in 3DS patients; and 24.1 seconds (sem 1.4) per screw in PIF patients (Fig. 2).
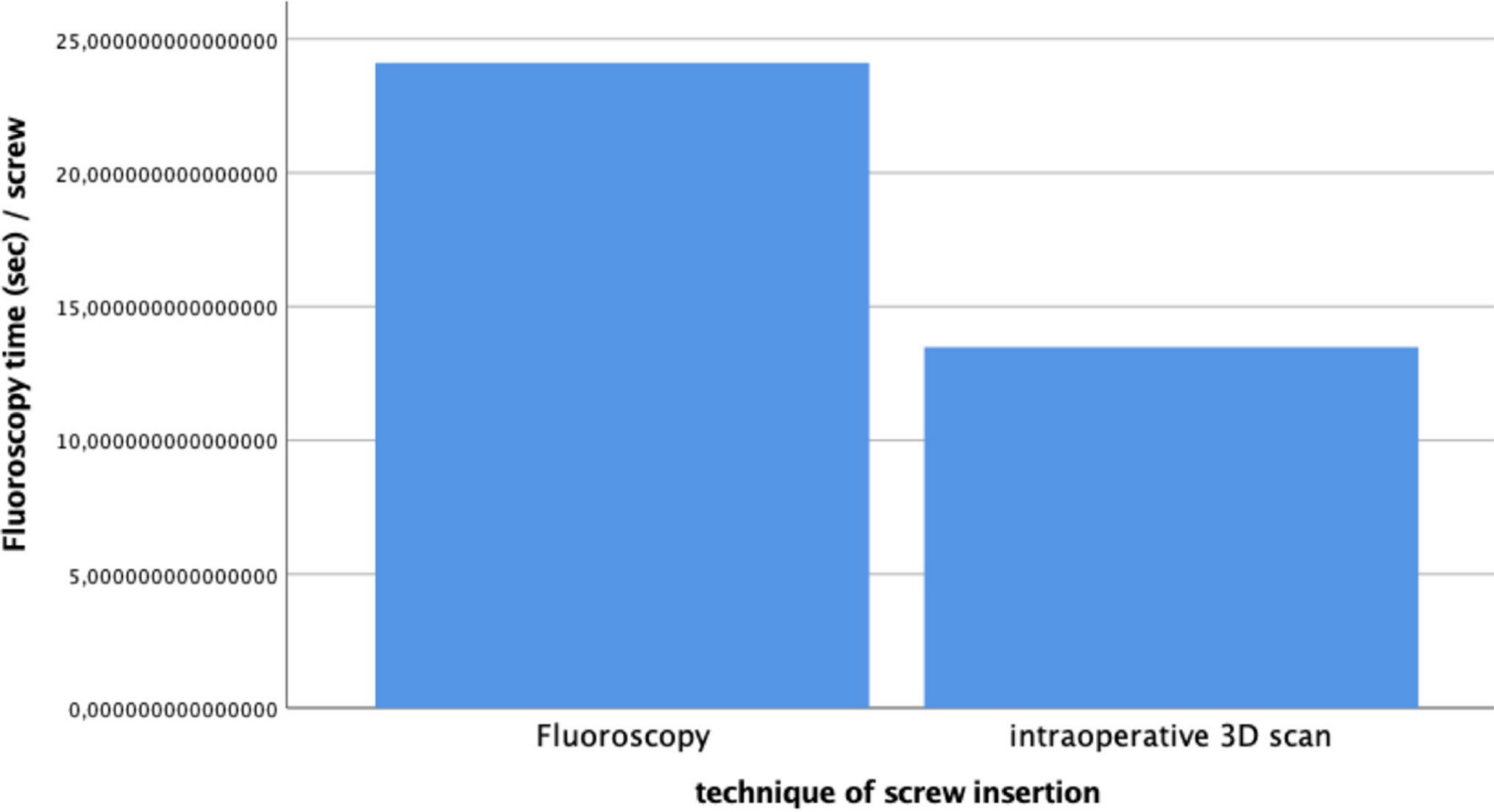
Effective dose of radiation of pedicle screw insertion guided by fluoroscopy versus pedicle screw insertion guided by navigation and image acquisition by intraoperative 3D scan.
The difference between 3DS and PIF was significant (p < 0.0001) with a high statistical power (0.80).
Complications
In the PIF group three malpositioned screws had to be revised within one week of surgery, two due to neurological deficits and one due to radicular pain. No other complications and no anomalies in the neuromonitoring occurred in all other patients of the three groups.
Discussion
Doody et al 13 showed that cumulative effective dose of standard radiographs, performed for diagnosis and follow-up of scoliosis, correlates with incidence of breast cancer in scoliosis patients. Since PIF and PIN lead to relevant and possible cancer inducing effective doses,6,21 we should not only focus on the reduction of effective dose by optimizing technique and frequency of standard radiographs for diagnosis and follow-up of scoliosis, but on procedure-related effective dose too. We conducted this investigation to analyze which technique, PIF, 3DS or CTS, leads to the lowest effective dose for the patient. An alternative to PIF (the fluoroscopic technique) is the free hand technique, where the pedicles are felt by probes and ball-tipped guides without radiographic control. Radiation is only applied after the instrumentation to control the screw positions. Usually several levels are controlled simultaneously. This technique leads to a lower effective dose for the patient and for the surgical team than the fluoroscopic technique and also a lower effective dose for the patient than the navigated technique and, if the surgical team leaves the room for the control radiographs, the same reduction of effective dose for the surgical team.
However, Vaccaro et al 1 reported a breaching rate of 40% in the free hand technique. Insertion of PIF shows a breaching rate of 2% to 30% and insertion of PIN shows a breaching rate of 2% to 15%.2–6 A breaching rate of 0% cannot be achieved by either technique.
Experienced and skilled surgeons might have a lower breaching rate in the free hand technique than less experienced surgeons in the navigated technique. However, statistically, according to available data, the navigated technique shows the lowest breaching rate.
Whether a lower breaching rate justifies a higher procedure-related effective dose cannot be determined. In our opinion it cannot be decided if a higher risk of postoperative pain, neurological deficits and possible revision surgery is ‘outweighed’ by the stochastical risk for cancer by a higher effective dose or vice versa. However, if PIF or PIN are applied, reduction of the procedure-related effective dose as much as possible is essential.
This investigation showed the lowest effective dose in 3DS. CTS showed a higher effective dose than 3DS and PIF.
There was a reduction of dose of exposure to radiation and fluoroscopy time by 56% (13.5 seconds navigation by 3DS versus 24.1 seconds without navigation) when navigation by 3DS was applied compared with the fluoroscopic technique.
There are reports of higher overall doses of radiation by PIN versus PIF7,9–11 in heterogeneous groups of patients. However, in a previous investigation, 6 we could show that in patients without deformity operated on using a MIS technique without interbody fusion, dose of exposure to radiation of patients was reduced by 41% and for surgeons by 81%.
This result can further be explained by the more difficult insertion of pedicle screws in deformed vertebrae compared with vertebrae without deformity. A former report states that rate of screw accuracy is significantly higher in PIN than in PIF in scoliosis surgery. 22 Depicting a pedicle in the correct plane by fluoroscopy is more challenging in patients with deformity than in patients without deformity and may take more fluoroscopy time.
This part of the study, the comparison of PIF with 3DS, has several possible biases. A different C-arm was used in the retrospective group of PIF patients, thus the comparison of dose of radiation of PIF with 3DS is of lower validity. Less modern image intensifiers might produce images of lesser quality which necessitates more than one image to clarify the position of the implant. However, the fluoroscopy time of 13.5 seconds per screw in 3DS patients versus 24.1 seconds per screw in PIF patients seems to indicate that the 3DS technique needed less radiation than the PIF technique.
Furthermore, the PIF patients were operated on by three different surgeons. This might have led to a bias. However, all three surgeons were experienced (at least eight years of experience in deformity surgery) and applied the same technique of pedicle screw insertion in the same institution. Additionally, in PIF all segments were instrumented by pedicle screws, whereas in 3DS and CTS, to reduce effective dose, hooks and tapes were applied for cranial segments, i.e. only one or two 3D scans had to be performed (3DS) or not all segments had to be included in the CTS. This is a possible bias since more challenging pedicles might have been instrumented in PIF than in 3DS and CTS. However, effective dose per screw in 3DS and CTS is the same for all types of pedicles since image acquisition does not dependent on form and shape of the instrumented pedicle, and thus this bias may not be crucial.
These possible biases may render the results of the comparison between the effective dose of PIF with 3DS less valid than the results of the comparison between 3DS and CTS, even if the analysis achieved a high statistical power. In spinal segments with a lower degree of deformity the difference in effective dose between PIF and 3DS might be lower than in spinal segments with a higher degree of deformity. However, the mean effective dose of all spinal segments of PIF was significantly higher than the mean effective dose in 3DS (which is not dependent on degree of deformity), with a high statistical power.
We also compared navigation by CTS with navigation by 3DS. Hecht et al 3 showed that there is no significant difference in accuracy of pedicle screw placement between CT-based navigation and 3D scan-based navigation, which is why we did not analyze accuracy of screw placement. CTS led to a 97.5% higher dose of exposure to radiation (1.0 mSv per screw in CTS versus 0.025 mSv per screw in 3DS) than 3DS. This might be due to the larger field of view in a CT scan compared with a 3DS and to the higher resolution of the CT scan compared with a 3DS. The 3D scan can be performed with a lower resolution than the CTS because the registration of the intraoperative images can be performed automatically (a reference clamp is placed before the 3D scan; after the scan the reference is already registered in relation to the images). The CTSs have to be registered intraoperatively by a matching process that requires a higher resolution.
The substantial advantage of CTS is that the CTS allows for meticulous preoperative planning, which is known to reduce the rate of wrong level surgery. 23 However, the results of this study suggest that a CTS before a surgical correction of a pediatric deformity should not be performed, especially since Miglioretti et al 21 showed that an effective dose of > 20 mSv was delivered in 6% to 14% of all spine CTs and that 270 to 800 spine CTs lead to one case of solid cancer.
For 3DS and CTS, the entirety of the operative team was not exposed to radiation since they could leave the operating room during fluoroscopic acquisitions. This seems even more valuable in the light of the report of Rampersaud et al 24 which states that spine surgeons are exposed to up to 12-fold higher dose rates of radiation than other non-spinal musculoskeletal surgeons.
With the fluoroscopic technique the surgical team could, theoretically, also leave the room for each fluoroscopic control, but it would be more often than in the 3DS technique. The plane of the fluoroscopic control often needs to be adjusted, in both planes, to gain acceptable visibility of the pedicle, so the surgeon may need to reenter the room more than once to guide the adjustment. This procedure (leaving and reentering the room) takes time and disturbs the flow of the surgery.
If the surgical team stayed in the room and stepped behind a lead panel, the surgical team must, according to the federal office for radiation protection, still wear lead due to scattered radiation, although eyes and hands would still be unprotected. Even if the resulting procedure-related effective dose to the surgical team would be very low, it would not be 0. The surgeon and the other members of the surgical team might choose to take this risk of exposing themselves to a minimal amount of scattered radiation.
Conclusion
When we compared different techniques of navigation, navigation by image acquisition with CTS of the levels to be instrumented showed a significantly higher (by 97.5%) dose of radiation per screw for the patient than navigation by image acquisition by a 3DS. Navigation by 3DS in posterior instrumented fusion of idiopathic scoliosis showed a significantly lower dose of radiation and fluoroscopy time (by > 50%) per screw for the adolescent patients than the fluoroscopic technique.
Footnotes
RK reports personal fees from Corin, Nuvasive and Medacta, outside the submitted work.
The other authors declare no conflict of interest relevant to this work.
JB: Conception and design, Data analysis and interpretation, Manuscript writing, Final approval of manuscript.
AS: Manuscript writing, Final approval of manuscript.
CS: Conception and design, Administrative support, Provision of study materials or patients, Manuscript writing, Final approval of manuscript.
MP: Provision of study materials or patients, Collection and assembly of data, Manuscript writing, Final approval of manuscript.
RK: Administrative support, Provision of study materials or patients, Manuscript writing, Final approval of manuscript.