
Abstract
Abstract
Purpose
Radiation-induced cancers due to imaging devices concern above all the growing child, however, to date, intraoperative irradiation doses are not well-documented in children. The goal of the study was to evaluate the intraoperative doses received by patients operated with the use of a C-arm in traumatology, as well as the lifetime attributable risk of cancer death (LAR) related to the irradiation of the imaging device.
Methods
From 1 April 2017 to 31 March 2019, we started a multicentre study and prospectively recruited all consecutive children who needed elastic stable intramedullary nailing (ESIN) for long-bone fracture. We collected demographic and operative data, with dose reports including duration and doses. The main outcome was the effective dose (ED) in millisievert (mSv), calculated with PCXMC software, and the secondary outcome was the LAR expressed as a percentage.
Results
In all, 51 patients operated on using 2D C-arm imaging were included in this study. The mean ED was 0.085 mSv (sd 0.10; 0.002 to 0.649). Overall LAR was 6.5 x 10−4% (sd 6.7 x 10−4%; 0.1 x 10−4% to 28.3x10−4%). Univariate linear regression showed a significant association between ED and irradiation time (p < 0.001). There was no significant association between ED and other outcomes (p > 0.05).
Conclusion
Treatment of long-bone fractures by ESIN found a low level of effective doses with utilization of the C-arm device in current practice. Further studies on a larger sample are needed to confirm these results.
Level of Evidence
II
Introduction
In orthopaedics and traumatology, the surgeon routinely uses imaging devices such as the 2D C-arm in the operating room in order to guide the surgery. 1 Radiation-induced cancer risk is still a cause for concern for growing children, because they have higher sensitivity to radiation and longer life expectancy. This makes them more likely to develop radiation-induced cancer later in their lifetime.2–4 Several studies reported an increasing risk with diagnostic and therapeutic imaging, 3 especially of the thyroid, 5 breast, 6 brain 7 and skin 8 cancers, as well as leukaemia. 9 Therefore, optimizing radiation exposure from imaging devices is crucial for the growing child.
In recent decades, imaging device evolutions have tended to a decrease of the radiation dose. Efforts are given in current practice to limit the exposure of the children. Surgeons are aware of the fact that the dose is proportional to the number of times we press on the C-arm's pedal to get a new imaging acquisition. 1 However, the literature regarding intraoperative irradiation is relatively scarce, so the radiation doses related to imaging devices are not well-known in clinical practice, especially for long-bone fracture surgery.
Ionizing radiations have two main effects: deterministic and stochastic. Deterministic effects are due to high level of radiation, according to a threshold principle, doses > 100 millisievert (mSv). In this condition, the tissue damage is immediate; 10 a similar dose was received by liquidators after the Chernobyl accident in 1986. 11 This represents almost 23-times the mean natural irradiation of 4.3 mSv experienced by the Swiss population each year. 12 However, stochastic effects might occur with low-level doses (< 100 mSv) without the existence of a threshold following a dose-effect linear relationship. These effects are responsible for cancer generation, through a cumulative process of DNA damages, although this is not currently well understood. 2 Because radiation doses related to medical imaging devices are low, they fall beneath our attention. The effective dose (ED) represents the stochastic effect of ionizing radiations. Calculation of the radiation doses can be performed by PCXMC 2.0 (STUK, Helsinki, Finland), which is a software using a Monte Carlo simulation to obtain the ED in mSv, depending on organ sensitivity and their distance to the centre of the irradiation field. 13 This software is currently recognized for its reliability over numerous years. 14
Regarding surgical treatment of long-bone fractures, elastic stable intramedullary nailing (ESIN) is a well-known and adapted method for children. This includes forearm fractures, as well some femur, tibia and humerus fractures. 15
The aim of this observational study was to evaluate the intraoperative EDs received by the patients operated on with the use of a C-arm in our current practice in trauma, as well as the lifetime attributable risk (LAR) of cancer death caused by the radiation exposure from the imaging device during ESIN of long-bone fractures. LAR represents the risk of death by cancer after radiation exposure: a fatal cancer risk of almost 5% per mSv is related to medical imaging. 16 In addition, the hypothesis was to have lower ED and LAR with younger age, with lower body mass index (BMI) and with surgeon level.
Patients and methods
From 1 April 2017 to 31 March 2019, we prospectively recruited in two University Hospitals (Geneva and Brussels) all consecutive children who sustained an appendicular fracture treated by ESIN and required an imaging device exposition. All the patients with a fracture of a long bone on an extremity (arm, forearm, clavicle, thigh and leg) were included. All patients were operated on according to the original technique, 17 with standard radiological protection measures, such as wearing a shield and a lead apron for patients and surgeons.
The research protocol was approved by the Ethic Commissions of the Geneva canton (protocol number: 2016-01338) and of Brussels. Information letters for parents and children were given. All the parents and children older than ten-years-old signed an additional written consent form for this study before inclusion.
The inclusion criteria were: patients < 18-years-old, who needed ESIN surgery and were exposed to a 2D C-arm during surgery. The exclusion criteria were: patients older than 18-yearz-old, who required a surgery without the use of an imaging device, lack of information for the calculation of the ED and absence or refusal from the parents of informed consent.
Demographic data such as sex, age and the operated limb were collected. We also collected operative data such as operative time in minutes; surgeon level (junior or senior, a junior surgeon was defined as a resident or a registrar); and imaging information, considering above all dose reports including duration in seconds and dose-area product (DAP), the absorbed dose multiplied by the area irradiated, and expressed in milligray multiplied by cm2 (mGy.cm2). At our institutions, juniors always performed surgery under the supervision of a senior surgeon, always present during the whole procedure. The complications and the radiological expected results were also recorded. The radiological results were considered as expected when the alignment, with a 5° accepted deviation, and the reduction of the fracture, were obtained.
The PCXMC software needs to enter data such as the age of the patient (Fig. 1). Through the choices of ‘newborn, 1, 2, 5, 10, 15 and adult’ ages, 14 we considered the closest age category for each patient. The irradiation field was defined as the mean length and width in cm × cm of the most irradiated region. For comparative purposes, standard settings proposed in the software were used as follows: the focus to skin distance (FSD) was defined as 80 cm for all patients, with a filtration of 2.5 mm of aluminium (Al) and a voltage of 80 kV. The central point of irradiation was manually adapted on the mathematical phantom of the software, and the data were recorded. Then, the Monte Carlo simulation was performed using energy of 150 keV with a number of 20 000 electrons, according to standard settings of the software. Then, the DAP was entered in the software for calculation of the ED. Finally, the LAR was estimated using age, sex and ethnic origin of the patient and the ED result.
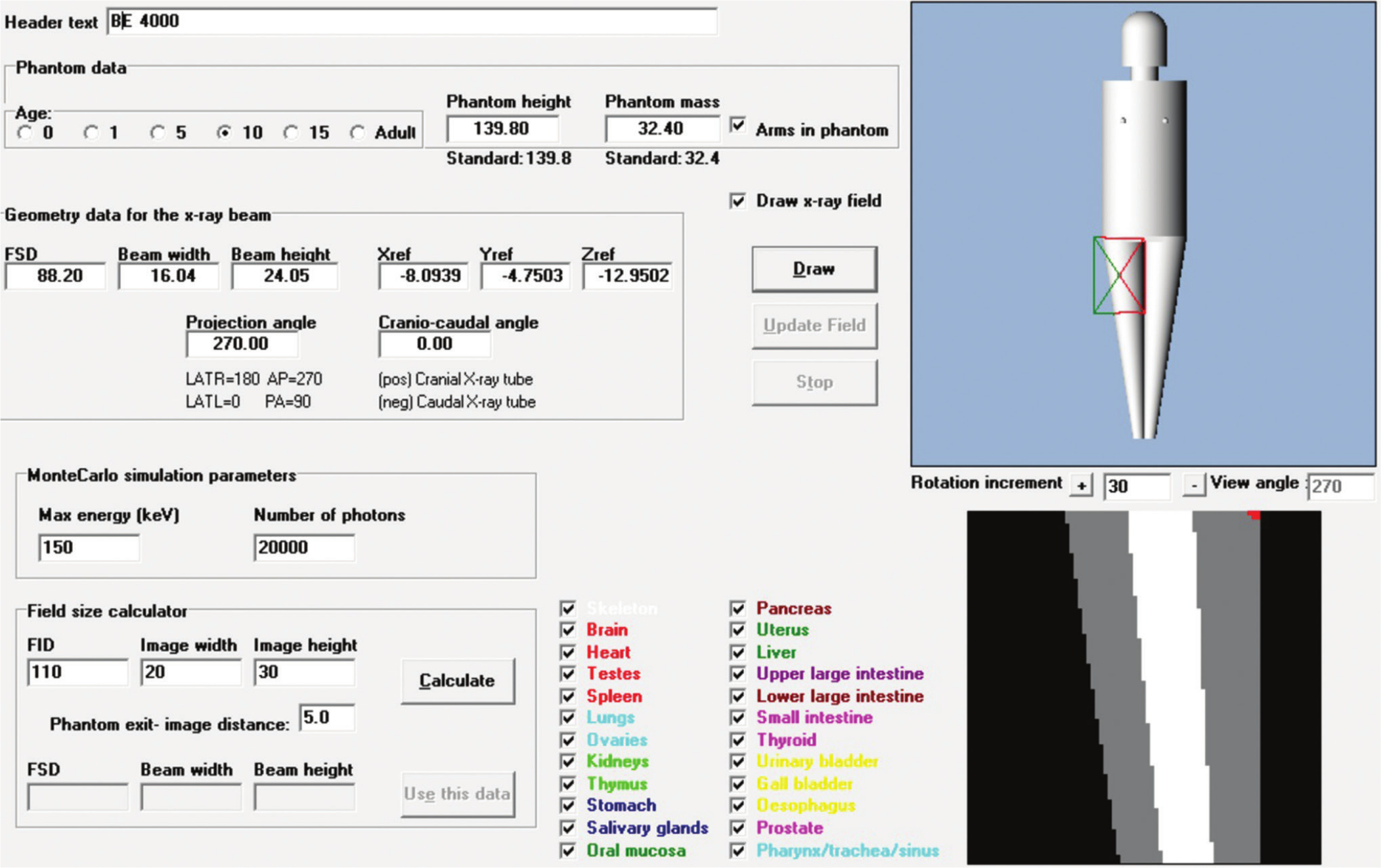
Screenshot example of the first step of the use of the PCXMC software. Note the following parameters: age group, height, weight, focus to skin distance and width and height of the imaging field. The field centre was positioned on the extremity such as the example.
The main outcome was the ED calculated in mSv with the PCXMC software, and the secondary outcome was the LAR as a percentage.
We compared ED and LAR according to the surgeon level, BMI and age. To limit age and sex bias, BMI-for-age-sex was computed as a z-score according to de Onis et al 18 and body weight status categories were defined using World Health Organization recommended cut-offs. 19
Patients were divided in two age-groups: ‘less than or equal to 8-year-old’ versus ‘more than 8-year-old’. The eight-year-old threshold was chosen in order to have similar sample in each group. Results were assessed for the whole series as well for forearm and femoral diaphysis.
Analyses used R software (v.3.1.3) and the RStudio interface (RStudio Team 2016, Boston, Massachusetts, USA). Uni- and multivariable linear regression analyses were performed to assess associations between ED and patients (age, BMI, sex) and surgical (operative time, irradiation time, operator level, level of surgery) characteristics. Additional analyses were conducted to ensure no violation of the assumptions of residuals linearity and homoscedasticity of regressions, but the results were not reported. Finally, age groups were compared using Student's t-test for continuous outcomes and Pearson chi-squared for dichotomous outcomes. Level of significance was set at p < 0.05. Cohen's effect size (ES) and 95% confidence interval were reported.
Results
In total, 57 patients were eligible; among these, five patients were excluded due to missing irradiation data and one because of an aberrant result considered as a data recording error, which was 1000-times less than the mean values. Among the remaining 51 patients, there were 14 girls and 37 boys. The mean age was 9.4 years (sd 3.7; 4.4 to 16.6). Mean height was 136 cm (sd 24; 90 to 180) and mean body weight was 36 kg (sd 18; 15 to 84). Mean BMI was 18.3 kg.m2 (sd 4.2; 12.4 to 30.9). Fractures affected upper extremities in 43 cases (84%) and lower extremities in the remaining eight cases (16%). Each main region was divided into two secondary regions, which were allocated as follows: 43 upper extremities (four clavicles, five arms and 34 forearms) and eight lower extremities (six thighs and two legs).
The mean operative time from incision to closure was 66 minutes (sd 38; 22 to 159). Particularly for forearm both bones and femoral shaft fractures, mean operative time was respectively 57 minutes (sd 30) and 83 minutes (sd 53). In all, 42 patients (82%) were operated by a junior surgeon assisted by a senior, and the remaining nine patients (18%) by a senior alone.
The mean overall intraoperative imaging time was 121 seconds. For the forearm fractures, the time was 137 seconds, and 95 seconds for the femur.
The mean overall DAP was 446 mGy.cm2. It was 440 mGy.cm2 for the forearm and 669 mGy.cm2 for the femur.
The mean overall ED was 0.085 mSv. Mean ED was 0.091 mSv and 0.051 mSv for the forearm and femur, respectively. The mean overall LAR was 6.5x10−4%. Specifically for the forearm, it was 6.9x10−4 and 4.5x10−4 % for the lower extremity. Detailed results are summarized in Table 1.
Irradiation data
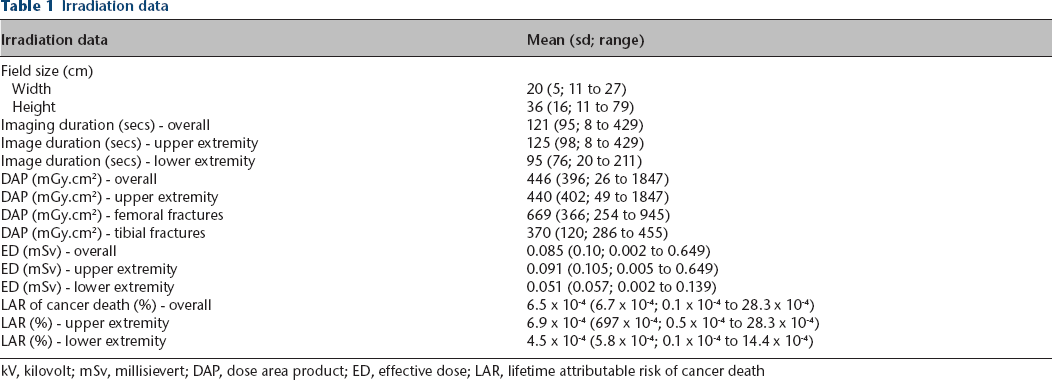
kV, kilovolt; mSv, millisievert; DAP, dose area product; ED, effective dose; LAR, lifetime attributable risk of cancer death
There were neither intraoperative nor immediate postoperative complications. At follow-up, two (4%) fracture recurrences and one (2%) bursitis were reported, and among them one (2%) needed an unexpected reoperation. In all, 42 (81%) implant removals were performed from six to 12 months postoperatively according to our institutional protocol. Radiographic results were satisfactory in all cases.
Univariate linear regression (Fig. 2) showed a significant association between ED and irradiation time (p < 0.001). There was no significant association between ED and all other outcomes including age, sex, BMI and surgery time (p > 0.05). Multivariate linear regression (Table 2) confirmed the absence of a confusion effect with only significant association with irradiation time.
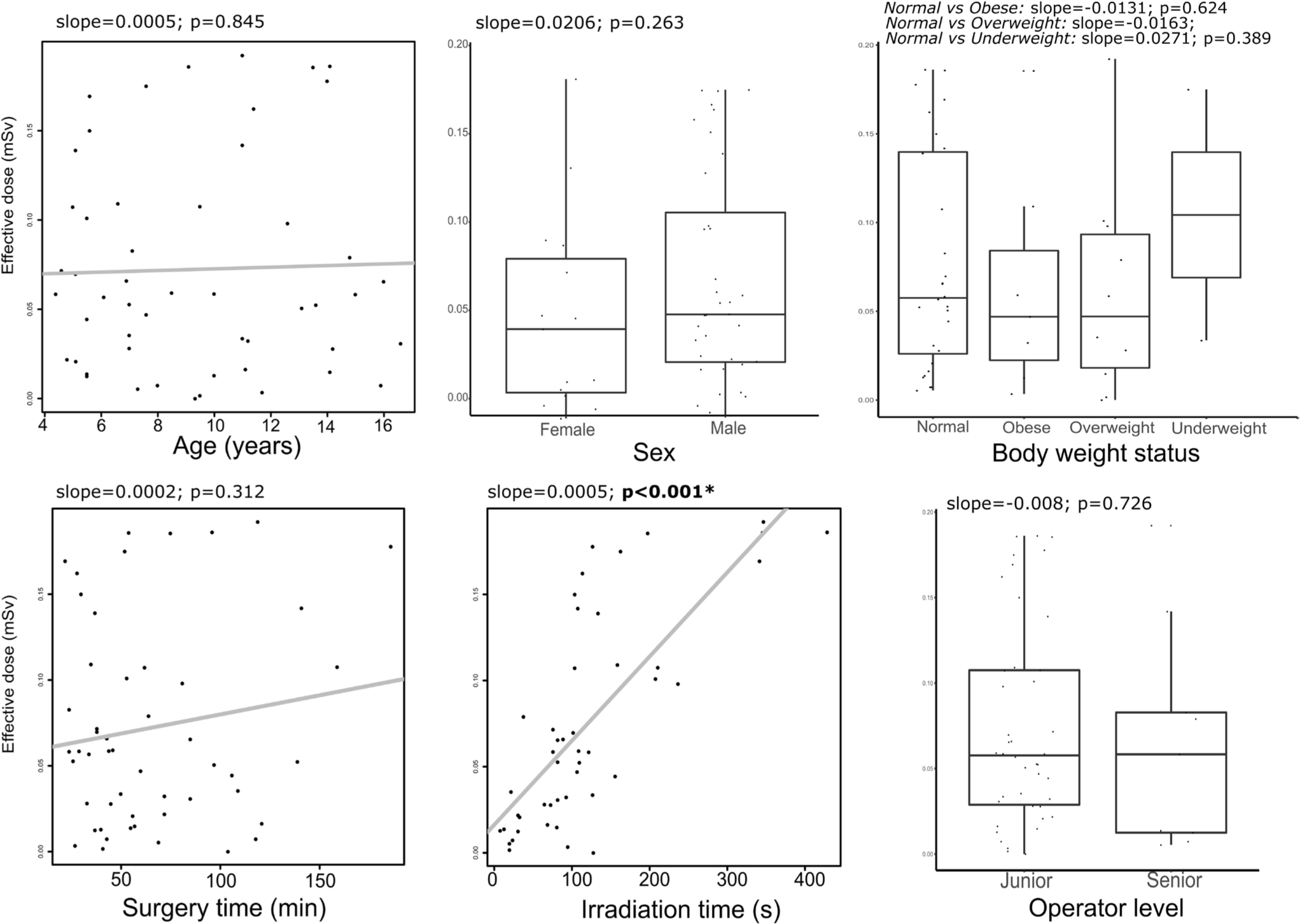
Univariable linear regression results with respectively scatterplot and boxplot of effective dose (in mSv) with general and surgical characteristics of the 51 patients. Level of significance is set at p < 0.05 (slope, the linear regression coefficient; p, the p-value; s, seconds).
Multivariate linear regression of effective dose (in mSv) with general and surgical characteristics of ESIN surgeries of the 51 patients
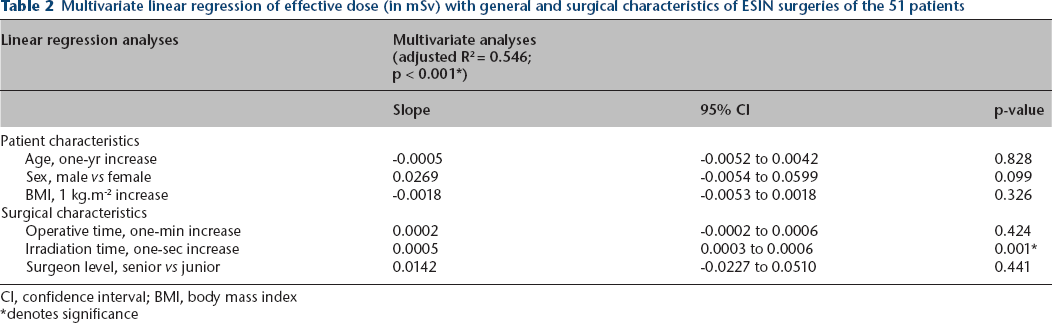
CI, confidence interval; BMI, body mass index
denotes significance
According to the patients’ age, with a median value of eight years, we only found a significant difference in operative time, with a lower time for the less than or equal of eight years group in comparison with the more than eight years group: 49 minutes versus 82 minutes, respectively (p < 0.001) and also for the width of the irradiation field (p = 0.0279), related to a lower height with younger age. All these results are summarized in Table 3.
Age groups comparison (eight and less versus more than eight years old)
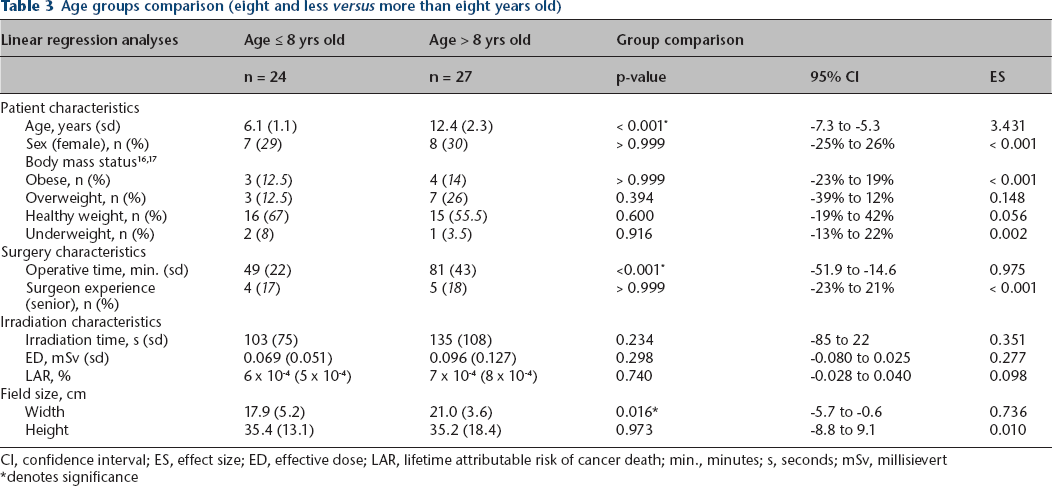
CI, confidence interval; ES, effect size; ED, effective dose; LAR, lifetime attributable risk of cancer death; min., minutes; s, seconds; mSv, millisievert
denotes significance
Discussion
The most important finding in this study was the low level of overall ED calculated, and the associated LAR, for patients operated on using a C-arm in our current practice in ESIN of long bone fractures. The main result of ED was 0.085 mSv and of LAR was 6.5x10−4%. In our series, mean operating irradiation was 121 seconds and DAP was 446 mGy.cm2.
Literature about radiation dose related to intraoperative imaging devices in children is rare. Only a few studies have been published, especially about imaging duration rather than radiation dose.
Kraus et al 20 published a study in 2007 about ESIN for supracondylar fractures on 54 children, slightly younger than our patients (5.9 years). The mean operative time was 51 minutes (sd 31; 14 to 105) and the mean intraoperative imaging time was 80 seconds (sd 56; 18 to 228).
Uçar 21 reported on 43 ESINs of femoral shaft fractures in children with a mean operative time of 71 minutes and a mean fluoroscopy time of 80 seconds. With a similar technique in femur, Sun et al 22 found an operative time of 53 minutes (sd 15) and an intraoperative fluoroscopy time of 65 seconds (sd 29).
In another study Kraus et al 23 published in 2008 on ESIN of the lower extremities they provided irradiation information and surgical considerations about femoral and tibial shaft fractures. For femoral fractures, he found operative duration and irradiation time of 42 minutes (18 to 129) and 70 seconds (12 to 193), respectively. The mean DAP was 336 mGy.cm2 (53 to 1901). For tibial fractures, the imaging time was 42 seconds (6 to 168) and the operative time was 28 minutes (12 to 51).
Other authors who performed ESIN of the lower extremities found imaging duration between two and three minutes,24,25 and between seven and 17 minutes for the study from Joeris. 26 Other differences such as lower irradiation doses might be explained by the improvement of image quality with decreasing doses in more recent imaging devices. Regarding the operative time, the shorter time of some series versus our experience may be due to the high level of assistance to junior surgeons in our teaching hospitals.
The LAR was never reported in the paediatric orthopaedic literature although we did find some studies in paediatric cardiology. Hill et al 27 performed a phantom study on cardiac catheterism. He found higher mean ED of 0.36 mSv (0.14 to 0.58) for the newborn phantom and 0.41 mSv (0.22 to 0.79) for the five-year phantom. These results were established for a 60 seconds duration of continuous fluoroscopy. LAR was between 0.19% and 2.03% for the newborn and ranged from 0.15% to 2.62% for the five-year phantom, clearly higher than our results. Varghese et al 28 also published on cardiac catheterism and found an ED between 2.5 mSv and 6.1 mSv, with a LAR from 0.05% to 0.08%, according to the imaging technique performed (angiography with flat panel detector). The cardiac zone of imaging with more sensitive organs and the different imaging device may explain higher ED and LAR.
Astonishingly, the hypotheses of lower ED and LAR with younger age, with lower BMI-for-age-sex and with higher surgeon level were not confirmed. BMI and age were not correlated to ED. Maybe this absence of difference could be explained by reduced irradiation field centred on the specific limb during the surgery. Arms and legs have similar dimensions even through different ages for children. Thus, BMI and age could not have been correlated to ED.
We found some limitations in the current study. Firstly, the small sample of patients who were operated on in the leg region did not enable an adequate comparison with the literature. Secondly, we did not perform a comparison between two imaging modalities, so we provided only a description of our results in the field of irradiations. Thirdly, there was a measure bias in the dose calculation. In the software, there were only the following ages: newborn, one year, five years, ten years, 15 years and adult. This obliged us to consider the closest age group for dose calculation. Besides, we could not intraoperatively measure the exact FSD in clinical practice, considering this distance modifying every time during the surgery. For reproducibility purposes, we considered the standard FSD of 80 cm for all patients, according to personal experience. Moreover, voltage of 80 kV and 2.5 mm of Al filtration were used for all patients according to standard settings in the software. Including this measurement bias, the accuracy of the ED estimation should be supported by the consideration of other parameters. Finally, we had only eight cases considered as treated exclusively by senior surgeons in this series. The dose difference related to the surgeon experience could not be reached in this paper, because of a lack of cases. Further studies with larger samples are needed in order to confirm this result.
The use of 2D imaging raises questions about 3D imaging with navigation in the operating room. From one minute of 2D fluoroscopy, the dose would be an average of four-times that in the same conditions with the O-arm, according to a phantom study. 29 Nowadays, other 3D imaging devices are in development around the world, especially cone-beam computerized tomography with flat panel detector, allowing a dose reduction. 30 Advances in imaging devices may decrease doses while increasing image quality with more optimized imaging technology.
This study could be a basic reference for further irradiation studies. We think that according to these results, in the future, radiation dose related to the imaging devices can be further optimized, especially with 3D imaging devices and navigation, which were not studied here, but are under our attention now.
Conclusion
Treatment of long-bone fractures by ESIN in children found an overall low level of ED and low LAR of cancer death with utilization of the 2D C-arm device in current practice. These values were not correlated either to age, BMI or operation duration. These results are encouraging but keep us aware of the need to optimize radiation exposure in children, especially for the future through the development of new imaging technologies.
Footnotes
The other authors declare no conflict of interest relevant to this work.
PLD: Collected data, Performed critical revision of the manuscript.
OM: Collected data, Performed critical revision of the manuscript.
MSM: Designed the study, Interpreted data, Performed critical revision of the manuscript.
ATF: Interpreted data with statistical analyses, Performed critical revision of the manuscript.
DC: Interpreted data, Performed critical revision of the manuscript.
PL: Designed the study, Interpreted data, Performed critical revision of the manuscript.
All authors have been actively involved in the drafting and critical revision of the manuscript and provided final approval of the version to be submitted.