
Abstract
Abstract
Purpose
The aim of this study is to assess the pelvis's morphology and spatial orientation of the acetabulum, and their relation to the severity of Congenital Femoral Deficiency (CFD) using 3D imaging. Defining these pathologies is crucial for adequate surgical correction.
Methods
The shape and structure of the acetabulum and pelvis were evaluated in 14 children with unilateral CFD via 3D computed tomography (CT) scans, and then analysed with geometric morphometrics (Procrustes ANOVA). The association between pelvic directional asymmetry and CFD classifications (Aitken, Paley) was assessed. The affected acetabulum's orientation was compared to the non-affected side, and the variability of orientation in different CFD types was evaluated (bivariate correlation).
Results
The hemipelvis with CFD is characterized by a smaller acetabulum, a laterally curved ischium and a less upright ilium (p < 0.001). Multivariate regressions revealed a greater level of pelvis asymmetry in more severe types of CFD (p < 0.001). The acetabulum orientation assessment showed a significant decrease in mean anteversion (1.3°) and inclination (9.6°) angle, when compared to the non-affected side (26°and 17.1° respectively; p < 0.001).
Conclusions
The affected side of the pelvis is considerably smaller and more deformed, and this should be considered during limb lengthening. The acetabulum presents with significant dysplasia due to its severe retroversion and steepness (superoposterior distortion). This should not be interpreted as a simple wall deficit, but as a complete acetabular misalignment (often misinterpreted in 2D imagery). Using transiliac osteotomies (e.g. Dega, Salter) is debatable due to abnormal acetabular orientation (superoposterior malalignment). Therefore, alternative options, e.g. San Diego or triple pelvic osteotomy, should be considered.
Introduction
Congenital Femoral Deficiency (CFD) is one of the most common congenital longitudinal deficiencies affecting the entire pelvis and surrounding structures, including the femoral bone, acetabulum and soft tissues. Due to the complexity of hip deformity, it is an orthopaedic condition which is challenging to treat. While the treatment of the short and deformed femur is well established, there is still ongoing discussion on addressing the methods of correction of the malformed hip socket.1,2 The lack of appropriate correction leaves considerable acetabulum deficiency, which in turn increases the risk of hip instability especially during limb lengthening. 3 Little is known about the morphology of the acetabulum and its spatial orientation in CFD when compared with other pathologies, such as Developmental Dysplasia of the Hip (DDH).4,5 Nevertheless, many authors still describe its structure in detail with implications for surgical treatment.2,6,7 Among the existing studies concerning the acetabulum in CFD, the pathology is either identified descriptively, or with the use of 2D methods (where accuracy may be limited).6,7 Moreover, throughout the growth period the risk of recurrence of hip instability is high, even if the deficiency of the acetabulum and other elements of the pathology were previously corrected.3,8 The reasons leading to this decline in hip stability are unknown, however a lack of full correction of acetabular deformity may be the most important reason. Therefore, all of the above have prompted an evaluation of whether the assumptions based on 2D studies are correct, and if the surgical methods chosen to address them are adequate.
The shape and height of the pelvis in CFD are also subjects that are poorly delineated in literature. This knowledge in turn could be applied to improve the assessment of limb discrepancies, especially during lower limb lengthening. 9
Despite the increasing popularity of 3D techniques, their usage in properly diagnosing the anatomy of the acetabulum and hemipelvis in CFD is still lacking. Thus, the purpose of this study was to:
assess the spatial orientation of the acetabulum in individuals with CFD in 3D conditions, and its relation to the severity of the deformity;
assess whether CFD only causes changes in the acetabulum or in the entire pelvis.
Materials and methods
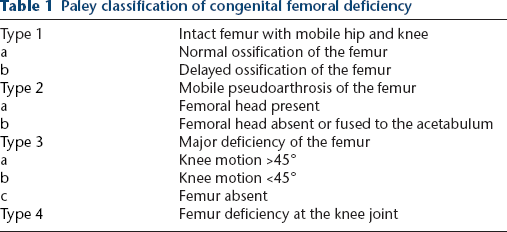
After obtaining approval from the institutional review board, a retrospective review of pelvic computed tomographies (CT) was performed. In total, 20 children with CFD were evaluated, who had not undergone previous hip or lengthening surgeries. After initial analysis, six pelvic CT scans were rejected due to insufficient characterization of the pelvic morphology. The remaining 14 patients showed unilateral CFD, which was categorized according to the classification put forth by Aitken and Paley (Table 1, 2 and 3). The average age of the individuals included in this study was 8.4 years (range three years to 16.9 years) at the time of performing the CT examinations. All pelvises were scanned using a GE LightSpeed VCT 64-slice CT (GE Healthcare, Wauwatosa, Wisconsin, USA) with a standard protocol (0.63 or 1.25-mm slice thickness), and saved as Digital Imaging and Communications in Medicine (DICOM) images. Virtual 3D model reconstructions of the pelvic girdle were generated from these CT images, using the segmentation software, InVesalius (Centro de Tecnologia da Informação Renato Archer (CTI), Campinas, Brazil).
Paley classification of congenital femoral deficiency
Aitken classification of congenital femoral deficiency

Detailed analysis of patients with congenital femoral deficiency included in this study.
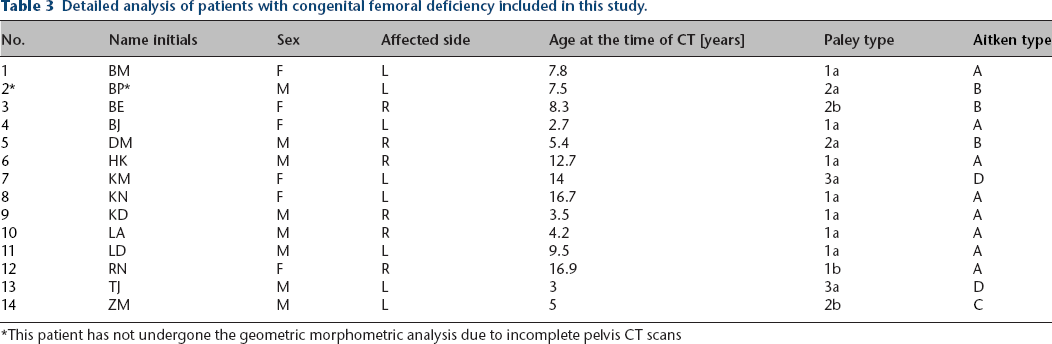
This patient has not undergone the geometric morphometric analysis due to incomplete pelvis CT scans
Once the 3D models were obtained, two important steps were taken to accurately describe pelvic morphology in relation to the severity of the disease; the acetabular axis measurement and pelvic shape analysis through anthropological methods.
Acetabulum axis measurement
All acetabulum measurements were completed based on the 3D reconstructions of pelvic CT scans, with the use of rapid-prototyping techniques (Rhinoceros, Robert McNeel & Associates, Seattle, Washington, USA; ScanIP, Simpleware, Exeter, UK). The acetabulum axis was set according to a previously published technique, described in detail by Jozwiak et al. in BMC Musculoskeletal Disorders (Fig. 1). 10 The anterior pelvic plane was initially set as the reference plane to determine the acetabulum axis measurement based on the Anterior Superior Iliac Spines (ASIS) and pubic symphysis. However, in our cohort, ASIS were deformed on the affected side which significantly changed the position of the reference plane and disturbed the axis measurement. As a result, this marker was rejected and the Sacrum Base Plane (SBP) was used instead as the reference plane as it did not distort the measurements (Fig. 1d). 10 The SBP is established by the sacral base, and is defined as a plane interpolated from the mesh of points located on the surface of the sacrum base (usually over 150 points). The vertical plane is perpendicular to the horizontal plane and coincides with the geometric centre of the SBP and the midpoint of a line connecting the centres of the pubic tubercles. 10

Steps to determining the acetabular axis:
Due to the non-normal distribution of data, the Wilcoxon test was used to compare differences in the acetabulum position between affected and unaffected sides. The relationship between the category of CFD and acetabulum axis measurements of the affected pelvis side was also analysed using Spearman's rank correlation, separately for both classifications (Aitken and Paley).
All statistical analyses were significant at level p < 0.05 and carried out using R software (The R Foundation for Statistical Computing, Vienna, Austria).
Pelvic shape analysis
3D reconstructions of the pelvic girdles were examined using geometric morphometrics, enabling investigators to carry out sophisticated analyses of the shape.11,12 On each 3D reconstruction of the pelvic girdle, 53 anatomically homologous points, called landmarks, were digitized twice by the same observer using Landmark software (version 3.0; IDAV, Davis, California, USA). The points (Fig. 2) on the pelvic girdle were established based on standardized landmarks put forth by previous research, 12 however, the number of landmarks on the acetabulum were increased in order to better evaluate the changes of this structure.
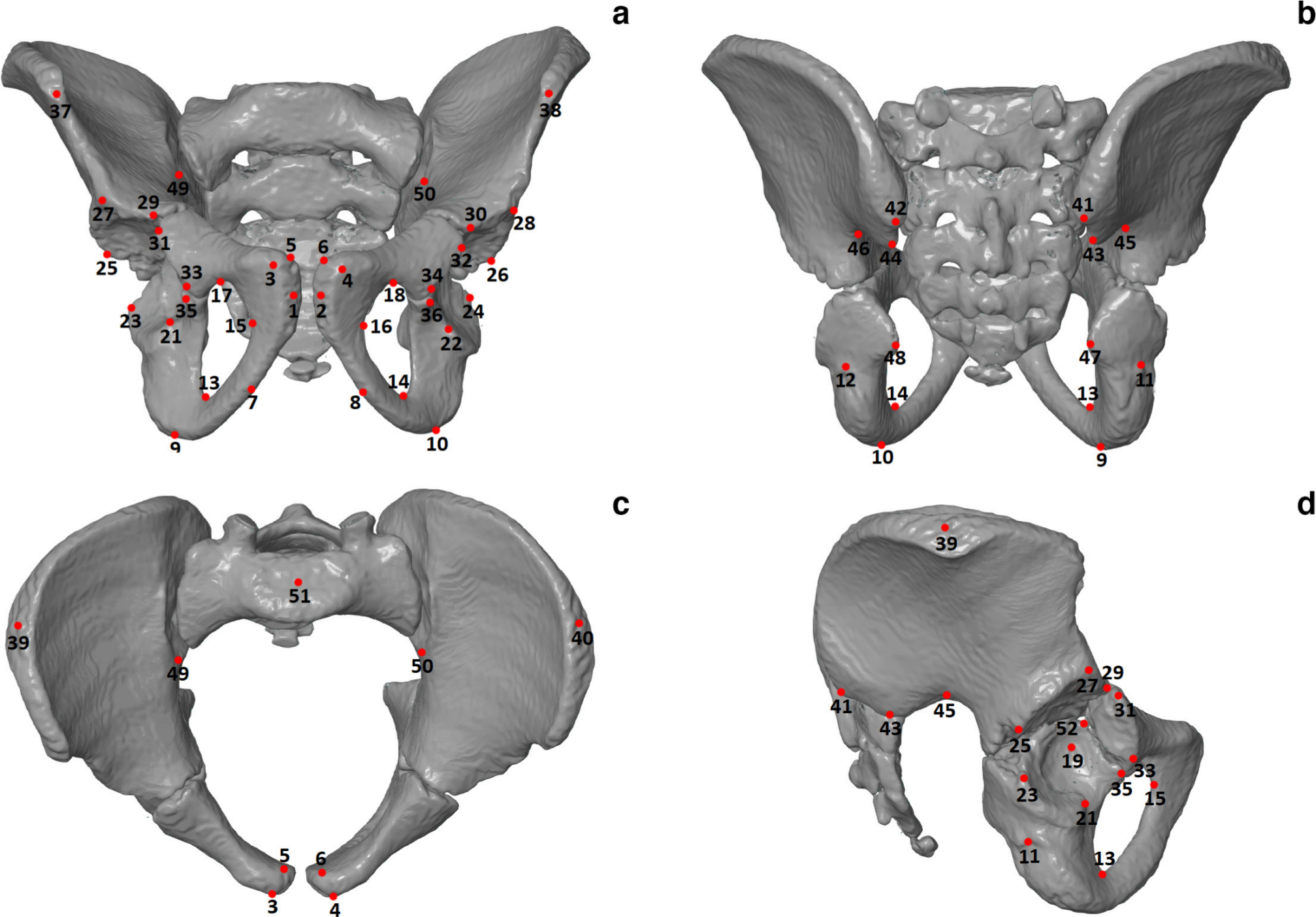
Pelvic girdle with landmarks (red dots):
After digitization, all the pelvises were calibrated to the same size in order to compare their shapes. 13 Next, Procrustes analysis of variance (ANOVA) was calculated to investigate whether differences in pelvic shape and size are significant between individuals and each side of the body. Furthermore, a multivariate regression was used to analyse the association between the shape of the pelvis and acetabulum, and both types of CFD classification separately (Aitken and Paley). All statistical analyses were significant at level p < 0.05 and carried out using MorphoJ (Manchester, UK) and GraphPadInstat (San Diego, California, USA) software.
Results
Acetabulum axis measurement
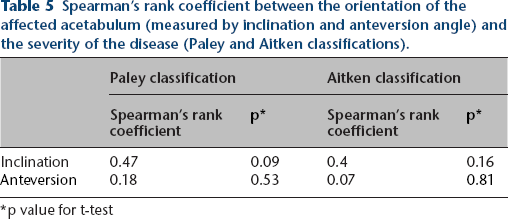
Statistical analysis of the acetabulum orientation based on the measurements of the axis revealed that the affected acetabulum has significantly decreased the anteversion angle (9.6° on the affected side versus 17.1° on the healthy side, p < 0.001), as well as the inclination angle (1.3° versus 26°, respectively; p < 0.001) (Table 4, Fig. 3). In regards to Spearman's correlation between the orientation of the affected acetabulum and the severity of the disease, the measured angles did not show a significant relationship with the types according to Paley classification (p value 0.09 and 0.53 for Inclination and Anteversion, respectively) and Aitken classification (p value 0.16 and 0.81 for Inclination and Anteversion, respectively) (Table 5). Additional evaluation of the anterior wall via geometric morphometrics revealed that there is a tendency to diminish not only the size of the posterior wall, but also the anterior wall of the acetabulum.
Comparison of acetabulum orientation between affected and non-affected side of the pelvis (Inclination and Anteversion Angle).
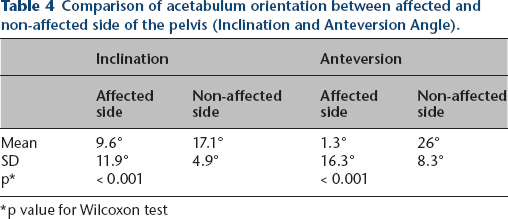
p value for Wilcoxon test
Pelvic girdle with acetabular axis in two basic planes;
Spearman's rank coefficient between the orientation of the affected acetabulum (measured by inclination and anteversion angle) and the severity of the disease (Paley and Aitken classifications).
p value for t-test
Pelvis shape analysis
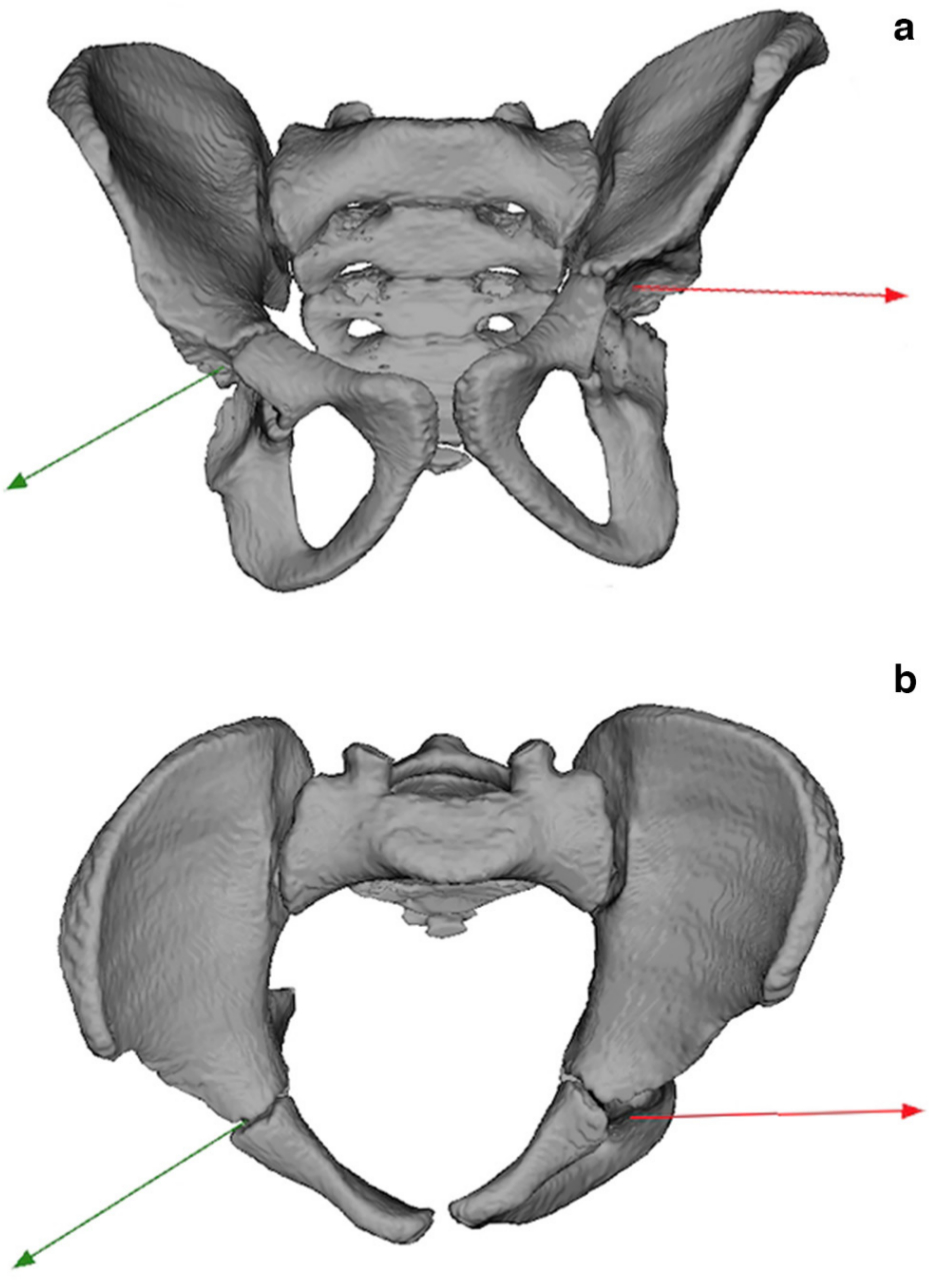
The differences in pelvic size and shape between the affected and non-affected side are significant (p < 0.001; Table 6). The side of the pelvis with CFD is characterized by a smaller acetabulum, a less upright ilium and laterally curved ischium (Fig. 4).
Results of the Procrustes ANOVA for the differences in pelvic shape between individuals and each side of the body (affected and non-affected).
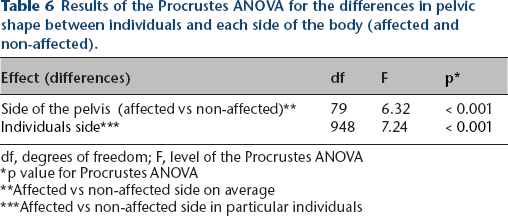
df, degrees of freedom; F, level of the Procrustes ANOVA
p value for Procrustes ANOVA
Affected vs non-affected side on average
Affected vs non-affected side in particular individuals
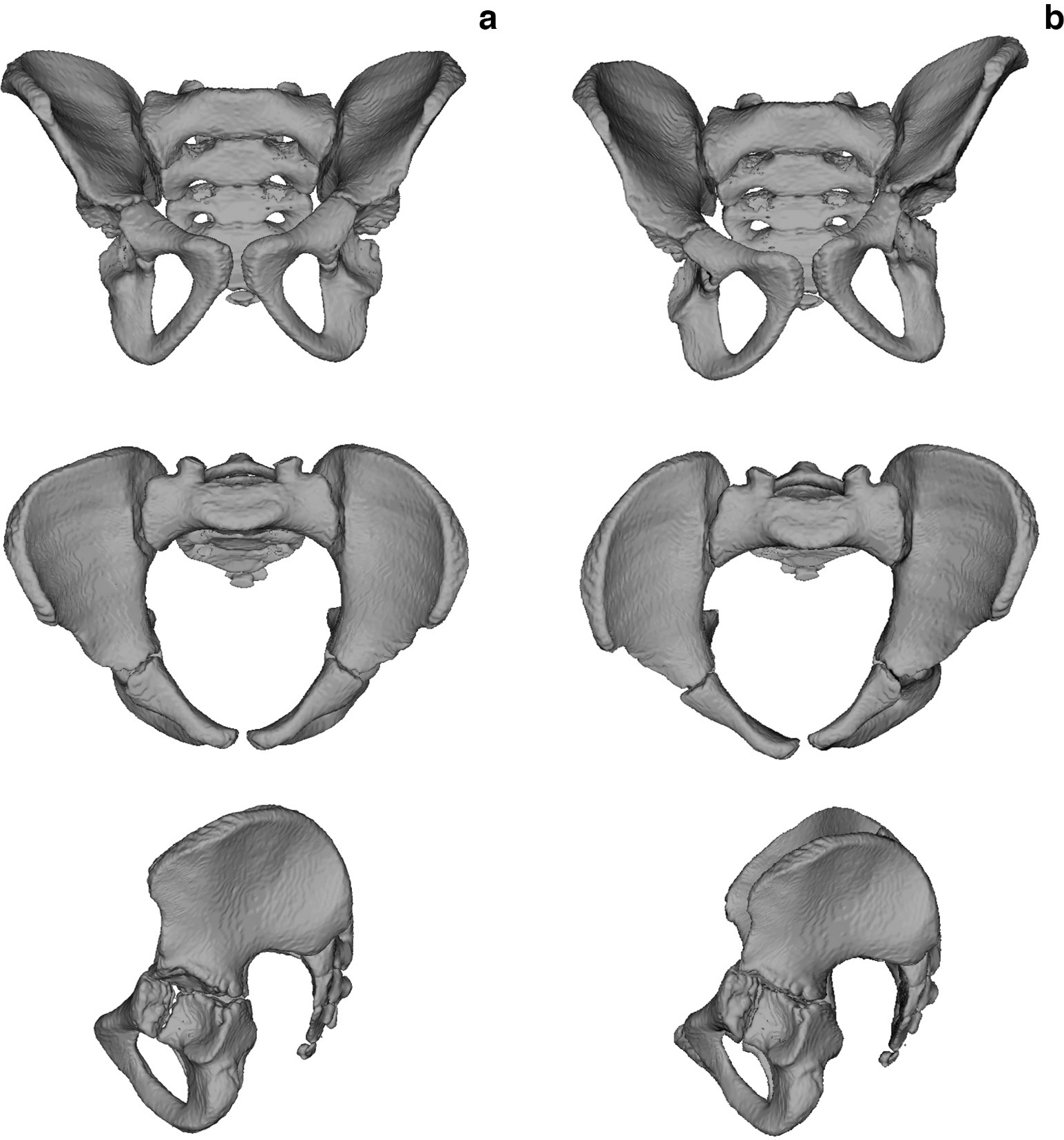
Directional asymmetry of the pelvic girdle:
The association between pelvic size and shape was not significant, therefore subsequent statistical analyses were carried out without taking size into account. All multivariate regressions were positively significant (p < 0.001), meaning that the most severe type of CFD (according to Aitken and Paley) is characterized by greater differences in pelvic shape between each side of the body. The greater the severity of the disease, the smaller the acetabulum and more bent the ischium on the affected side of the pelvic girdle. Nonetheless, the type of CFD also influences the pelvic shape on the non-affected side. Along with the classification of CFD, the ilium is aligned more vertically, and the acetabulum is larger on the non-affected side (Fig. 5).
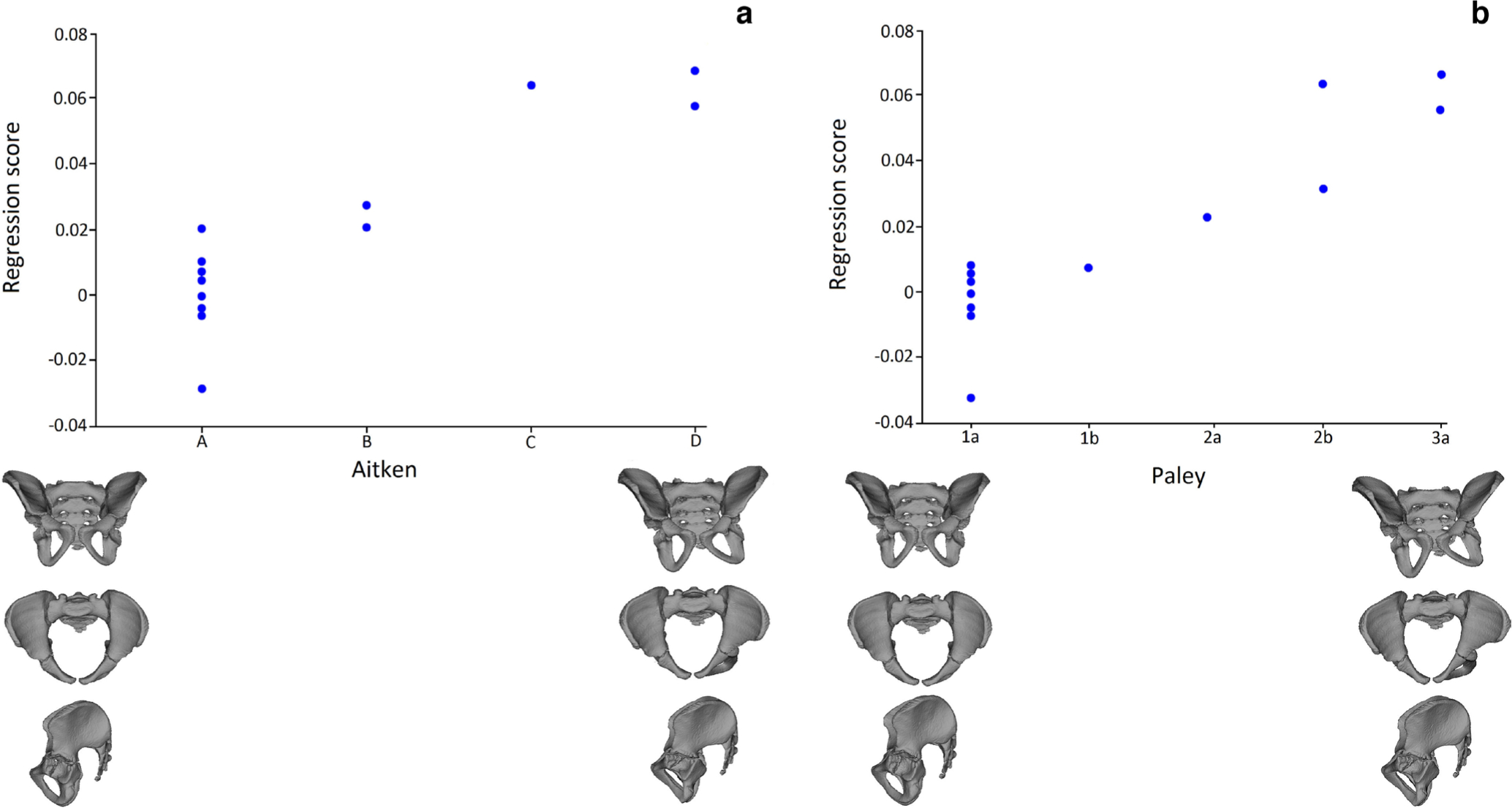
Scatterplots of the association between asymmetry component of the pelvic shape and type of CFD derived from the multivariate regression:
Discussion
This study presents the anatomical considerations of the acetabulum and pelvis in CFD via 3D morphology. Acetabular morphology has been demonstrated to be influenced by pelvic position. 14 It must be emphasized that describing the deficit of the acetabular wall based on 2D scans, such as plain radiographs or simple CTs,6,7,8 may give rise to extensive measurement errors coming from the parallax phenomenon (e.g. measurements of some parameters such as acetabular version or anterior acetabular index are dependent on the position of the pelvis during examination).5,15,16 Our study avoids these problems by using 3D techniques for all of the measurements, making it a very precise method of evaluating the acetabulum and pelvis. However, further studies are needed concerning relations between the 2D and 3D measurements in patients with CFD, as well as how these relations and the severity of the disease alter hip stability during and after femoral lengthening. Yet, this study also has its limitations. The number of pelvises taken into account is low due to the limited number of patients born with the disease, thus it is possible that other patterns of acetabular deficiency exist but were not present in the current cohort. 17 Nevertheless, the number of subjects studied here is comparable to other research (e.g. in Biko et al. and Dora et al., seven and 14 hips were taken into account respectively).6,7 This study also did not consider the entire hip joint with the proximal femur, which could show relevant relations between the acetabulum and the femoral head. However, this was omitted intentionally since the acetabulum seems to be much more problematic to interpret than the deformed femur. Next, the distribution of types, both in Aitken and Paley classification, is not symmetrical in the presented cohort. However, it is in accordance with the frequency of these types in the population. Finally, this study only presents the considerations concerning the static position of the pelvis and the hip. Potential future studies could also focus on how the presented parameters affect the gait and how they change during gait.
The presented results clearly show that the acetabulum in CFD is severely dysplastic with changes in its orientation – the acetabulum axis is deviated posteriorly and upwards. These results are only partially consistent with the previous research; Biko et al. stated that the deficit is mainly posterior or antero-posterior, 6 while Dora et al. found that there is a posterior wall deficit in conjunction with normal or prominent anterior wall in acetabula. 7 While previous studies focused on the particular acetabular wall deficits, our study shows the spatial nature of the deformity with the above mentioned deviation of the acetabulum's axis. However, the lack of significant association between the type of CFD and differences in acetabulum orientation (Spearman's rank correlation not significant, however showing a positive trend between the inclination angle and the severity of the disease) may be caused by more global changes inside the acetabulum, in which the decrease in the length (or depth) of the anterior wall accompanies the deficit in the posterior wall. However, it should be noted that the correlation between acetabular orientation and classification could be insignificant because it was severely underpowered.
The above mentioned changes impact not only the acetabulum, but also the affected side of the pelvis (and non-affected side to a lesser degree). The side of the pelvis with CFD is characterized by a smaller acetabulum, a laterally curved ischium and less upright ilium. This makes the affected side of the pelvis shorter than the opposite side. Additionally, significant changes in the shape and position of the ilium influences the levels of iliac spines (ASIS is lower on the affected side), which may disturb the measurements of limb length. One must take this into account during examination of patients with CFD, and refer more to the radiological assessment than to the clinical examination based on the leg length measurements, especially while getting close to the equalization of the limb length during lengthening procedures.
Finally, the obtained results suggest that current techniques used to address the acetabulum deficits, such as Dega transiliac osteotomy or Salter osteotomy, may not be sufficient to fully secure the hip during further limb lengthening.7,18 Since the orientation of the acetabulum is skewed posteriorly and superiorly, we predict that the San Diego pelvic osteotomy (modification of Dega procedure, which enables better posterior coverage), or triple pelvic osteotomy in older children, might be better methods for the proper redirection of the acetabulum walls.18,19 Despite this, further investigation including prospective studies comparing different surgical techniques or experimental models should be performed, as has been done previously in DDH cases by Caffrey et al. 20
In conclusion, this study clearly shows that the acetabulum in CFD is distorted globally, with its axis skewed mainly posteriorly and superiorly. The severity of the disease influences the size of the acetabulum, making it smaller. However, it does not affect the range of the acetabulum orientation disruption. Finally, in this study we proved that the deformity affects not only the acetabulum on the pelvis side, but also the remaining parts of the pelvis.
Footnotes
Acknowledgement
The authors would like to thank Dr. Raymond W. Liu, MD for suggestions which helped to improve the quality of this study.
MS: Took part in the creation of the research design and formation of the study methodology, Participated in the interpretation of results, Searched the literature, Drafted the manuscript.
AMK: Took part in the creation of the research design and formation of the study methodology, Carried out geometric morphometrics analysis, Took part in the interpretation of results, Revised the statistical data, Created images for the manuscript.
PK: Searched databases for the patients, Took part in formation of the study methodology, Drafted the manuscript.
MR: Took part in formation of the study methodology, Carried out radiological evaluation of data.
PP: Participated in the interpretation of results, Drafted the manuscript, Provided the language edition of the article.
MJ: Searched databases for the patients, Took part in formation of the study methodology, Drafted the manuscript.