
Abstract
Abstract
Purpose
The purpose of this study was to investigate post-therapeutic lower extremity rotational profiles in children with developmental dislocation of the hip (DDH), the differences between these values and those of normal children, and the relationship between these differences and clinical and radiological results.
Methods
In 82 lower extremities of 64 patients, the foot-progression angle was measured clinically and the transmalleolar axis angle photographically, and hip rotations and thigh–foot angle were measured both clinically and photographically. The data obtained were compared with Staheli's data for normal children. In addition, clinical and radiographic data were compared within subgroups and with Staheli's data. Student's t-test and one-way ANOVA were used for statistical evaluation.
Results
The medial rotation of the hip, the average clinical value was 44.66°, and the photographic value was 42.28°. Lateral rotation of the hip, the average clinical value was 38.01°, and the average photographic value was 37.29°. Thigh–foot angle, his angle was clinically 8.23° and photographically 9.68°. Angle of the transmalleolar axis, the photographic average was 21.59°. Foot-progression angle, the clinical average was 10.70°. It was determined that the lower extremity rotational profiles of children with DDH treated after walking did not differ from those of normal children, but that the internal and external hip rotations of McKay type III and IV patients were below those of normal children and of McKay type I and II patients.
Conclusion
Lower extremity rotational profiles in children with DDH who received appropriate treatment were the same as those for normal children.
Introduction
Rotational disorders are frequently encountered in the pediatric population. When rotational profile values exceed normal limits, the condition is called a torsional deformity. While there is a large amount of data on assessment methods and treatments for frontal and sagittal plane deformities, rotational problems in the transverse plane have been neglected due to the difficulty of assessment. At present, these deformities can be gauged by a number of electronic techniques including tomography, facilitating the determination and evaluation of variations. Few studies have been published on lower extremity rotational deformities, and these have been done on children with no concurrent pathology [1–8]. Staheli et al. [5] established the lower extremity rotational profiles of normal children, providing the clinician with a more objective and quantitative standard of measurement. To date, one study has been performed on the lower extremity rotational profiles of children with cerebral palsy [1]. Insufficient attention has been given to transverse plane deformities concurrent with other anomalies and deformities that affect lower extremity rotational profiles.
Deformities and variations of the lower extremity in the transverse plane may be concurrent with benign in-toeing, as well as with serious conditions such as developmental dislocation of the hip (DDH), clubfoot, and neuromuscular diseases. The most important component of the potoanatomy of DDH is increased femoral anteversion, which directly affects the lower extremity rotational profile [3]. The profile may also be altered by surgical methods implemented during therapy, particularly derotation osteotomy, and the positions of fixation and of devices used after fixation, and complications such as avascular necrosis and sclerosis.
In the present study, the post-therapeutic lower extremity rotational profiles in children with DDH and the differences between these values and those of normal children were assessed, and the relationship between these differences and clinical and radiological results was investigated.
Materials and methods
The subjects of our study were children with DDH who had been treated either conservatively or surgically and whose therapy, including rehabilitation, had ended at least 2 years before. A total of 82 lower extremities of 64 patients were assessed, including both extremities of the 18 bilateral patients, and the side with dislocation of the hip in the 46 unilateral patients. The average age at the start of treatment was 3.33 years, and the average age when measurements were made was 7.12 years. There were 51 girls and 13 boys. Open reduction, Salter, shortening, and derotation osteotomy were performed on 30 of the hips; open reduction, Still, shortening, and derotation osteotomy on one; open reduction and Salter osteotomy on 12; open reduction and derotation osteotomy on nine; open reduction alone on 15; and closed reduction on 16.
The measurements and techniques described below, which Staheli et al. [5] used in normal children, were used in the assessment of lower extremity rotational profiles.
Foot-progression angle
This is the angle between the long axis of the foot and the line of progression. The patient, after stepping in powder, was made to walk on a black wooden surface with a longitudinal line down the middle, and then the angle between the foot's long axis and the line were measured. A plus sign indicates an out-toeing angle, and a minus sign an in-toeing angle. For each lower extremity, the foot-progression angle recorded was the average of six measurements.
Hip rotation
Internal and external hip rotations were measured with the patient in the prone position and the knees at 90° flexion. Measurements were made both clinically by goniometry and photographically. For photographic measurement, images were taken with a digital camera from the caudal towards the cranial while the patient was made to perform internal and external hip rotations, and then the images were transferred to a computer. Lines were drawn on the printouts, and internal and external hip rotations were measured.
Thigh–foot angle and transmalleolar axis angle
The thigh–foot angle was measured clinically and photographically, and the transmalleolar axis angle was measured only photographically. The angle between the long axis of the foot and the thigh was measured goniometrically with the patient in the prone position, the knee at 90° flexion, and the ankle in the neutral position. For photographic measurement, the most prominent points of the lateral and medial malleolus were marked with a skin pen with the patient in the same position, and these points were connected. In the position in which the clinical measurement was made, the camera was placed over the feet and, again, the images taken were transferred to a computer, printouts were obtained, and measurements were made [1]. A line parallel to the thigh was drawn on the printout and connected to the line between the malleoli. In the angle formed in-between, 90° were subtracted and the resulting angle was designated the transmalleolar axis angle [2]. The axis of the foot was drawn on the printout, and the angle between it and the axis of the thigh was designated the thigh–foot angle. Positive values indicate an out-toeing angle, and negative values an in-toeing angle.
Values concerning DDH were compared with Staheli's values for normal children. The following were considered normal: lateral rotation of the hip, 40° (range 25°–65°); medial rotation of the hip, 45° (range 15°–60°); transmalleolar axis, +20° (range 0°–45°); thigh–foot angle, +10° (range −5° to 30°); and foot-progression angle +10° (range −3° to 20°).
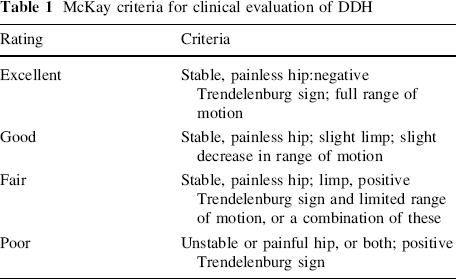
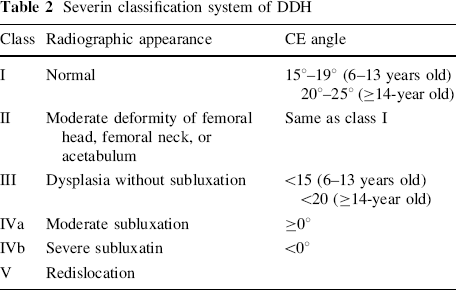
Clinical results were assessed according to McKay's criteria [9], and radiological results according to Severin's radiographic criteria [10, 11] (Tables 1, 2). The relationship between clinical and radiological results and lower extremity rotational problems was investigated (Tables 3, 4). In addition, the hips were divided in two groups; children who underwent derrotation osteotomy, in whom the anteversion was changed surgically (group a, n = 40) and children who had open or close reduction in whom the anteversion was not changed surgically (group b, n = 42). Lower extremity rotational profiles of group a and group b were compared.
McKay criteria for clinical evaluation of DDH
Severin classification system of DDH
Lower extremity rotational profile values of types according to Sever's radiological criteria
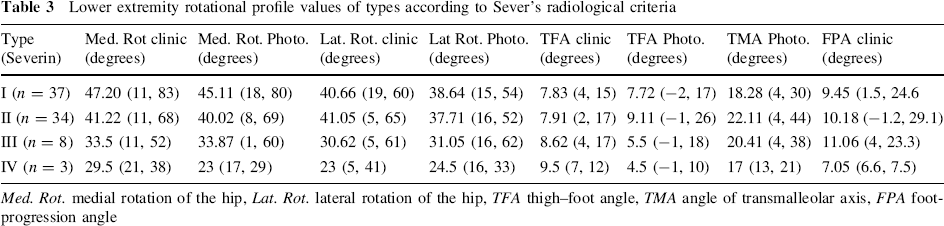
Med. Rot. medial rotation of the hip, Lat. Rot. lateral rotation of the hip, TFA thigh–foot angle, TMA angle of transmalleolar axis, FPA foot-progression angle
Lower extremity rotational profile values of the types according to McKay's clinical criteria
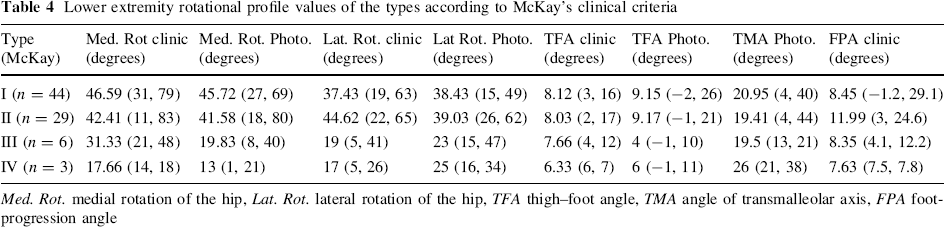
Med. Rot. medial rotation of the hip, Lat. Rot. lateral rotation of the hip, TFA thigh–foot angle, TMA angle of transmalleolar axis, FPA foot-progression angle
Student's t-test and one-way ANOVA were used in statistical evaluation of the results.
Findings
No significant difference was found between any photographic and clinical measurement data (p > 0.05). Therefore, photographic measurements other than foot-progression angle were compared with Staheli's normal child values.
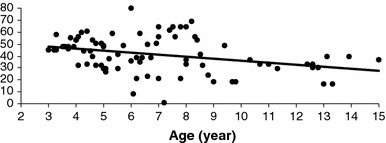
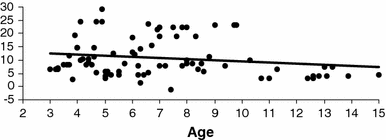
Medial rotation of the hip
The average clinical value was 44.66° (range 1°–83°), and the photographic value was 42.28° (range 1–80°) (Fig. 1). No significant difference was found between the medial rotation of the hip measurements of all patients and Staheli's normal child data (p > 0.05). However, McKay type III and IV patients had significantly lower medial rotations of the hip than normal children and than type I and type II patients (p < 0.05). There was no significant difference between types according to Sever's radiological classification or between these types and normal children (p > 0.05).
Hip internal rotation (photographic)
The average photographic value of medial hip rotation of group a was 41.66° (range 12–62°) and group b was 40.88° (range 1–80°). No significant difference was found between the medial rotation of the hip measurements of group a and group b (p > 0.05).
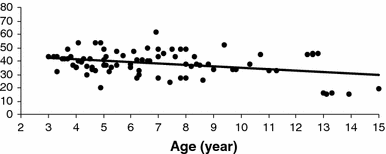
Lateral rotation of the hip
The average clinical value was 38.01° (range 11–83°), and the average photographic value was 37.29° (range 15–62°) (Fig. 2). Lateral rotation of the hip showed no significant difference with Staheli's value for girls of 40° (p > 0.05). Although Sever and McKay type III and IV patients had significantly lower values for lateral rotation of the hip than type I and type II patients and normal children, the differences between these groups turned out to be insignificant because of low numbers of patients (p > 0.05).
Hip external rotation (photographic)
The average photographic value of lateral hip rotation of group a was 36.31° (range 16°–62°) and group b was 34.55° (range 15°–47°): No significant difference was found between the lateral rotation of the hip measurements of group a and group b (p > 0.05).
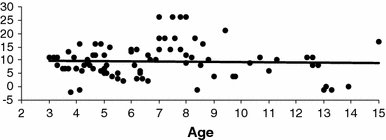
Thigh–foot angle
This angle was clinically 8.23° (range 2°–17°) and photographically 9.68° (range −2° to 26°) (Fig. 3). There was no significant difference between the average values of all patients and normal child values. The average thigh–foot angle of Sever type I patients was 7.71, which was significantly different from the normal child value (p < 0.05). This difference, however, was within the range for normal children, and was thought not to be clinically significant.
Thigh–foot angle (photographic)
Photographic thigh–foot angle of group a was 8.18° (range −2° to 20°) and group b was 7.90° (range −1° to 20°). The difference between group a and b was not significant (p > 0.05)
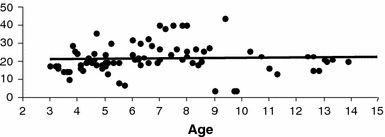
Angle of the transmalleolar axis
The photographic average was 21.59° (range 4°–44°), and was in accordance with normal child values (Fig. 4). Again, intergroup differences and differences between patients and normal children were insignificant (p > 0.05).
Angle of transmalleolar axis (photographic)
This angle's average value of group a was 21.54° (range 4°–44°) and group b was 18.83° (range 4°–40°) and differences between this two group were not significant (p > 0.05).
Foot-progression angle
The clinical average was 10.70° (range −1.2° to 29.1°) (Fig. 5). The average of all foot-progression angles as well as the average values of types according to clinical and radiological results were similar to those of normal children.
Foot-progression angle (clinic)
The clinical average value of group a was 9.55° (range −1.2 to 29.1°) and group b was 10.16° (range 1.5–23.3°). Again, differences between group a and group b children were insignificant (p > 0.05).
Discussion
It is agreed that increased femoral and acetabular anteversion resolves spontaneously in infants when normal acetabulofemoral realignment is achieved [12, 13]. In children older than 18 months, however, spontaneous resolution is rare, and some cases require surgical correction [12, 13]. Normal lower extremity rotational profiles can be expected in children with DDH who received appropriate treatment in the early period with good outcomes [3, 12, 13]. The purpose of the present study was to investigate the lower extremity rotational profiles of children with DDH who received late treatment; it was shown that average internal and external hip rotations did not significantly differ from the values of normal children. However, hips with moderate and poor outcomes had values lower than normal for both internal and external rotations. If there were an external rotation deficit or surplus alone, this outcome could be interpreted as excessive femoral anteversion. However, because both hip rotations were low and this outcome was only observed in cases with poor and moderate clinical results, we thought that it might be associated with stiffness in the hip.
The thigh–foot angle and the transmalleolar axis angle reflect tibial and hindfoot rotation [2, 4–6]. The present study shows that tibial and hindfoot rotation were normal in infants.
During childhood and adulthood, this food-progression angle exhibits very little variability, the average normal value being +10 (range −3 to 20). The average and the low–high values obtained for children with DDH were the same as those for normal children.
The most important component of the potoanatomy of DDH is increased femoral anteversion, which directly affects the lower extremity rotational profile [3]. The profile may also be altered by surgical methods implemented during therapy, particularly derotation osteotomy. We detected that lower extremity rotational profile of children with DDH who underwent derotational osteotomy did not differ from children who had open or closed reduction in whom the anteversion was not changed surgically. In our opinion, the reason for this similarity is that derotational osteotomy is correct in excessive femoral anteversion and after derotational osteotomy, these hips resemble each other where anteversion is normal.
Conclusion
It was observed that the lower extremity rotational profiles of children with DDH who received appropriate treatment did not differ significantly from those of normal children, but that internal and external hip rotations in McKay type II and IV cases were below the averages of normal hips and McKay type I and II hips. In addition, no difference was found between patients treated by derotation osteotomy and others.