
Abstract
Abstract
Purpose
Unicameral bone cysts (UBCs) are most often found when accompanied by a pathological fracture. In these cases, the doctor must determine the optimal timing for the surgery. The purpose of this study was to evaluate the outcome of immediate surgery as compared with delayed surgery in paediatric pathological fractures due to UBCs.
Methods
This retrospective study assessed the medical records of 65 patients between January 2012 and September 2016. Group A included 34 patients who underwent immediate surgery, including curettage, demineralized bone matrix and fixation with elastic stable intramedullary nailing. Group B included 31 patients who underwent the same surgery several months later. The outcome evaluations included the radiological changes, brace fixation time, cyst healing time, at the first-, third- and sixth month, and final visit.
Results
The mean brace fixation time was 26.3 days (sd 5.7) for group A and 53.8 days (sd .1) for group B (p = 0.012). According to radiological evaluations, 3/34 patients in group A and 5/31 in group B had recurrence after the first surgery. A second surgery was performed in all cases of recurrence, and all fractures were healed at the last visit. There was no significant difference in the recurrence rate between the two groups (p = 0.4631), and healing times were also similar (p = 0.6033).
Conclusion
Both the immediate and delayed surgery were safe for the treatment of UBCs with fractures. We suggest immediate surgery for shorter fixation time and early activity.
Level of evidence
IV
Keywords
Introduction
Unicameral bone cysts (UBCs), also known as simple or solitary bone cysts, usually occur on the metaphysis of the long bones. 1 Approximately 80% of these cysts are found in children aged ten to 20 years old at the proximal femur and humerus, and about 85% are first diagnosed when the patients present with pain and pathological fractures. 2 Radiographs are typically adequate for diagnosis and show UBCs as central, lytic lesions with clear borders on the metaphysis of the long bones. Larger lesions may thin the cortical bone, but there is no periosteal response or soft-tissue mass. When the child is over ten years old and the bone cyst matures, the epiphysis and lesion gradually separate, and the cyst may eventually heal and be replaced by normal bone tissues.1,2
Surgical treatment is indicated when bone cysts with pathological fractures, especially in weight-bearing areas, are associated with persistent pain and malunion such as coxa vara. There have been many treatments for UBCs. Steroid injection treatment was widely used for its low risk, low cost and rapid recovery. However, the cure rate was low, and treatments needed to be repeated many times. Curettage and autologous bone graft were used when steroid injection treatment failed; however, the recurrence rate was still as high as 40% to 80%. 3 Our study focused on the treatment combination of curettage, bone graft and elastic stable intramedullary nailing (ESIN) for internal drainage, and whether it is better to perform surgery immediately or to delay surgery for some time after the fractures are healed.
Patient and methods
Patients
This retrospective study assessed records for UBC fracture surgeries performed in our hospital between 1 January 2012 and 30 September 2016. The hospital's ethics committee approved the study. Children's guardians approved the use of the clinical data of their children in this study. Children under 18 years old diagnosed with a pathological fracture who underwent surgery due to a UBC in the humerus or femur were included. The indications for surgery included UBC diameter occupying over 50% of the bone diameter and an active UBC in the weight-bearing femur bone (inactive UBCs were included). The exclusion criteria were UBCs accompanied with other diseases, UBCs without fracture, fracture treated by other methods, age > 18 years and losing the patient during follow-up. The patients differentially diagnosed by nuclear MRI as having aneurysmal bone cysts, non-ossifying fibromas, fibrous dysplasias (especially for diaphyseal tumours), brown tumours of hyperparathyroidism and osteomyelitis were also excluded in this study. UBCs usually present as low-to-intermediate signals on T1-weighted images and a bright and homogeneous signal on T2-weighted images. A database search identified 75 patients who suffered pathological fractures with UBC. Four patients with peroneal cysts, three with radius and ulna cysts and three treated with steroid injection were excluded. In all, 65 patients were included in this study. Patients who underwent surgery immediately by curettage, demineralized bone matrix (DBM) and ESIN were assigned to group A. Patients who in whom surgery was delayed after the pathological fracture healed were assigned to group B. All patients were pathologically proven to have UBCs.
Group A included 34 patients (23 male and 11 female) and group B included 31 patients (21 male and ten female) (Table 1). The mean age was 8.30 years (sd 3.82) in group A and 8.04 years (sd 2.95) in group B (p = 0.9959). UBCs were located in the proximal humerus and proximal femur in 14 and 20 patients, respectively, in group A, and 13 and 18 patients, respectively, in group B (p = 0.9505). There were 11 active UBCs in group A and nine in group B (p = 0.7948).
Patients’ demographic data and evaluation of the surgery effect
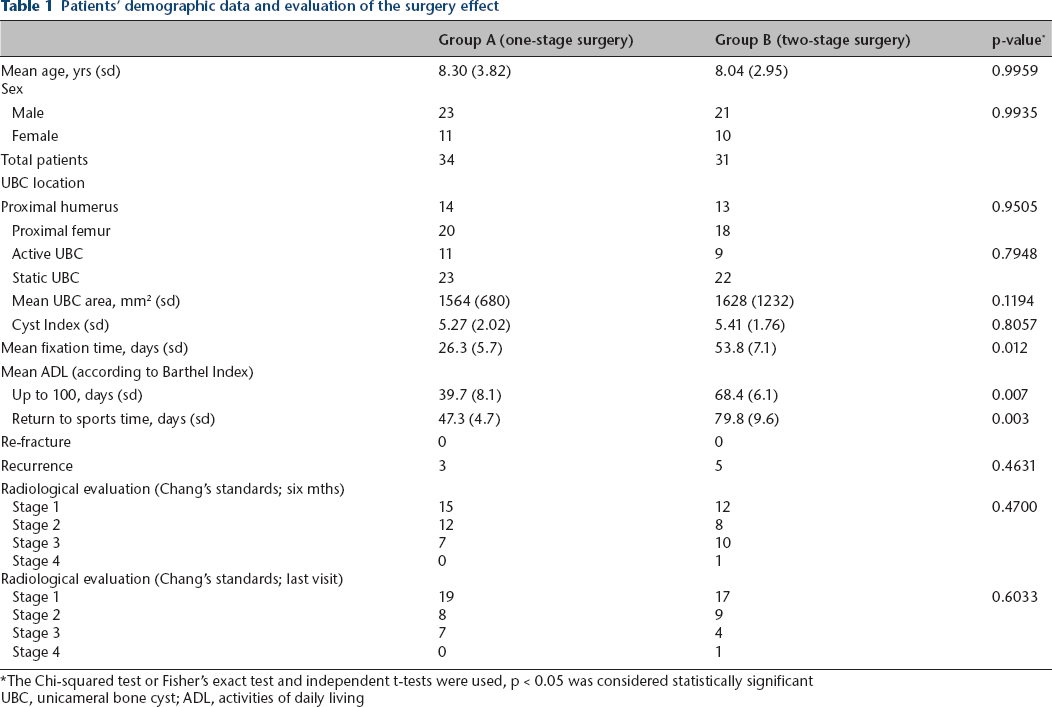
The Chi-squared test or Fisher's exact test and independent t-tests were used, p < 0.05 was considered statistically significant
UBC, unicameral bone cyst; ADL, activities of daily living
Surgical technique
All surgeries were performed by the same clinical team in the same hospital. General anaesthesia was adopted for all the patients. The surgery procedure included curettage, ESIN internal fixation and bone graft. The first step in group A was reducing the displaced pathological fractures by ESIN, according to the technique detailed by Metaizeau. 4 Preoperative anteroposterior radiographs were used for assessment of the diameter of the nails. A nail diameter approximately 40% of the medullary canal was typically used. For patients with cystic lesions abutting the proximal growth plate, the nails could be fixed across the physis for stability. The second step was curettage. After creating a cortical window at the thinnest and easiest path, curettage was performed to remove the fibrous membrane lining the cyst wall, and then the cyst wall was broken and removed. Scraped tissues were sent for pathological examination. The third step was bone grafting. DBM was used to fill in the cyst, making sure all the cavities were filled. The surgical procedure for group B was similar, with the added step of callus removal when necessary before creating a cortical window.
External fixation
All group A and B patients had their fractures fixed by braces postoperatively. The fixation time was measured by the days of the patients who were fixed by braces. The humerus was fixed by a shoulder abduction brace, and the proximal femurs were fixed by a hip chevron brace. Once the bone callus was grown enough braces were removed immediately for exercise.
Follow-up and evaluation
For group A patient exercise was started two to three weeks post-surgery, according to individual patient evaluation. For group B patients, exercise was postponed until the healing of the UBC, according to the callus growth seen on radiographs. Radiological evaluations helped assess the healing of the cyst according to the classification proposed by Chang et al. 5 Chang's standard was defined as: Grade 1 (healed), which was cyst filled by the formation of new bone with or without a small, static, radiolucent area < 1 cm in size; Grade 2 (healing with defect), which was the presence of a static, radiolucent area less than 50% of the diameter of the bone with enough cortical thickness to prevent fracture; Grade 3 (persistent cyst), which was the presence of a radiolucent area > 50% of the diameter of the bone and with a thin cortical rim; Grade 4 (recurrent cyst), which was cyst reappearing in a previously obliterated area or a residual radiolucent area increasing in size. If the pathological fracture reoccurred or no improvement was seen on the radiographs after six months (Chang's Grade 3 or 4), the treatment was considered as failed. The area of the cyst was defined as the square of the diaphysis diameter on anteroposterior radiographs. 6 Both groups were evaluated postoperatively at two weeks and at one, three, six, 12 and 24 months, including the last visit within this period.
Each evaluation included clinical and radiological examinations. Clinical evaluation included assessment of complications such as pain and interference with daily life activities. We adopted the Barthel Index of Activities of Daily Living (ADL) as the evaluation method. 7 It assesses a person's ability to perform feeding, transfers, personal grooming and hygiene, toileting, walking, negotiating stairs and controlling bowel and bladder functions. A score of 100 means the total recovery of ADL. In this study, the time (days) required to achieve a score of 100 in patients who did was recorded.
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics for Windows, version 20 (IBM Corp., Armonk, New York). Chi-squared tests and independent t-tests were used to compare continuous and categorical variables, respectively. A two-tailed p-value < 0.05 was considered statistically significant.
Results
In all, 54 patients attended follow-up visits for at least 24 months. The duration of follow-up ranged from 24 to 37 months (mean 30.7). Table 1 shows the detailed patient characteristics at presentation. Table 2 shows the detailed information about the lower limbs. Radiographs representative for patients in groups A and B are shown in Figures 1 and 2, respectively. In group A, 14 patients had UBCs in the proximal humerus and 20 had UBCs in the proximal femur. A total of 13 patients in group B had UBCs in the proximal humerus and 18 patients had UBCs in the proximal femur. There was no significant difference in the UBC site between these two groups (p = 0.9505). There was also no difference between the number of active and static UBCs, with 11 active and 23 static UBCs in group A and 9 active and 22 static UBCs in group B (p = 0.7948). The UBC mean area was 1564 mm2 (sd 680) in group A and 1828 (sd 1232) in group B, and there was no significant difference between these groups (p = 0.1194). The Cyst Index (CI) was the ratio of the projected surface to the square of the diaphyseal bone diameter. 8 The mean CI in group A was 5.27 (sd 2.02) and it was 5.41 (sd 1.76) in group B, and there was no significant difference between these groups (p = 0.8057).
Evaluation of the surgery effect in 38 patients with proximal femur unicameral bone cysts
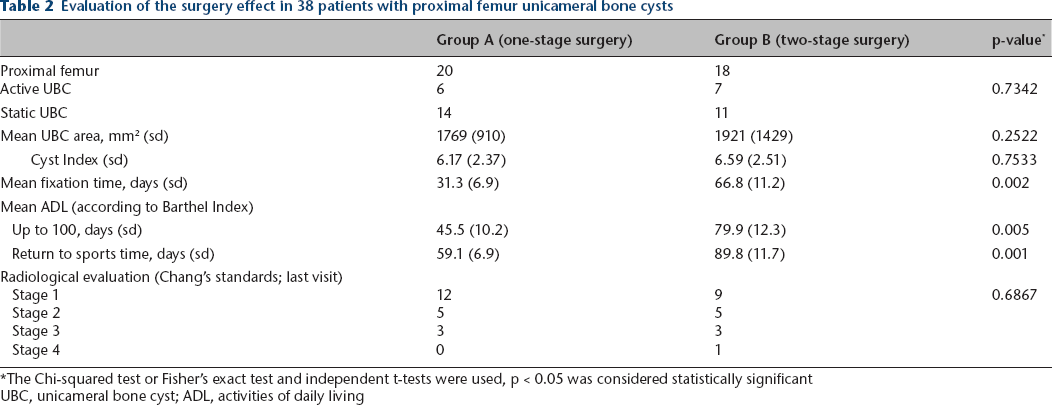
The Chi-squared test or Fisher's exact test and independent t-tests were used, p < 0.05 was considered statistically significant
UBC, unicameral bone cyst; ADL, activities of daily living

A seven-year-old boy with a pathological fracture of the left proximal femur (group A):
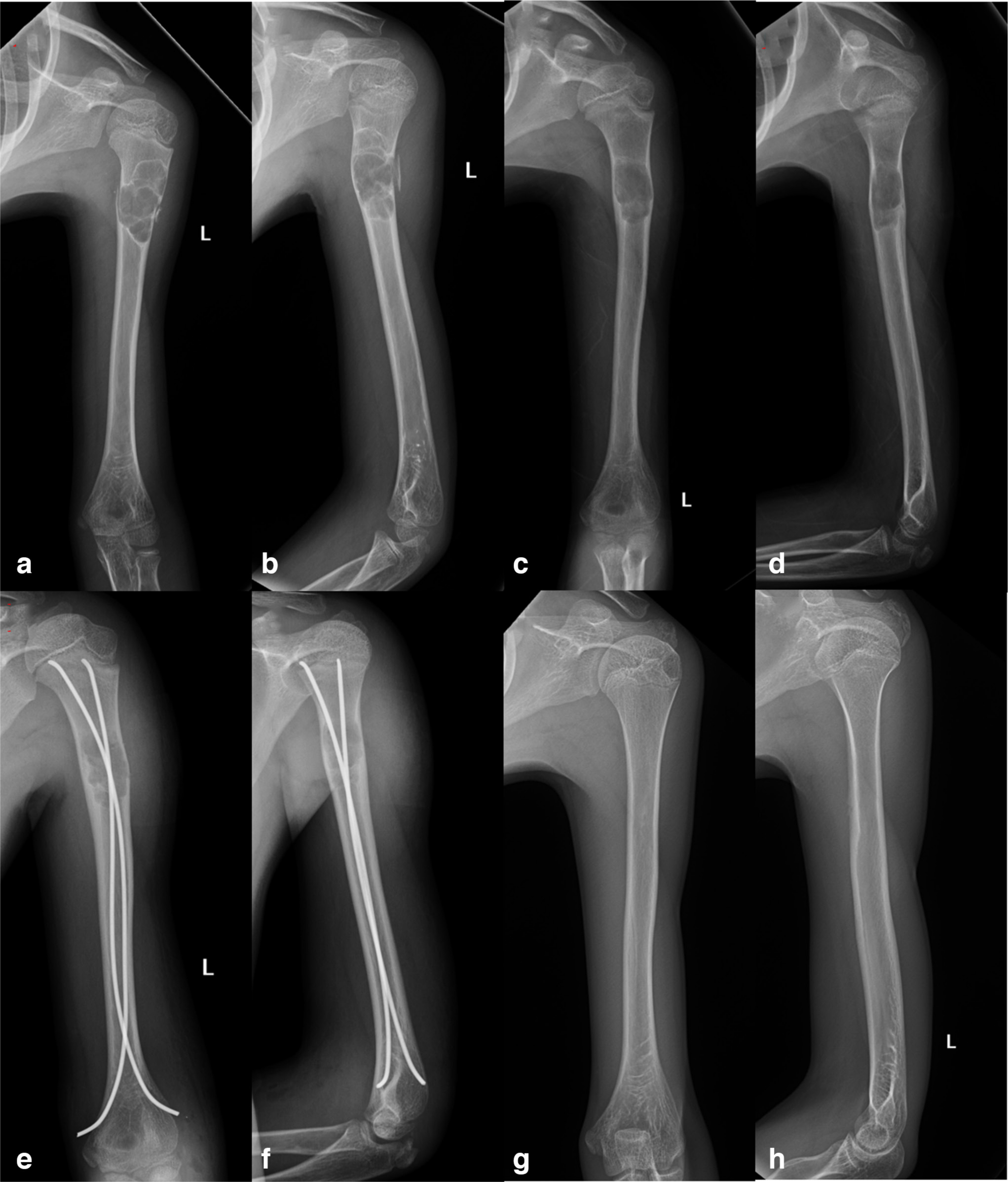
A ten-year-old boy with a pathological fracture of the left proximal femur. (group B):
There was a significant difference in brace fixation time between these two groups, with a mean duration of 26.3 days (sd 5.7) in group A and 43.8 days (sd 7.1) in group B (p = 0.0012). No refracture occurred in both groups. No patient had pain in either group on the last visit. Regarding the lower limbs, there was also a significant difference between the two groups (Table 2).
At the six-month follow-up, 27/34 group A patients and 20/31 group B patients had acquired good results on radiological evaluation according to Chang's standards. No significant difference was found between both groups (p = 0.4700). On the last visit (> 24 months), 27/34 patients acquired good results in group A and 26/31 patients acquired good results in group B; no significant difference was found between these groups (p = 0.6033). Only one patient in Group B showed no improvement after the operation. The patient underwent curettage and bone graft two more times and finally recovered.
Discussion
Treatment of UBC is controversial, and no single treatment can achieve ideal results. 1 There are several major concerns regarding the management of pathological fractures from UBCs. UBC is a benign pathological lesion, and its aetiology remains uncertain. The most accepted theory is mechanical trauma and venous obstruction of the bone. UBCs may show no clinical symptoms, so they may not be discovered and may not affect quality of life. According to some scholars, UBCs may heal naturally as the child grows. 2 However, in most cases, the patients are usually diagnosed when presenting with pathological fractures.8,9 Patients who received conservative treatment were not included in this study. In our clinical centre, patients with inactive UBCs (> 12 years old, separated from physis by a zone of normal cancellous bone, multiloculated cavity, thick membrane, frequent giant cells, cholesterol slits, hemosiderin and osteoblasts) were encouraged to undergo conservative treatment. Active cysts are close to the physeal line. For active UBCs in the weight-bearing femur bone, patients were encouraged to undergo surgery. The physicians determined if the child needed surgery immediately or if the repair should be postponed. The second dilemma is the choice of surgical procedure.
There are many surgical methods in the literature. These include conservative treatment, bone grafting, curettage and bone grafting, decompression with drill holes, cannulated screws, 10 ESIN,10–12 percutaneous injection of steroids, 13 bone substitutes,12,14 DBM 3 and bone marrow aspiration. 3 Our operation procedure includes curettage, which helps to eliminate the inner membrane wall of the UBC, which is the source of the cyst fluid and destructive enzymes, as well as ESIN, which is a method for internal drainage of the cyst. Decompression of the cyst and an injection of steroid or osteogenic materials are also important. In our study, we used DBM, which has recently served as a bone substitute in many orthopaedic fields with favourable results. 14 Some studies reported deep vein thrombosis from the allogeneic bone treatment of UBCs; 15 however, in our study, there were no thrombosis complications. Although the detailed mechanism needs more study, our method showed high healing rates with low recurrence of pathological fractures caused by UBC.
In 1981, Catier et al 16 first reported ESIN for the treatment of UBC in two patients. Knorr et al 17 and Santori et al 18 then reported successful treatment of their patients. Roposch et al 19 reported 32 simple bone cyst cases with pathological fractures that were treated by ESIN; 94% (30/32) achieved ideal results and only two patients needed a second operation. The recurrence rate was 6%. A retrospective series of 116 cases using ESIN, curettage and calcium phosphate cement showed healing in 113/116 patients. 11 Most studies in the literature show that ESIN yields an ideal result. In this study, ESIN facilitated internal drainage and decompression of the UBC and contributed positively to cyst healing. ESIN also provided internal fixation of the pathological fractures and helped the patients walk in the early stages of recovery. Another reason we chose ESIN was that all the patients were young children who weighed < 50 kg. There is some concern about internal fixation using ESIN causing tumour dissemination to the surrounding area. In this study, those we treated were all diagnosed with typical UBCs, which were benign tumours that could not be disseminated. The follow-up results proved that ESIN was safe.
Conversely, Norman-Taylor et al 20 proposed nonsurgical treatment in pathological fractures due to UBCs. Even patients with refracture after initial presentation with displacement achieved union but there were some major complications such as coxa vara and femoral head necrosis. Norman-Taylor et al 20 concluded that the initial fractures needed significant time to heal, as well as other therapies such as steroid injections or DBM grafts, and even with these methods, recurrence and refractures were more frequent, leading to coxa vara and a short limb length. In this study, we demonstrated that surgical treatment for all patients with pathological fractures is much safer and is accompanied by fewer complications, especially when the UBC occurs in the femur (Table 2).
Many surgeons worry about the risk of early operation and whether the patient will heal after curettage, bone graft and ESIN fixation; hence, they prefer to postpone the surgery and choose conservative treatment, such as fixation by brace or splint. Some surgeons prefer to operate after bone callus growth, as the fractures are more stable, and the operation seems much easier. However, this study demonstrated that the fixation time was significantly longer in patients who had delayed surgery than in those who had early surgery. It was also noted that a lengthy delay in fixation was disturbing for children from our clinical experience. A comparison of the complications in this study proved that early operation, including curettage, bone graft and ESIN, could achieve the same results as a delayed operation. Erol et al 21 also reported that a very similar combination treatment of curettage, grafting and ESIN, achieved a high cure rate in humerus UBCs. The extended curettage and grafting stimulated bone formation and ESIN not only contributed to continuous drainage of the cyst but also provided stability to the pathological fractures. 21
Finally, open surgery allows full observation of the cavity of the cyst, ensuring that adequate allograft bone is used to fill the cavity, because insufficient allograft bone may lead to inadequate healing of the UBC and eventual recurrence. 14 Another advantage of open surgery is the opportunity to perform a confirmatory biopsy. The differential diagnosis of UBC includes aneurismal bone cyst, fibrous dysplasia, non-ossifying fibroma, giant cell tumour and more critically osteosarcoma and Ewing's sarcoma. There was a significant difference in the brace fixation time, ADL time and return to sports time between these two groups, especially for the femur UBCs (Table 1 and Table 2). The main reason is that the delayed operation needed two separate periods for bone healing, the first is during pathological fracture when it happened and the second is after a delayed operation; brace fixation was also needed postoperatively.
UBCs located in weight-bearing lower limbs were much more important for patients ADL. Many studies focused on different fixation methods depending on the location of the UBC lesion.4,15,20 Pathological fractures associated with UBCs in the proximal femur are often accompanied by malunion, growth arrest, coxa vara, coxa valga and avascular necrosis. In this study, we used ESIN combined with DBM for the treatment of UBCs in the proximal femur. There was also no significant difference in the healing of UBCs between the two groups in this study, but there was a significant difference in the ADL, fixation time and return to sports time between the two groups (Table 2). However, longer follow-up time for complications such as coxa vara, coxa valga and avascular necrosis is required in further studies.
This study has some limitations. Primarily, the retrospective design is susceptible to bias compared with a prospective design. Further, our patient sample was small, and comparisons with other methods are required to assess the outcomes of our approach. Further studies might add control groups with treatments such as steroid injection, cannulated screws, bone marrow injection or percutaneous minimally invasive surgery for comparative analysis. Again, a longer follow-up time is needed to observe the recurrence of UBCs radiologically, especially for juvenile patients. Finally, we used the most aggressive treatment method, including curettage, allograft and ESIN fixation. As the aetiology of UBC becomes clearer, a much safer mini surgery may replace our method.
Conclusion
Both the immediate and delayed treatment with curettage, allograft and fixation with ESIN are safe surgical methods for UBC with pathological fractures. However, early surgical treatment may result in shorter fixation time without any increase in adverse events or recurrence. We suggest immediate surgery for a shorter fixation time and early activity.
Footnotes
Acknowledgements
Chongqing Science and Technology Commission (cstc2017jcyjAX0010, cstc2018jcyjAX0143). Chongqing Health and Family Planning Commission with Science and Technology Commission (2019MSXM081). The Fifth batch of outstanding talents support program for universities in Chongqing Natural Science (2017-29). National Natural Science Foundation of China (81001197).
KC: Participated in its design, drafted the manuscript.
YS: Conceived the study, draft the manuscript, read and approved the final manuscript.