
Abstract
Abstract
Purpose
By means of a case series we wanted to describe and correlate the clinical and imaging features of bone marrow oedema syndrome (BMOS) of the foot and ankle in children.
Methods
A retrospective data study was performed on patients born on or after 01 January 2001 who underwent multiple MRI scans of the foot and ankle for pain symptoms. Six patients who presented with increased signal intensity on T2-weighted MR imaging without any underlying causes or concomitant pathology were included.
Results
All patients, three boys and three girls with a mean age of 11 years (8 to 14), displayed patchy areas of increased signal intensity on T2-weighted and turbo inversion recovery magnitude (TIRM) images. On average, six tarsal bones were involved (4 to 8). In all patients, treatment consisted of rest and/or protected weight-bearing. The mean time for symptoms to improve during treatment was 6 months (1 to 16). The mean duration of treatment was nine months (3 to 16). In all patients clinical and imaging symptoms were strongly correlated and regressed in time.
Conclusion
BMOS as a pathological entity should be considered in paediatric patients with foot and ankle pain without a clear underlying cause, and characteristic T2-weighted and TIRM signal intensity increase on MRI images. As BMOS is transient and self-limiting, conservative treatment is advised while the oedema regresses. An early diagnosis of this pathology could prevent unnecessary diagnostic investigations and invasive treatments.
Level of Evidence
IV
Introduction
Bone marrow oedema syndrome (BMOS) refers to a group of conditions characterized by extremity pain and increased interstitial fluid within the bone marrow, with unknown cause.1–4 First used as a general term in knee pathology by Hofmann et al in 2004, 1 it has been described as acute bone marrow oedema, bone marrow lesions, (migratory) transient osteoporosis, regional migratory osteoporosis and transient bone marrow oedema (TBMO). 5 It is a relatively rare condition, not often described for the upper limb or in the paediatric population, 5 mostly affecting the hip and knee in middle aged men and younger women.3,6 Because foot and ankle involvement in BMOS is quite uncommon, and has rather unspecific symptoms, there is often a delay in diagnosis, which leads to an extended period of pain and impaired functionality in daily life.1-3,7-9 BMOS is characterized by a self-limiting course as the symptoms usually disappear within three to 12 months.10,11 Treatment of BMOS focusses on pain relief and shortening of symptom duration if possible.1,3 Symptomatic treatments can consist of non- or partial weight-bearing by means of a cast or walker boot, nonsteroidal anti-inflammatory drugs, calcium, calcitonin, physio-, relaxation and massage therapy.2,3,12-16 Pharmacological treatments include iloprost, a synthetic prostacyclin analogue9,11,17-23 bisphosphonates and vitamin D.2,7,24-28 Surgical treatment consisting of core decompression or drilling have mostly been described in the proximal femur.22,29
Only a few case reports have been published concerning BMOS in the paediatric population.16,30-33 In imaging studies, which are focused on tarsal bone marrow in children, high-signal T2-weighted changes of the bone marrow on MRI are mostly considered to be a normal, physiological finding representing residual hematopoietic marrow instead of a pathologic entity.34–37 A limitation of many of these studies is the lack of clinical data and thus the absence of a correlation between MRI findings and the clinical evaluation.
In this study we would like to re-evaluate the underdiagnosed concept of BMOS in the foot and ankle in a paediatric population. By means of a case series we observe the correlation between clinical symptoms and MRI imaging features.
Materials and methods
A retrospective database search was conducted using image viewing software (CARESTREAM Vue PACS, Carestream Health Inc., Rochester, New York, USA), querying MRI scans of the foot and ankle in a population born on or after 1 January 2001. Only patient cases of children who had multiple MRI scans were included (21 cases in total). Images and protocols were scrutinized by the first author (HDH). In total, 12 cases were selected for this study based on MRI susceptibility for BMOS. We excluded fractures, osteochondral lesions, tarsal coalitions, tendon pathology, inflammatory and infectious disease and malignancies, as these diagnoses could generate a secondary bone marrow oedema image. Patients with imaging but no clinical data records were also excluded. The following data was recorded from patient files: sex, date of birth, medical history, affected side, history of trauma to the affected limb, previous treatments, date of first clinical visit, duration of symptoms before diagnosis, anamnestic symptoms, clinical symptoms, type and duration of treatment, date of amelioration of symptoms, recurrence of symptoms and length of follow-up. These clinical data were reviewed by the first author (HDH), who was not involved in the clinical care of these patients. For the imaging data, the date of the first pathological MRI, the date of improvement of MRI features and localization of the bone marrow oedema were recorded. All images of the selected cases were reviewed by the first author and a specialist musculoskeletal radiologist (JDR). After reviewing the remaining cases, six cases were excluded because of discrete subchondral fracture lines (three) and merely physiological appearance of the bone marrow oedema pattern (three). MRI scans in our hospital were performed on a 1.5-tesla magnet MRI (Siemens Medical Systems, Erlangen, Germany) and two review scans were executed in another hospital. The standard MRI technique used in our hospital for ankle imaging included coronal, sagittal and axial T1-weighted sequences, axial T2-weighted sequences and sagittal turbo inversion recovery magnitude (TIRM), T2 3D-double-echo steady state with water excitation and T2-weighted sequences. In total six patient cases are discussed in this article.
In addition to the first query, a second query was performed on the same patient population to provide a control group. Patient cases of children with single or multiple MRI scans were selected and imaging protocols were scrutinized. Patient cases with imaging protocols susceptible for BMOS were excluded. In total, ten cases were included in the control group, two cases featuring bilateral MRI imaging. The following data was recorded from patient files: sex, date of birth, date of the MRI, medical history, history of trauma to the affected limb, anamnestic and clinical symptoms, diagnosis and treatment. MRI images of the selected cases were reviewed by the first author (HDH) and a specialist in musculoskeletal radiology (JDR).
Descriptive statistics were performed using Excel (Microsoft Excel 2016, Redmond, Washington, USA). No comparative tests were performed.
Results
Demographics
Full demographic and clinical data are listed in Table 1. We reviewed three male and three female patients in total. Only one patient (case 1) presented with a medical history of Immunoglobulin A vasculitis (Henoch-Schönlein purpura) and Hashimoto thyroiditis. The mean age at presentation of symptoms was 11 years (8 to 14) and the mean follow-up was one year and one month (5 months to 2 years 1 month). All patients presented with unilateral symptoms.
Demographic and clinical features
Clinical features and disease course
In all children, no report of hip-or knee-related pathology was noted. Three children presented with a minor trauma prior to the symptoms necessitating consultation, consisting of an ankle sprain in one patient and an undisplaced metatarsal fracture at least three months prior to first presentation in two other patients, as detailed in Table 1. In all patients, the prior trauma was treated by another physician, before consulting a foot and ankle surgeon at our clinic.
The average duration of symptoms before the first visit was six months (1 to 15). Three patients presented with a history of pain solely during sports. The other three patients complained of pain during stance and walking, with one patient unable to support their weight on the affected limb at first presentation. Two patients presented with swelling, one with isolated swelling of the ankle and one with swelling of both the ankle and hindfoot. The patient with a history of inflammatory diseases showed no localized joint inflammation, thus no joint aspiration or rheumatological investigation was performed. There was no report of skin colour, temperature or texture changes, nor of muscle atrophy or allodynia. On clinical examination, two children showed decreased passive mobilization of the hindfoot. No clinical ankle instability was reported in these children. In four patients, the pain was localized to the sinus tarsi, in one patient at the navicular bone and in one patient at the lateral mid- and hindfoot (Table 1).
Relative rest and restricted weight-bearing as tolerated were advised to all patients. Two patients (cases 3 and 6) did not receive any additional treatment aids. Orthotic insoles were prescribed for two patients (cases 1 and 2). A weight-bearing short leg cast was used as a protective aid in three cases (cases 2, 4 and 5) for four weeks (Table 1).
The average time for initial symptoms to improve during treatment was six months (2 to 15). Two patients had recurrent symptoms after initial improvement (cases 1 and 4) (Fig. 1). Another patient (case 5) demonstrated a prolonged disease course with stagnation of pain. Only one patient (case 2) showed clear migration of clinical symptoms (Fig. 2). Mean duration of treatment was nine months (3 to 15). Eventually all children were able to return to their daily activity and premorbid sports level, with a complete resolution of all symptoms.
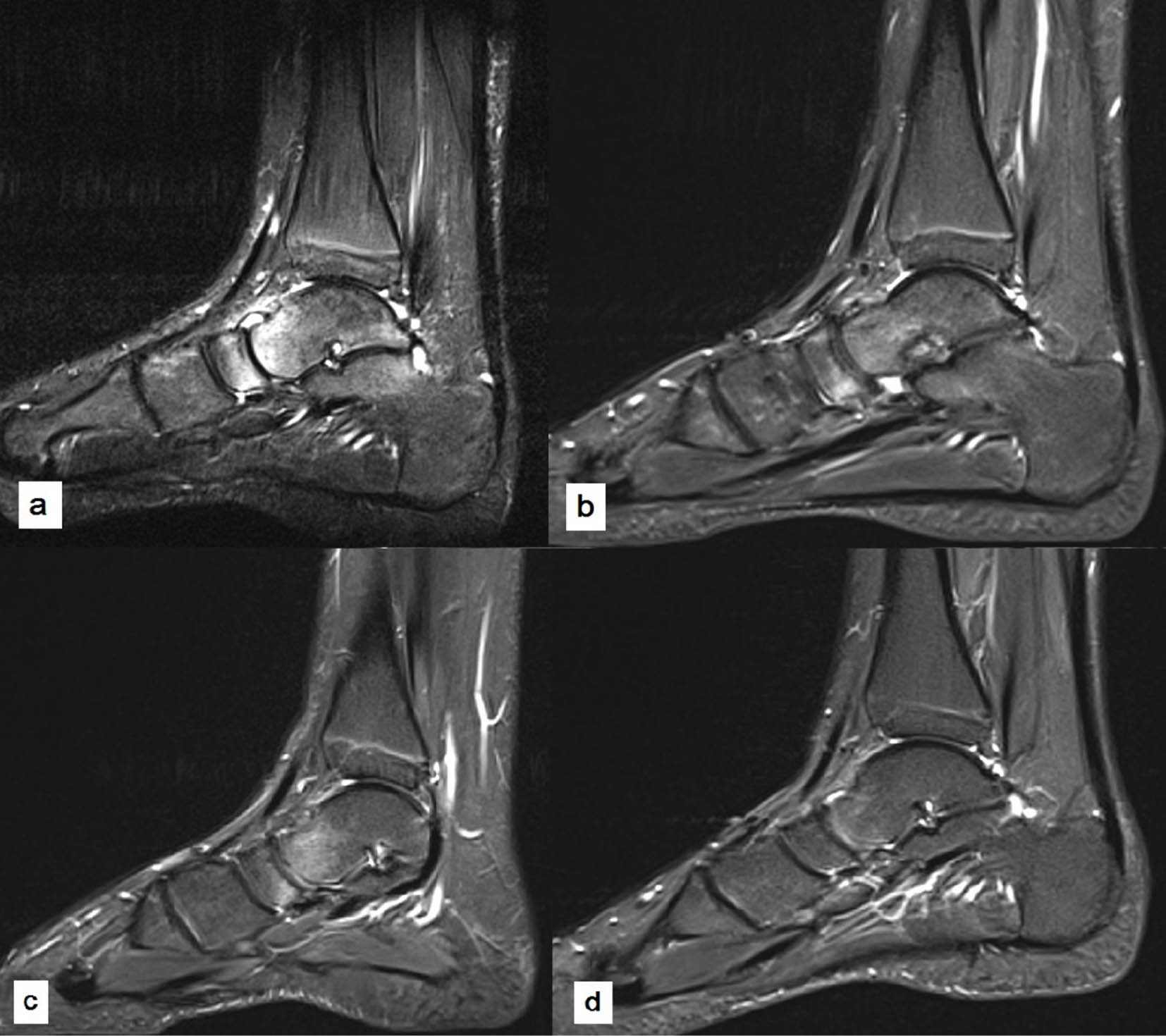
A recurrent disease course was seen in this 14-year-old boy (case 4), as documented by turbo inversion recovery magnitude sagittal MR imaging. Presenting initially with pain in the tibiotalar and subtalar joint and bone marrow oedema appearing to be centred in the talonavicular joint
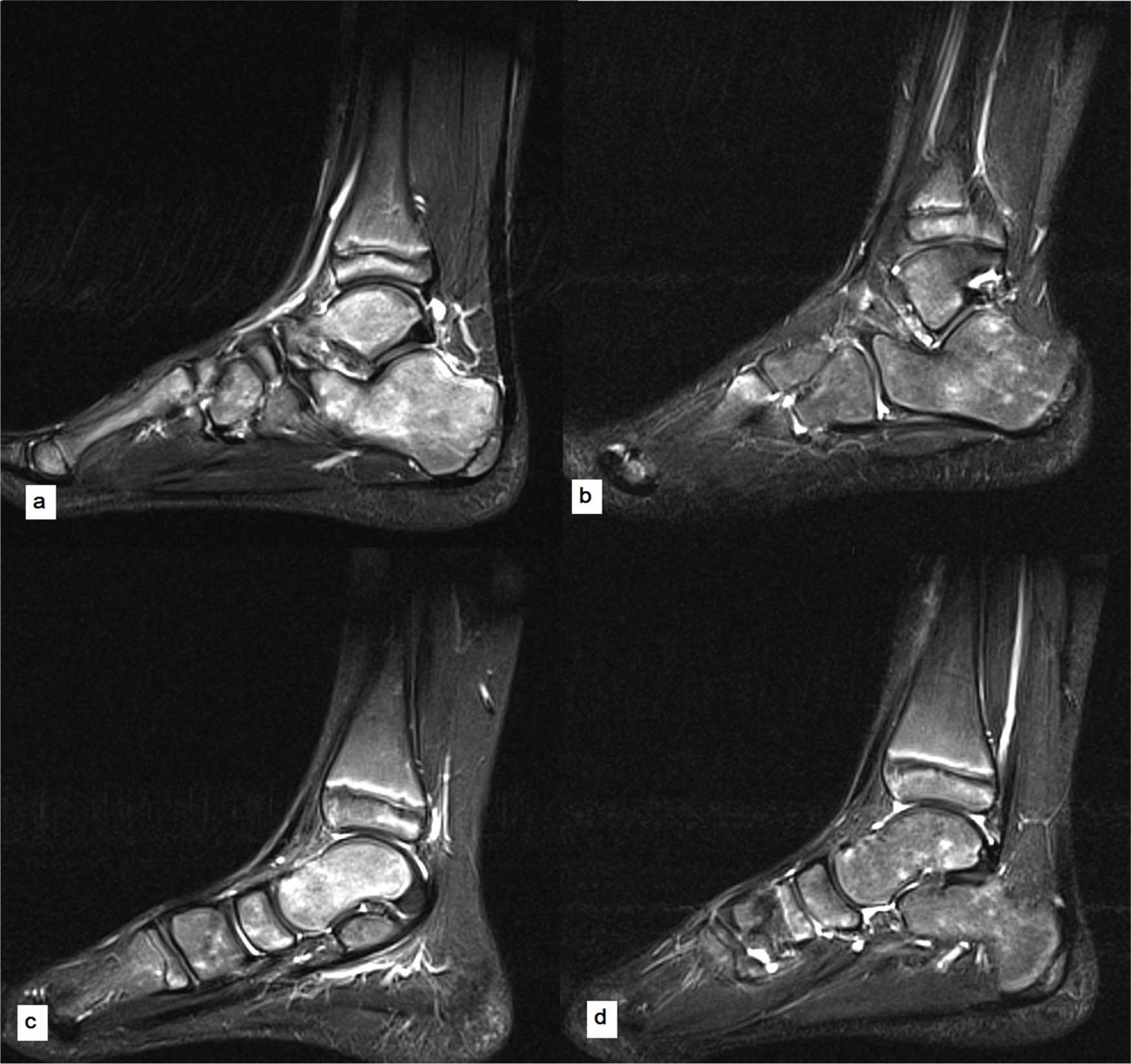
Sagittal turbo inversion recovery magnitude MR imaging sequences of an eight-year-old boy (case 2), performed for atraumatic pain in the sinus tarsi on weight-bearing initially
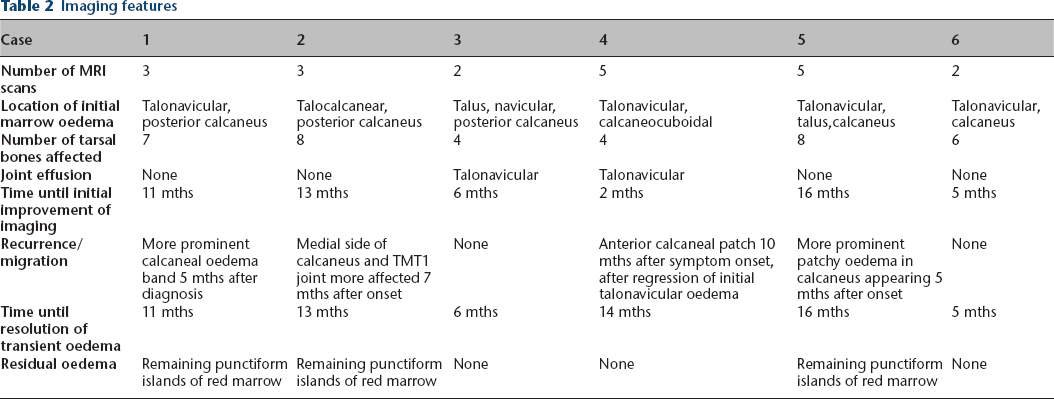
Imaging features
All imaging features are summarized in Table 2. All patients had at least two MRI scans, and two patients (case 4 and 5) had up to five. In all patients, MRI images showed the presence of patchy areas of increased signal intensity on T2-weighted and TIRM images, with a decreased signal intensity on T1-weighted sequences (Fig. 3). On average, six tarsal bones were involved (4 to 8). The main localization of these patches was in the talar neck and navicular bone (100%). A second important localization was the posterior portion of the calcaneus, observed in five children (83%), where in four of these patients a similar bow-shaped area of increased intensity was observed (Fig. 4). No apophyseal involvement in the calcaneus was reported. In two patients (cases 3 and 4) the presence of talonavicular joint fluid was observed. No patient showed any tendon or ligament injury or pathology, nor other imaging features associated with chronic ankle instability (such as anterolateral impingement signs, anterior talofibular ligament avulsions, peroneal injuries or synovitis, peroneal retinaculum pathology or talar osteochondral lesions). 38

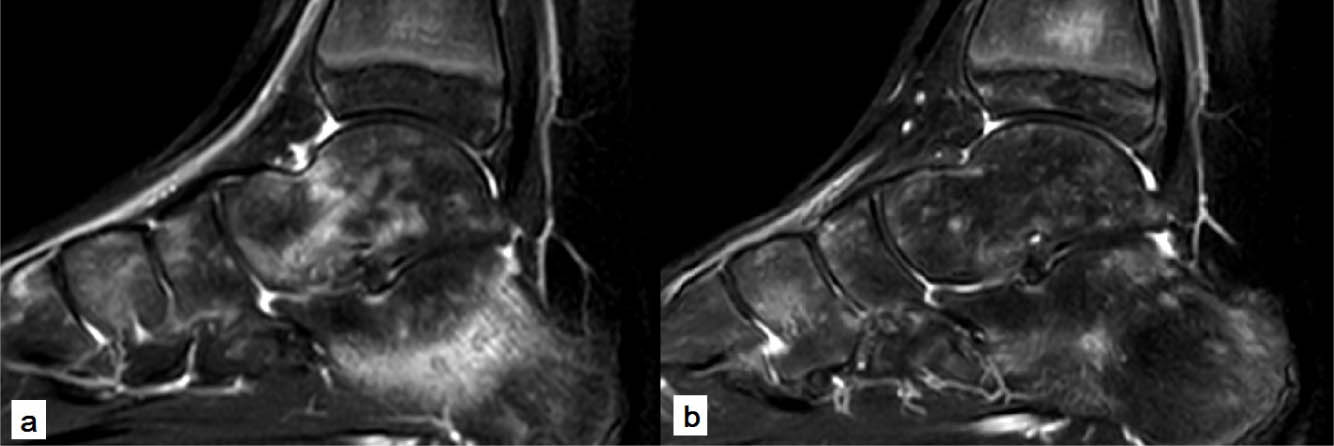
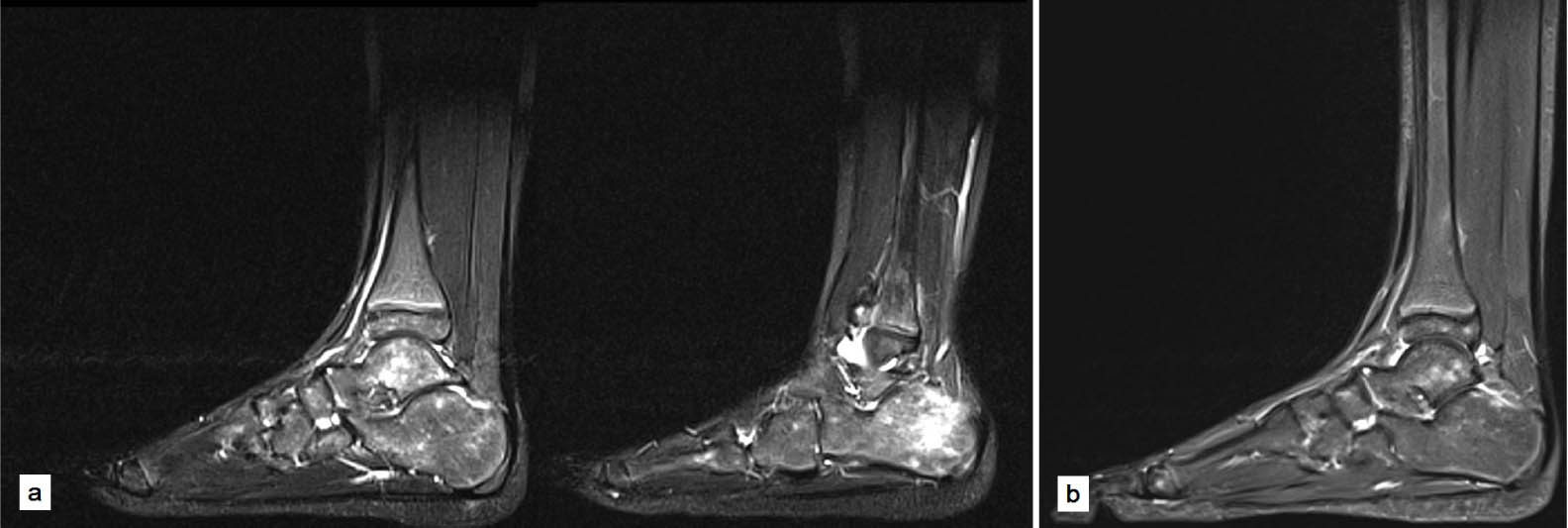
MR imaging on diagnosis of bone marrow oedema syndrome in a ten-year-old boy (case 6) with pain in the sinus tarsi area, showing characteristic findings of increased signal intensity on turbo inversion recovery magnitude
Nine-year-old girl (case 1) presenting initially with pain localized to the sinus tarsi area, with T2-w MR imaging showing patchy areas of increased signal intensity at the anterior talar body and bow-shaped at the midportion of the calcaneus
Imaging features
In all patients, a concurrent amelioration of clinical symptoms with a regression of the patchy bone marrow oedema was observed. In multiple cases, persistent diffuse punctiform increase in signal intensity was found on MRI images, with regression of the patchy areas and absence of symptoms (Fig. 5).
Turbo inversion recovery magnitude sequencing sagittal images of the foot and ankle in an eight-year-old girl (case 5) presenting with pain on the lateral aspect of the mid- and hindfoot, unable to bear weight at initial diagnosis
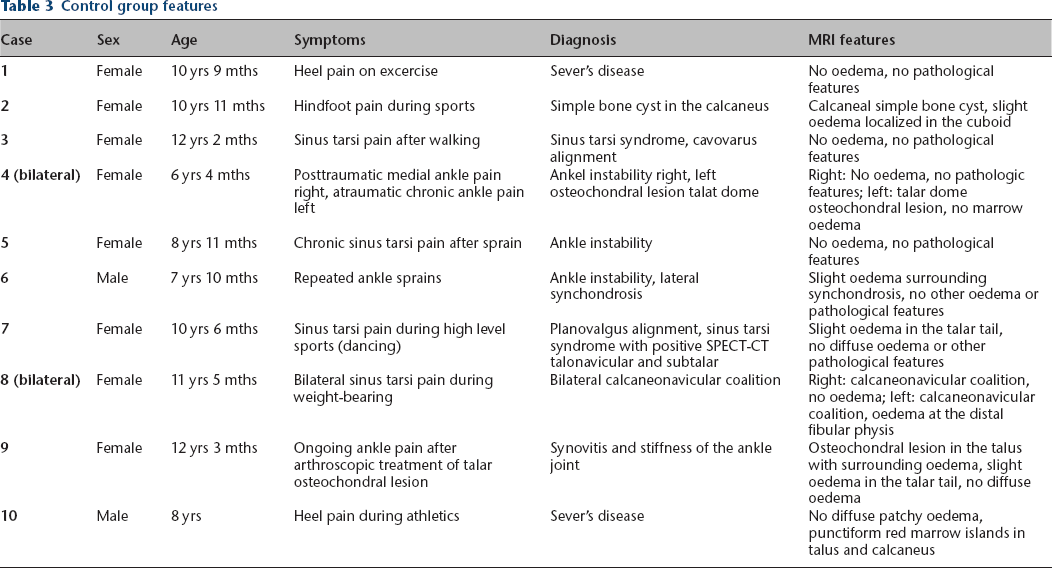
Control group
In order to provide a control group, ten patients undergoing MRI imaging of the foot and ankle for different diagnoses were reviewed. This group comprised two male and eight female children, with a mean age of nine years (6 to 12). All clinical and imaging features of these cases are summarized in Table 3. None of these children had a significant medical history. Two children were diagnosed with Sever's disease, another two children showed a sinus tarsi syndrome, based on planovalgus in one and repetitive hindfoot stress in the other child. Two cases were diagnosed with ankle instability, one child demonstrated a simple bone cyst in the calcaneus. One patient was diagnosed with ankle synovitis and a slow rehabilitation after arthroscopic treatment of an osteochondral lesion at the talar dome. Two children featured bilateral ankle MRI imaging, one being diagnosed with ankle instability on one side, and an osteochondral talar lesion on the contralateral ankle. The other child had a bilateral symptomatic calcaneonavicular coalition. None of the MRI images in these cases showed the presence of patchy areas of increased signal intensity on T2-weighted and TIRM images (example in Fig. 6). One child of eight years old showed small punctiform increased signal intensity foci in the posterolateral talus and posterior calcaneum, suggesting physiological residual islands of red bone marrow with a clinical diagnosis of Sever's disease.
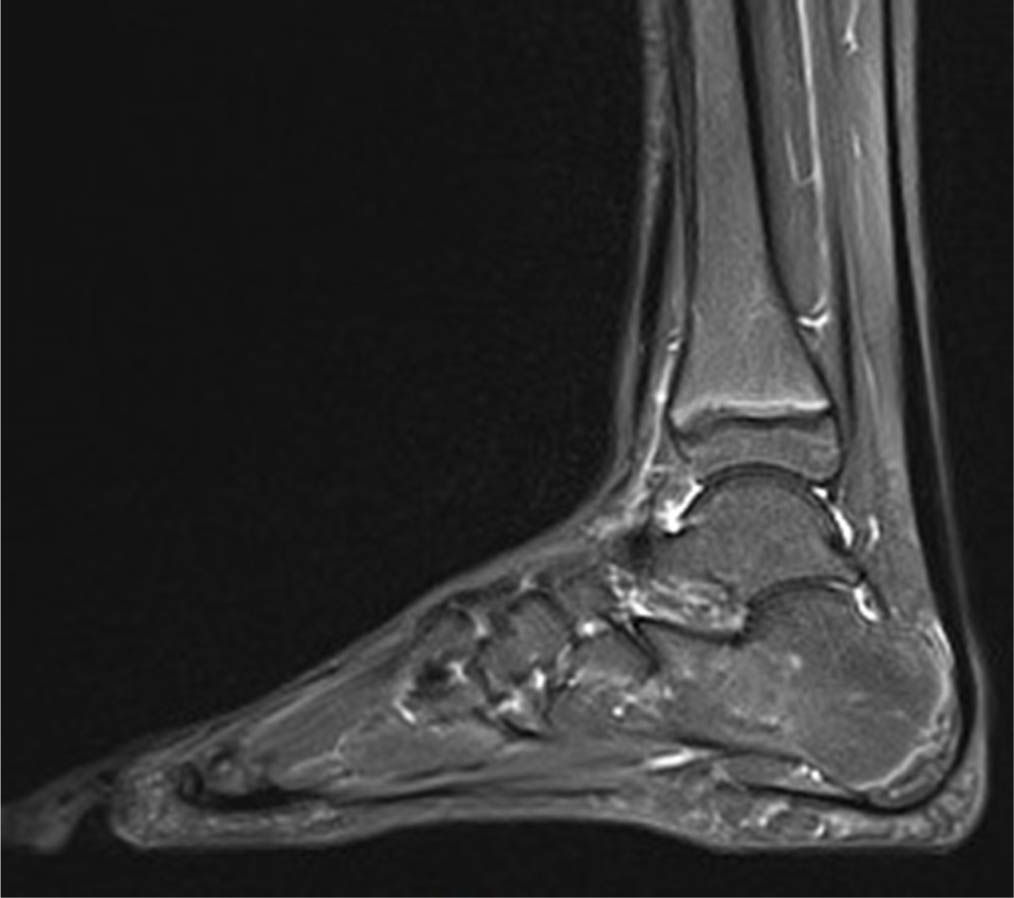
Sagittal turbo inversion recovery magnitude sequencing image of the foot and ankle in a 12-year-old girl (control group case 3) diagnosed with a sinus tarsi syndrome and cavovarus alignment after presenting with pain in the sinus tarsi area after walking. MRI imaging shows no pathological features and no patchy oedema in the tarsus.
Control group features
Discussion
In this study we describe six paediatric patients with BMOS of the foot and ankle. The ages of the patients varied between eight and 14 years. To our knowledge, this is the first case series to be described in an exclusively skeletally immature population, where clinical data shows a similar course as imaging features.
Few articles have been published concerning TBMO in children. In 2002, Aigner et al 31 reported a case of TBMO in the acetabulum of a 15-year-old girl, which was successfully treated by iloprost. MRI imaging showed a characteristic low-intensity signal in T1-weighted and an increased signal in T2-weighted sequences. Both sequences normalized three months after treatment. Kröger et al (2004) 32 described the case of an eight-year-old boy suffering from TBME in both hands and feet. MRI imaging of both joints showed BMOS, yet radiographic examination showed marked osteopenia in the tarsal area, making the diagnosis of transient osteoporosis more likely. No biopsy was performed to confirm the diagnosis of osteoporosis, and a spontaneous improvement of symptoms was observed within three months. In 2010, Orr et al 16 reported a case series of 14 juvenile and young adult patients with prolonged, atraumatic foot and ankle pain, showing characteristic imaging features on MRI. Follow-up MRI imaging was performed for four patients. Three patients showed an improvement in marrow intensity which could be correlated to their clinical improvement. One patient, who showed a prolonged symptom duration, had no improvement in MRI imaging. Two studies have suggested that the focal high intensity areas on T2 or STIR image sequences in foot and ankle MRI imaging in children could be physiological, due to residual red bone marrow.34,37 However, these imaging studies did not correlate the imaging data to the clinical data.
Reports of BMOS of the foot and ankle in adults often describe a unique localization of bone marrow oedema8,11,23,39-41 as well as more diffuse patterns of the affected bones.2,12,14,16,42 Most often and most prominently involved is the talus, which is also observed in our series. Typical findings of BMOS include migration of the oedema pattern and a recurrence of symptoms. 40 The migratory character could be explained by recurring ischemic events in vessels. 4 Migration of marrow oedema can occur within the tarsus, or to other joints often diagnosed with BMOS such as the hip or knee joint.2,8,12 In our case series two children showed a migratory pattern of oedema within the tarsus, one of them after improvement of initial symptoms (case 4). In adult BMOS patients follow-up MRI imaging shows an overall improvement in T2-weighted sequence intensity corresponding to an amelioration of pain.15,18,25,39,43,44 Several studies have reported an (incomplete) resolution of marrow oedema after treatment but these studies made no connection to symptomatic findings.7,17,19,22,23,41 In 23% of BMOS patients a recurrence of symptoms can be seen when the foot and ankle are affected, often after an average time interval of eight months.2,11,13,14 Singh et al 2 reported a recurrence rate of 44% within the ipsilateral foot with a mean follow-up of 15.6 months. In our patient group we had one patient (case 4) with recurrent BMOS symptoms at another site within the tarsal bones, returning eight months after symptom and oedema regression in T2-weighted MRI sequences. Another patient showed a prolonged disease course, with symptoms and MRI images taking up to 16 months to improve.
Three of our patients presented after a minor trauma several months before initial imaging. In a paediatric population minor trauma should be considered to be part of the daily life of playing children, and should not be expected to lead to such fulminant osseous reaction patterns. Some authors suggest TBMO to be one of several possible terms for a pathology also comprising algodystrophy or complex regional pain syndrome, 3 however, none of our cases demonstrated typical clinical signs of algodystrophy, such as skin or vasomotor changes, or muscle atrophy. Common diagnoses to be ruled out at this age are Sever's disease or ankle instability, of which none of our patients showed clinical or radiological findings.
The pathophysiology of BMOS remains discussed up until today. Risk factors of BMOS are chemo- or radiotherapy, corticosteroid therapy, alcohol or nicotine abuse, (micro)trauma, sickle cell anaemia, lipid metabolism disorders, rheumatic diseases or vitamin C deficiency.3,8,23,45 Several authors have shown a higher rate of bone turnover and vitamin D deficiency to be associated to BMOS.42,46 Screening of hypovitaminosis could be useful in BMOS patients, but this was not performed in our group.
All our patients received conservative treatment measures, comprised of rest and restricted weight-bearing. Orthotic insoles, full weight-bearing cast and a short leg walker boot were added to the treatment when necessary. No standard treatment protocol was implemented. Adult BMOS patients are often treated conservatively with physical therapy, nonsteroidal anti-inflammatory drugs and other immobilizing orthoses such as a stiff soled postoperative shoe.2,12-16 In literature, the use of iloprost, a vasoactive synthetic prostacycline analogue, has been shown to provide favourable results, with significant improvements in both function and pain scores, and a (partial) regression of marrow oedema signal on MRI.11,17-23,41,43 Iloprost causes a dilatation of arterioles and venoles, decreasing capillary permeability and inhibiting thrombocyte aggregation.11,47 A single case report recorded the use of iloprost in a 15-year-old girl diagnosed with BMOS of the acetabulum, with pain in rest decreasing after three days of treatment, and without report of adverse effects. 31 Iloprost has been proven to be safe and efficient in other indications for use in children, with observation of minor adverse effects such as headache and hypotension.48–52 However, as insufficient long-term data concerning the efficiency or safety of the product is available, the indication to use iloprost for a self-limiting transient condition such as BMOS seems questionable. Decompressive drilling of the bone has been described in the proximal femur.22,29 A single retrospective case series on drilling the calcaneus for chronic heel pain was published by Santini et al in 2003, 53 showing moderate clinical results for this technique, performed for multiple diagnoses. This pathology shows diffuse involvement of multiple tarsal bones in our case series, and has a likely self-limiting disease course. Since an overall good response to conservative treatment measures, we believe surgery with its possible complications should be avoided in paediatric BMOS. We advise applying conservative treatment measures tailored to the patient and their symptoms, varying from relative rest in milder cases to non-weight baring casts when disabling pain is present. The main goal of treatment is to minimize pain symptoms while maintaining the patients’ functionality. Reassuring the patient and their parents of the self-limiting course of the disease is an important aspect.
We believe that connecting imaging data to clinical symptoms is necessary to provide a correct diagnosis, especially in children, and guide further diagnostic processes and treatment decisions. In our case series, we found a distinct pattern of patchy involvement in multiple locations of the foot, irrespective of the patient's age, regressing in parallel with clinical symptoms. This is an important finding, since in earlier imaging studies in children, clinical data could often not be linked to MRI findings. We propose that once the diagnosis is confirmed, clinical symptoms should guide the further treatment.
We provided a control group, by reviewing a population of children of a corresponding age with clear underlying clinical and imaging-based diagnoses. None of these children showed the well-defined patchy area involvement of increased signal intensity on T2 and TIRM-weighted images, supporting our hypothesis.
There are several limitations to this study that must be taken into consideration. The first limitation is the small sample size and the follow-up being limited to the clinical course of each patient. All clinical information was retrieved from patient files and no objective measurement tools for pain and function improvement were used. Several children were included after minor trauma, as stated above however, we do not believe such daily traumatisms in the life of a child could lead to a fulminant marrow oedema reaction. We do not exclude the fact that bone marrow oedema in the talus, calcaneus or navicular could be possible because of a contusional reaction, that can be sustained for several months and difficult to differentiate from a bone bruise. Differentiation between physiological, residual red bone marrow, altered weight-bearing patterns and pathological BMOS should be further studied by prospective, comparative studies in a paediatric population. We believe the strength of this case series is the clear parallel progression of clinical and MRI data over the whole course of the disease.
Conclusion
In this case series both clinical and MRI data of six paediatric patients with BMOS of the foot and ankle is reported. As BMOS is transient and likely self-limiting, we believe no pharmacological treatment is warranted, and conservative treatment measures should be implemented to improve patient comfort during the disease course. The clinical progression of symptoms shows a parallel course to the MRI findings, making consecutive follow-up MRI imaging unnecessary. A swift and correct diagnosis of BMOS, based on clinical findings and bone marrow oedema patterns on MRI with no definite underlying causes, could prevent unnecessary diagnostic investigations and invasive treatments for patients.
Footnotes
NVB: Conception and design of study, Revising the manuscript critically for important intellectual content, Approval of the version of the manuscript to be published.
SP: Revising the manuscript critically for important intellectual content, Approval of the version of the manuscript to be published.
AVR: Conception and design of study, Revising the manuscript critically for important intellectual content, Approval of the version of the manuscript to be published.
JDR: Analysis and/or interpretation of data, Approval of the version of the manuscript to be published.
SV: Conception and design of study, Analysis and/or interpretation of data, Revising the manuscript critically for important intellectual content, Approval of the version of the manuscript to be published.