
Abstract
Abstract
Purpose
This study was designed to review the diagnostic yield of single photon emission computed tomography-computed tomography (SPECT/CT) in children with complex foot/ankle pain.
Methods
We reviewed the records of 33 patients with complex foot and ankle pain referred for SPECT/CT (36 scans) performed between 1st September 2009 to 30th September 2019. All patients had foot and ankle radiographs and 18 out of 33 patients had undergone magnetic resonance imaging (MRI) prior to SPECT/CT. The diagnostic contribution of SPECT/CT was established at the time of the scan during a multi-disciplinary team meeting.
Results
The patients’ mean age was 13.4 years (range six to 16.5 years) and 58% were female. In total, 18 patients had undergone previous surgical treatment. SPECT/CT was found to have decisive clinical value compared with radiographs and CT/MRI in 28 out of 36 cases. In ten patients it prompted surgical management (coalition excision, arthrodesis), in seven patients it redirected conservative management, in six patients it excluded other pathology and in five patients it showed additional/unexpected focal areas of mechanical stress, thus avoiding surgery. When compared with MRI, SPECT/CT added further clinical information in 13 out of 18 cases. SPECT/CT added decisive clinical value in five out of five patients with accessory ossicles, eight out of nine patients with tarsal coalition, five out of seven patients with surgically treated Congenital Talipes Equinovarus (CTEV) and four out of five patients with neuromuscular feet. In eight out of 36 cases SPECT/CT confirmed the diagnosis without adding significant information.
Conclusions
SPECT/CT can identify foci of active mechanical stress at cortical bone level in children with unexplained complex foot and ankle pain, particularly in the multiply operated foot, accessory ossicles and tarsal coalitions.
Level of Evidence
IV
Introduction
Diagnosis of foot and ankle pathology in children can provide a significant clinical challenge to the orthopaedic surgeon. Children with foot and ankle pain often present with vague, chronic symptoms, and the close proximity of multiple small joints can make localization and differentiation between organic and functional pain difficult. In many cases diagnosis is complicated by comorbidities relating to an underlying syndrome, previous surgical intervention or trauma, which may affect interpretation of the clinical and radiological findings. Conventional imaging with plain radiographs, computerized tomography (CT) and magnetic resonance imaging (MRI) is the current main aid to establishing a diagnosis and facilitating surgical planning. However, in children with complex, longstanding pain, accurate diagnosis remains a challenge and treatment outcomes are variable.
After plain radiographs, MRI has become the imaging reference standard for undiagnosed foot and ankle pain due to its high sensitivity and specificity for benign osseous and soft tissue pathology1–3 and its strong correlation with findings at surgery. 4 However, MRI is of limited benefit with subtle structural abnormalities and multiple coexisting pathologies and provides poor physiological data.5,6
In contrast, whole body planar bone scintigraphy provides pathophysiological data by identifying foci of abnormal bone metabolism and turnover. Bone seeking phosphates and diphosphates are radiolabelled with technetium-99m and show a high affinity to areas of increased metabolic activity. It has been used successfully in the diagnosis of malignant metastatic bone lesions; 7 however its resolution is limited by the 2D images, and lacks the anatomical precision required for surgical planning. 8
The addition of single photon emission computed tomography (SPECT) combines planar bone scintigraphy with tomography to acquire data and map 3D tracer distribution. In SPECT/CT, a low dose unenhanced CT scan is performed at the end of the acquisition of the static planar images with the patient in the same position; the SPECT images are then superimposed onto the CT images to create a high resolution SPECT/CT dataset with improved attenuation correction. 9 This hybrid technique provides detailed anatomical data from the CT and correlates this directly to the functional data from the SPECT scan. In symptomatic patients, SPECT/CT has a greater specificity than MRI alone 10 and has given clinicians a new insight into many pathological conditions not possible through conventional imaging modalities.11,12 The role of SPECT/CT is expanding rapidly in adult orthopaedics where it has been used to diagnose osteochondral lesions, tarsal coalitions, occult fractures and painful accessory bones; 13 however its use in the paediatric population remains poorly studied.
The objective of this study was to assess the diagnostic value of SPECT/CT as an adjunct to conventional imaging modalities in the management of foot and ankle pathology referred to a tertiary paediatric orthopaedic centre. Further analysis was performed focusing on specific conditions: tarsal coalitions, Congenital Talipes Equinovarus (CTEV), accessory ossicles and pathology secondary to neurological conditions.
Methods
The electronic radiology database at our tertiary referral hospital was used to identify all patients aged 16 years and under who had undergone a SPECT/CT for foot and ankle pathology between1st September 2009 and 30th September 2019. The search identified 33 consecutive patients with a total of 36 SPECT/CT scans. The clinical and radiological results of these 36 scans were reviewed.
Electronic records were analysed to review the following outcomes of interest: clinical presentation, radiological findings and impact of SPECT/CT on management. All SPECT/CT scans were discussed in the week after the scan at the Ortho-Radiology Multi-Disciplinary Team (MDT) meeting and the discussion was documented in the clinical notes. For the purposes of this study, all clinical and radiological data was synthesized. From the MDT outcome and the subsequent patient's management recorded in the clinical notes, a decision was made as to whether the SPECT/CT scan results had influenced the further clinical management (‘added value’ to the clinical picture). As the period of study was 10 years, this year, the senior surgeon and the senior nuclear medicine consultant (DME, LB) reviewed all scans and the clinical database to confirm/refute the added value of SPECT/CT.
All children included in the study were being investigated for chronic foot and ankle pain. All cases had had at least one form of conventional imaging (radiographs, CT or MRI) prior to SPECT/CT. In all cases SPECT/CT was performed with the aim of clarifying the site of the pain because a significant level of diagnostic uncertainty remained following initial imaging. No patients presenting with acute pain were investigated. In the presence of bilateral pathology and/or symptoms, the indication for SPECT/CT was unilateral, focusing on the most symptomatic side.
The study was registered as a service evaluation with the Research and Development Office at our tertiary referral hospital (Great Ormond Street Hospital).
Bone scintigraphy with SPECT/CT
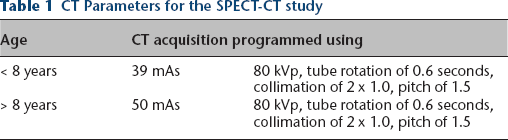
The SPECT/CT was performed using the radiopharmaceutical technetium-99m hydroxymethylene diphosphonate ([99mTc]Tc-HDP). General anaesthetic/sedation was not required and there were no reported adverse reactions to the radiopharmaceutical. Via a low energy general purpose collimator, dynamic blood flow images were obtained in the first minute after injection, with a frame rate of one frame/five seconds; planar blood-pool phase images were acquired immediately afterwards. Delayed static images of both feet were acquired using a low energy high resolution collimator. All patients were scanned on a Siemens True-point Symbia T2 SPECT/CT scanner (Siemens Healthcare, Erlangen, Germany). Both feet were immobilized in a symmetrical position on the gamma camera couch using Velcro straps, to ensure no movement occurred during image acquisition. At the end of the SPECT study a low dose unenhanced CT scan of both ankles and feet was performed with the patient in exactly the same position as for the SPECT study. The CT parameters varied slightly according to the patients, with mAs increasing with age and in the presence of surgical metalwork (to reduce artefact) (Table 1). At the time of the SPECT/CT scan the radiographer marked the site of pain on a representative foot and ankle diagram, which helped to correlate the area of increased uptake to the site of pain. A whole body sweep acquisition was performed at the end of the SPECT/CT to rule out bone pathology elsewhere in the skeleton.
CT Parameters for the SPECT-CT study
The 3D SPECT images of both feet were reconstructed using the Ordered Subsets Expectation Maximization algorithm. The reconstructed SPECT images were then fused with the CT images on a Hermes workstation using the Hybrid 2 Viewer software programme (Hermes Medical Solutions, Stockholm, Sweden). The quality of SPECT/CT co-registration of the images was considered excellent.
A SPECT/CT scan was considered abnormal and consistent with ongoing abnormal mechanical stress if a focal area of increased tracer uptake was noted at unexpected sites. The intensity of tracer uptake was considered proportional to the level of mechanical stress at that site. Increased vascularity on the blood-pool images was consistent with an ongoing active inflammatory process. The physiologically prominent, normal, tracer uptake within the distal tibial and fibular physes was noted in all scans but did not present a problem in interpreting abnormal findings. The SPECT/CT scans were double-reported by a nuclear medicine consultant with 20 years’ experience in paediatric nuclear medicine and a senior paediatric radiologist (ME, LB) with a special interest in nuclear medicine. The radiation dose given by an isotope bone scan in a child/adolescent is around 2.7 mSv (equivalent to one year of natural background radiation in central England). 9 In our experience the CT study component, with selected low dose parameters, gave little additional radiation (0.5 to 1.2 mSv, mean 0.75 mSv). The amount of radiation is higher than a plain film or a CT of both feet owing to the additional radiation from the bone scintigraphy; however, the added benefit, which justified the SPECT/CT study, was the ability to differentiate active ongoing mechanical stress at cortical bone level from longstanding inactive sclerosis on CT, not responsible for clinical symptoms.
Results
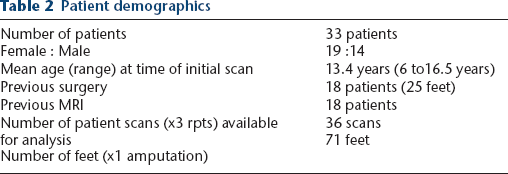
A total of 36 SPECT/CT scans in 33 consecutive patients, mean age 13.4 years, were reviewed. In all, 58% of patients were female (Table 2). Scans of 71 feet were available for analysis: one patient had had an amputation.
Patient demographics
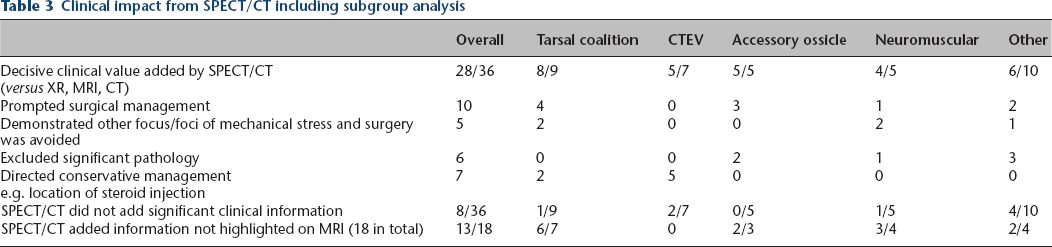
All the SPECT/CT scans were discussed at the weekly Ortho-Radiology MDT and the discussion documented in the clinical notes. Following review of the SPECT/CT scans and of the clinical notes, taken at the time of the scans, for the purpose of this study, SPECT/CT was found to have changed management, adding decisive clinical value compared with conventional imaging in 28 of 36 cases (77%) (Table 3). In ten cases it prompted surgical management such as coalition excision, realignment osteotomy or arthrodesis. In 18 cases it aided diagnosis and directed conservative management; surgery was avoided in five patients. In eight out of 36 cases SPECT/CT confirmed the diagnosis without adding significant clinical information.
Clinical impact from SPECT/CT including subgroup analysis
Asymptomatic feet
In total, 22 feet (31%) were asymptomatic at the time of the scan and among them 20 out of 22 scans showed no abnormality on bone scan SPECT/CT. In two asymptomatic feet the SPECT/CT showed increased tracer uptake: one was a child with bilateral GMFCS II cerebral palsy and the other a child with bilateral tarsal coalitions.
Symptomatic feet
Patients presented with a variety of underlying foot and ankle pathologies (Table 4).
Demographic data related to underlying condition
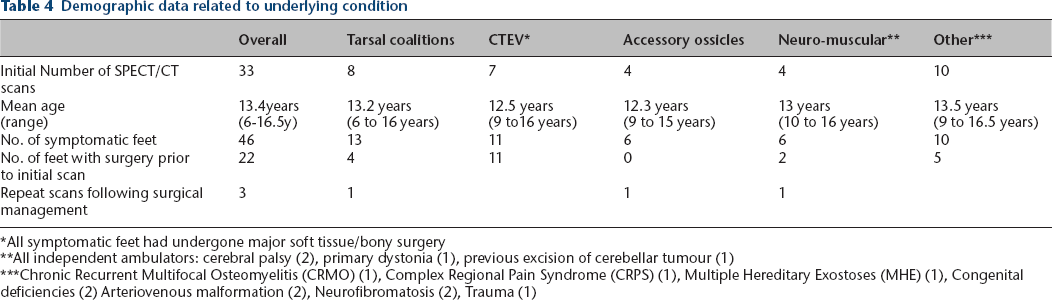
All symptomatic feet had undergone major soft tissue/bony surgery
All independent ambulators: cerebral palsy (2), primary dystonia (1), previous excision of cerebellar tumour (1)
Chronic Recurrent Multifocal Osteomyelitis (CRMO) (1), Complex Regional Pain Syndrome (CRPS) (1), Multiple Hereditary Exostoses (MHE) (1), Congenital deficiencies (2) Arteriovenous malformation (2), Neurofibromatosis (2), Trauma (1)
Three patients underwent surgery as a result of their initial assessment and investigations, but due to persisting changed symptoms a further scan was performed at a mean 15 months post-surgical intervention (Table 4).
In symptomatic feet, the mean time between MRI scan and SPECT/CT was 9.6 months (range two to 36 months) with a median of six months. When compared with the previous MRI, SPECT/CT added relevant information in 13 of 18 cases by demonstrating increased osteoblastic activity, thus enabling us to distinguish between a mature inactive abnormality and an abnormality with increased metabolic activity, compatible with ongoing active mechanical stress (Table 3, Fig. 1).

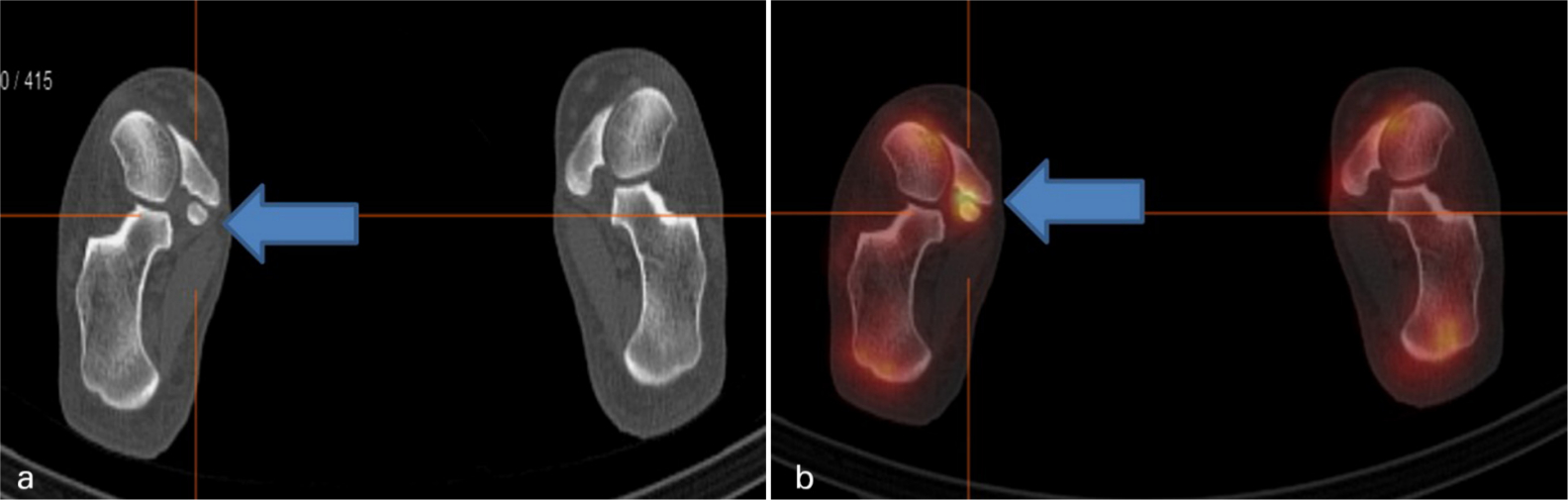
Tarsal coalition: 15-year-old female. Two years of widespread left foot pain on exertion and at rest; reluctant to bear weight. No movement at left subtalar joint.
Based on clinical assessment and initial imaging, patients were subdivided into broad categories, which were analysed further to identify the particular benefit of SPECT/CT in relation to certain conditions (Table 3).
Tarsal coalitions
Nine patients with a known diagnosis of tarsal coalition were reviewed. Three feet had undergone previous surgery. SPECT/CT added decisive clinical information in eight out of nine cases. In four cases it prompted surgical management (two arthrodeses and two coalition resections). The indications for surgery had been unclear based on clinical and plain film/MRI findings (Fig. 1, Table 3).
Congenital Talipes Equinovarus (CTEV)
Scans from seven patients with CTEV were reviewed; all patients had undergone extensive previous foot surgery, with a resulting degree of stiffness and deformity; five patients had already undergone revision surgery. In all of them, pain was difficult to localize. In five cases, SPECT/CT added diagnostic value directing management towards non-surgical options (Fig. 2, Table 3 and 4).
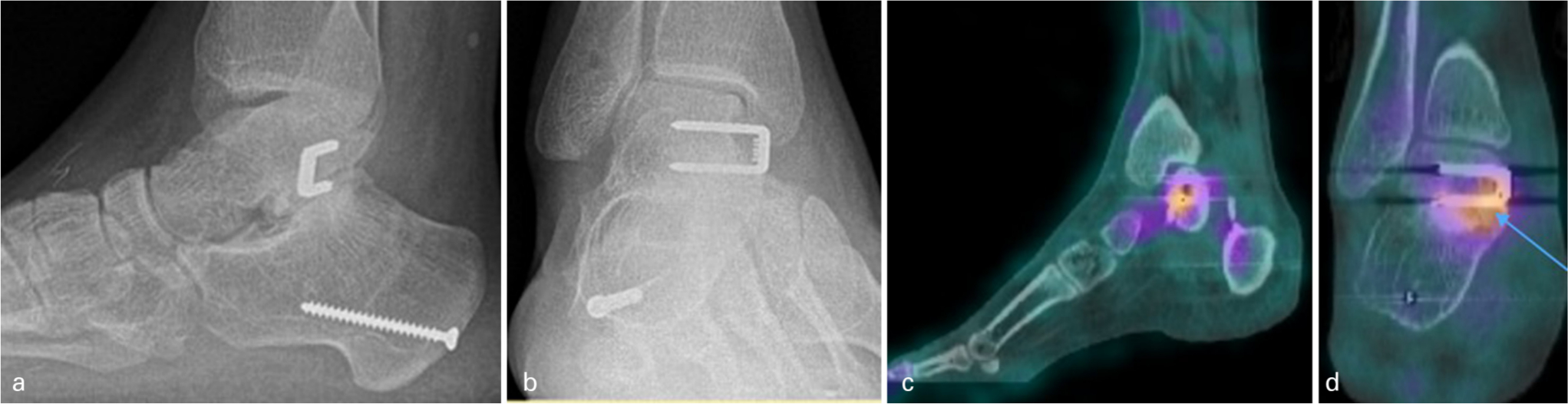
Multiply operated CTEV:
Accessory ossicles
SPECT/CT was shown to give decisive clinical value in all five cases. In three cases it highlighted an active area of tracer uptake assumed to be the pain generator that guided surgical management. In two cases it excluded other pathology (Fig. 3, Tables 3 and 4).
Accessory ossicle: 15-year-old girl with a known accessory navicular ossicle presenting with a four-year history of right-sided medial arch pain. MRI was unremarkable with no evidence of bone marrow oedema.
Neuromuscular feet
A further subgroup of five scans in four patients with chronic pain secondary to neurological conditions was analysed. All patients were able to walk independently. None of the feet were fully flexible. On three occasions in two patients, the SPECT/CT scan was prompted by pain following surgery. One such scan prompted further surgery, but revision surgery was avoided in the other two. Overall, SPECT/CT was deemed to have added further clinical value in four cases, prompting surgery in one case (Tables 3 and 4).
Others
This group comprised ten patients with a variety of pathologies that could have been responsible for their foot and ankle pain. Four patients had undergone previous surgery (Tables 3 and 4). SPECT/CT added clinical value in six cases.
Although the primary indication for SPECT/CT was always the investigation of unilateral severe symptoms, in 13 cases the contralateral foot did have mild/moderate symptoms: in ten out of 13 feet minor increased activity was identified in association with a tarsal coalition or a surgically treated CTEV.
Discussion
The complex anatomy and function of the foot is a diagnostic challenge for the orthopaedic surgeon when presented with a patient in pain. Multiple small joints in close proximity, as well as a variety of potential foot and ankle pathologies, make pain hard to localize and define. Differentiating between old and new pathology is challenging, and it can be difficult to determine the difference between functional and organic pain, particularly in the paediatric population.
Conventional imaging techniques are adequate in the management of the majority of these cases; however, there are a significant number of cases where diagnostic uncertainty remains. Plain radiographs, CT and MRI have been used routinely in the assessment of foot and ankle pain and, in the majority of cases, this has been sufficient for diagnosis and effective management. However, plain radiographs can only identify gross pathology, with a limited role in the diagnosis of chronic pain. Similarly the use of CT, whilst providing accurate anatomical detail, is not able to differentiate between old settled structural abnormality and anatomical changes due to ongoing active mechanical stress. 14
MRI, the current advanced imaging technique of choice, detects areas of bone marrow oedema (BMO) corresponding to acute inflammation, which is considered to relate to areas of pain. However, BMO often covers a wide anatomical area and so is less clinically useful in areas with multiple small joints. Whilst MRI is diagnostic in most instances of foot and ankle pain in children, it is not sensitive in detecting areas of mechanical stress at cortical bone level and, therefore, when considering surgical intervention, it lacks the anatomical precision required for surgical planning. Furthermore, patients with chronic pain in the presence of metallic implants are poorly investigated with MRI.
Our patient population consisted of patients under investigation for longstanding foot and ankle pain where there was diagnostic uncertainty. The increased osteoblastic activity demonstrated on SPECT/CT was correlated with the site of pain, recorded by the radiographer at the time of the SPECT/CT scan on a representative foot and ankle diagram, to identify the origin of the pain generator. In cases of bilateral pathology, the area of increased osteoblastic activity was often more pronounced in the symptomatic foot when compared to the less symptomatic foot.
Review of SPECT/CT results on the asymptomatic feet further increased the diagnostic accuracy of the scan, adding specificity. In total, 20 of 22 asymptomatic feet also showed a normal SPECT/CT scan and only two asymptomatic feet showed foci of increased tracer uptake, one in a patient with cerebral palsy and abnormal gait pattern and the other in a patient with bilateral tarsal coalition where the cortical bone stress may have not yet reached a symptomatic level. The findings in these two patients could be due to a pathological load, causing excessive mechanical stress, on an anatomically abnormal foot (for example, a flat foot), which had not yet become symptomatic, with a resulting increased osteoblastic activity causing focally increased tracer uptake.
The CT component of the SPECT/CT study provides the anatomical precision required to localize the metabolically active abnormality. Although small numbers, these results provide further confirmation that increased metabolic activity can be accurately correlated to the site of pain, thus representing the pain generator.
On the other hand, the SPECT component of the SPECT/CT study allowed differentiation between focal areas of longstanding sclerosis on CT with no increased osteoblastic activity on SPECT, in keeping with settled old reactive changes, from sclerosis on CT associated with increased uptake on the SPECT, consistent with areas of ongoing active abnormal mechanical stress. In patients with multiple deformities and, often, multiple previous surgeries, the ability to distinguish between what is abnormal but quiescent from what is abnormal but metabolically active is essential for surgical planning, and this is where SPECT/CT may have a benefit compared to conventional imaging modalities.
A striking finding in our study was that the BMO found on MR imaging did not necessarily correlate with the area of increased activity seen on SPECT/CT images. In 13 of 18 patients with both MRI and SPECT/CT imaging, SPECT/CT demonstrated a focal area of increased osteoblastic activity, not correlated to MRI changes, which corresponded to the site of pain (Table 3). We accept that there was a median delay of six months between MRI and SPECT/CT and that the previous BMO may have resolved at the time of the SPECT/CT even in these patients with chronic symptoms, but the findings are in line with what has been observed in orthopaedic adult practice 15 and indicates that SPECT/CT may have a role to play in complex foot problems where MRI does not identify a specific origin of pain.
In our study the CT component gave a very low added radiation dose whilst greatly increasing the diagnostic accuracy by providing a precise anatomical localization of the areas of mechanical stress at cortical bone level.
Subgroups
When analysing which patient subgroup would benefit most from SPECT/CT we reviewed four distinct pathologies: tarsal coalitions, CTEV, accessory ossicles and patients with neuromuscular disease and altered gaits. In our small series, patients with accessory ossicles and tarsal coalition had the highest rate of clinical benefit, with clinical value added by SPECT/CT in five out of five and eight out of nine patients respectively. In these conditions it can be difficult for the surgeon to determine whether the pain is generated from the ossicle/coalition or is due to altered mechanical loading on surrounding joints. Furthermore, MR imaging in mature coalitions may not highlight active pathology whereas SPECT/CT does do so (Fig. 1).
The third group where SPECT/CT was clinically beneficial was in patients with CTEV. All seven patients with CTEV included in the study had received surgical intervention, thereby increasing the potential locations for the pain generators. (Fig. 2). Through highlighting areas of active mechanical stress, SPECT/CT helped differentiate between old, treated and new pathology in five of these cases, and may be particularly useful in assessing postoperative foot and ankle pain. Further to this, in patients with metal work who cannot undergo MRI, SPECT/CT is a potentially helpful imaging technique. 16
Limitations
A significant limitation of our study is its retrospective nature, with the consequent selection bias, and the small number of cases for each subgroup. However, the purpose of the study was not to demonstrate the accuracy of SPECT/CT in complex adolescent foot pain, but to show that further prospective evaluation in a larger series is justified. Similarly, this study does not comment on outcome and the hypothesis that patient outcomes improve through the use of SPECT/CT is yet to be proven.
Another limitation is the way the primary outcome of the study (i.e. whether SPECT/CT added clinical value) was established: this was not done in a randomized fashion, and we did not have a control group. However, the SPECT/CT scans were all discussed in the weekly Ortho-Radiology MDT meeting at the time the investigation was performed; the discussion was documented in the clinical notes and clinical care continued. All SPECT/CT scans and clinical information were re-reviewed by the radiologist and the orthopaedic surgeon. The decision as to whether SPECT/CT added clinical value to the patient's management was based on the change in management that SPECT/CT introduced: this had been recorded in the clinical notes, which were reviewed for the purpose of this study. Therefore, the added value of SPECT/CT was not the result of a subjective decision at the time of this review.
Conclusion
These preliminary results show that, by identifying foci of active mechanical stress at cortical bone level, SPECT/CT may be a further valuable imaging modality to investigate children with complex foot and ankle pain in cases where there is diagnostic uncertainty. It may have particular relevance in the multiply operated foot and in tarsal coalitions.
Footnotes
The other authors declare no conflict of interest.
OR: Data acquisition, Data analysis and interpretation.
NG: Data acquisition, Data analysis and interpretation.
ME: Data analysis and interpretation, Manuscript drafting.
LB: Data acquisition, Data analysis and interpretation, manuscript drafting, Manuscript revision.
DME: Study design, Data acquisition, Data analysis and interpretation, manuscript drafting, Manuscript revision.