
Abstract
Objective
The aim of this paper is to describe the clinical features and radiological appearance of a rare and complex lower leg and foot deformity in hyperlax children.
Methods
Four children were included in the study; of these, two had bilateral feet involvement. All deformities were present since birth, comprising a pentad of conditions: (1) pathologic external tibia and fibula torsion, (2) ball and socket ankle joint with medial subluxation and talus medial subluxation, (3) excessive hindfoot valgus, (4) peroneal and Achilles tendon displacement anterior to the lateral malleolus and (5) generalized ligament laxity. All children had failed cast manipulation. Only two had undergone a minimal soft tissue procedure, but there had been no improvement.
Results
All patients were ambulatory and pain free at the mean age of 6.5 years.
Conclusion
Conservative or minimal soft tissue procedures are not effective in restoring the anatomy of such feet.
Introduction
External rotation of the tibia is a part of the normal growth and development process of an infant's lower extremities [1, 2].
Pathologic external rotation deformity of the tibia and fibula in isolation is a rare condition and was first described by Lowman in 1919 and then by Levine [3]. The association with paralytic conditions, such as poliomyelitis, cerebral palsy and myelomeningocele, has long been recognized [4].
Congenital anterior dislocation of the peroneal tendons is an infrequently reported condition in the neonate and is usually associated with a calcaneovalgus deformity of the foot [5]. The association with a convex pes valgus deformity [6] and pes planus with severe pronation of the heel in multiple chromosomal deformities has also been described [7].
Anterior displacement of the Achilles tendon relative to the lateral malleolus has not been previously been reported.
Congenital ball and socket configuration of the ankle joint can be an entity on its own or be associated with congenital shortening of the lower extremity and a relatively short fibula. It may be the result of adaptive changes in the distal tibia and fibula epiphyses in response to congenital abnormalities of the tarsal bones of which subtalar fusion is the most prevalent. Increased mobility of the ankle, as found in Larsen syndrome, may be a contributory factor [8–10]. An association with excessive external tibial torsion has not been described earlier.
We describe four children with this pentad of unique deformities. The children clinically presented with generalized hyperlaxity, an excessive hindfoot valgus with well-aligned midfoot in relation to the forefoot and a prominent medial mallleolus nearly touching the floor on weight bearing. Severe external tibia and fibula torsion was present with displacement of the peroneal tendons and Achilles tendon anterior to the distal fibula.
Materials and methods
The four patients were treated at the pediatric orthopedic clinic of King Faisal Specialist Hospital and Research Center in Riyadh, Saudi Arabia (which is the main tertiary care hospital for the 22 million inhabitants of Saudi Arabia) for more than 18 months period. They complied with the inclusion criteria of the study, which included manifestation of (1) excessive external tibial torsion, (2) valgus hindfoot, (3) anterior dislocation of the peroneal tendons and Achilles tendon in relation to the lateral malleolus, (4) a ball and socket ankle joint and (5) generalized ligament laxity. The deformities had been present since birth, and all children were ambulant. Of the four patients, two had bilateral involvement. Both unilateral cases involved the right side. The average age of the children at presentation was 6.5 years. Two feet had previous undergone unsuccessful soft tissue surgical attempts to correct the deformities.
Clinical examinations of the feet were performed to assess the range of motion of the hindfoot and midfoot joints, instability and correctability. Joint hyperlaxity was measured by the Beighton hypermobility score [11]. Associated syndromes and neurologic conditions were excluded. External tibia and fibula torsion was measured clinically by the Staheli prone rotation profile. The rotational profile of the femurs and the foot progression angles were measured in a similar fashion and compared in the unilateral cases. Lower limb lengths were determined clinically by measuring the femurs and the tibiae individually. All four patients were referred to the genetic and metabolic diseases clinic where they were examined by a pediatric genetics consultant; a chromosomal analysis of the patients and their parents was performed.
Radiographic assessment
Anterior–posterior (AP) and lateral standing radiographs of the ankle were performed to assess the dome of the talus in relation to the tibia plafond and to determine the fibula station [12], which is an indicator of the position of the distal fibula physis in relation to the tibia plafond. Varus and valgus stress radiographs of the ankle demonstrated an instability. The AP and lateral standing views of the feet enabled an evaluation of the tarsal and metatarsal relationships and the hindfoot relationship to the ankle joint. Tibia rotation was measured by a computed tomography (CT) scan, with cuts through the proximal tibia and the distal tibia and fibula. Truncated three-dimensional (3-D) images were reconstructed, and measurements were taken from the transverse line of proximal tibia against the bimalleolar axis. This 3-D CT reconstruction demonstrated the bony relationships of the foot and ankle [13, 14]. Magnetic resonance imaging (MRI) studies of the feet of all patients were performed to evaluate the joint configuration, ligament integrity and attachment and tendon bone relationships.
Results
Of the four patients who presented with this pentad of conditions, two had bilateral and symmetric involvement of the feet and the other two had unilateral involvement, with only the right side being affected. The average age of the patients at evaluation and presentation was 6.5 years (range 6–7 years). All children were male. All of the deformities had been present since birth. Three children were the product of full term spontaneous vaginal vertex deliveries and one by means of caesarian section. The developmental milestones had been normal, and the average walking age was 12–14 months. Two patients had consanguineous parents.
One child had ambiguous genitalia and an undescended testis. One of the children with bilateral involvement demonstrated bilateral short first metacarpal bones but normal thumb function. Genetic evaluation did not reveal any associated syndromes or chromosome abnormalities. All were ligamentous lax (average 5 points).
All of the children had been briefly treated during the postnatal period at the referral hospitals by cast manipulations. In all children, this treatment had failed to correct the deformity, and further conservative treatment was abandoned. Two children had surgical attempts at correction that comprised limited soft tissue releases of the Achilles tendons.
The children were all ambulant and participated functionally in daily activities. The main complaint was the valgus appearance of the feet and loss of propulsion. None of the children experienced pain or instability.
The two children with unilateral involvement demonstrated mild shortening of the affected tibia—1.0 and 0.7 cm, respectively. The femurs of all patients were of equal length.
The rotational profile of the femurs was normal, with medial rotation excursion measuring an average of 45° and lateral rotation excursion an average of 30°. The hips and knees had a full range of motion, and no angular deformities of the lower limbs were present (Table 1).
Distribution of measurements and deformities
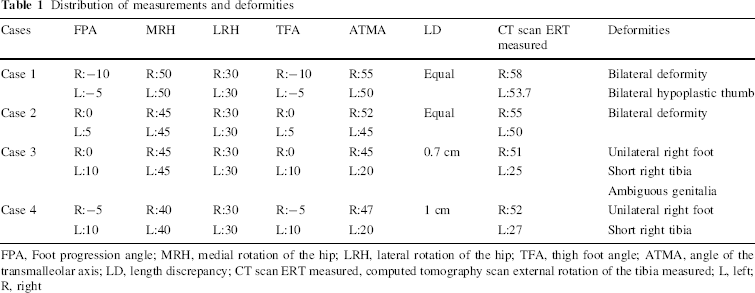
FPA, Foot progression angle; MRH, medial rotation of the hip; LRH, lateral rotation of the hip; TFA, thigh foot angle; ATMA, angle of the transmalleolar axis; LD, length discrepancy; CT scan ERT measured, computed tomography scan external rotation of the tibia measured; L, left; R, right
Clinical appearance
The hindfoot was in excessive valgus with the midfoot and forefoot, which were well aligned in relation to one another, and the forefoot appeared normal. The midfoot was in slight adduction in relation to the hindfoot, with a flattening of the medial arch. The medial malleolus appeared prominent and virtually touched the floor on weight bearing (Figs. 1, 2). The lateral malleolus was palpated just posterior and medial to the shortened Achilles tendon. The peroneal tendons lay approximately 2 cm anterior to the lateral malleolus and were shortened. Ankle movement was restricted, with an average dorsiflexion of 15° and an average plantar flexion of 10°. The hindfoot was everted more than 20° and could not be brought to neutral. Subtalar motion was restricted. The pronated talus was palpable below the medial malleolus and could not be reduced. The forefoot and midfoot could easily be reduced in relation to the hindfoot. There was moderate loss of muscle power of the tibialis posterior, toe extensors, peroneal muscles and gastrocnemius soleus complex. The average muscle power was graded as 4. No sensory deficit was present. The children walked on the medial aspect of the foot, with a short stride length, lack of propulsion and a slight internal rotation foot progression (range 0–15°). Weight bearing on the tips of the toes was not possible.

Frontal clinical picture

Clinical picture showing the prominent medial malleolus that touches the floor with weight bearing
Radiological findings
Standing AP and lateral foot X-ray
The AP standing radiograph revealed excessive valgus of the hindfoot with reciprocal divergence of the talus and calcaneus (diverging proximally instead of distally); the average talo-calcaneal angle was assessed to be 15°. The midfoot can be seen to be adducted in relation to the hindfoot at the level of the midtarsal joint, with an average talo-first metatarsal angle of 51°. The lateral malleolus lies directly posterior to the tibia on this view, reflecting the external torsion (Fig. 3). The fibula station is not relatively short, which is often the case in congenital ball and socket ankle joints.
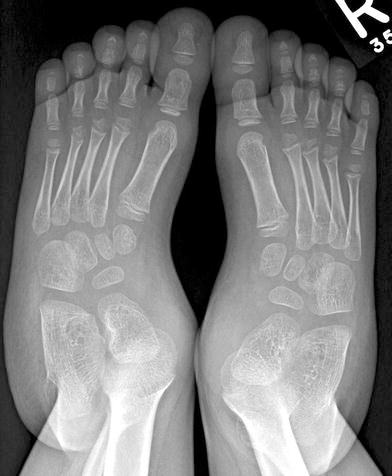
Anterior-posterior standing X-ray of a child with bilateral deformity
The AP view of the ankle joint demonstrates the ball and socket configuration (Fig. 4).

Anterior-posterior X-ray view of the ankle showing the ball and socket configuration
Valgus stress of the ankle joint results in a 90° medial subluxation of the talus body from the ankle mortise, and varus stress reduces the talus dome within the ankle mortise.
Computed tomography scan and shaded surface display 3-D rendering of the CT images
The pathologic distal bimalleolar external rotation is well demonstrated, with the lateral malleolus situated directly posterior to the distal tibia (Fig. 5). There is no synostosis between the talus and calcaneus.
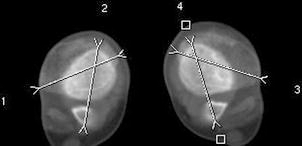
Computed tomography of the bimalleolar axis in relation to the transverse line of the proximal tibia
Magnetic resonance images
Axial proton-density-weighted T1 MRI images demonstrated the soft tissue components of the deformity. The peroneal tendons are seen to be displaced anterior to the distal fibula, with non-visualization of the superior peroneal retinaculum, which is suggestive of complete absence or tear. The Achilles tendon is located lateral and anterior to the lateral malleolus (Fig. 6). The intact interosseous ligament is clearly seen to be intact. The coronal MR image shows the pronation of the hindfoot (talus and calcaneus as one unit) in relation to the tibial plafond (Fig. 7). The medial deltoid ligament intact and in continuity but stretched. There is no synchondrosis between the talus and the calcaneus evident by MRI.

T1 axial image just proximal to the level of the ankle, showing the posteriorly located fibula with peroneal tendons (green arrow) and Achilles tendon (red arrow) displaced anteriorly in relation to the fibula

T1 coronal image showing the pronation of the hindfoot in relation to the tibial plafond
Discussion
The exact etiology of this fascinating and complex deformity of the foot and ankle joint has not yet been clearly determined. The components have all been described separately but not in combination or association with each other. It is not clear if one aspect of the pentad, such as the ball and socket ankle joint, precipitates a cascade of developing adaptive deformities as ambulation commences. It would appear, however, that the deformity is present from birth and that not all cases are bilateral. There are no apparent changes in the distal tibia and fibula physes, which may contribute to a rotational growth disturbance. In the unilateral cases, the slightly shortened tibia is probably secondary. The external tibia and fibula torsion averages 53°, which quite significantly exceeds the normal mean of 30–34°. The ball and socket ankle joint does not have the usual association with fibula hypoplasia or tarsal coalition. The talo-calcaneal interosseus ligament is intact, with pronation of the hindfoot in relation to the tibial plafond. The deltoid ligament is intact but elongated. The superior peroneal ligament is attenuated, which is probably secondary.
The version of the tibia and fibula is unique to the normal growth and development of the infant leg and has been documented to change throughout skeletal development from internal to external torsion to an average of 20° in adolescence. This is due to a torsional effect on the epiphysis, which produces a spiral lengthening of the bone through the long axis. The resulting torsion is postural—partly due to the tendency of the child to lie supine with feet and legs rotated outwards and partly due to the increased base of support resulting from standing with the feet pointing outward [15–17]. External tibial torsion presents at all ages and does not show a tendency to decrease. The majority of children with increased femoral anteversion and intoeing gait correct their gait by compensatory external tibial torsion, which does not exceed 30° [18].
Rotational growth of the tibia is difficult to quantify both clinically and radiologically. Three-dimensional CT reconstruction has become the standard diagnostic procedure to measure torsional deformities of the tibia. The mean torsion of the right tibia is 36.46° and that of the left tibia is 33.07° [19].
In 1962, Ruszczynska reported on a case which he termed congenital posterior dislocation of the distal end of the fibula. The clinical pictures and radiographs of this case are similar to those we report here, but there is no reference in this earlier study to the other components of the pentad [20]. A case of bilateral congenital subtalar dislocation was reported by Kaufmann et al.[21] in which the patient also ambulated on the medial malleoli and the medial aspect of the feet. The dislocated subtalar joints were connected by a thick fibrous band laterally and required an open reduction [21]. Our patients had pronation of the talus and calcaneus as one unit in relation to the tibial plafond, with maintained articulation between the talus and calcaneus.
The postulated etiology of peroneal tendon subluxation has been aplasia of the retromalleolar grooves or weakening of the peroneal sheath or both (Ehrlich, Edwards).
Aplasia was not evident in any of our cases. The subluxation and shortening of the peroneii and attenuation of the superior retinaculum is probably secondary to the excessive external tibia and fibula torsion.
All of our patients have normal intellectual function, and no neuromuscular signs were detected. The moderate weakness of the tibialis posterior, extensor hallucis longus, peroneii and gasrocnemius soleus complex can probably be attributed to the poor limb posture and function.
This complex of deformities is resistant to conservative treatment as manipulation and casting trials failed to correct the deformity in any patient.
Conclusion
We have described a unique and rather complex deformity of the foot and ankle in children that comprises a pentad of conditions: hyperlaxity, severe external tibia and fibula torsion, a ball and socket ankle joint, pronation of the hindfoot in relation to the tibial plafond resulting in a valgus hindfoot, anterior displacement of Achilles tendon and peroneal tendons lying in front of the fibula. Cast manipulations or minimal soft tissue procedures are not capable of addressing this deformity. Due to the complexity of this pentad, combined soft tissue and bony procedures to address the different aspects and levels of the deformities may be needed to achieve good outcomes.
Footnotes
Acknowledgment
We acknowledge Sama Ilyas for the preparation of this manuscript.