
Abstract
Abstract
Purpose
Spinal sagittal alignment restoration has been associated with improved functional outcomes and with reduced complications rates. Several limitations exist for radiological analysis in cerebral palsy (CP) patients. The goal of this study was to summarize the existing literature and report the important considerations to evaluate in a CP patient undergoing spinal surgery.
Methods
A retrospective radiological analysis was performed, including non-ambulant CP children with progressive scoliosis. Full-spine sitting radiographs performed pre-and postoperatively were required to measure spino-pelvic sagittal parameters.
Result
A total of 23 non-ambulating CP patients were included, mean age 16.0 years (standard error of the mean 0.5). Two distinct groups of patients were identified. Group 1 (61%) were patients with less trunk control (lumbar lordosis (LL) < 50°), retroverted and vertical pelvis (mean sacral slope (SS) 11.4° and pelvic tilt (PT) 38.1°) and anterior imbalance (mean sagittal vertical axis (SVA) 5.9 cm) and Group 2 (39%) were patients with better trunk control (LL > 60°, anteverted and horizontal pelvis (mean SS 49.3°, PT 9.7°) and posterior imbalance (mean SVA 5.8 cm). Postoperative measures showed significant impact of surgery with a PT reduction of 19° (p = 0.007), a mean SS increase of 15° (p = 0.04) and a LL gained of 10° (p = 0.2).
Conclusion
Sagittal spino-pelvic alignment in non-ambulating CP patients remains difficult to assess. The current literature is poor but our radiological study was able to define two distinct groups among Gross Motor Function Classification System (GMFCS) level V patients, based on the quality of their trunk control. All possible factors that may influence head and trunk posture should be systematically considered and optimized.
Level of evidence
Level IV
Introduction
Spinal sagittal alignment restoration has become a ‘hot topic’ in the spine community during the last decade. It has been associated with improved functional outcomes in adult spine deformity (ASD), and with reduced complication rates in adolescent idiopathic scoliosis (AIS).1,2 Pelvic parameters are now commonly measured preoperatively on lateral radiographs, but several limitations exist for the radiological analysis of cerebral palsy (CP) patients. First, the visibility of pelvic landmarks is reduced in patients in the sitting position (Gross Motor Function Classification System (GMFCS) IV and V) and is even worse in cases of pelvic obliquity, frequently encountered in CP patients considered for surgery (Fig. 1). Second, the reliability of static measurements to evaluate the actual physiological balance can be questioned in such patients presenting dynamic instability. Third, the visibility of endplates is often poor, due to osteopenia and the deformity itself. The only reliable radiological measures available for curves analysis are, therefore, Cobb angles and their reducibility, which explain the scarce literature on CP spinal sagittal alignment.3–6
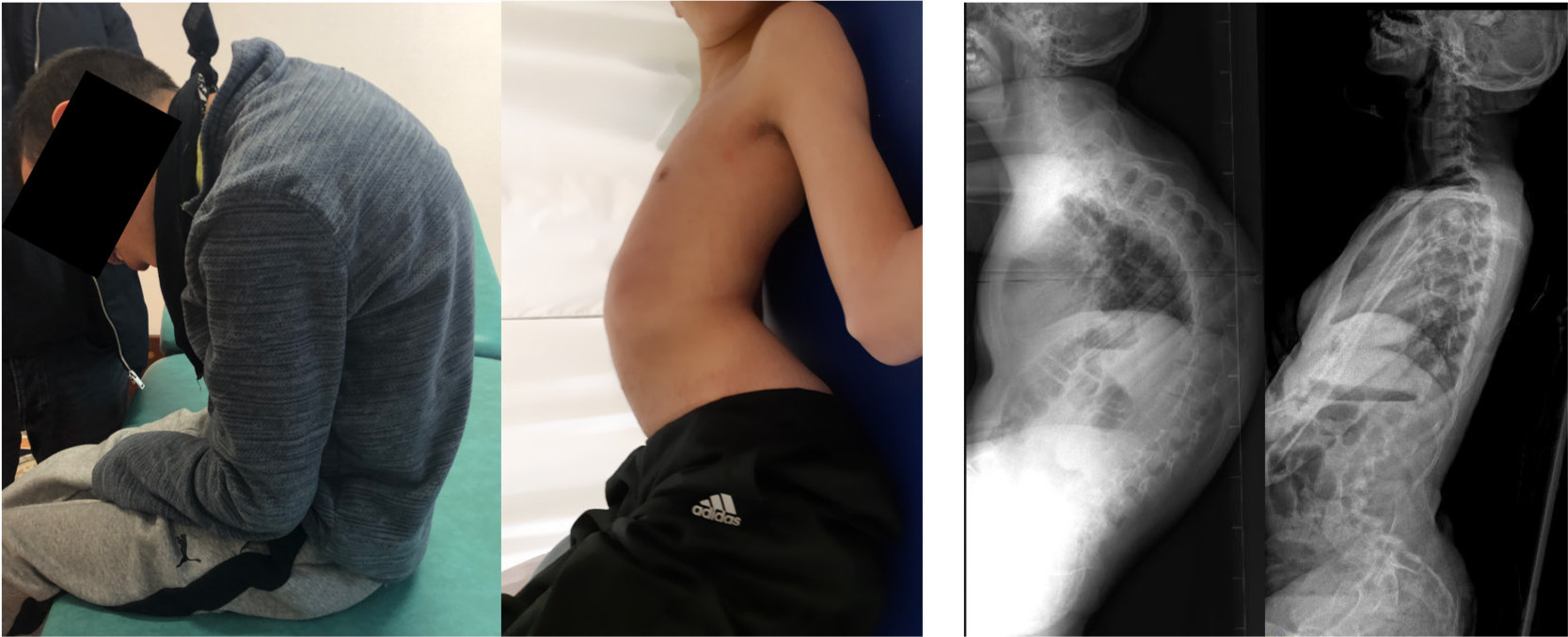
Photographs of two patients with major anterior and posterior imbalance. Radiographs showed poor visibility of pelvic landmarks and osteopenia, making pelvic parameters not measurable.
The goal of this study was, therefore, to summarize the existing literature and report the important considerations to evaluate in a CP patient undergoing spinal surgery.
This article was conceived by the neuromuscular and spine study groups of the European Paediatric Orthopaedic Society (EPOS) based on the presentations of the authors given at the society's 37th annual meeting in Tel Aviv, Israel (5 April 2019) in a two-hour focus session on CP and associated spine deformities. Based on an additional literature review (PubMed, Cochrane) and two decades of surgical experience and functional analysis in the field of neuromuscular spine deformities during growth, the authors highlight the current anatomical and biomechanical understanding, its practical implications for the clinical and radiographic assessment and the surgical strategy when it comes to the decision as to whether or not to include the pelvis in the fusion.
Materials and methods
Literature review
A bibliographic search in Medline and Google database from January 1995 to March 2019 was performed. The keywords included ‘cerebral palsy’, ‘sagittal alignment’, ‘spine’, ‘neuromuscular scoliosis’ and ‘head control’, used individually or in combination. Relevant literature was analyzed, summarized and discussed based on author's experience.
Retrospective series
A retrospective monocentric radiological analysis was performed on all CP patients operated on for scoliosis at our institution between January 2015 and October 2017. A minimum two-year follow-up was required. Inclusion criteria were: 1) non-ambulating CP patients < 19 years old; 2) progressive scoliosis responsible for spinal imbalance or pelvic obliquity; and 3) full-spine sitting radiographs performed before and after surgery. Patients with only supine radiographs and incomplete data were excluded. Demographic data and the level of motor function (GMFCS classification) were reported.
Sagittal plane radiological analysis included pelvic and spinal parameters, measured on SpineEOS software (EOS Imaging, Paris, France). Maximal thoracic kyphosis (maxTK), maximal lumbar lordosis (maxLL) and the number of lordotic levels were reported. Global sagittal balance was appreciated using the sagittal vertical axis (SVA). 7 All surgeries were performed under spinal cord monitoring by one of the two senior spine surgeons of the department. Patients were fused from T2 to the pelvis, using 5.5-mm cobalt-chromium rods and hybrid constructs (combination of pedicle screws and sublaminar bands).
Statistical analysis was performed using SPSS statistics 23.0 (SPSS Inc., Armonk, New York). A Shapiro-Wilk test was performed to assess data distribution. Continuous numeric data was expressed as means ± standard error of the mean (sem) using absolute values. Groups were compared with two-tailed Mann-Whitney, variables were with non-parametric distribution. A p < 0.05 was considered significant.
Results
Patients
A total of 72 consecutive CP patients were operated on during the study period. However, 45 cases were excluded because only supine radiographs were available before surgery, and four additional patients could not be included due to the low visibility of radiographs (Fig. 1). Final radiological analysis was, therefore, performed on 23 patients, mean age 16.0 years (sem 0.5; 11.4 to 19.0).
Preoperative sagittal alignment
Radiological measurements are summarized in Table 1. Two distinct groups of patients were identified according to the maxLL and the number of vertebrae included in the lumbar lordosis (Fig. 2). In Group 1 (n = 14, 60.9%), patients had a lumbar lordosis < 50° with four or less lordotic levels. The thoracic kyphosis was long, with an apex located between T8 and T10, and the pelvis was vertical (low sacral slope) and retroverted (high pelvic tilt). These patients with less trunk control did not have enough compensatory mechanisms and were anteriorly imbalanced (mean 5 cm). Group 2 (n = 9, 39.1%), corresponded to patients with better trunk control. Lumbar lordosis was greater (> 60°, p < 0.05), with five or more lordotic levels. Mean thoracic kyphosis was significantly lower (37°, p < 0.05) and thoracic hypokyphosis was more frequent (four cases). Pelvis was horizontal (high sacral slope) and anteverted (low pelvic tilt), and SVA was more posterior imbalance (5 cm on mean Fig. 3 and Table 2).
Sagittal pelvic and spinal parameters measurements in the 23 operated cerebral palsy patients. Data is expressed as mean, standard error of the mean (sem) and range
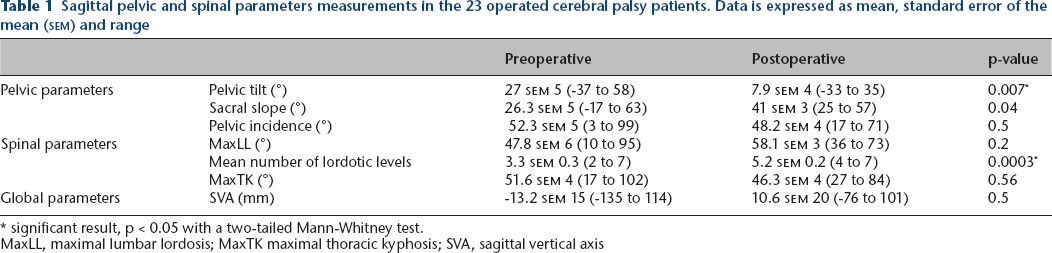
significant result, p < 0.05 with a two-tailed Mann-Whitney test.
MaxLL, maximal lumbar lordosis; MaxTK maximal thoracic kyphosis; SVA, sagittal vertical axis
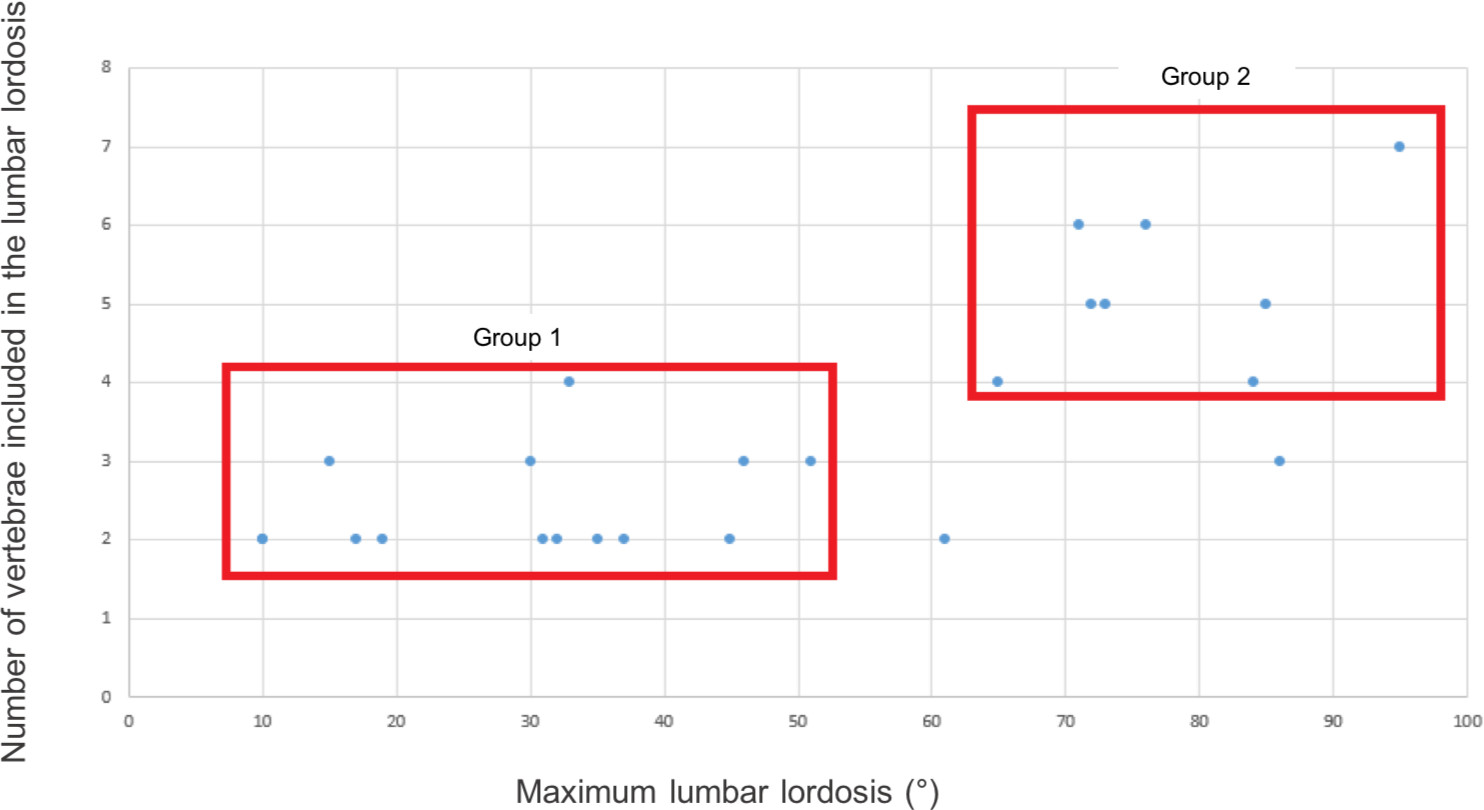
Patients’ distribution according to maximal lumbar lordosis and the number of lordotic levels.
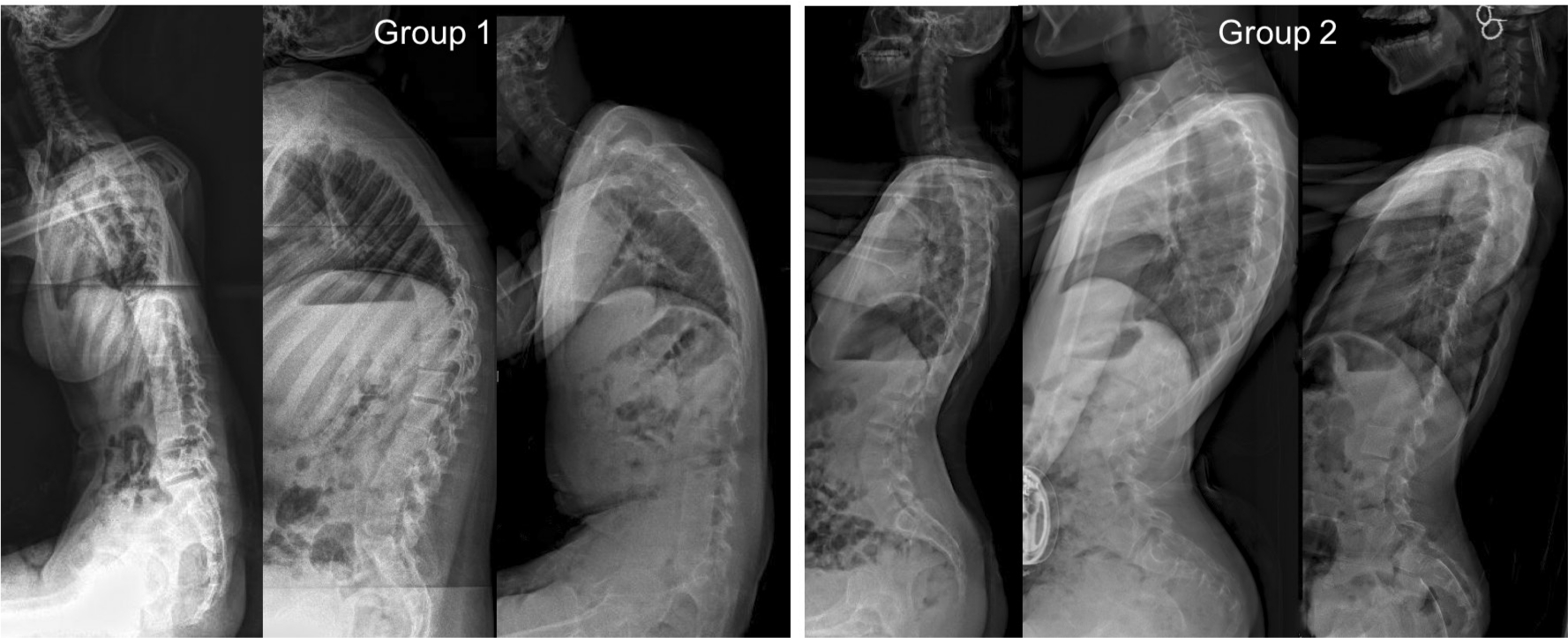
Illustration of sagittal alignment of the two distinct groups of patients. Group 1 were patients with poor trunk control and anterior imbalance. Group 2 were patients with better trunk control and posterior imbalance.
Comparison between Group 1 (n = 14, lower trunk control) and Group 2 (n = 9, better trunk control). Data is expressed as mean and standard error of the mean (sem)
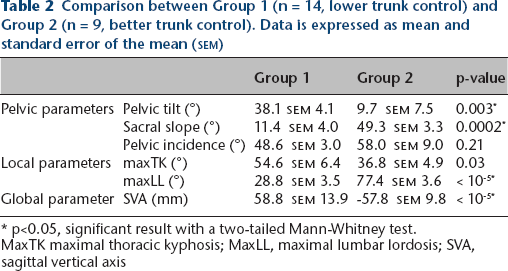
p<0.05, significant result with a two-tailed Mann-Whitney test.
MaxTK maximal thoracic kyphosis; MaxLL, maximal lumbar lordosis; SVA, sagittal vertical axis
Postoperative sagittal alignment
Surgery had a significant impact on sagittal alignment (Fig. 4). Pelvic parameters were significantly modified, with a mean pelvic tilt reduction of 19° (p = 0.007) and a mean sacral slope increase of 15° (p = 0.04). Lumbar lordosis gained 10° on mean, but this change did not reach significance (p = 0.2). The important finding was that spinal harmony was restored in most of the cases, with four or more lordotic levels observed in the instrumented spine in 85% of the cases (versus 29% before surgery) and with a lumbar lordosis adapted to pelvic incidence (i.e. LL-PI < 10°) in 75% of the patients (versus 8% preoperatively). Despite these improvements, only 47% of patients were considered balanced (SVA < 25 mm) on the latest sitting radiographs.

Postoperative result in a 16-year-old girl. The patient was initially with anterior imbalance and low lumbar lordosis (Group 1). Postoperatively, there was a posterior imbalance (sagittal vertical axis 63 mm) but spinal harmony was restored.
Discussion
It is now commonly accepted in the spine community that sagittal alignment should always be analyzed before surgery, and ideally be restored after the procedure to improve functional outcomes and reduce mechanical complications.1,7 However, such assessment based on static long-length sagittal radiographs can be difficult in CP patients, often affected by osteopenia, pelvic obliquity, hip contracture and dynamic instability. The literature is, therefore, very poor on the subject, with only six relevant articles available for analysis (only one including GMFCS V patients) and sagittal alignment parameters are currently lacking.3–6,8,9
Sagittal alignment in CP patients according to GMFCS level
To assess the degree of disability in children with CP, the GMFCS is traditionally used. 10 Patients with walking abilities are classified from GMFCS I to GMFCS IV level, while non-ambulant patients are GMFCS V. Three studies have explored and described the spino-pelvic sagittal alignment of walking CP patients, who often present retraction of hip flexors (right anterior, iliopsoas).3,8,9 Pelvic incidence was found to be similar to that of healthy controls, indicating that the shape of the pelvis was not affected by the disease. 3 However, the pelvis was anteverted (low pelvic tilt) and sacrum was more horizontal (high sacral slope). Lumbar lordosis was reduced compared with controls and not correlated with pelvic incidence. As a result, ambulant CP patients usually had anterior imbalance (positive SVA > 25 mm) in standing position.
Results of the current series on non-walking CP can be compared with previously reported data in ambulant CP patients (Table 3). Pelvic incidence was found to be similar, but the pelvis was more retroverted and sacrum more horizontal in non-ambulant CP children. Lumbar lordosis was similar and thoracic kyphosis increased but as a whole, non-ambulant children had more posterior imbalance (negative SVA) in the sitting position. Spino-pelvic sagittal measures of walking CP did not correspond to any of the group described in our series. Therefore, spino-pelvic parameters from walking CP are not similar to those of sitting CP.
Comparison of sagittal spino-pelvic alignment averaged measures between ambulant and non-ambulant cerebral palsy (CP) children
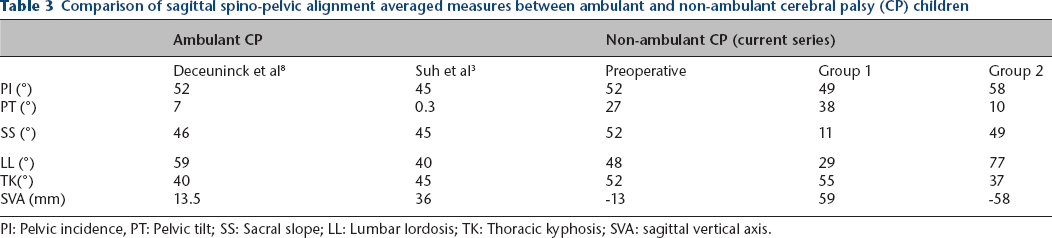
PI: Pelvic incidence, PT: Pelvic tilt; SS: Sacral slope; LL: Lumbar lordosis; TK: Thoracic kyphosis; SVA: sagittal vertical axis.
Bernard et al 9 have investigated the influence of the GMFCS level on the sagittal alignment of ambulating CP children (GMFCS I to IV). They reported that the higher the GMFCS is, the higher the pelvic tilt (retroversion) and the lower sacral slope (vertical sacrum) are. However, no correlation was found regarding pelvic incidence and global sagittal balance (SVA). In our study, all patients were GMFCS V. However, our results confirm that even patients with poorer trunk control (Group 1) tend to have a more retroverted pelvis and a more vertical sacrum than those with better trunk control (Group 2), probably traducing the inefficiency of compensatory mechanisms and therefore the anterior collapse of the spine.
How should sagittal alignment analysis influence surgical planning in CP children?
The results of our study showed that the three questions proposed by Le Huec et al 7 to guide surgical decisions were necessary but not sufficient in the CP population. Pelvic incidence still needs to be assessed to evaluate the necessary postoperative lumbar lordosis but the visibility of the hips and/or the upper sacral endplate can be very poor. The second question (is the patient balanced?) is rarely positive. In addition, balance is a dynamic concept and should, therefore, be evaluated clinically and not radiologically in CP children. The third question (are there compensatory mechanisms?) is always positive. It helps understanding of the preoperative situation but does not influence surgical strategy.
The hip function and range of movement should always be evaluated before surgery, as it could be worsened after pelvic fixation with significant postoperative pelvic tilt and sacral slope modification. The maxTK is a key parameter to analyze to determine instrumentation and fusion levels. In hyperkyphotic patients (Group 1), the risk of proximal junctional kyphosis (PJK) or proximal junctional failure is higher, and fusion should always be extended to T2, or even above in some cases of cervical hyperlordosis. 11 In hypokyphotic patients (Group 2), sublaminar bands or uniplanar screws should be considered to avoid the flattening effect of monoaxial pedicle screws.12,13 Finally, in the rare but challenging cases of hyperlordosis encountered in Group 2, an anterior approach can be discussed before posterior fusion to perform a multilevel disc release or a shortening osteotomy, in order to adapt the postoperative maxLL to pelvic incidence.
Impact of surgery on sagittal alignment in CP patients
The only paper to date that has focused on this question found that sagittal alignment was not significantly modified after posterior fusion. 6 However, this study only included 14 CP patients, among which nine were ambulant and only five were GMFCS V.
Results of our cohort of non-ambulating patients do not confirm this finding, since the lumbopelvic sagittal alignment changed after the procedure, especially in Group 1 with poor trunk control. Pelvic parameters were significantly modified, with a significant increase in sacral slope (p = 0.04) and a decrease in pelvic tilt (p = 0.007). These changes show that compensatory mechanisms (retroversion and vertical sacrum) were not necessary any more after surgery to avoid the anterior spine collapse in severe GMFCS V children. A trend toward maxLL increase was also noted, and more importantly the harmonious shape of the spine was restored, with four or more lordotic levels observed in the instrumented spine in 85% of the cases (versus 29% before surgery) (Fig. 4). Most of the anterior imbalances were corrected, and the most frequent radiological finding was a posterior shift of the fusion mass in sitting position at follow-up. However, no PJK occurred during follow-up, and these SVA measurements on static radiographs need to be further studied and compared with clinical evaluation in the CP population to establish their relevance.
Improving sitting position is the main goal of spine surgery in non-ambulant CP children and some hamstrings lever-arm dysfunction might compromise functional outcomes. Indeed, Group 1 patients with a retroverted pelvis presented shortened hamstrings, and additional distal and/or proximal lengthening was considered to adjust to the postoperative corrected lumbar lordosis. Conversely, Group 2 patients often had shortened hip flexors, which can also require additional procedures if verticalization is still possible after the spino-pelvic fusion.
Improving head control before surgery
Some degree of trunk and/or head control deficit is present in all CP children, in relation to the severity of the neurological impairment and often in correlation with their spinal condition.14,15 Improving head and trunk control should, therefore, be considered during spinal follow-up. In addition, controlling head position is also crucial in the long term to prevent cervical myelopathy. 11 Therapeutic interventions can be passive or active. Da Costa et al 16 have investigated the effect of passive supports, and showed that the level of trunk support (depending on the degree of impairment) improved head stability. They recommended adequate passive head support to optimize the patient's installation by providing gaze stability, but also improving environmental interaction and respiratory and digestive functions.16,17 Spinal orthoses are commonly used as trunk supports, and there is some evidence that bracing may slow down deformity progression while maintaining or improving head and trunk function and stability.18–20 Another option is to use active supports, such as the Headpod (Euromove, Villeneuve-d'Ascq, France), which act like physiotherapy exercises and have also been associated with improved postural control.21,22 Finally, early physical therapy remains crucial and should not be neglected in severe CP patients, not only to help better control their head and trunk, but also to improve upper limb function and visuospatial perception.23,24 In their study, Simon et al 23 reported for example the effectiveness of lateral decubitus handling exercises over ventral decubitus, by recording neck and trunk electromyographic activity tested in three different positions.
In conclusion, sagittal spino-pelvic alignment in non-ambulating CP patients remains difficult to assess, but the pelvifemoral complex should always be evaluated before a surgical procedure. The current literature is poor but our radiological study was able to define two distinct groups among GMFCS V patients, based on the quality of their trunk control. All possible factors that may influence head and trunk posture should be systematically considered and optimized. Finally, dynamic sagittal balance analysis is probably the next step in preoperative CP evaluation, and gait analysis should be further studied in such patients with ambulatory ability to improve the algorithm of surgical decisions.
Footnotes
ASE: Data collection and analysis.
AP: Manuscript revision.
ALS: Data analysis, Manuscript writing.