
Abstract
Objective
Total hip arthroplasty (THA) affects pelvic posture and spinal alignment. These postural changes may further predispose patients to mechanical complications (MCs) after THA. The aim of this study was to conduct a systematic review to investigate whether any high-quality studies have assessed the association between sagittal spinal alignment and MCs after primary THA.
Methods
Inclusion criteria for studies were adult patients (age ≥18 years), primary THA, pre- and postoperative spinopelvic standing sagittal radiographs acquired preoperatively and at a minimum of 6-month follow-up, measurements of spinopelvic parameters, and reporting of possible MCs after THA. The review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines.
Results
Six articles met the inclusion criteria. Although several studies confirmed the importance of spinal alignment when planning THA, these mainly investigated pelvic mobility as a risk factor for THA dislocation. Radiological follow-up imaging practices varied, and studies focused on different individual spinopelvic parameters.
Conclusion
Based on our study findings, no conclusions can be drawn regarding the association between sagittal spinal alignment and MCs after primary THA. Further research is needed to improve our knowledge of the connection between MCs after THA and sagittal spinal alignment.
Keywords
Introduction
Since the early years of modern total hip arthroplasty (THA), the Lewinnek safe zone (determined according to an inclination of 40° ± 10° and an anteversion of 15° ± 10°) has been used for optimal acetabular component orientation to reduce the risk of hip dislocation. 1 However, several studies have since provided evidence that the Lewinnek safe zone does not always predict stability.2–4 When Lewinnek first described the safe zone, the acetabular anteversion and inclination were measured from a supine radiograph taken perpendicular to the anterior pelvic plane (APP).1,2 During postural changes, however, the acetabular cup does not remain static and instead moves with the spinopelvic motion. Furthermore, spinal malalignment may change pelvic mobility and position, which can result in an acetabular cup being out of the expected safe zone.3–5
Sagittal spinal malalignment and compensatory mechanisms are common in adults with symptomatic degenerative spinal conditions without previously diagnosed adult spinal deformity.6,7 Increased pelvic tilt (PT) leads to pelvic retroversion and excessively anteverted acetabular components and is one of the earliest changes seen in the development of spinal malalignment.6,8–10 Additionally, THA affects pelvic posture and spinal alignment.11–16 These changes may further predispose to mechanical complications (MCs), such as hip dislocation, in cases where the sagittal spinal malalignment has not been adjusted with optimal acetabular cup positioning, even though the cup is positioned within the Lewinnek safe zone.11,12,14,17–20
Despite advances in surgical techniques and improvements in implant design, dislocation is still a common complication (3.5%–4.8%) after THA21,22 that leads to early revision surgery (17%–33% of THA revisions).23–26 Recent studies on THA revision and THA dislocation rarely acknowledge the aspect of spinal alignment or mobility.5,12 Conversely, some studies appear to emphasize the importance of full spine radiographs in analyzing spinal alignment and compensatory mechanisms in patients undergoing THA surgery.6,12,27
The aim of this study was to conduct a systematic review to investigate whether the association between sagittal spinal alignment and MCs after THA has been investigated in high-quality studies. A further aim of the study was to ascertain whether there are uniform methods for radiographic imaging and assessment of sagittal spinal alignment with spinopelvic parameters.
Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. 28 The review was registered in the PROSPERO international database of prospectively registered systematic reviews on April 28, 2020 (CRD42020167209). In this study, we received funding for a literature search and English language proofreading from Central Finland Hospital Nova, Jyväskylä, Finland.
Because of the systematic review study design, the data were anonymized, and none of the patients can be identified. Thus, approval from an ethics review committee for the study and patient consent was not required.
Literature search and study selection
We searched MEDLINE, Scopus, Web of Science, the Cochrane Central Register of Controlled Trials, and Medic (University of Helsinki) databases. A trained informatician (TO) assisted in the development of the search strategy (Appendix A). The search period was from January 2000 through 6 May 2021. The initiation date was pre-evaluated to cover all recent published literature that includes THA and spinopelvic parameters. The end date was set to the beginning of the analysis. Any published observational studies, case–control studies, or randomized controlled trials assessing the association between the MCs of primary THA and spinopelvic parameters were considered.
Inclusion criteria for the studies were adult patients (age ≥18 years), primary THA, pre- and postoperative spinopelvic standing sagittal radiographs acquired preoperatively and at a minimum of 6-month follow-up, measurement of spinopelvic parameters, and reporting of possible MCs after THA. THA dislocation, subluxation, impingement, or aseptic loosening were defined as MCs, although studies that did not provide a more precise definition of MCs were also included. Exclusion criteria were case reports or review articles, studies written in a language other than English, and those without clear documentation that the operation was primary THA. The types of outcome measures were (1) changes in spinopelvic parameters after THA and (2) MCs after THA during follow-up.
Data collection and analysis
After removing duplicates, three authors (JR, KK, SH) together screened the article titles and abstracts to identify potentially eligible studies. The full text of potentially eligible studies was assessed independently by the authors. Eighty-two full-text articles failed to meet the inclusion criteria and were excluded. Finally, six studies were included in the review (Figure 1).

Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) 2009 flow diagram. 36
From the included studies, three authors (JR, KK, SH) together extracted the study design, follow-up time points, primary endpoint, main and secondary outcomes, hip and spine measurements, MCs, inclusion and exclusion criteria, sample sizes, and patient characteristics (age, sex, and diagnosis leading to THA). Disagreements in screening, inclusion of studies for full-text review, and data extraction were resolved by the senior author (KK).
Measurement of changes in spinopelvic parameters
Two authors (KK, SH) of this review calculated the change in each spinopelvic parameter after THA by subtracting the reported preoperative parameter from the reported postoperative parameter. However, it was not possible to perform the calculation if the preoperative and/or postoperative parameters were not reported in the study. The change in spinopelvic parameters was reported as positive (+) if the magnitude of the parameter increased after THA and negative (−) if the magnitude of the parameter decreased after THA.
Assessment of risk of bias in the included studies
Two authors (KK, SH) independently assessed the quality and evaluated the risk of bias for the included studies using the Quality In Prognosis Studies tool. This tool considers six bias domains: selection of study participants (I), study attrition (II), prognostic factor measurement (III), outcome measurement (IV), study confounding (V), and statistical analysis and reporting (VI). The six domains each contain three to seven prompting items for which the adequacy of reporting is assessed “yes,” “partial,” “no,” or “unsure” to guide ratings of “low,” “moderate,” or “high” risk of bias.29,30 We considered a study to have a low risk of bias if rated low or moderate in all six domains, with at least four domains considered to be low. We considered a study to have high risk of bias if two or more domains were rated high. The remaining studies were rated as having a moderate risk of bias. Any disagreements in the assessment between the two assessors were resolved by the senior author (KK).
Results
After exclusion, six studies were included in the review. The included studies were published between 2017 and 2021 (Table 1). Two studies were conducted in France, two in the United States, one in Turkey, and one in Japan. Among 646 participants, sex was reported for 501 (78%). Of these 501 participants, 299 (60%) were women and 202 (40%) were men. Participants’ ages ranged from 21 to 84 years (mean 63 years) (Table 2). Time points, follow-up periods, and the included views in radiographs are presented in Table 3.
Information of six included articles.

THA, Total hip arthroplasty.
Characteristics of the included articles.
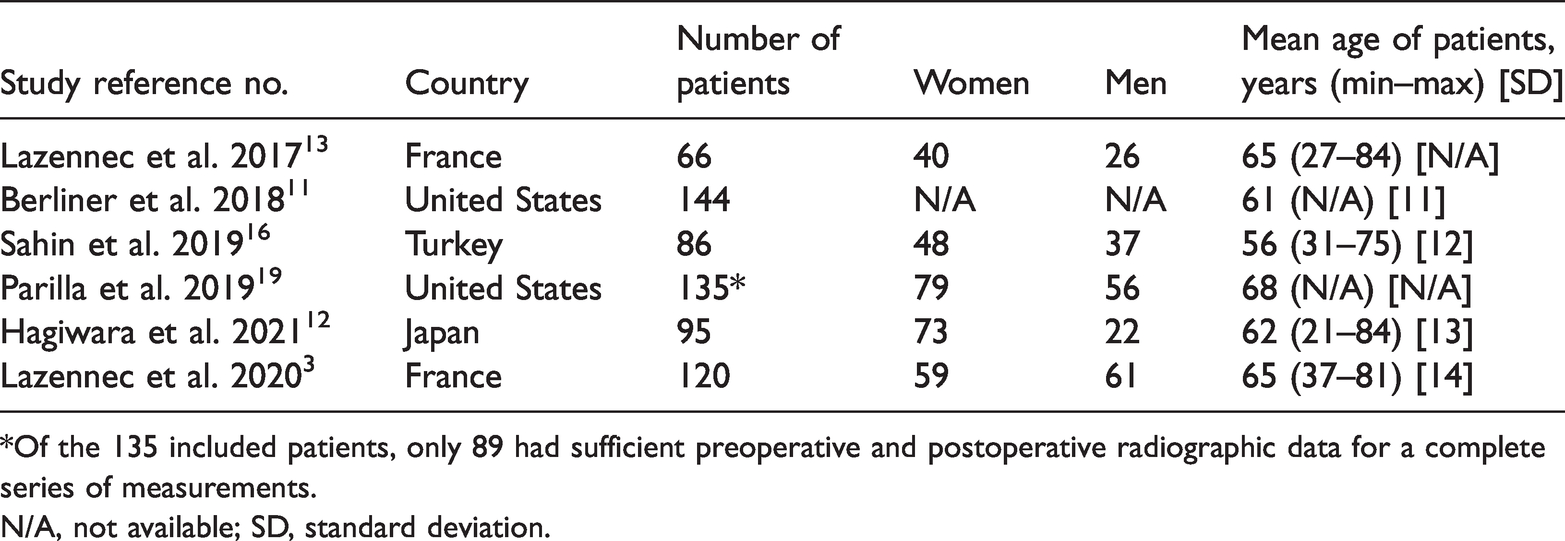
*Of the 135 included patients, only 89 had sufficient preoperative and postoperative radiographic data for a complete series of measurements.
N/A, not available; SD, standard deviation.
Imaging modalities in the six included articles.
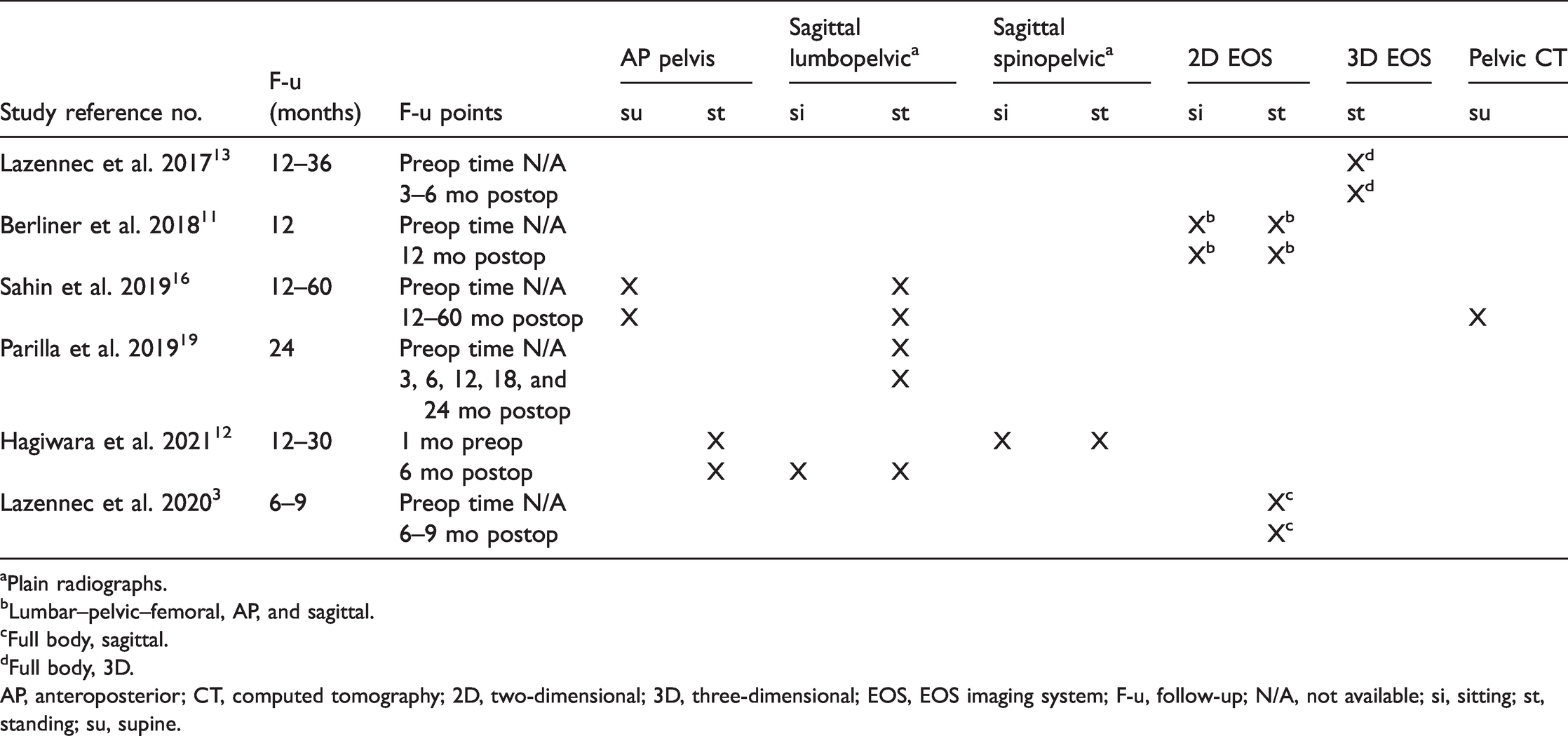
aPlain radiographs.
bLumbar–pelvic–femoral, AP, and sagittal.
cFull body, sagittal.
dFull body, 3D.
AP, anteroposterior; CT, computed tomography; 2D, two-dimensional; 3D, three-dimensional; EOS, EOS imaging system; F-u, follow-up; N/A, not available; si, sitting; st, standing; su, supine.
The mean postoperative changes in spinopelvic parameters are shown in Table 4. In the six included studies, spinopelvic parameters were measured pre- and postoperatively at a minimum of 6 months follow-up, as follows: sacral slope in all six studies, lumbar lordosis in four studies, spinopelvic tilt in three studies, pelvic incidence in four studies, sagittal vertical axis (SVA) in two studies, APP in one study, sagittal spinopelvic translation (SSPT) in one study, and pelvic incidence minus lumbar lordosis mismatch (PI-LL) in one study. Thoracic kyphosis or any other angular measurement of global sagittal spinal alignment (T1 pelvic angle, T1 or T9 sagittal angle) were not measured in any of the six included studies. The measurement of sagittal spinopelvic parameters is shown in Figure 2.
Postoperative changes in spinopelvic parameters in different positions.
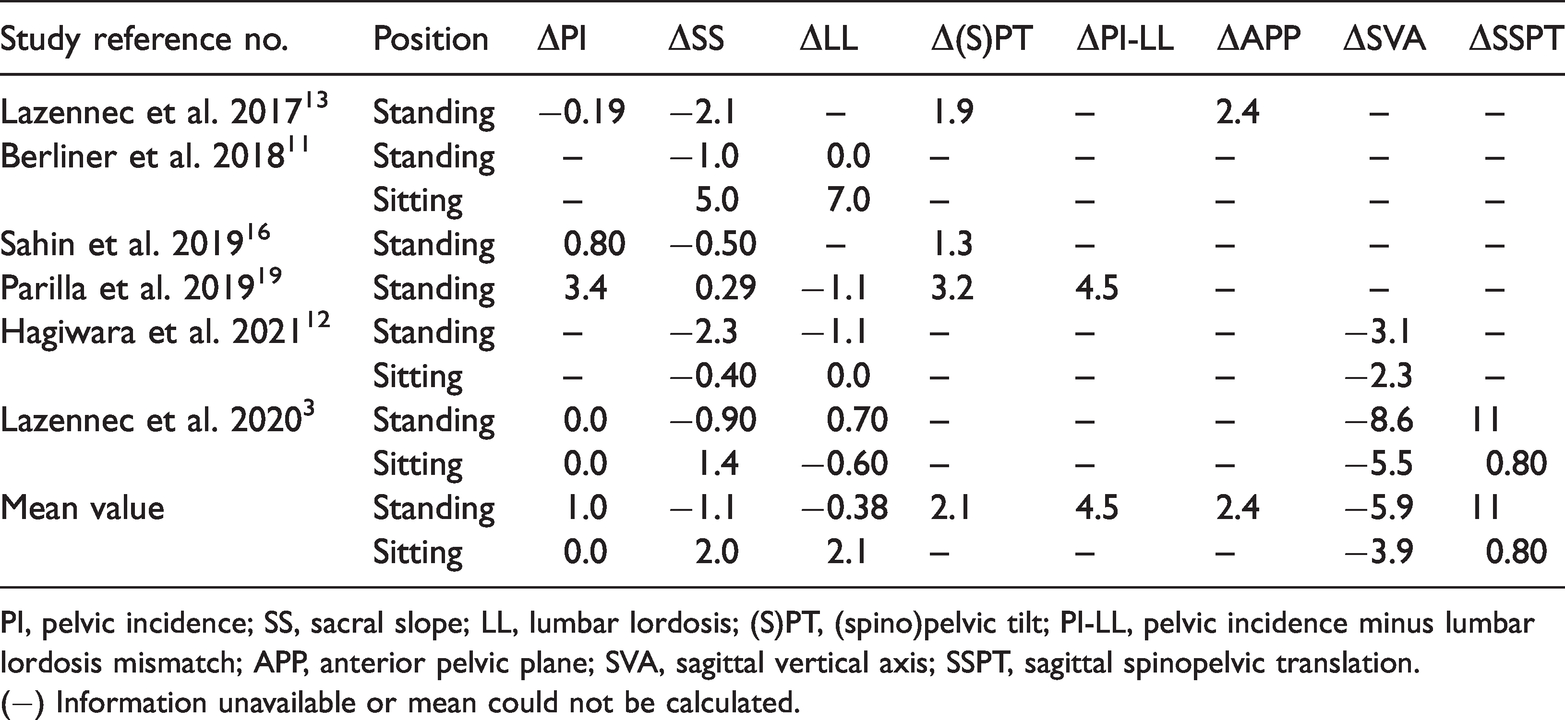
PI, pelvic incidence; SS, sacral slope; LL, lumbar lordosis; (S)PT, (spino)pelvic tilt; PI-LL, pelvic incidence minus lumbar lordosis mismatch; APP, anterior pelvic plane; SVA, sagittal vertical axis; SSPT, sagittal spinopelvic translation.
(−) Information unavailable or mean could not be calculated.
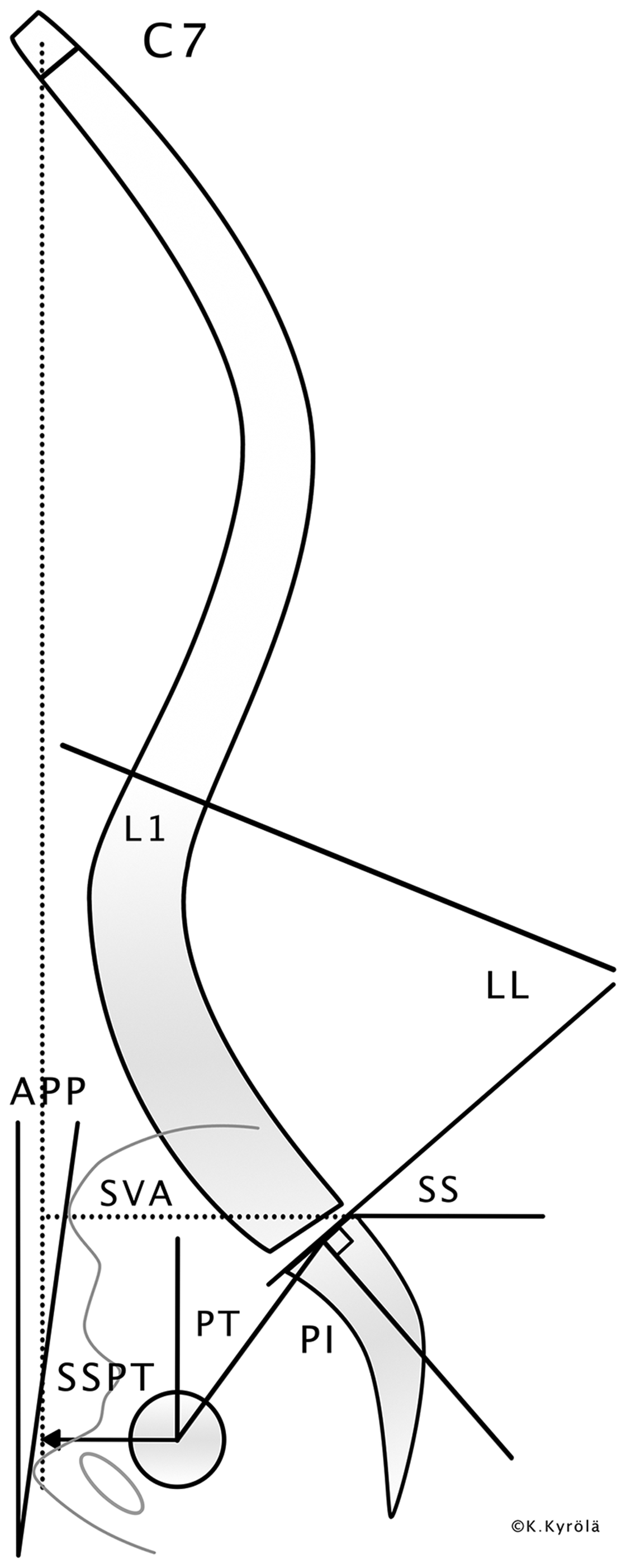
Sagittal spinopelvic parameters reported in the included articles (courtesy of Kati Kyrölä).
During follow-up, MCs of THA were reported in two studies.3,19 No MCs occurred in the remaining studies. In total, 29 of the 646 (4.5%) patients had an MC (Table 5).
Mechanical complications of total hip arthroplasty during the follow-up period.
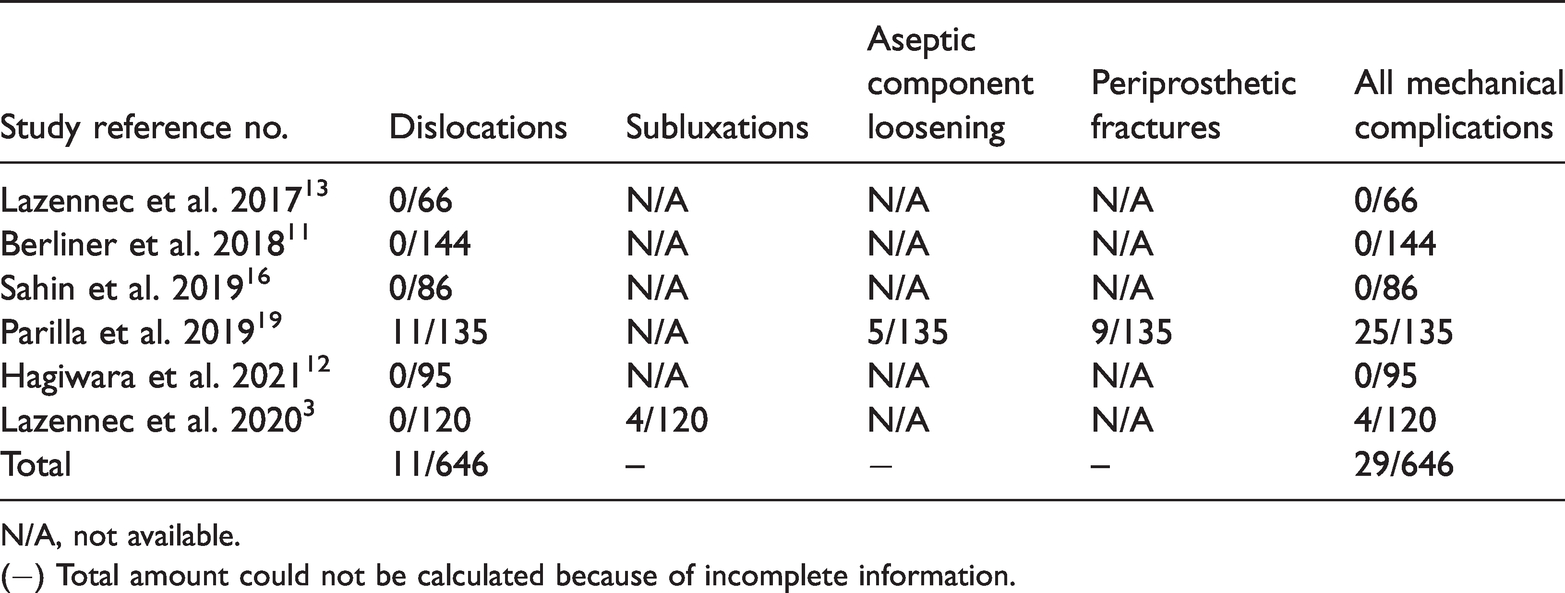
N/A, not available.
(−) Total amount could not be calculated because of incomplete information.
Three studies were considered to have low risk of bias, two to have moderate risk, and one to have high risk (Table 6). Study participation was rated as moderate risk of bias in all studies. Study attrition was judged as low risk of bias in only two studies. Prognostic factor measurement was the only domain rated as low risk of bias in every study; outcome measurement was rated as low risk of bias in five studies. Study confounding was scored as low risk of bias in three studies, moderate in two studies, and high risk in one study. Statistical analysis and reporting were assessed as low risk of bias in four studies, moderate in one, and high risk in one study.
Summary of risk of bias according to the Quality In Prognosis Studies tool.

□ High risk of bias. ● moderate risk of bias. ◊ low risk of bias.
Discussion
The findings of this systematic review suggested that there is limited evidence on how spinopelvic parameters change after primary THA and whether these changes are a risk factor for MCs, such as dislocation. Even though three of the included studies were judged to have a low risk of bias because of incompletely reported and heterogeneous data, no clear conclusions could be drawn regarding how spinal sagittal alignment and MCs after primary THA are associated.
According to our review, it can be concluded that radiographic imaging practices are neither standard nor uniform. Indeed, in some studies included in this review, spinopelvic parameters were followed with a full-body low-dose 2D or 3D X-ray imaging system (EOS) whereas in other studies, spinopelvic parameters were followed with lumbopelvic or full-spine radiographs (Table 3).
In the discussions, three of the included studies seem to confirm the importance of global spinal alignment when planning THA to better understand the hip–spine relationship and identify those patients at high risk for MCs after THA.3,11,12 In the data, however, the articles did not focus on spinal alignment. SVA was the only reported parameter that measures global sagittal alignment of the spine (Table 4). Unlike angular measurements, SVA is prone to image scaling bias and the compensatory mechanisms of the malalignment. 31 Global angular parameters were not reported in any of the included studies. Other spinopelvic parameters were inconsistently measured across the six studies. The terminology of spinopelvic parameters was also not completely uniform. As an example, an anteversion could refer to either a pelvic anteversion or an acetabular anteversion, depending on whether the author was an orthopedic spine surgeon or a joint replacement orthopedic surgeon. There is evidence of a strong correlation between certain spinopelvic parameters (SVA, PT, and PI-LL) and disability and health-related quality of life among adult patients with spinal deformities, 32 and these parameters were measured in some included studies.
The total number of dislocations was reported in all studies, but different MCs were comprehensively specified in only one study 19 (Table 5). Indeed, some of the included studies mainly investigated pelvic mobility instead of global spinal alignment as a risk factor for THA dislocation. Berliner et al. found that patients with fixed spinal alignment are at higher risk for posterior dislocation in the seated position after THA compared with patients who have normal spinal mobility. 11 Moreover, those authors reported that even when hip arthritis has been treated with THA, patients with fixed spinal alignment are unable to accommodate and flex through their spine because the pelvis does not roll back. This may therefore predispose patients to a higher risk for posterior dislocation in the seated position. 11 Hagiwara et al. suggested that a pre-operative flatback with a rigid spine leads to post-operative posterior impingement, and a pre-operative well-balanced spine leads to post-operative anterior impingement. 12 Lazennec et al. found that patients with negative sitting SSPT are at higher risk for THA dislocation than patients with positive sitting SSPT. 3
The main strength of our study is that it covered the entire period during which the spinopelvic parameters are in frequent clinical use.33–35 Additionally, we performed a comprehensive literature search of various electronic databases. This study has several limitations, however. For example, our search did not cover articles published before 2000. The inclusion criterion concerning possible MCs eliminated several relevant articles. Furthermore, the follow-up time was relatively short and concentrated only on the immediate risks related to a possible association with spinal alignment, not long-term changes in the spinopelvic structure.
In conclusion, the findings of this systematic review suggest that there are no high-quality studies on how spinopelvic parameters change after primary THA and whether these changes are risk factors for MCs. According to our study, no conclusions can be drawn regarding the association between sagittal spinal alignment and MCs after primary THA. Because the mechanical measurement of Lewinnek’s safe zone does not guarantee the absence of complications, further studies with larger patient series, standard uniform full-spine sagittal radiographs, and long-term follow-up are required. Such studies would increase our understanding and knowledge of the association between MCs after primary THA and sagittal spinal alignment.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221116976 - Supplemental material for Association between sagittal spinal alignment and mechanical complications after primary total hip arthroplasty: a systematic review
Supplemental material, sj-pdf-1-imr-10.1177_03000605221116976 for Association between sagittal spinal alignment and mechanical complications after primary total hip arthroplasty: a systematic review by Hiltunen Susanna, Repo Jussi, Karjalainen Teemu and Kyrölä Kati in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605221116976 - Supplemental material for Association between sagittal spinal alignment and mechanical complications after primary total hip arthroplasty: a systematic review
Supplemental material, sj-pdf-2-imr-10.1177_03000605221116976 for Association between sagittal spinal alignment and mechanical complications after primary total hip arthroplasty: a systematic review by Hiltunen Susanna, Repo Jussi, Karjalainen Teemu and Kyrölä Kati in Journal of International Medical Research
Supplemental Material
sj-pdf-3-imr-10.1177_03000605221116976 - Supplemental material for Association between sagittal spinal alignment and mechanical complications after primary total hip arthroplasty: a systematic review
Supplemental material, sj-pdf-3-imr-10.1177_03000605221116976 for Association between sagittal spinal alignment and mechanical complications after primary total hip arthroplasty: a systematic review by Hiltunen Susanna, Repo Jussi, Karjalainen Teemu and Kyrölä Kati in Journal of International Medical Research
Footnotes
Acknowledgement
The authors thank Tuulevi Ovaska (TO, University of Eastern Finland), who assisted in the development of the search strategy.
Data availability
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary material. Further information can be requested in writing from the corresponding author.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received funding for a literature search and English language proofreading from Central Finland Hospital Nova, Jyväskylä, Finland.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.