
Abstract
Abstract
Introduction
Simple bone cysts (SBCs) are common in children and adolescents. The risk of refracture and the probability of spontaneous healing in SBCs are mainly dependent on the activity of the cyst and can be quantified with the Cyst-Index. Avoiding pathological fractures is the primary goal. Our study presents a comparison of two different bioresorbable bone graft substitutes (BGSs) in the minimally-invasive treatment of SBC in the active stage by percutaneous cyst aspiration and injection.
Methods
Between 2006 and 2017, 38 patients (aged two to 37 years; mean age 12.4 (sd 5.6)) were treated with percutaneous cyst aspiration and refilled with bioresorbable BGSs in three hospitals. The cysts of 21 patients (11 humerus, five femur, four calcaneus, one fibula) were refilled with porous beta-tricalcium phosphate (PB-TP group) (ChronOS Inject) and of 17 patients (nine humerus, six femur, one calcaneus, one fibula) with hydroxyapatite/calcium sulphate (H/CS group) (CERAMENT|BONE VOID FILLER). There were 13 (62%) preceding fractures in the PB-TP group and eight (47%) in the H/CS group. The follow-up of all patients was at least two years. During follow-up, radiological healing (modified Neer classification), activity level, refracture rates, recurrence rates, resorption period and complications were analyzed.
Results
In all, 21 patients treated with PB-TP group experienced 27 operations (one refracture, three recurrences and one persistent cyst). A total of 17 patients treated with H/CS experienced 20 operations (one refracture and one recurrence). After six weeks, 95% in the PB-TP group returned to unrestricted activity with one refracture in the femur due to insufficient biomechanical stability and all returned to unrestricted activity in the H/CS group. Partial or complete radiological response was observed in 81% after 13 months (sd 3.4). Three recurrences (14%) occurred in the PB-TP group and one recurrence (6%) occurred in the H/CS group. The refracture rates were similar in both groups; one (5%) in the PB-TP group and one (6%) in the H/CS group. All H/CS treated cysts showed completed resorption after two years, whilst in PB-TP treated cysts no resorption occurred in five cases (25%) (p = 0.031). Two (10%) wound infections occurred in the PB-TP group and no infections occurred in the H/CS group.
Conclusion
Both PB-TP and H/CS can provide stability and prevent refracture in patients with single bone cysts at the upper extremity or the foot. For the proximal femur, additional stabilization is necessary, due to the weight-bearing and associated high refracture rate. The H/CS bone graft substitute has a better resorption rate than the PB-TP graft.
Level of Evidence
III
Keywords
Introduction
The simple bone cyst (SBC) is a benign fluid-filled cystic lytic lesion 1 which is common in children and adolescents, with two/three to one male predominance. About 80% of patients are in their second decade. SBCs contain serosanguinous or serous fluid, and they are located centrally in the metaphyses of the bone. Although SBCs can affect any bone, they mainly occur in the long bones; the most common sites are the proximal humerus (50%), the proximal femur (25%) and the proximal tibia. 2 The precise pathogenesis of SBC is unknown to date; they are presumed to develop as a result of a bone growth defect where the fluid fills this defect which leads to thinning and expanding of the overlying bone. 1
SBCs typically remain asymptomatic and are often discovered incidentally. However, since the cysts can thin out and weaken the involved bone cortex, SBCs are associated with a high risk of fracture. 3 The risk of a fracture and the probability of spontaneous healing in SBCs are mainly dependent on the activity of the cyst and can be quantified with the Cyst-Index4–5. Currently recommended treatment options include curettage and bone-grafting, intralesional injections with corticosteroids, bone marrow, demineralized bone matrix (DBM) or calcium-phosphate bone cement, 6 decompression, internal fixation and also combinations of these. 7 Even though the treatment options are all associated with high recurrence rates, 8 it has been shown that active treatment strategies are normally superior to conservative treatment. 9 The primary goal of the treatment of SBCs is avoiding pathological fracture.
The aim of this study was to retrospectively compare the outcomes of patients that were treated with one of two different bioresorbable bone graft substitutes (BGSs), one beta-tricalcium phosphate (BT-TP) and one hydroxyapatite/calcium sulphate (H/CS), that were used in a minimally invasive treatment concept of percutaneous cyst aspiration, lavage and intralesional injection.
Patients and methods
Study design and materials
We retrospectively collected and analyzed the data of patients who had undergone a percutaneous treatment of active SBC at the University Children's Hospital Basel, the Cantonal Hospital Aarau and the Cantonal Hospital in Bellinzona, Switzerland, using two different BGSs between 2006 and 2017.
In all cases the diagnosis of SBCs was confirmed by histology.
The two bioresorbable BGS were ChronOS Inject (DePuy Synthes, Oberdorf, Switzerland) and CERAMENT|BONE VOID FILLER or CERAMENT|G (BONESUPPORT AB, Lund, Sweden).
ChronOS Inject BONE VOID FILLER consists of PB-TP. The total porosity is about 55%, the pore size is 300µ. 10
CERAMENT|BONE VOID FILLER consists of 40% hydroxyapatite and 60% calcium sulphate (H/CS), with an initial porosity of 40% to 50% and an average pore size of < 1 mm. CERAMENT G is made of the same ceramic powders as CERAMENT BONE VOID FILLER. It is mixed with gentamicin sulphate in a saline solution to generate an injectable material. 11
The first 21 patients treated by PB-TP were the PB-TP group and the following 17 patients treated by H/CS were the H/CS group.
Cyst-Index and cyst activity levels were collected before the operation. All patients were treated by percutaneous cyst aspiration followed by injection of the above-mentioned bioresorbable bone cements. At follow-up, we assessed patients’ radiological healing (modified Neer classification 12 ), refracture rates, recurrence rates, resorption rates and complications.
Surgical technique
Indications for the surgery were pain (potentially caused by micro fractures), cysts with a high fracture risk (according to Cyst-Index) and/or relapse after fracture. Anatomical locations with higher risk of infection, e.g. at the foot, were managed using a BGS containing gentamicin (H/CS group).
The percutaneous cyst aspiration method was described by Clayer. 13 The main procedure includes:
fluoroscopy localization;
percutaneous aspiration of the cyst over two percutaneous needles (trocars) and controlled by fluoroscopy;
installation of contrast fluid for analysis of size and additional walls;
mechanical destroying of additional cyst walls;
lavage with hydrogen peroxide followed by saline wash out;
injection of bioresorbable bone cement and controlled again by fluoroscopy.
Cyst healing grade
After the percutaneous aspiration operation, the patients were followed up quarterly during the first year and every six months during the second year. Modified Neer Classification was used as radiological measure for the healing of SBC.12,14–16 Final radiographic outcome was assessed 24 months after the surgery and the healing time was recorded.
Fully healed was defined as ‘cyst filled by new bone, with no or only small radiolucent area(s) of < 1 cm in diameter’. Healed with defect (partially healed cyst) was defined as ‘radiolucent area(s) with a diameter that is smaller than 50% of the diameter of the bone, with enough cortical thickness to prevent fracture’. Persistent cyst was defined as ‘radiolucent area with a diameter that is larger than 50% of the diameter of the bone and with a thin cortical rim, but no increase of the size of the cyst’ (continued restriction of activity or repeated treatment is required for this grade). Recurrence was defined as ‘cyst reappearing in a previously obliterated area, or increased size of a residual radiolucent area’. Healed outcome was defined as ‘a cyst that has fully healed or healed with defect’. Not healed outcome was defined as ‘persistent cyst and recurrent cyst’.
Cyst activity and Cyst-Index
Cyst activity: a cyst with a distance from the growth plate of ≤ 0.5 cm was considered active, whereas a cyst with a distance from the growth plate of > 0.5 cm was considered latent.12,17 The distance was measured by GE Centricity web review (General Electric Company, Boston, Massachusetts, United States).
Cyst-Index: the Cyst-Index is the ratio between the projected surface and the square of the diaphyseal bone diameter.4,5,18 The surface and diaphyseal bone diameter were measured by AutoCAD (Version 2019, Autodesk Inc., Mill Valley, California, United States).
Statistical analysis
SPSS 26.0 (IBM, Armonk, New York) was used for the statistical analyses. The differences between rates were assessed by a chi-squared test or a Fisher exact test. All tests were performed at a significance level of α = 0.05. The graph was created with GraphPad Prism (Version 6.0c, San Diego, California, United States).
Results
Between 2006 and 2017, 38 patients (mean age: 12.4 years (sd 5.6); 2.6 to 37.3) with SBC were treated with percutaneous cyst aspiration at the three participating hospitals. All patients and/or their parents agreed to be enrolled in the study and signed the informed consent form. Demographic data of SBC patients are reported in Tables 1, 2 and 3. The minimum follow-up of all patients was two years.
Demographic data for patients with simple bone cyst (SBC)
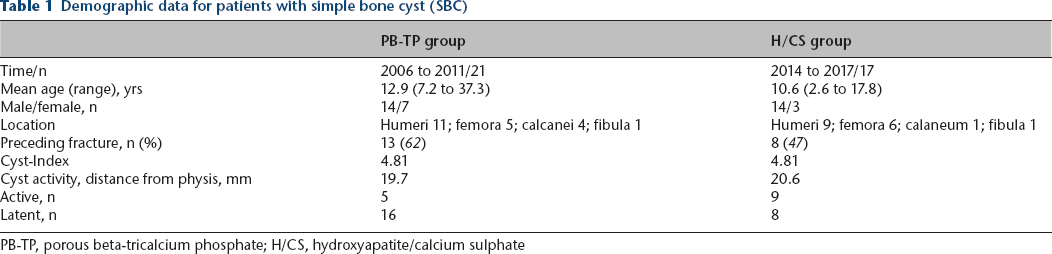
PB-TP, porous beta-tricalcium phosphate; H/CS, hydroxyapatite/calcium sulphate
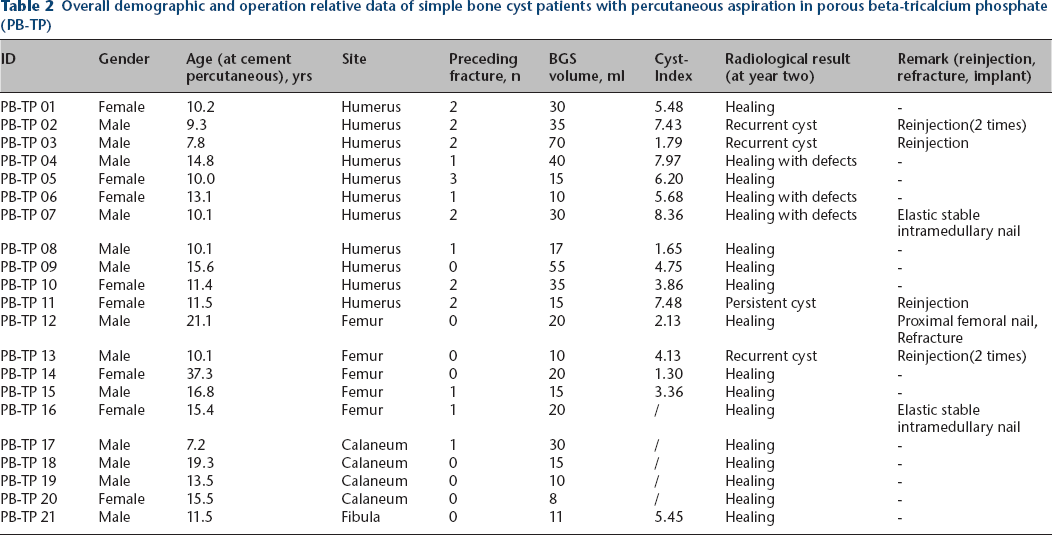
Overall demographic and operation relative data of simple bone cyst patients with percutaneous aspiration in porous beta-tricalcium phosphate (PB-TP)
Overall demographic and operation relative data of simple bone cyst patients with percutaneous aspiration in hydroxyapatite/calcium sulphate (H/CS) group
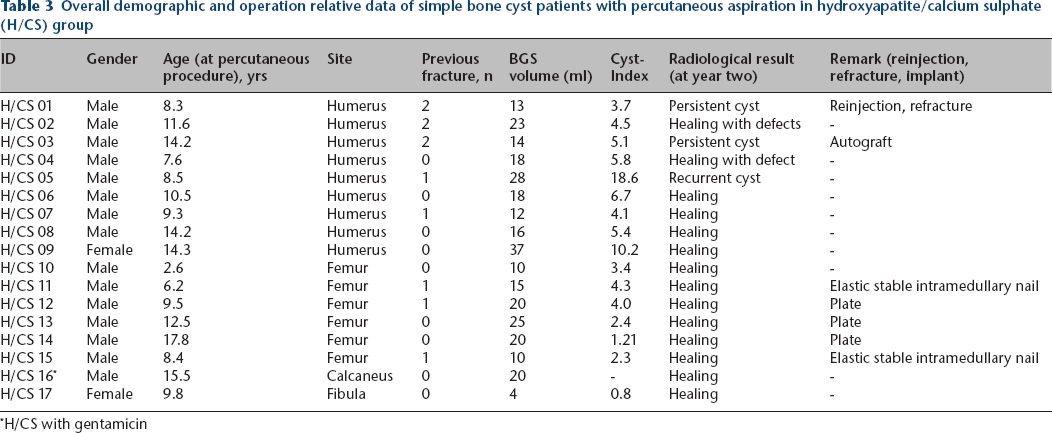
H/CS with gentamicin
Cyst activity and Cyst-Index
Average cyst activity was not statistically different in the two groups (19.7 mm in the BP-TP group and 20.6 mm in the H/CS group). However, concerning the classification in active and latent cysts according to the definition, 23.8% of the SBCs were classified as active in the PB-TP group versus 52.9% in the H/CS group. The Cyst-Index scored exactly the same value of 4.81 in both groups.
PB-TP group
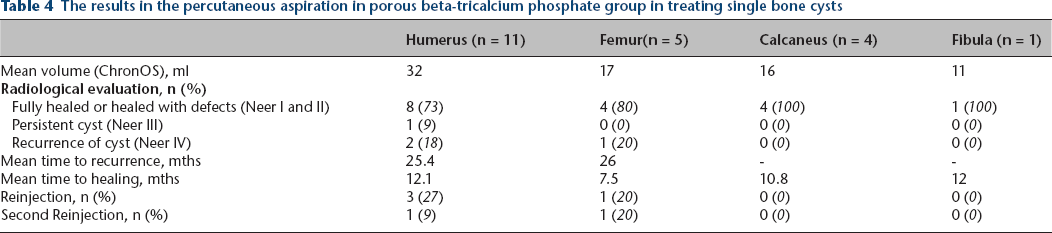
In total, 21 patients with a mean age of 12.9 years (7.2 to 37.3) were enrolled in the PB-TP group (Table 1). Affected bones were humerus (11), femur (five), calcaneus (four) and fibula (one). In all, 13 (62%) of the patients had previous pathological fractures through the cysts. During follow-up, three recurrences (14%) of cysts and one persistent cyst were recorded after a mean of 25.4 months (Table 4). These cases were treated with repeated aspiration of cyst liquid and injection of PB-TP. In two of the recurrent cysts, the aspiration and injection of PB-TP had to be repeated for a second time. In total, the 21 patients had 27 aspiration and PB-TP injection treatment episodes. One patient (5%) had a refracture at the femur after six months.
The results in the percutaneous aspiration in porous beta-tricalcium phosphate group in treating single bone cysts
H/CS group
A total of 17 patients with a mean age of 10.6 years (2.6 to 17.8) were allocated to the H/CS group (Table 1). Affected bones were humerus (nine), femur (six), calcaneus (one) and fibula (one). Eight (47%) of the patients had previous fractures. There was one recurrence of a cyst and two persistent cysts. The recurrence did not require further treatment, while one of the persistent cysts was treated with repeated aspiration and injection of H/CS and the other was curetted and filled with autograft. In total, the 17 patients had 18 aspiration and PB-TP injection treatment episodes and one open revision surgery. One patient (6%) had a refracture at the humerus after six months. This was in the same patient with a persistent cyst treated by repeated aspiration and injection.
Cyst healing grade
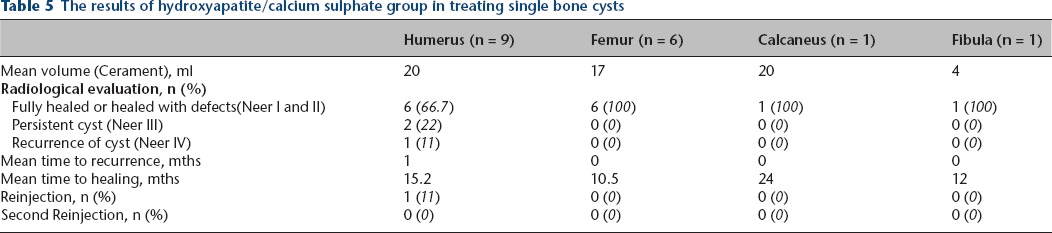
Neer I and II grades (fully healed and healed with defects) were observed in 31 (81.6%) of all patients. Healing rate was 81.0% in the PB-TP group, with four Neer III and IV graded (persistent or recurrent cyst) cases (Table 4). In the H/CS group, the healing rate was 82.4%, with 3 Neer III and Neer IV graded cases (Tables 5 and 6) (p = 1.000).
The results of hydroxyapatite/calcium sulphate group in treating single bone cysts
Outcomes of porous beta-tricalcium phosphate (PB-TP) group and hydroxyapatite/calcium sulphate (H/CS) group
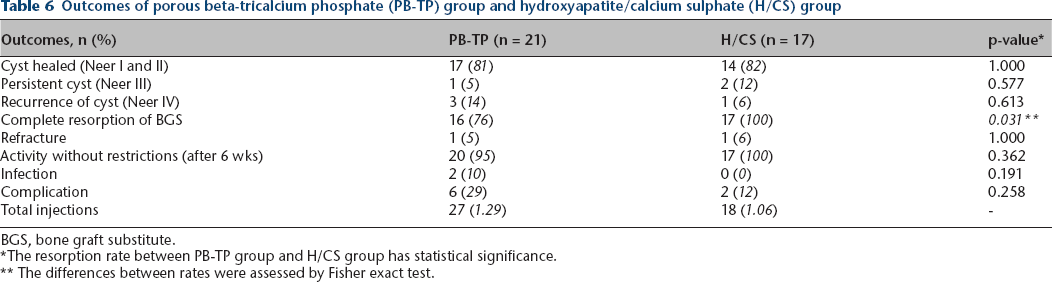
BGS, bone graft substitute.
The resorption rate between PB-TP group and H/CS group has statistical significance.
The differences between rates were assessed by Fisher exact test.
The mean healing time in the PB-TP group was 13.3 months (sd 1.6) and 11.5 months (sd 1.4) in the H/CS group (p = 0.461) (Fig. 1).
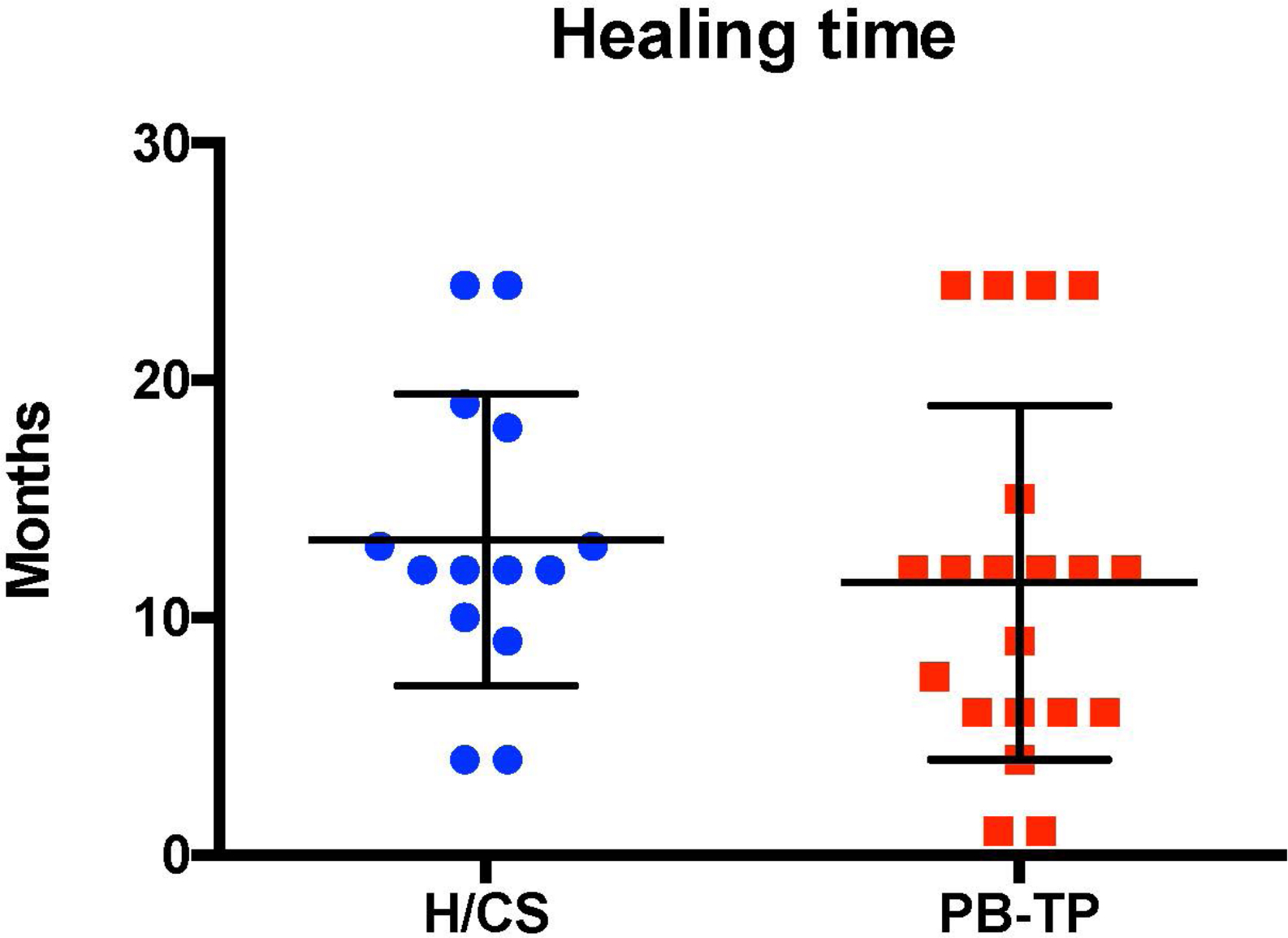
Results of healing time in porous beta-tricalcium phosphate (PB-TP) and hydroxyapatite/calcium sulphate (H/CS) group (p = 0.461).
The resorption rate at 24 months was 76% (five incomplete resorption cases) in the PB-TP group and 100% in the H/CS group. This difference was statistically significant (p = 0.031) (Table 6).
After six weeks, 95% of the patients in the PB-TP group had returned to unrestricted activity. One refracture in at the femur occurred because of insufficient biomechanical stability. In all, 100% of the patients in the H/CS group had returned to unrestricted activity (p = 0.362) (Table 6).
Two wound infections were recorded in the PB-TP group after percutaneous cyst aspiration, whereas no infection occurred in the H/CS group (p = 0.191) (Table 6).
The total complication rates (recurrence, refracture and infection) were 29% in the PB-TP group and 12% in the H/CS group (p = 0.258) (Table 6).
Discussion
The treatment of SBC
Different strategies have been developed to treat symptomatic SBCs in the past: 7 curettage and bone grafting, intralesional injections with corticosteroids, bone marrow, DBM or calcium-phosphate bone cement, decompression and internal fixation. In this study, we used the percutaneous aspiration method to inject two different bioresorbable BGSs. It is a minimally invasive method with little soft tissue involvement and scarring (Fig. 4). Therefore, the recovery time is very short. In our study, the bone healing rate was comparable with other injection methods reported in the literature; 9 it was 84.2% in total, 95.2% in the PB-TP group and 82.4% in the H/CS group. A recent meta-analysis 9 reported the following healing rates: overall injection healing rate 81.3%; 77.4% after MPA (medroxyprogesterone acetate) injection; 77.9% after bone marrow injection; and 98.7% after bone marrow and DBM injection. In our study, the percutaneous aspiration resulted in early unrestricted activity; almost all patients (except for one refracture case) were able to return to unrestricted activity six weeks after the operation, and with an aesthetically pleasing scar.
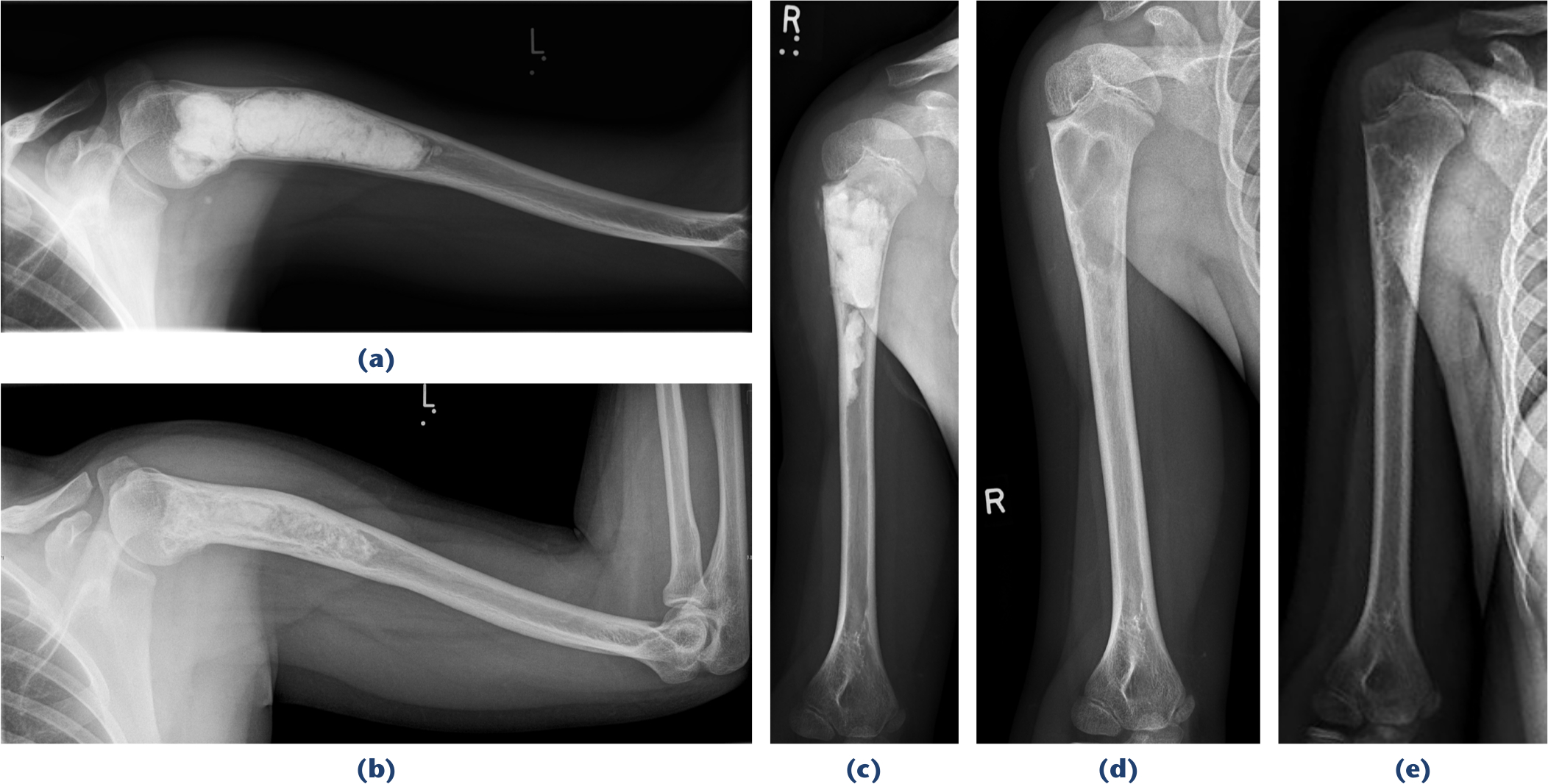
Radiograph of different resorption situation: a and b) an incomplete resorption single bone cyst (SBC) case by using porous beta-tricalcium phosphate;

Absorption processing in a fibula hydroxyapatite/calcium sulphate filled case;
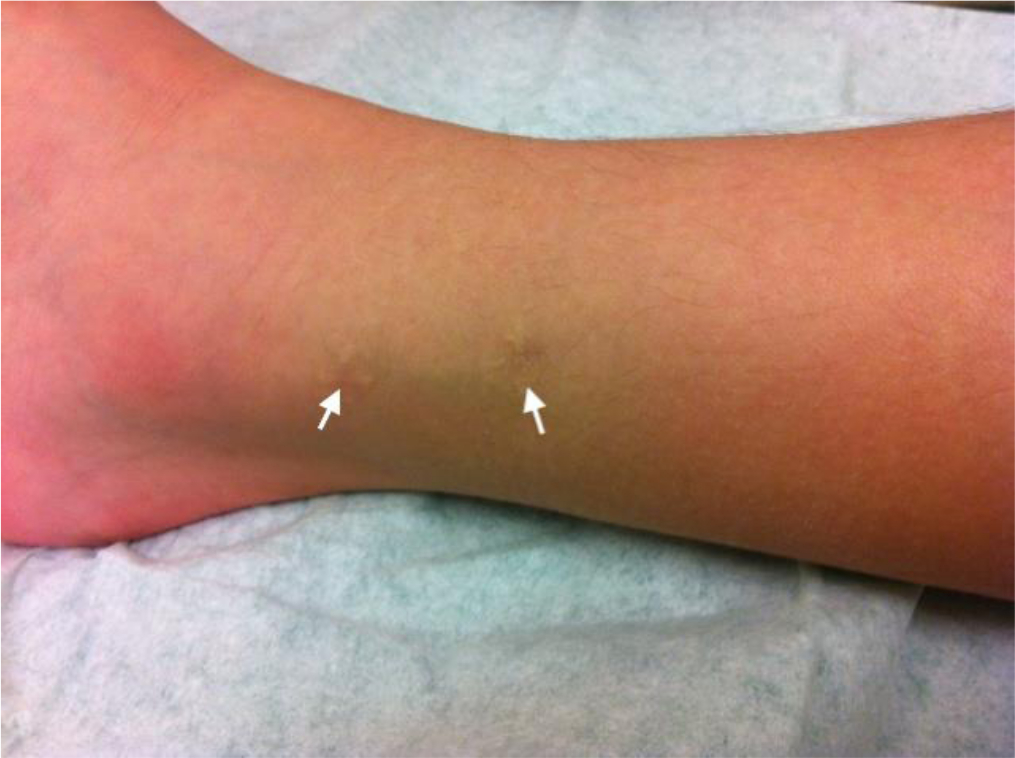
Cutaneous scar after operation. White arrows are two inserting points, both the child and her parents are satisfied with the outcome.
Flexible intramedullary nails were used to provide structural stability in fracture cases, which can disrupt the cyst lining and may decompress the cyst.7,19 Roposch et al 19 demonstrated that treatment with intramedullary nails without curettage provided an almost 100% healing rate of SBC in long bones. Intramedullary nails were described as an efficient acute treatment for SBC that present with a fracture. 20 In procedures where other nails are used, the nail ends often disturb the tissue in the insertion region and a second operation is required for removal of the metal. 21 Jamshidi et al 22 reported of using locking plate and fibular strut-graft augmentation to reconstruct the of SBCs of proximal femur in 14 paediatric patients and got a favourable outcome without recurrence and response. In our experience, additional stabilization is only necessary for the proximal femur, due to the weight-bearing function of this bone and the associated high refracture rate.
The conservative therapy is mainly used in patients in which the SBC was incidentally discovered or in cases with no dislocated fractures at the upper limb. The indication of surgery normally includes: patients with pain, high risk fracture risk mentioned above, fracture after recurrence and dislocated pathologic fracture. Actually, the main aim in treatment is prevention for pathological facture and symptom management.
Cyst-Index
Using the Cyst-Index to predict the risk of fracture in SBC patients was first described by Kaelin and MacEwen. 4 The Cyst-Index is used to evaluate and estimate the risk of a pathological fracture and the spontaneous outcome. A Cyst-Index of > 3.9 for the humerus and > 3.6 for the femur indicates that almost no further risk of a pathological fracture exists. 5 It has been the subject of controversial discussion, however, whether the Cyst-Index is a good predictor for SBC fracture. Vasconcellos et al 18 considered the Cyst-Index to be a non-accurate predictor for fracture, however, Pireau et al 23 considered the Cyst-Index as the best predictor for the risk of SBCs’ fracture.
Complications
The common complications of SBCs include recurrence, refracture, infection and epiphyseal arrest.7,12,22,24 A 15% complication rate was reported by Oppenheim and Galleno, 24 and included infection, coxa vara, epiphyseal arrest and limb shortening. Nystrom et al 25 reported of four SBC patients that were treated by aspiration and injection of calcium sulphate; three of them experienced acute laryngospasm and one patient developed a temporary tachyarrhythmia, which the author hypothesized that it was associated with the injection of calcium sulphate or a systemic calcium bolus. The possible reason could be the local toxicity and acidic microenvironment caused by calcium sulphate. 26 None of the 38 patients that participated in our study has developed laryngospasms or tachyarrhythmia; this is probably due to the development of the new calcium material. Two patients in the PB-TP group suffered from an infection after the percutaneous cyst aspiration and no infection occurred in the H/CS group (p = 0.191) (Table 6). The total complication rates (recurrence, refracture and infection) were 29% in the PB-TP group and 12% in the H/CS group (p = 0.258) (Table 6).
Resorption
Resorption of the BGSs should be observed carefully, as osteoclasts activated by resorption may release clastokines, including Tartrated Resistant Acid Phosphatse (TRAcP), sphingosine-1-phosphate, Bone Morphogenetic Protein-6 (BMP6), wingless-type 10b, hepatocyte growth factor, collagen triple helix repeat-containing protein 1, where these factors activate preosteoblasts and osteoblasts.27–29 Kurashina et al 30 demonstrated that the degradation rate of the materials may be one of the affecting factors in ceramic-induced osteogenesis. In our study, the resorption rate at two years follow-up was 76.2% (five incomplete resorptions) in the PB-TP group and 100% in the H/CS group; this difference was statistically significant (p = 0.031). This difference is probably caused by different major constituents of two bioresorbable cement: ChronOS Inject with PB-TP and in CERAMENT BONE VOID FILLER and CERAMENT G with H/CS. However, evidence to compare the resorption times of different cement material is lacking. Winkler et al 31 demonstrated that tricalcium phosphate ceramics show more rapid degradation than hydroxyapatite ceramics which was related to pronounced particular desintegration of tricalcium phosphate ceramics. In our study, H/CS consists of 40% hydroxyapatite, which is lower than in other studies, the hydroxyapatite microparticles embedded in the calcium sulphate show a different resorption profile than commonly used hydroxyapatite blocks. However, the clinical resorption parameters maybe different and should be carefully observed.
Limitations
The small sample size may have led to a choosing bias. The retrospective nature of this study and the fact that the trial is insufficiently powered allow no conclusion on which cement material is superior or on the verification that the injection of bone cements is superior to any other treatment.
Conclusion
Percutaneous cyst aspiration can offer many advantages for patients including: minimal invasion procedure, easy postoperative management, reduced school absence, early unrestricted activity and an aesthetically pleasing scar. Both cement materials can provide stability and prevent refracture of patients with SBCs at the upper extremity or the foot. For the proximal femur, additional stabilization is necessary, due to the weight-bearing and associated high refracture rate. The H/CS bone graft substitute has a better resorption rate than the PB-TP graft.
Footnotes
Acknowledgements
We would like to thank Dr Mark Clayer, Department of Orthopaedic and Trauma, Royal Adelaide Hospital, Adelaide, South Australia. The percutaneous aspiration was instructed to the corresponding author during his fellowship.
PK: Data collection, Manuscript preparation.
CA: Data collection, Manuscript preparation.
VDR: Data collection, Manuscript preparation.
AHK: Study design; Supervision; Writing – review and editing.