
Abstract
Abstract
Purpose
To report functional mobility in patients with diplegic cerebral palsy (CP) at long-term follow-up after single-event multilevel surgery (SEMLS). The secondary aim was to assess the relationship between functional mobility and quality of life (QoL) in patients previously treated with SEMLS.
Methods
A total of 61 patients with diplegic CP, mean age at surgery 11 years, eight months (sd 2 years, 5 months), were included. A mean of eight years (sd 3 years, 10 months) after SEMLS, patients were contacted and asked to complete the Functional Mobility Scale (FMS) questionnaire over the telephone and given a weblink to complete an online version of the CP QOL Teen. FMS was recorded for all patients and CP QOL Teen for 23 patients (38%).
Results
Of patients graded Gross Motor Function Classification System (GMFCS) I and II preoperatively, at long-term follow-up the proportion walking independently at home, school/work and in the community was 71% (20/28), 57% (16/28) and 57% (16/28), respectively. Of patients graded GMFCS III preoperatively, at long-term follow-up 82% (27/33) and 76% (25/33) were walking either independently or with an assistive device at home and school/work, respectively, while over community distances 61% (20/33) required a wheelchair. The only significant association between QoL and functional mobility was better ‘feelings about function’ in patients with better home FMS scores (r = 0.55; 95% confidence interval 0.15 to 0.79; p = 0.01).
Conclusion
The majority of children maintained their preoperative level of functional mobility at long-term follow-up after SEMLS.
Level of Evidence
IV
Introduction
Cerebral palsy (CP) is a disorder of movement and posture caused by a defect or lesion of the immature brain. 1 Differential growth between muscle-tendon units and bone results in muscle-tendon contractures, torsion of long bones and joint contractures or instability.2–4 The musculoskeletal sequelae of CP contribute to gait impairments, activity limitations and participation restrictions.4,5 Over the last three decades, single-level surgery has been replaced with the concept of single-event multilevel surgery (SEMLS), in which deformities at multiple anatomical levels are addressed during the same operative procedure.6–8
Studies evaluating SEMLS for children with CP usually focus on gait-related outcomes. 8 There are now multiple reports that SEMLS improves gait kinematics at both short9–13 and long-term follow-up.10,13 However, the impact of SEMLS on functional mobility and quality of life (QoL) is less well understood as these domains have not been fully investigated.8,14,15 The literature on function and QoL following SEMLS for children with CP is limited by small study samples9,16–20 and short-term follow-up.12,17,18,20–23 Previous studies have reported stability of the Gross Motor Function Classification System (GMFCS) in patients with CP over time,24–26 including after SEMLS, 27 and the GMFCS is suggested as an ideal classification tool. The primary aim of this study was to report the functional mobility of patients with diplegic CP at long-term follow-up after SEMLS with respect to their preoperative Gross Motor Function Classification System (GMFCS) grade. We hypothesize that patients would maintain functional mobility at long-term follow-up relative to their preoperative mobility status. The secondary aim was to assess if functional mobility is related to QoL in patients previously treated with SEMLS.
Materials and methods
Study design and setting
This study was a case series of children with CP that underwent SEMLS in a tertiary referral centre between 1 January 2005 and 31 December 2016 (level IV evidence). The study was approved by the Clinical Governance and Audit Team (ID: 5085).
Participants
Patients were included if they met the following criteria: 1) diplegic CP; 2) GMFCS I to III; 5 3) SEMLS at age ≤ 18; 4) and completed the Functional Mobility Scale (FMS) questionnaire at long-term follow-up. 28 SEMLS was defined as two or more bone and/or soft-tissue procedures at two or more anatomical levels bilaterally during one operative procedure. 8
The gait laboratory database at our institution identified 74 eligible patients. Of these, 13 were excluded: six underwent surgery at a different unit and seven could not be contacted. Only one patient was classified as GMFCS I. As patients graded GMFCS I and II are, by definition, independent ambulators, these groups were combined when performing analyses.
Outcome measures
Patients undergoing SEMLS at our institution are routinely assessed with 3D gait analysis preoperatively and six, 12 and 24 months postoperatively. The cohort of 61 patients included in the study was subsequently contacted to evaluate long-term functional mobility and QoL. In May 2018 we contacted the patients meeting the inclusion criteria by telephone. If appropriate we asked the patient, but if not, we asked the parents to complete the FMS questionnaire over the telephone. FMS rates walking ability at three specified distances (five metres, 50 metres and 500 metres), taking into account the range of assistive devices a child/adolescent might use. 28 These distances represent the patient's mobility at home, school/work and in the community.
Following completion of the FMS questionnaire over the telephone, we assessed QoL using an online adapted version of the CP QOL Teen self-reported version 2. 29 The CP QOL Teen is a condition-specific QoL instrument that reports on five domains of QoL including ‘general wellbeing and participation’, ‘communication and physical health’, ‘school wellbeing’, ‘social wellbeing’ and ‘feelings about function’. Following the authors’ permission, minor adaptions were made to make the questions applicable to the age of all patients (11 years, 10 months to 31 years, 4 months). Questions pertaining to school-related issues were modified for adults at work (e.g. ‘How do you feel about how you are accepted by other students at school or individuals at work?’) and a question relating to changes during puberty were only asked to those under 18 years old. The adapted CP QOL was converted into an online questionnaire, using REDCap electronic data capture tools (Vanderbilt University Medical Centre, Nashville, Tennessee), 30 and a link to complete it online was sent to patients or parents. In an attempt to increase participation, an e-mail reminder was sent one and two weeks after the initial invitation to those who had not completed the online questionnaire.
Due to concerns about multiple testing when the QoL domains are examined against the FMS, hypotheses were formulated prior to the study. Firstly, we hypothesized that in patients graded GMFCS I and II preoperatively, better ‘feelings about function’ would be associated with better community FMS scores. Secondly, we hypothesized that in patients graded GMFCS III preoperatively, better ‘feelings about function’ would be associated with better home FMS scores.
Although all 61 patients completed the FMS questionnaire over the telephone at long-term follow-up, only 23 (38%) responded to the weblink to complete the online CP QOL Teen self-reported version 2. There were no significant differences in sex, GMFCS grade, age at surgery, preoperative Gait Profile Score (GPS), 31 FMS scores or age at long-term follow-up between responders and non-responders.
The GPS at the routine 24-month postoperative gait analysis was compared with the preoperative value. A medical records review was performed to identify the surgical procedures performed as part of the SEMLS.
Statistical analysis
Continuous variables were summarized by mean and sd. Change in GPS was analyzed using a paired t-test. FMS was summarized by median and range. The associations between the five domains of QoL and FMS scores were summarized using Pearson correlation coefficients and tested for statistical significance. The QoL postulates were examined using methods of linear regression. Comparison of QoL domains between GMFCS grades I and II versus grade III utilized Student t-tests. The analyses were performed using IBM SPSS Statistics 24 (Armonk, New York). Statistical significance was concluded when p < 0.05.
Results
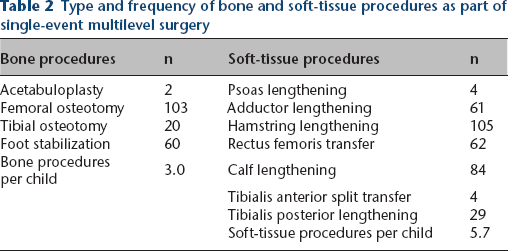
Demographics of the 61 included patients are reported in Table 1. There was a significant improvement in GPS from preoperative to 24 months postoperatively (mean 3.3°; sd 4.8; p < 0.001). There was a mean of 3.0 bone (sd 1.5) and 5.7 soft-tissue (sd 2.0) procedures per child as part of the SEMLS (Table 2).
Demographics of included patients
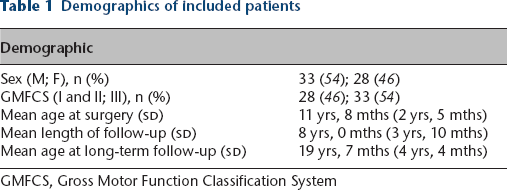
GMFCS, Gross Motor Function Classification System
Type and frequency of bone and soft-tissue procedures as part of single-event multilevel surgery
Of patients graded GMFCS I and II preoperatively, at long-term follow-up the median FMS score at home, school/work and in the community was 5 (1 to 6), 5 (1 to 6) and 5 (1 to 6), respectively. At long-term follow-up, the proportion walking independently at home, school/work and in the community was 71% (20/28; Fig. 1a), 57% (16/28; Fig. 1b) and 57% (16/28; Fig. 1c), respectively.
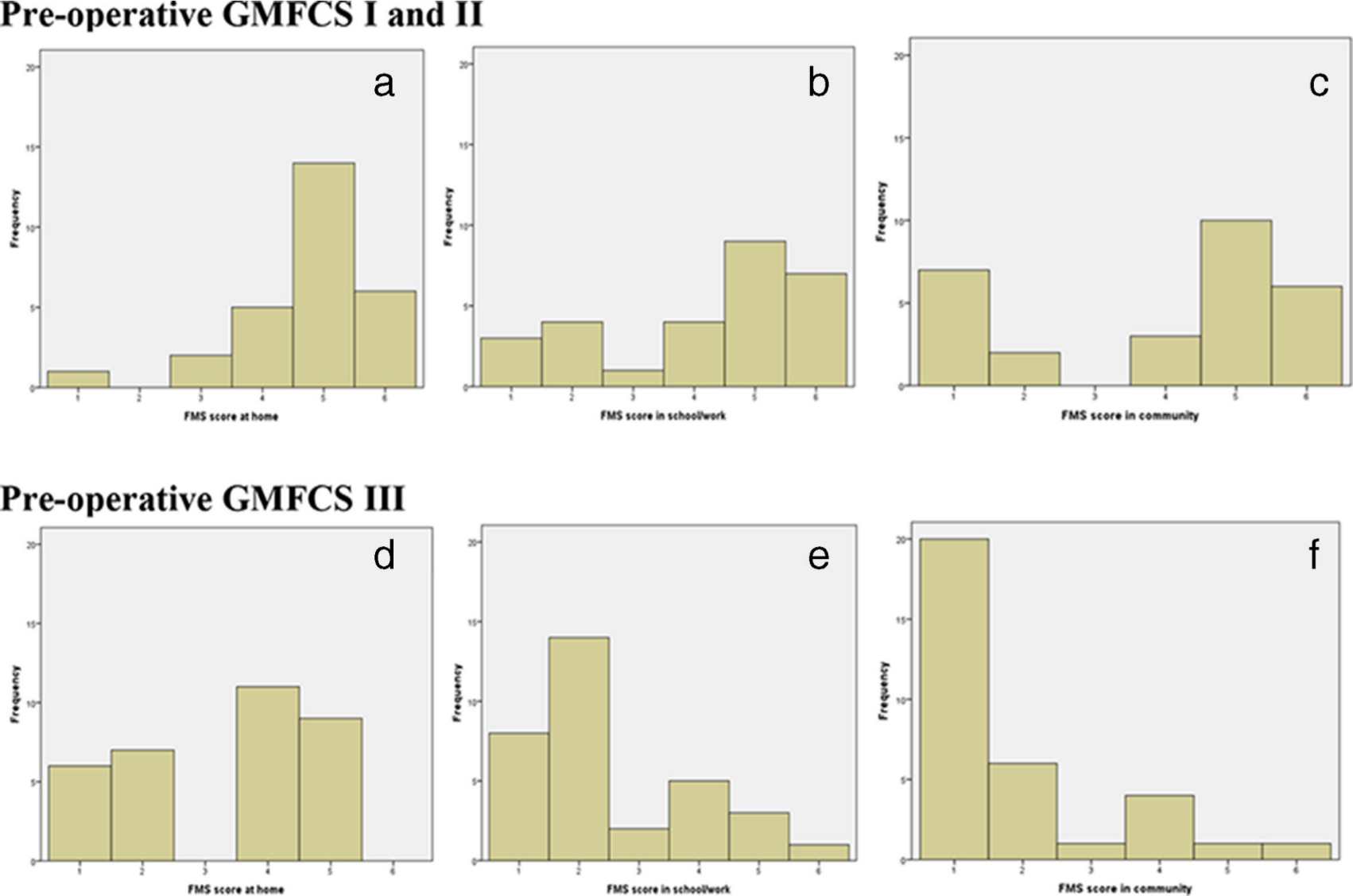
Histogram of Functional Mobility Scale (FMS) scores at long-term follow-up. Scores are shown for patients with respect to their preoperative Gross Motor Function Classification System (GMFCS) grade. Scores for children graded GMFCS I and II at home
Of patients graded GMFCS III preoperatively, at long-term follow-up the median FMS score at home, school/work and in the community was 4 (1 to 5), 2 (1 to 6) and 1 (1 to 6), respectively. Some patients graded GMFCS III preoperatively had acquired independent walking after SEMLS. At long-term follow-up, the proportion walking either independently or with an assistive device at home and school/work was 82% (27/33; Fig. 1d) and 76% (25/33; Fig. 1e), respectively. At long-term follow-up, 61% (20/33; Fig. 1f) of children graded GMFCS III preoperatively required a wheelchair over community distances.
The mean scores for the five QoL domains, both overall and according to preoperative GMFCS grade, are shown in Table 3. There were no statistically significant differences between the GMFCS grades for any domain.
Mean (sd) score for each domain of the Cerebral Palsy Quality of Life Teen (CP QOL Teen) for the entire cohort and comparison between groups based on preoperative Gross Motor Function Classification System (GMFCS) grade.

Significance tests were obtained by applying Student t-tests
There was a statistically significant association between home FMS score and ‘feelings about function’ (r = 0.55; 95% confidence interval (CI) 0.15 to 0.79; p = 0.01). When comparing the regressions of ‘feelings about function’ with home FMS in the two GMFCS groups it was found that there was no statistically significant difference between the groups (p = 0.89). There was no significant association between community FMS and ‘feelings about function’ (r = 0.22; 95% CI -0.24 to 0.59; p = 0.34). All other associations between any of the five QoL domains and home, school/work and community FMS scores were all non-significant (minimum p = 0.11).
Discussion
SEMLS is the standard treatment for correcting the musculoskeletal manifestations of CP. Most studies examining change following SEMLS focus on gait. Of the studies assessing function and QoL, the majority are limited by small study samples or insufficient length of follow-up. This study attempted to overcome these limitations by reporting the FMS in 61 children after a mean follow-up of eight years. The children included in this study had routine gait analysis preoperatively and at six, 12 and 24 months postoperatively. After 24 months the GPS had decreased by a mean of 3.3°, representing a two-fold improvement with respect to the minimally clinically important difference (1.6°). 32 Table 2 reports a mean of 3.0 bone and 5.7 soft tissue procedures per child as part of the SEMLS, comparable with a recent large multicentre study that reported 8.7 procedures per child as part of SEMLS. 13
Of patients graded GMFCS I and II preoperatively, at long-term follow-up, eight years later, over two-thirds were walking independently at home and over half were walking independently at school/work and in the community. Previous studies have reported that following a deterioration at three and six months postoperatively, the FMS returns to baseline by 12 months. 33 This study adds to previous short-term studies by reporting outcomes at long-term follow-up. Our findings suggest that some of these children may be losing functional mobility in the longer term. However, the overall functional mobility of patients at final follow-up in this study echoes a recent long-term follow-up of children with flexed-knee gait that maintained function into adulthood following SEMLS. 10
A previous short-term study reported that while 71% of children graded GMFCS III were using a wheelchair for community distances preoperatively, this had reduced to 58% at nine months and 50% at 12 months postoperatively. 33 Rodda et al 9 also reported improvements in functional mobility, but over a longer follow-up of five years. Although their study included a longer follow-up, it is limited by the inclusion of only ten patients. In our study, 61% (20/33) of patients graded GMFCS III preoperatively were using a wheelchair over community distances after a mean of eight years. Given that a large majority of patients graded GMFCS III require a wheelchair for community distances, the reported use at long-term follow-up in this study represents a success of surgery.
Gorton et al 12 compared the change in function and QoL in a cohort of 75 children with spastic CP that underwent SEMLS with a matched cohort that did not undergo surgery. Despite reporting significant improvements following SEMLS, the study only reported outcomes after 12-month follow-up. Similarly, Cuomo et al 22 reported that SEMLS improved QoL in a cohort of 57 ambulatory children with CP. However, the mean follow-up time was only 15.2 months. We hypothesized that better ‘feelings about function’ would be associated with better community FMS scores in those graded GMFCS I and II preoperatively, and better ‘feelings about function’ would be associated with better home FMS scores in those graded GMFCS III preoperatively. These pre-specified hypotheses were not confirmed. Although there was a significant association between ‘feelings about function’ and home FMS scores, it applied to patients irrespective of their GMFCS grade. A review by Livingston et al 34 reported that while functional status measures such as the GMFCS are reliable indicators of variations in physical function, they do not correlate consistently with psychosocial wellbeing.
Shelly et al 35 examined the strength of association between function and QoL domains using the CP QOL Child. In contrast to our study, all domains of QoL in their parent proxy-report were significantly associated with function levels, except access to services. For the child self-report, feelings about function, participation and physical health and pain and feelings about disability were significantly associated with functional level. It may be that function plays a less important role in QoL for older children and young adults in this cohort, or that we simply failed to detect significant associations because of the small sample that completed the QoL questionnaire.
This study has limitations to consider. First, there were no preoperative FMS or QoL data and there was no control group. This makes it difficult to draw conclusions about the effect SEMLS has on these parameters. However, this study adds to the literature by providing valuable information on the functional mobility of an unselected cohort of patients following SEMLS that has not previously been reported. Second, only 38% (23/61) of patients responded to the QoL survey. The lack of significant associations between FMS and QoL may be due to the small patient numbers. Third, the CP QOL Teen self-reported version 2 is not validated for the entire age range of the study participants. Minor adaptions were made in an attempt to make the questionnaire more applicable. This allowed valuable insight into patients across a wide range of ages that would otherwise not be possible.
In conclusion, this study reports that the majority of patients graded GMFCS I and II preoperatively are still ambulating independently at long-term follow-up. Similarly, the majority of patients graded GMFCS III preoperatively either walk independently or with an assistive device at home and school/work eight years after SEMLS. Despite the favourable functional mobility at long-term follow-up, there was little evidence in this small cohort to establish a link between functional status and quality of life.