
Abstract
Abstract
Purpose
Assessment of surgical treatments on gait in patients with bilateral cerebral palsy (CP) is often performed in short-term studies. The purpose of this study was to analyze the influence of single-event multilevel surgery (SEMLS) on long-term evolution of gait using gait deviation index (GDI) and walking speed.
Methods
In all, 28 patients with bilateral CP (Gross Motor Function Classification System I to III) with two clinical gait analyses (CGA) were included (mean age: 9.0 years (sd 2.9) at the first CGA, 19.6 years (sd 4.1) at the last, all of them at skeletal maturity). GDI, walking speed and their changes were calculated. Statistical analysis was performed to observe differences between baseline and follow-up CGA. Pearson's correlations were conducted to evaluate the associations between GDI and walking speed changes with: GDI at baseline and walking speed at baseline. GDI and walking speed evolution have been analyzed for two groups of patients: with and without SEMLS.
Results
Regardless of the treatment, GDI was significantly higher at follow-up CGA (baseline: 73.1 (sd 13.1) versus follow-up: 80.1 (sd 13.2); p = 0.014). Significant negative correlations were found between GDI change and GDI at baseline (r = -0.52; p = 0.004) and between walking speed change and walking speed at the baseline (r = -0.70; p < 0.001). Regarding the group of patients with or without SEMLS, only significant improvement of GDI was found for patients with SEMLS (at baseline: 69.0 (sd 12.1) versus follow-up: 77.8 (sd 11.2); p < 0.05).
Conclusion
Analysis at skeletal maturity showed a gait quality maintained for patients without SEMLS and an improvement for patients with SEMLS.
Level of evidence
Level III
Keywords
Introduction
Cerebral palsy (CP) is the most common motor neurone disability in children, exhibiting significant heterogeneity in all of its many aspects: aetiology, presentation, functional severity, movement and posture disorders, comorbidities, treatment options, individual health trajectories and outcomes.1,2 This heterogeneity makes monitoring patients over time very complex, particularly with regards to the long-term evolution of their walking.
Between 50% and 80% of patients with CP can walk. They present with a variety of gait deviations depending on the severity of their functional impairment, type of CP, predominant spasticity and possibly other factors. 3 Identifying gait deviations through childhood and into adulthood is essential to understanding and correcting them. Clinical gait analysis (CGA) provides objective information about the gait of patients with CP and is a useful tool for evaluating long-term gait evolution in clinical practice.4–6 Several scores summarizing patient gait quality have been proposed for children with CP, such as the gait deviation index (GDI) and the gait profile score (GPS). 7 GDI and GPS have been used quite extensively to evaluate the short-term (one year or less) and medium-term (less than five years) effects of treatments on CP gait.4,8–13 The heterogeneity of CP disorders means that treatments are varied (e.g. physiotherapy, orthoses, botulinum toxin injection, rhizotomy, single-level surgery (SLS) and single-event multilevel surgery (SEMLS)); they can sometimes be combined. In children with CP, the aim is to reduce the impact of motor impairments on any functional limitations, gait impairments or activity limitations that are due to a musculoskeletal pathology. 14 Among the different treatments, SEMLS is considered standard care for improving gait and function in patients with CP and more specifically patients with bilateral CP. 15 SEMLS is defined as a surgical procedure combining several techniques (muscle/tendon lengthening, releases or transfers and bone osteotomy) to correct deformities (in muscles and bones) in at least two levels of the lower limbs (i.e. hip, knee, ankle and foot) in one surgical period. 16 The positive effects of SEMLS have been shown to persist five years or more after surgery.11,16 However, the long-term evolution of the gait (more than five years of follow-up) in young adults with bilateral CP remains not well known. In 2018, Dreher et al 17 investigated the long-term efficacy of multilevel surgery in ambulatory children with bilateral spastic CP in a large cohort of 231 children (Gross Motor Function Classification System (GMFCS) I to III) evaluated at short term (1.1 years (sd 0.4)) and to long term (9.1 years (sd 0.3)) with CGA and clinical examination. This study was a multicentre cohort study. The authors observed that children maintained their improvement in GPS (11.4° (sd 3.1°)) after nine years of follow-up post-surgery. In addition, in 2016, Putz et al 18 analyzed the effects of SEMLS on young adults (mean age: 26.1 years (sd 8.3)) with bilateral CP two years after surgery. They compared three groups of patients: no surgery, SEMLS and other surgery. The authors found that GPS had significantly improved for all groups. In addition, they observed that the improvement in GPS for patients with SEMLS in childhood was less obvious than the two other groups. However, the long-term evolution of the gait (more than five years of follow-up) in young adults with bilateral CP, whether SEMLS or not, remains poorly described in the literature.
Thus, the present study's first objective was to evaluate, after end of growth, the long-term evolution (more than five years) of walking, using the GDI and the dimensionless walking speed of young adult patients with bilateral CP, independently of their GMFCS level or type of treatment. The second objective was to analyze the following relationships over the time in between: 1) GDI at baseline and change in GDI; and 2) walking speed at baseline and change in walking speed. The third objective was to gauge the long-term influence of SEMLS alone on the GDI and walking speed and then to observe if there are also some differences for these parameters in patients without SEMLS.
Patients and methods
This longitudinal retrospective study included part of the data available in our current CP cohort. Analyses of the gait function of young adults with ambulant CP were carried out using two CGA time points at least five years apart. The present study was approved by the local ethics committee (Comity Ethic Research (CER): 10-135). All participants gave their written informed consent.
Patients
Patients with CP who underwent a CGA between 1993 and 2013 were contacted for a new CGA if they met the following inclusion criteria: 1) diagnosed with bilateral spastic CP using clinical symptoms and medical imaging; 2) aged between five and 15 years old at the first CGA; 3) > 15 years old at the latter CGA (occurring between 2010 and 2019); 4) an interval between CGAs more than five years; 5) the ability to walk (with or without assistive devices); and 6) a GMFCS level from I to III (Fig. 1). General patient characteristics, such as age, sex, diagnosis and treatments (botulinum toxin injections, lower-limb orthotic management and lower-limb surgeries) were obtained from electronic medical records. From this selection, the patients were divided into two groups: patients with SEMLS and patients without SEMLS. In patients without SEMLS, there were patients without surgery and patients with only single-level surgery.
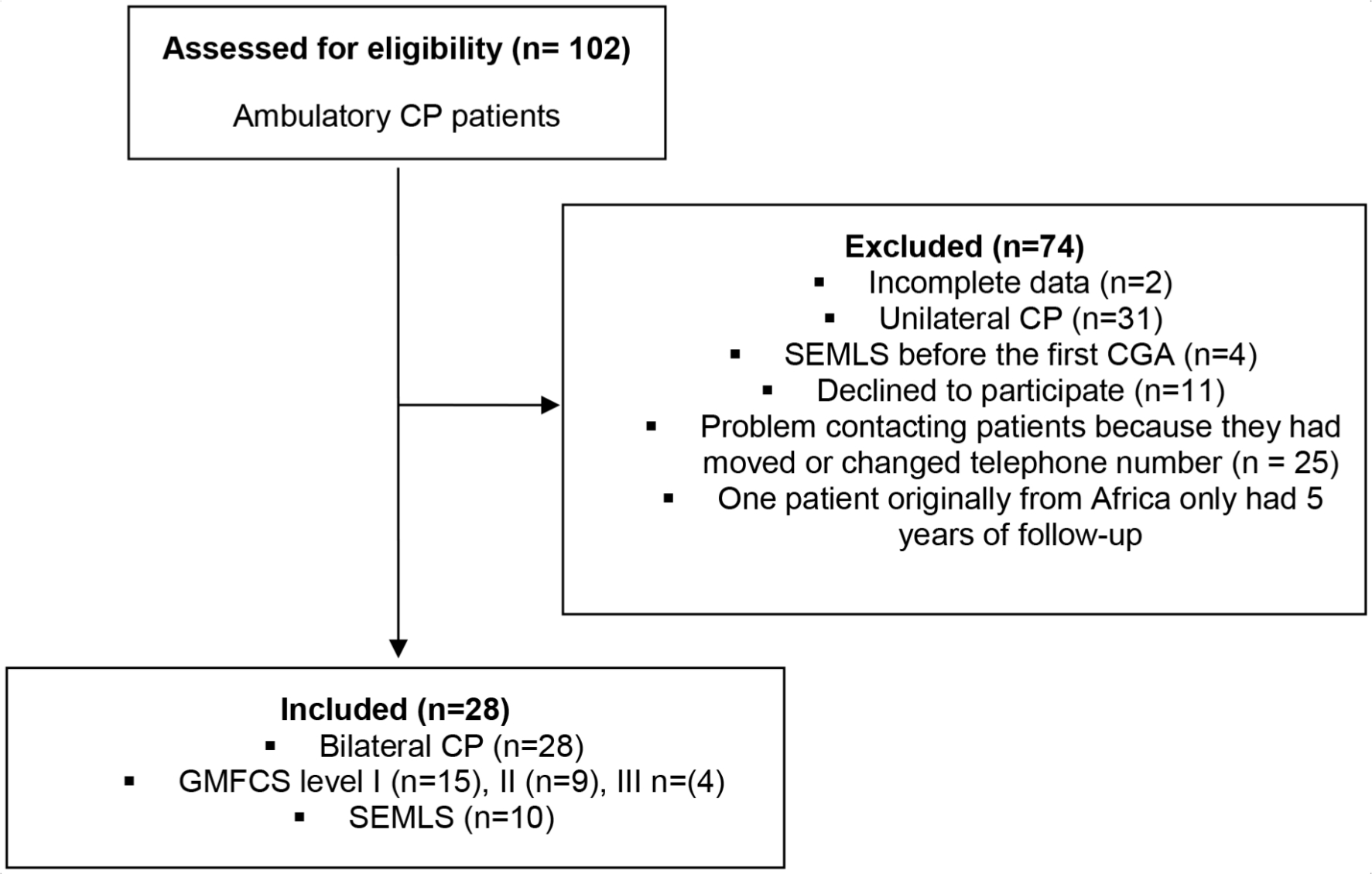
Flow chart of the inclusion and exclusion criteria leading to the selection of the study's 28 cerebral palsy (CP) patients (SEMLS, single-event multilevel surgery; CGA, clinical gait analysis; GMFCS, Gross Motor Function Classification System).
Objective gait assessment
From 1993 to 2008, CGA was performed using a six-camera motion analysis system (Vicon 460, Oxford, UK). From 2008 to 2014, CGA was performed using a 12-camera motion analysis system (Vicon Mx3+, Oxford, UK). Since 2015, CGA has been performed using a new 12-camera motion analysis system (Oqus 7+, Qualisys, Göteborg, Sweden). Each evaluation system used the Conventional Gait Model to place markers on the lower limbs and pelvis 19 Patients were asked to walk barefoot, at the speed of their choice, along a 12-metre walkway. At least five gait cycles of data were collected for each patient. The Visual 3D (C-Motion, Inc., Germantown, Maryland, USA), open-source Biomechanical ToolKit 20 and Matlab R2012b (MathWorks, Natick, Massachusetts, USA) software packages were used for kinematics, data analysis and GDI calculations, respectively.
Biomechanical outcomes
The GDI was the main outcome characterizing gait quality. For patients with bilateral CP, GDI assessments of the left and right limbs were averaged. GDI at the second CGA, minus baseline GDI, was calculated and called GDI change. Dimensionless walking speed 21 was analyzed at baseline and follow-up CGA, and the difference was called the dimensionless walking speed change. Three categories of GDI change were defined based on the clinically small but detectable change of 10.8 points on the GDI. 7 Values < -11 corresponded to a deterioration in gait, values between -11 and +11 corresponded to no detectable change and a value > +11 corresponded to an improved gait.
Clinical outcomes
For each patient whose baseline CGA occurred before 1997, a GMFCS level was estimated, by an orthopaedic paediatric surgeon (GD) from the assessment's videos of gait and functional movement.22,23 In addition, the GMFCS (Expanded and Revised) was used for the different age classes. 24
Statistical analysis
Because the data were normally distributed, we calculated means and sd to describe the data. For the study's first objective, a two-tailed, dependent Student's t-test for paired samples compared the whole cohort's GDIs and dimensionless walking speeds at the baseline and follow-up CGAs. For the second objective, Pearson's correlations were computed to assess relationships between GDI change and dimensionless walking speed change and GDI and dimensionless walking speed at baseline, respectively. Correlation coefficients of 0.0 to 0.30 were considered weak, 0.30 to 0.50 were fair, 0.50 to 0.70 were good and > 0.70 were high. 25
The third objective considered the two groups of patients: with SEMLS and without SEMLS. For patients who had undergone SEMLS and due to the number of patients, a dependent Student's t-test for paired samples compared GDIs and dimensionless walking speeds for these groups between first and last CGA. Because of the number of patients, the same analysis was also done for patients without SEMLS using non-parametric statistics with: median, interquartile range (IQR) and a Wilcoxon signed rank test. Statistical analyses were performed using STATA software, version 13.1 (StataCorp LP, College Station, Texas). Statistical significance was fixed at p < 0.05 (two-sided).
Results
Patient cohort characteristics at the baseline and follow-up CGAs
The present study included 28 patients with bilateral CP (19 male), with a mean interval of 10.5 years (sd 3.7) between CGAs. Mean ages at baseline and follow-up CGAs were 9.0 years (sd 2.9) and 19.6 years (sd 4.1), respectively. Mean body mass index at baseline and follow-up CGAS were 16.3 kg/m2 (sd 2.5) and 20.5 kg/m2 (sd 3.9), respectively. Table 1 summarizes each participating patient's characteristics and Table 2 summarizes the surgical procedures undergone during the follow-up period.
Individual characteristics. Patients in bold underwent a change in their Gross Motor Function Classification System (GMFCS) level. Age, gait deviation index (GDI) and its change, normalized walking speed and its change are presented
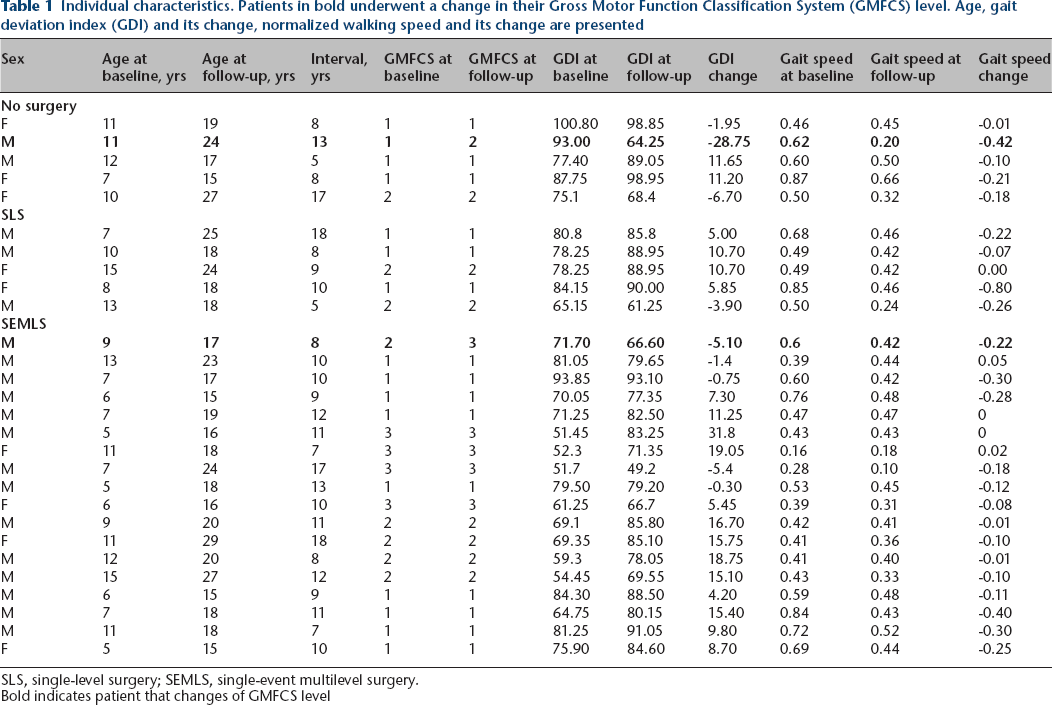
SLS, single-level surgery; SEMLS, single-event multilevel surgery.
Bold indicates patient that changes of GMFCS level
Individual treatments for each patient
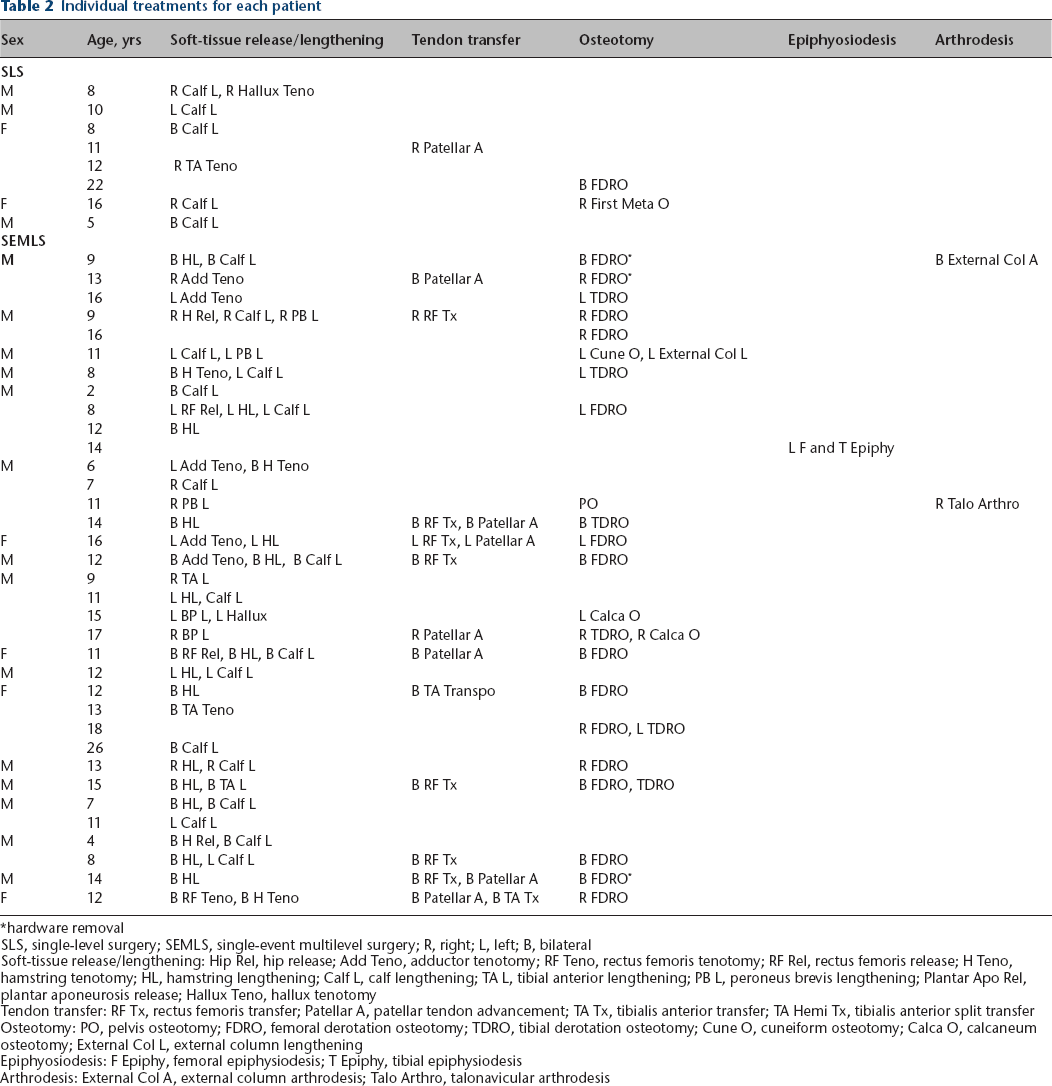
hardware removal
SLS, single-level surgery; SEMLS, single-event multilevel surgery; R, right; L, left; B, bilateral
Soft-tissue release/lengthening: Hip Rel, hip release; Add Teno, adductor tenotomy; RF Teno, rectus femoris tenotomy; RF Rel, rectus femoris release; H Teno, hamstring tenotomy; HL, hamstring lengthening; Calf L, calf lengthening; TA L, tibial anterior lengthening; PB L, peroneus brevis lengthening; Plantar Apo Rel, plantar aponeurosis release; Hallux Teno, hallux tenotomy
Tendon transfer: RF Tx, rectus femoris transfer; Patellar A, patellar tendon advancement; TA Tx, tibialis anterior transfer; TA Hemi Tx, tibialis anterior split transfer
Osteotomy: PO, pelvis osteotomy; FDRO, femoral derotation osteotomy; TDRO, tibial derotation osteotomy; Cune O, cuneiform osteotomy; Calca O, calcaneum osteotomy; External Col L, external column lengthening
Epiphyosiodesis: F Epiphy, femoral epiphysiodesis; T Epiphy, tibial epiphysiodesis
Arthrodesis: External Col A, external column arthrodesis; Talo Arthro, talonavicular arthrodesis
Cohort GDIs and walking speeds between the baseline and follow-up CGAs
Mean GDI was significantly higher at the follow-up CGA (baseline 73.1 points (sd 13.1) versus follow-up 80.1 points (sd 13.2); p ≤ 0.014) and the mean GDI change was 7.0 points (sd 13.8). Mean dimensionless walking speed was significantly lower at the follow-up CGA (baseline 0.53 (sd 0.18) versus follow-up 0.38 (sd 0.13); p < 0.05). An overview of each patient's GDI over time, showing their treatment group and GMFCS level, is presented in Figure 2.
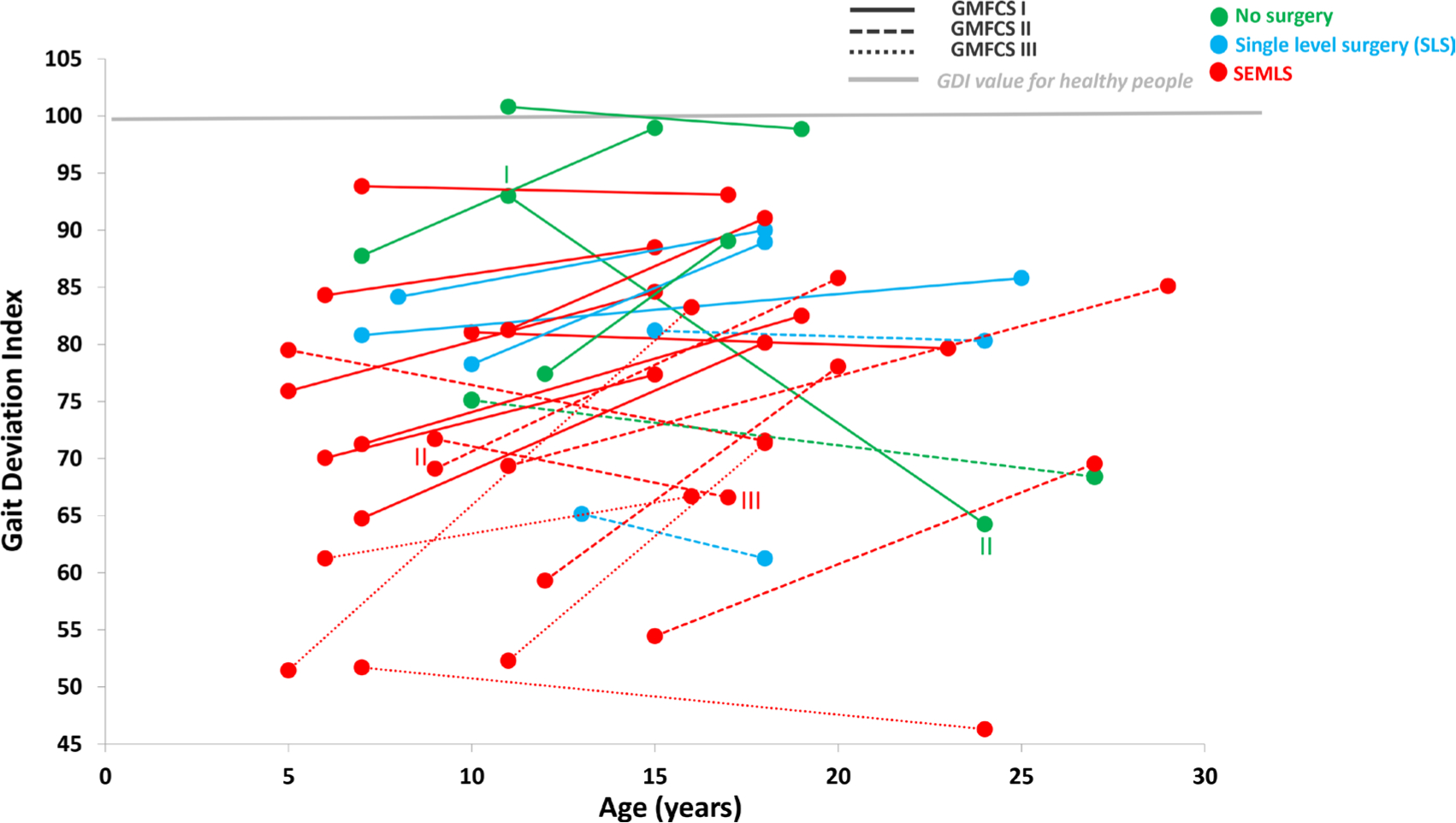
Gait deviation index (GDI) at the baseline clinical gait analysis (CGA) and follow-up CGA in function of the treatment and Gross Motor Function Classification System (GMFCS) level (SEMLS, single-event multilevel surgery).
Correlations for the whole cohort
Pearson correlation coefficients showed significant negative correlations between GDI change and GDI at baseline (r = -0.52; p = 0.004) and between dimensionless walking speed change and walking speed at baseline (r = -0.70; p < 0.001).
GDI and walking speed change for patients who underwent SEMLS
The characteristics of patients who underwent SEMLS are summarized in Tables 2 and 3. They showed a significant improvement in GDI (baseline 69.0 points (sd 12.1) versus follow-up 77.8 points (sd 11.2); p < 0.05). A significant decrease in dimensionless walking speed was observed over time (baseline 0.49 (sd 0.17) versus follow-up 0.38 (sd 0.11); p < 0.05). With a small but clinically detectable change of +/- 10.8 GDI points used as the measure of change, no patient presented with a degraded GDI, ten showed no evolution (55%) and eight presented an improved GDI (45%).
Characteristics of patients who underwent single-event multilevel surgery (SEMLS) (mean and sd) and patients without SEMLS (median and interquartile range (IQR)) at their baseline and follow-up clinical gait analysis (CGA), with proportions for sex, Gross Motor Function Classification System (GMFCS) level, age, body mass index (BMI), gait deviation index (GDI) and its change and normalized walking speed and its change are presented
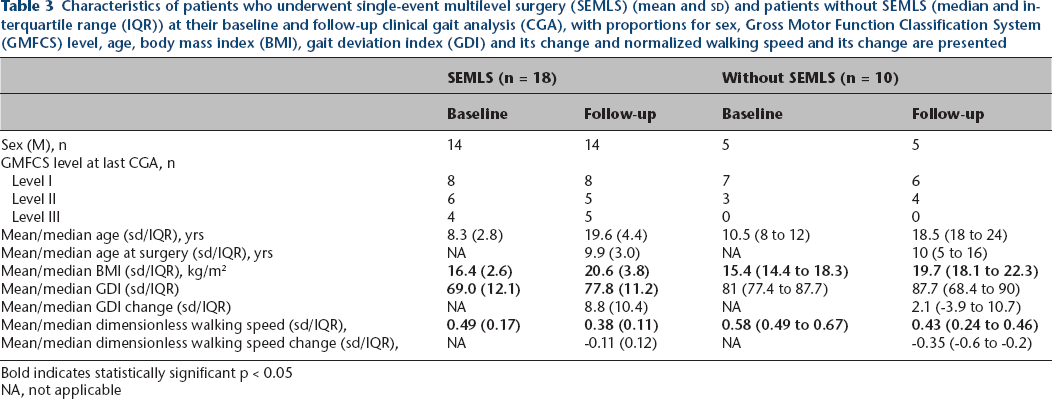
Bold indicates statistically significant p < 0.05
NA, not applicable
GDI and walking speed change for patients without SEMLS
The characteristics of patients without SEMLS are summarized in Tables 2 and 3. They showed no significant difference in GDI (baseline 81.0 points (IQR 77.4 to 87.7) versus follow-up 87.7 points (IQR 68.4 to 90); p = 0.995). A significant decrease in dimensionless walking speed was observed over time (baseline 0.58 m/s (IQR 0.49 to 0.67) versus follow-up 0.43 m/s (IQR 0.24 to 0.46); p < 0.05).
Discussion
The present study's objective was to evaluate the long-term evolution (mean 10.5 years) in the gait quality of patients with bilateral CP, especially those who had undergone SEMLS.
The first global observation was that improvements in the cohort's gait quality occurred during the important transition period between childhood and young adulthood, when the skeleton, muscles and body attain maturity. But the second significant observation was that patients with bilateral CP who had undergone SEMLS around the peak of their pubertal growth spurt (ten to 12 years old) showed improved gait quality over time, when patients without SEMLS seem to be maintained.
More severely affected children with bilateral CP generally tend to walk more slowly and undergo SEMLS at a younger age, which may reflect greater limitations in their gait quality (significant negative correlation between dimensionless walking speed change and dimensionless walking speed at the baseline CGA: r = −0.70; p < 0.001). Moreover, it has been shown in the literature that in the majority of patients with bilateral spastic CP gait deteriorates with time 26 because of increased deformities. Decreases in walking speed observed in patients with CP can be attributed to several factors, such as growth, changes in body mass, reduced strength, reduced range of movement, changes in gait pattern (evolution from an equinus to a crouch gait pattern), the progressive development of contracture pain, fatigue, reduced balance or social environments.4,26,27 Furthermore, in a healthy population, normalized or dimensionless walking speed decreases as children grow up. 28 Therefore, the cohort's decrease in dimensionless walking speed is not necessarily negative when the gait score is maintained or improves over time.
Ten patients in the cohort did not undergo SEMLS during the follow-up period. In this group, no statistical differences were observed for their median GDIs (IQR): 81.0 (77.4 to 87.7) at the baseline CGA and 87.7 (68.4 to 90) at follow-up. These patients thus had better initial levels of functionality and mobility (GMFCS level I and high GDI scores) at baseline than patients who underwent SEMLS. Their gait quality remained steady but did not improve during the period of transition to young adulthood. This observation emphasizes the significance of the levels of function and mobility at baseline. Indeed, patients with a high level of function at baseline will maintain their gait quality over time without the need for SEMLS, contrary to patients with lower levels of function and mobility at baseline. A significant negative correlation (r = -0.52, p < 0.001) was found between the GDI change and the GDI at baseline, thus confirming that patients with a low baseline GDI improved more than patients with a high one over a follow-up of about ten years. This result also showed that patients with a good initial walking quality have a smaller margin for improvement than those with a poor initial level of gait quality.
However, Table 1 and Figure 2 show that two patients’ GMFCS levels worsened during the long follow-up period. One patient went from GMFCS level I to II between the two CGAs, with substantial deteriorations in GDI and walking speed (GDI change of -28.7 and dimensionless walking speed change of -0.41 m/s). At the follow-up CGA, this patient walked with crutches, whereas at his baseline CGA, he walked without assistive devices. This specific case is particularly interesting because over 13 years the boy's results reflected the natural gait evolution for patients with bilateral CP, as described by Bell et al. 29 A second patient went from GMFCS level II to III, with a decrease in dimensionless walking speed of -0.22 m/s and a decrease in GDI score of -5.1 over eight years of evolution. Notably, four years after his baseline CGA, the patient returned to the laboratory for a new CGA because a significant worsening appeared in his mobility and function. The CGA revealed a GDI change of -20.8 points, with a significant crouch gait and the inability to walk without a walking frame. The patient underwent SEMLS just after this CGA. The evolution between the second CGA, just before SEMLS, and the follow-up CGA (four years later), showed a significant 15.7 point improvement in the GDI, although the patient never recovered the GDI level calculated at his baseline CGA (overall GDI change of -5.1). This specific case highlights the potential positive impacts of SEMLS in improving gait quality: even though the patient still had to use his walker for longer distances, he did not have to for shorter distances.
Regarding the SEMLS group, most types of procedures used (Table 2) were derotational osteotomies (tibia and femur) with muscles/tendon lengthening (semi tendinosus, semi membranosus, gastrocnemius, Achilles tendon), transfer (rectus femoris) and patella advancement. These procedures are used to manage such gait impairments such as crouch gait and stiff-knee gait in order to re-establish lever arm function and then reinforce muscle activity during the gait. 30 Another positive point concerns the impact of these procedures on aesthetic aspects and patients’ feelings about their own body.31,32 Several longitudinal post-SEMLS studies have shown good results with muscular procedures such as muscular transfer, recession or lengthening as well as such bone procedures as femoral derotation osteotomy in children with spastic bilateral CP. 15 These studies showed that muscular procedures had good results in counteracting natural progressions in short-term joint limitations;10,33,34 ten years after surgery, however, some patients had a permanently poor response (i.e. gait score degradation) with, for example, a recurrence of flexed knee gait.35,36 Bone procedures also showed good results, provided overall correction and maintained those corrections nine years after surgery. 37 It is thus interesting to observe that different types of procedure do not have the same impacts on long-term gait evolution. 38 In their study on long-term evolution (10.9 years) in adults (mean age at baseline: 24.8 (sd 7.6)), Putz et al 39 showed that patients with bilateral CP who underwent SEMLS had an improved gait score (GPS) over time. Thus, SEMLS is an important treatment for managing CP impairments between childhood and young adulthood, but also during the adult period. These findings agreed with those of Švehlík et al, 11 showing the benefits of SEMLS after ten years of follow-up, with an age at surgery of around ten to 12 years being an important factor influencing long-term postoperative results.
The present study's main limitations were its small sample size and the heterogeneity of the patients due to the long follow-up time (mean of ten years between the two CGAs). Longitudinal assessments of patients with CP from childhood to adulthood revealed great variability in gait maturation, levels of impairment, treatments and combinations of treatments, clinical approaches to addressing gait deviations depending on the healthcare professionals involved, the influence of growth and participation levels. 40 Indeed, only a few parameters were considered, whereas the indication for treatments in CP is multifactorial. In the context of the International Classification of Functioning, Disability and Health (ICF), gait and clinical evaluation are only one part (body function and structure) of a holistic approach. 41 The treatment choice also depends on how participation, function, environmental factors and personal factors fit in with the ICF parameters. However, many co-factors could not be taken into account in this observational longitudinal study because the number of patients was too small for an appropriate adjustment to the statistical analysis. A similar, future study based on a larger cohort could be a proper way to integrate several ICF co-factors.
In conclusion, this study highlighted two important points in the transition from childhood to young adult: 1) during this ten-year follow-up period, the gait quality of patients with SEMLS improved whereas patients without SEMLS maintained their gait quality; and 2) SEMLS had a beneficial impact on gait quality, particularly for patients whose gait quality was poor at baseline. Another revelation from this study is that some patients who do not undergo surgery may experience a significant decrease in their gait score over time, which affects their level of function and capacity to perform activities in their daily life. These specific cases reflect the importance of actively trying to find better strategies for maintaining and improving the gait quality of CP patients over time. This strategy would require active collaboration by parents, patients and clinical teams to optimize gait quality rather than normalize it. Further long-term longitudinal studies based on larger cohorts would be needed to develop a better understanding of the implications of different treatment combinations on different CP gait quality profiles, and these should also consider environmental factors such as personal situation, social wellbeing and rehabilitation procedures. 15
Footnotes
Acknowledgements
This work was supported by the Center of Clinical Research of Geneva University Hospitals.
GdC: Fundraising, Data interpretation, Critical revision of the article for important intellectual content.
PL: Critical revision of the article for important intellectual content.
SA: Fundraising, Protocol development, Data analysis and interpretation, Critical revision of the article for important intellectual content.