
Abstract
Purpose
To describe self-reported life satisfaction and motor function of young adults with cerebral palsy (CP).
Methods
A total of 57 young adults with spastic CP classified as levels I (seven), II (25), III (16), IV (nine) by the Gross Motor Function Classification System, followed from childhood by our CP clinic, returned at a mean age of 27 years two months (SD 3 years 4 months). Self-reported life satisfaction and mobility status were measured by the Pediatric Outcomes Data Collection Instrument (PODCI), Patient-Reported Outcomes Measurement Information System (PROMIS), Functional Mobility Scale (FMS) and a project questionnaire. Surgical history and childhood mobility were confirmed from medical records.
Results
The Functional Mobility Scale demonstrated limited but stable mobility function from childhood to adulthood. The PROMIS and PODCI revealed limited motor function compared with a non-disabled normative reference (p < 0.05). Descriptive results showed high dependence on transportation, housing and income; although PROMIS subscales revealed satisfaction with social activities. Self-recall of childhood mobility function using the FMS correlated highly (r = 0.8; p < 0.0001) with historical records.
Conclusion
Although functional mobility is limited and community independence is not fully achieved in young adults with CP, these participants maintained childhood levels of mobility function into young adulthood, were satisfied with social roles and had minimal reports of pain.
Level of Evidence Level III
Introduction
Cerebral palsy (CP) is a group of movement and posture disorders resulting from nonprogressive disturbances to the foetal or neonatal brain. 1 The overall prevalence of CP worldwide is 2.11 per 1000 live births 2 and it affects approximately 10 000 babies born in the United States each year. Much of the specialized paediatric care for youth with CP aims to minimize the impact of musculoskeletal system impairments on mobility function. Many studies report on the long-term outcome of gait following single-event multilevel surgery during childhood and adulthood;3–9 however, the long-term effects on the quality of life in adults with CP who have received such specialized care are less clear. 9 Today, more than 90% of children with CP live to adulthood, most with normal life expectancy. 10 Recent literature reports declining quality of life in adulthood, with losses in mobility function,9,11–13 low levels of participation in social relationships14,15 and a low percentage of independent living.11,14,15 Paediatric providers urgently need information about how the care provided during childhood impacts adult outcomes for individuals with CP.
Specific approaches to clinical management during childhood and adolescence have the potential to minimize physical and social disparities in adulthood, but these links need clarification. Expert opinion and evidence of short-term gains currently guides best practices in paediatric orthopaedic care of children with CP, but there is little evidence describing the association between childhood treatment of individuals with CP and adult function and life satisfaction. 9 Examining the outcomes in adulthood of a cohort with known childhood treatments is the first step towards understanding the impact of clinical management, social support and comorbid conditions on the physical and social outcomes for adults with CP. Our paediatric orthopaedic practice had the opportunity to examine such a cohort. We undertook this study with the goal of describing patient-reported life satisfaction and mobility function in a sample of young adults with CP who received orthopaedic care in childhood from a single specialty programme. The broad philosophy of care in this programme was to closely monitor gait and optimize walking function via orthopaedic surgeries guided by instrumented gait analysis. A secondary purpose of the study was to examine the accuracy of adult recall of surgical history and mobility function during childhood.
Patients and methods
This project was part of an Institutional Review Board-approved research study that sought to describe long-term outcomes of surgical treatment for flexed-knee gait during childhood. It was not externally funded. Retrospective chart review identified patients with spastic CP treated for flexed-knee gait between 1991 and 2003 when they were between the ages of five and 20 years. Inclusion criteria consist of diagnosis of spastic CP, currently over the age of 21 years, had a complete gait analysis at least 6.5 years prior and had flexed-knee gait at the time of the previous gait analysis. Flexed-knee gait was defined as greater than 17° of knee flexion at initial contact; 17° was chosen because it corresponds to one sd above the mean knee flexion at initial contact for a typically developing 14-year-old child, the average age of all subjects at the time of initial gait analysis. 7 Participants were excluded if they did not meet inclusion criteria, or if we were unable to make contact with participants via mail or phone. Mobility function was reported according to the Gross Motor Functional Classification System (GMFCS)-Expanded and Revised 16 using the 12- to 18-year age band as levels. The self-report questionnaires were completed either independently or with the assistance of a parent or companion.
We administered the Pediatric Outcomes Data Collection Instrument (PODCI) adolescent form, 17 which is widely used both at our institution and elsewhere for children and adolescents with disabilities. 18 The PODCI adolescent form is intended for youth ages 11 to 18 years and is not validated for young adults. 19 The PODCI focuses on activities of daily living, mobility, pain, and participation and satisfaction, making it an appropriate tool to describe general physical and mental health-related function in a sample of young adults with CP.
The Patient-Reported Outcomes Measurement Information System (PROMIS) is a rigorously constructed, generalizable and clinically relevant set of patient-reported outcome measures developed at the National Institutes of Health. 20 Multiple PROMIS domains attempt to quantify the impact of disease and health problems on areas important to patients such as physical, mental and social well-being. 21 Many of the PROMIS domains are valid for use with a variety of health conditions, although validity of the PROMIS in adolescents and adults with CP has not been established. 22 Because many of the domains are computer-adaptive, the PROMIS presents a limited set of questions, making it more time-efficient than traditional questionnaires. The developers normalized the scoring system to a non-disabled adult population providing a stable reference for making comparisons to a variety of health conditions. 23 We administered select domains of the PROMIS including physical function, fatigue, pain interference, depression, satisfaction with participation in discretionary social activities and satisfaction with participation in social roles. We compared PODCI and PROMIS data from our sample with normalized scores for these measures.
All participants, with or without the assistance of a parent or companion, also answered a project-specific set of questions. Participants were asked about current and previous mobility status using the Functional Mobility Scale (FMS). 24 The FMS is a six-point ordinal scale describing the level of support needed for walking distances of 5 m, 50 m and 500 m. Questions are typically framed as “how do you walk at home (5 m)?, at school or office (50 m)?, and when you go to a shopping mall (500 m)?” Questions about prior mobility status required participant recall of walking performance during elementary, middle and high school timeframes.
We asked participants about current physical function compared with function in childhood and adolescence and about their satisfaction with childhood healthcare experiences, including physical therapy, orthopaedic surgery, wheelchair use and walking. Participants reported current work status, transportation status and living arrangements. We also asked participants to recall childhood surgical history.
All of the participants received paediatric care at our institution, allowing us to obtain a detailed surgical history. Additionally, all participants were followed at multiple visits to the gait analysis lab, which allowed us to report the 5-m FMS score according to video recordings obtained during elementary, middle and/or high school years. We used the gait video 5-m FMS score for comparison to evaluate the accuracy of participants’ recall of childhood mobility status.
Statistical analysis
To quantify young adult outcomes in physical function and life satisfaction, we utilized the PODCI and PROMIS normalized scores. We considered mean domain scores from our sample that were greater than 1 sd (± 10) from the normalized mean as clinically different from the non-disabled population.
We examined changes in mobility performance over time, as recalled and reported by participants, by comparing the self-reported FMS scores over time using a chi-squared test for preliminary analysis, ordinal-scale Friedman test, the log transformation of data and repeated measures analysis of variance.
To examine accuracy of participants’ recall of mobility status in childhood, we compared the gait video-scored 5-m FMS with the participants’ recalled 5-m FMS scores from childhood. We used Spearman's rank correlation to examine association, and the chi-squared test for concordance.
To examine accuracy of self-reported surgical history, we compared participant recall with the surgical records. We applied independent sample t-tests, and a simple linear relationship analysis.
Results
Retrospective chart review identified 200 patients with spastic CP treated for flexed-knee gait when they were between the ages of five and 20 years. Attempts were made to contact all 200 young adults via phone and mail to available contact information. Contact was made with 65 young adults and 57 agreed to participate in the research. Participants came to the gait lab for instrumented analysis and completion of a series of standard and custom patient-reported outcome measures. Participants were classified based on their current report of mobility function with the GMFCS-Expanded and Revised as levels I (seven), II (25), III (16) and IV (nine). At the time of this research study, the mean age of the participants was 27 years two months (sd 3 years 4 months). We did not evaluate cognitive status. All participants demonstrated verbal ability but not all could read at fourth-grade level. Participants completed the self-report questionnaires either independently or with the assistance of a parent or companion.
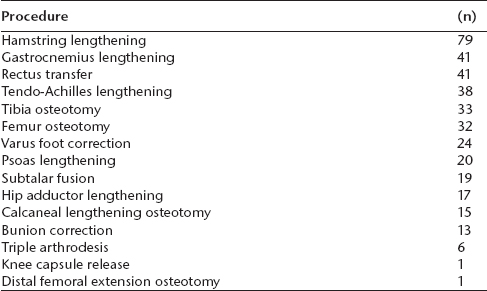
All 57 participants had had previous orthopaedic surgical intervention. The average participant had three past surgical events with an average of two surgical procedures per event. Table 1 describes specific surgical procedures.
Surgical history
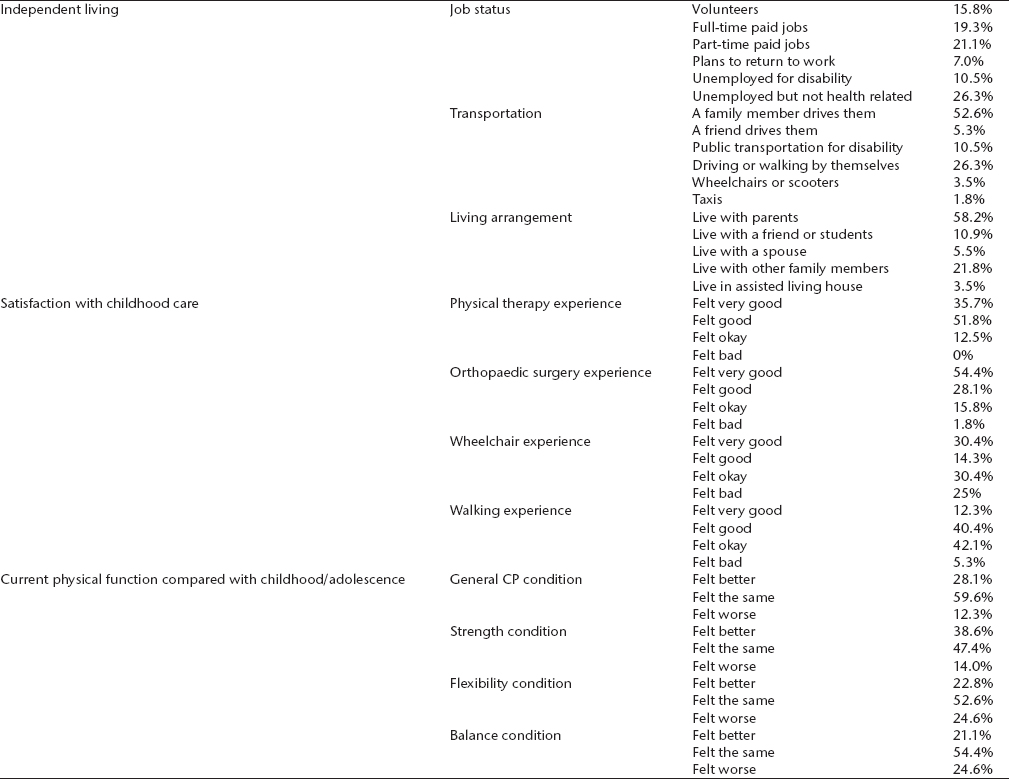
The information reported in our project-specific questionnaire revealed high levels of dependence for transportation and housing, mostly positive recollections of childhood healthcare experiences, and perceived stability in health condition. A majority of participants had a job (56.3%) or were looking for work (7%) and most were dependent for transportation and housing. Only 26% could drive a car and none of the participants lived alone, although 16% lived with a spouse or friend (Table 2).
Descriptive questionnaire
CP, cerebral palsy
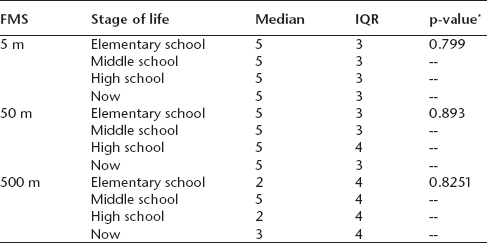
Self-reported changes in mobility performance over time as measured by participant recall of FMS (5 m, 50 m and 500 m) during elementary, middle and high school and current FMS report show no significant difference over time (5 m, p = 0.80; 50 m, p = 0.89; 500 m, p = 0.83) (Table 3).
Self-reported Functional Mobility Scale (FMS) over time (recall and present day)
p, comparison of change over time
IQR, interquartile range
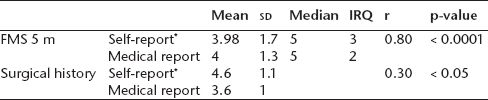
Spearman's rank correlation coefficient demonstrates a statistically significant strong correlation (r = 0.80; p < 0.0001) between the participant-recalled 5-m FMS scores compared with gait video-scored 5-m FMS scores (Table 4).
Functional Mobility Scale (FMS) self-report and surgical history versus medical records
Patient self-reporting about their recall of childhood mobility status
IQR, interquartile range; r, correlation coefficient
Using the PODCI, we measured subdomains of upper extremity function, transfers and basic mobility, sports participation, pain, happiness and global function. We considered differences of > 1 sd (10 points) from the normalized mean score as clinically different from an adolescent with no physical disability. For this sample of young adults with CP, the upper extremity, transfers and mobility and sports subdomain scores of the PODCI were significantly different from the normative reference scores. Scores from the pain and happiness subdomains were not significantly different from the normative reference scores. In contrast, only the physical function subscale scores from the PROMIS were significantly different from normative reference scores (Table 5).
Comparison between Pediatric Outcomes Data Collection Instrument (PODCI) and Patient Reported Outcomes Measurement Information System (PROMIS) results and non-disabled population
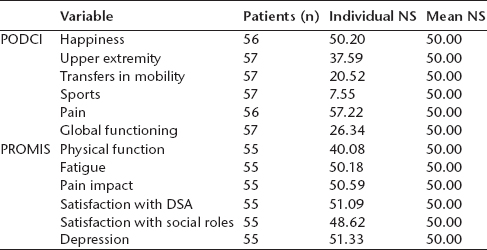
NS, normative score; DSA, discretionary social activities
Discussion
The primary goal of this study was to describe the quality of life and perceived change in motor function of a group of young adults with CP who received paediatric specialty care at a single institution with a unified approach to orthopaedic care and treatment of gait disorders. Results from this group demonstrate the perception of stable mobility function with minimal changes over time from school age to young adulthood. In this group, perceived mobility performance did not decline, but was stable at household and community distances according to self-reported FMS scores. Most participants also reported feeling approximately the same with regard to balance and strength compared with adolescence, with 39% feeling better, 47% feeling the same and 14% feeling worse about their strength and 21% feeling better, 54% feeling the same and 25% feeling worse about their balance. These results are inconsistent with literature reports of declining mobility function in adults with CP.11,25,26 Other authors suggest that aging with long-standing musculoskeletal impairments such as muscle weakness, spasticity and contractures, negatively impacts mobility in adulthood. Similar to our study though, these authors also rely primarily on patient-reported outcomes with little objective data from long-term outcome studies. Large, multi-site, controlled studies of adult outcomes are needed to better define changes in mobility function from childhood to adulthood in individuals with CP and to examine associations between adult outcomes and childhood care.
Physical function and mobility were clearly limited in our study sample, consistent with the GMFCS levels included in this group. The PODCI findings revealed scores in sports participation, transfers and mobility and upper extremity function that were > 1 sd below normal referenced scores. Similarly, the PROMIS physical function scores from our group were 1 sd below normalized PROMIS mean scores. Despite reporting limited physical function, participants in this study were satisfied with both their social roles and discretionary social activities, a finding consistent with self-reports of happiness on the PODCI. Our positive social engagement and participation findings are consistent with literature showing that a higher sense of self-efficacy correlates to higher physical and mental quality of life for individuals with disabilities. 26 Although neither the PODCI nor the PROMIS is validated for the age group (PODCI) or the health condition (PROMIS) studied here, and results need to be interpreted cautiously, we feel that these trusted instruments provide valuable insights not otherwise available in studies of adults with CP.
A lack of social service resources for adults with disabilities is associated with decreased quality of life. 27 Mesterman et al (2010) 27 report a high incidence of dependency for showering, cleaning, cooking, shopping and mobility outside of the home, which correlated to a lower quality of life for adults with CP. Although the sample of adults in our study had greater independence in mobility and most were independent in ambulation, most of our group was dependent for transportation (68%) and housing (83%) (Table 1). In our sample, only 19% had full-time paid employment and 21% were employed part-time compared with 80% to 90% of the non-disabled population who had competitive employment. 28 In the study by Mesterman et al, 27 23% of the adults with CP were in competitive employment and 15% were in sheltered workplaces. Rutkowski and Riehle 28 report that 29% of adults with CP worked in a competitive setting, and adults with hemiplegic distribution (46%) fared better in employment than those with quadriplegia (12%).
The perceived stability in walking and neuromotor function in our study group contrasts with literature reports of functional decline for individuals with CP as they reach adulthood.11,25,26,28 One possible explanation is that the mean age in our sample was 27 years, which may be too young to experience the negative consequences of aging reported in other studies of adults with CP. Perhaps the widely reported declines in motor function more typically occur in the fourth and fifth decade of life versus the third decade. An additional difference between reports of adulthood decline11,25,26 and this study is that all of the participants in the current study received orthopaedic treatments guided by modern gait analysis throughout childhood and adolescence. Most of our participants underwent multilevel surgeries. This high standard of care is not typical for the previously reported population of adults with CP. The specialized orthopaedic care received in childhood also may explain the degree of stability in mobility function experienced by the participants in our study.29,30
Large-scale, long-term outcome studies of adults with CP will require accurate historical data. In the absence of broad and consistent health registry data, such studies will need to rely on patient recall through self-reporting. This study examined the accuracy of such reporting for adults with CP. We examined the ability of young adults, who received childhood care at our institution, to recall their surgical history as well as their mobility function at different stages of childhood: elementary school, middle school and high school. Comparing our gait video records of participants during these childhood stages with the self-report, we found high levels of accuracy in classifying mobility function using the FMS scale. Participant recall of surgical history was less accurate. The young adults in our study frequently under-reported surgical procedures, resulting in low agreement with medical record reports. It appears as though the complex multilevel nature of the orthopaedic surgery episodes that were performed on participants demanded a level of detail that is not realistic to accurately recall. Additionally, participant recall of the timing and number of surgical episodes was not highly consistent with medical records. Reliance on participant recall of surgical history does not appear to be a reliable method for documenting orthopaedic treatments during childhood.
Limitations of this study include the lack of validity of the PODCI and PROMIS questionnaires for this study sample of adults with CP, which limits the generalizability of our results to a broader population. The PODCI was developed for use in children and adolescents with disabilities, but is not validated for adults. The PROMIS questionnaires used in this study were developed for adult populations and validated in health conditions that do not include adults with CP. Another limitation is the relatively high percentage of adults who met inclusion criteria but did not return for the study. Of the 200 young adults who were candidates, only 57 returned to participate. A large portion did not participate due to inaccurate contact information (68%). Of those identified, 13% chose not to return, and this could reflect limited transportation resources or mobility. Alternatively, it could represent adults who could not participate due to full-time employment obligations. We suspect that our final sample was skewed towards higher levels of motor function. The questionnaire data also noted that most of the participants had positive memories of their childhood orthopaedic and physical therapy care, which could be a reflection of a biased sample. Lastly, our study sample consisted of young adults who had been followed at a specialized children's hospital and treated with orthopaedic surgery guided by gait analysis. This level of specialized care is not representative of a broader population of adults with CP and may explain why our group maintained childhood levels of ambulation while the literature reports declining ambulation status of adults with CP.
Although functional mobility is limited and community independence is not fully achieved in young adults with CP, this study sample maintained childhood levels of functional mobility into young adulthood following specialty care by experienced physicians.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Ethical approval: Institutional IRB approval was obtained for this study.