
Abstract
Abstract
Background
Varus osteotomy of the proximal femur (VOPF) is one treatment option to prevent hip dislocation in children with cerebral palsy (CP). It is questioned whether the osteotomy should be performed in the displaced hip only, or if it should be performed bilaterally to prevent later displacement of the contralateral hip. CPUP is a register and healthcare programme for children with CP that was initiated in 1994 in southern Sweden. In the programme, range-of-motion and radiographic examination of the hips is performed regularly. These data have been analysed preoperatively and for 5 years postoperatively in children treated with unilateral VOPF.
Methods
Children with CP living in the counties of Skåne and Blekinge in the south of Sweden, who were treated with unilateral VOPF at least 5 years ago, were included in the study. The degree of hip displacement and the range of hip motion were analysed preoperatively and after 5 years. Repeat hip operations after the index operation were recorded.
Results
Twenty-four children fulfilled the inclusion criteria. Mean age at index operation was 7.6 (2.8–13.2) years. No child died within 5 years postoperatively, and no child was lost from follow-up. At follow-up after 5 years, 2 of the 24 children had been operated on with VOPF in the contralateral hip. The range of motion in both hips decreased, but the difference between the index hip and the contralateral hip did not change significantly.
Conclusion
Children with CP and unilateral hip displacement have a low risk of later contralateral displacement after being operated on with unilateral VOPF. This supports healthcare programmes that advocate unilateral VOPF in children with unilateral hip displacement.
Introduction
Children with cerebral palsy have an increased risk of hip dislocation, due to muscle imbalance and spasticity. The problem can, in most cases, be prevented by following a surveillance programme and by counteracting the effects of the muscle imbalance. Nonoperative treatments consist of proper positioning with the hips in abduction and extension. Operative treatments consist of adductor-psoas release, varus osteotomy of the proximal femur (VOPF) and pelvic osteotomy.
Several studies have shown that performing unilateral adductor-psoas release results in a high risk of displacement of the contralateral hip. Regarding VOPF, some studies have shown a low risk of contralateral displacement [1–3], whereas others have shown a higher risk [4–6], and the recommendations concerning bilateral or unilateral VOPF in children with unilateral displacement differ in the literature.
In 1994, a CP register and a healthcare programme, known as CPUP, were initiated for children with CP in southern Sweden (1.4 million inhabitants) [7, 8]. In the programme, all children are regularly examined clinically and radiographically. The examinations include measurement of hip range of motion. All children with hip displacement operated on with adductor-psoas tenotomy are operated bilaterally. All children operated on with VOPF have been operated on the displaced hip only.
In the present study, we analysed the development of both hips 5 years after being operated on with unilateral VOPF.
Materials and methods
The CPUP register includes all children with CP who were born after 1 January 1990 and are living in the counties of Skåne and Blekinge in southern Sweden (with a total population of about 1.4 million). The number of children with CP in the area corresponds to a prevalence of 2.4–2.6 per 1,000 living births [9, 10].
Our definition of cerebral palsy was that given by Mutch et al. [11]. The diagnosis is made by the child's neuropaediatrician. The CP subtype is classified according to the Surveillance of Cerebral Palsy in Europe network (SCPE) [12]. The gross motor function is classified according to the Gross Motor Function Classification System (GMFCS) [13]. In children measured before the publication of the GMFCS system in 1997, the child's GMFCS level reported from 1997 was used.
In the programme, a continuous standardized follow-up of gross and fine motor function, clinical findings, and treatment is done. The local physiotherapists examine the child and fill in a recording form twice a year until the age of 6 years, and then once a year. The recording form includes measurements of ranges of motion (ROM) in all major joints with a goniometer. The measurements are performed in standardized positions that are described in a manual accompanying the recording form.
The hips are examined on anteroposterior radiographs in the supine position at diagnosis, then at least once a year in children with GMFCS III-V until 8 years of age, and after that on an individual basis. Children in GMFCS II are examined at 2 and 6 years of age, and then on an individual basis. Children in GMFCS I are not examined radiographically, unless the clinical examination reveals decreased ROM. The degree of displacement is measured using the migration percentage (MP) [14] (Fig. 1).
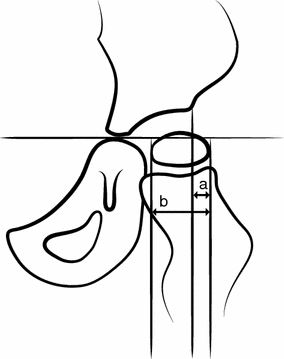
Measurement of the migration percentage (MP). MP = a/b × 100
In the present study, we included all of the children in the register who were treated with unilateral VOPF and had been followed up for at least 5 years; i.e. children treated in the period 1994–2005. The aim was to have a neck-shaft angle of 110–115° after the osteotomy. Increased femoral anteversion was corrected with derotation of the osteotomy. The numbers of hip operations after the index operation, the MP preoperatively and at 5 years postoperatively, and the ranges of hip abduction, internal and external rotation were recorded in both hips.
Paired t tests were used in the statistical analysis of the average change in the difference in ROM between the index and contralateral hip from the measurements before the index operation to the 5-year follow-up. 95 % confidence intervals were additionally calculated for the mean differences for each ROM. The standard limit of 0.05 for the P value of two-sided tests was considered statistically significant. The normality assumption with respect to data on the differences in ROM was evaluated using quantile plots.
The study was approved by the Medical Research Ethics Committee at Lund University (LU-443-99).
Results
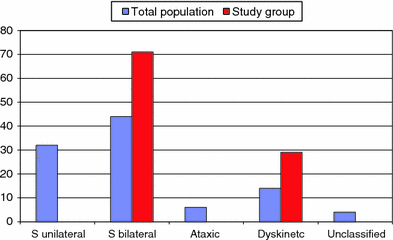
There were 24 children (19 boys, 5 girls) that fulfilled the inclusion criteria. Mean age at index operation was 7.6 (2.8–13.2) years. None of the children operated on with unilateral VOPF died within 5 years postoperatively, and no child was lost from follow-up. Twenty-three of the 24 children were in GMFCS IV or V (Fig. 2), and all had spastic bilateral or dyskinetic CP (Fig. 3). The characteristics of these 24 children are presented in Table 1.
Distribution of GMFCS levels (in percent) in the study group (24 children) compared to the total population with CP in Skåne and Blekinge in 2009 (693 children) [18] Distribution of subtypes (in percent) in the study group (24 children) versus the total population of all children with CP over the age of four in Skåne and Blekinge in 2009 (590 children) [18]. S Spastic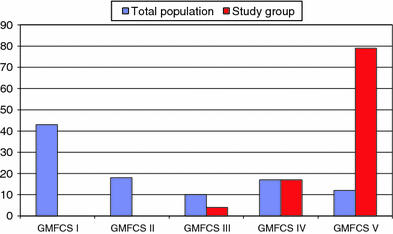
Characteristics of the 24 children treated with unilateral varus osteotomy of the proximal femur (VOPF)
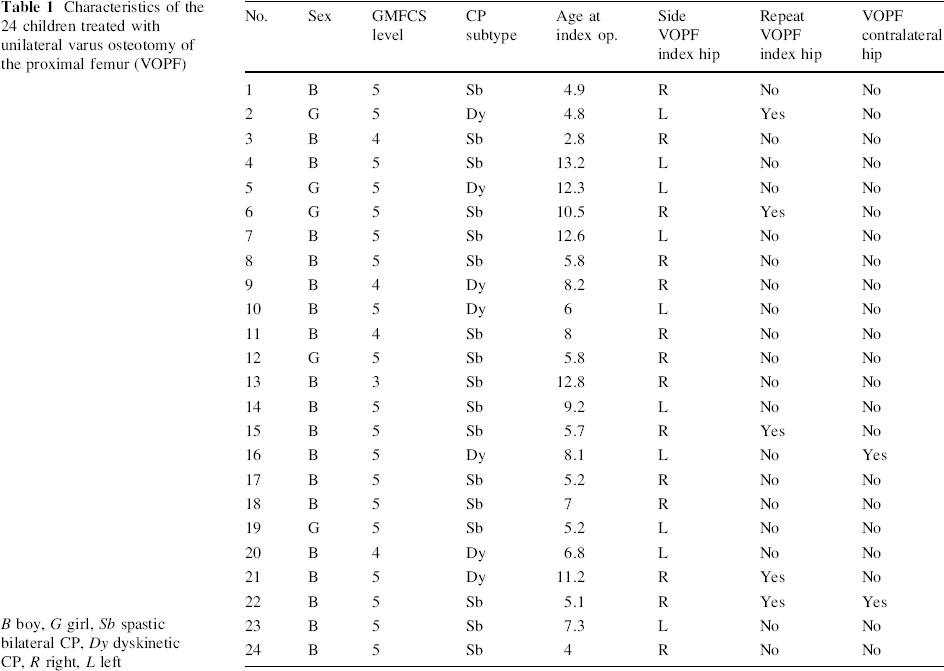
B boy, G girl, Sb spastic bilateral CP, Dy dyskinetic CP, R right, L left
Two children moved into the area after their index operations. For these two children, information on preoperative ROM is lacking. The result regarding ROM is consequently based on 22 children.
All 24 children were operated on with bilateral adductor-psoas tenotomy, 16 on a previous occasion and 8 simultaneously with the index procedure. Seven of the children were operated on with Dega osteotomy simultaneously with the index operation.
During the 5-year follow-up, 5 children had a repeat VOPF of the index hip and 2 children had VOPF of the contralateral hip 1 and 2.3 years after the index operation.
The MP before the index operation was 65 (38–100) in the index hips and 29 (7–52) in the contralateral hips. At follow-up, the MP was 34 (8–75) in the index hips and 26 (0–86) in the contralateral hips. The two contralateral hips operated on with VOPF had MPs of 50 and 29 at time of the index procedure. The boy with an MP of 50 % was in poor general condition, and it was therefore decided that only the most displaced hip would be operated on. At follow-up, 6 of the index hips had an MP exceeding 40 %. Three of them have been operated on with VOPF since the 5-year follow-up. One boy died 6 years after the index operation and had no reoperation. Two children had a decreasing MP and have not been reoperated on. Among the contralateral hips, 3 hips had an MP of more than 40 % at the 5-year follow-up. Two of them have a decreasing MP and no repeat surgery is planned. One of them represents one of the two contralateral hips operated on within 5 years. The third case (with an MP of 86 %) is a boy planned for surgery. The surgery has been delayed because of other medical problems.
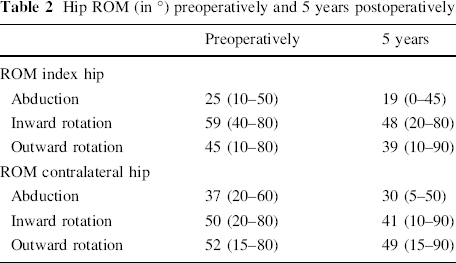
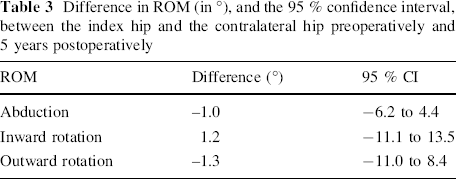
The mean range of hip abduction (examined with extended hips) decreased by 6° in the index hip and 7° in the contralateral hip between the preoperative examination and the 5-year follow-up (Table 2). The difference in the range of abduction between the index and contralateral hips was 12 (0–40) before the index operation and 11 (0–28) at follow-up. The range of hip rotation inwards/outwards decreased by 11/6° in the index hip and 9/3° in the contralateral hip. The mean difference in range of motion between the index and contralateral hips increased from 13° (0–55°) to 22° (0–60°) for inward rotation and from 13° (0–45°) to 17° (0–80°) for outward rotation. The changes in the difference in ROM between the hips preoperatively compared with during the follow-up were not statistically significant (Table 3).
Hip ROM (in °) preoperatively and 5 years postoperatively
Difference in ROM (in °), and the 95 % confidence interval, between the index hip and the contralateral hip preoperatively and 5 years postoperatively
Discussion
This study is based on a total population of children with CP, which is a major strength. All 24 children operated on with unilateral VOPF had severe motor impairment (GMFCS III–V). After 5 years, 2 of the 24 children had been operated on with FO in the contralateral hip. The difference in range of hip motion between the index hip and the contralateral hip did not change significantly during the 5 years.
One of the contralateral hips showed severe displacement at follow-up, and preventive surgery is planned for this boy. On the other hand, one of the two boys operated on with VOPF in the contralateral hip already showed displacementat the time of the index operation, and normally would have been operated on with bilateral VOPF on the first occasion.
The number of children in the study group is quite small. However, they represent a subgroup of a total population of children with CP, and no child was lost from follow-up. Another limitation is the lack of preoperative ROM measurements in two cases. All children were treated nonoperatively to reduce spasticity and muscle contractures, with standing frames and proper positioning when sitting and lying. Some children had spasticity-reducing treatment with botulinum toxin.
Several studies have shown that children operated on with unilateral soft-tissue release have a high risk of displacement of the contralateral hip [14–16], and these authors conclude that soft-tissue release should always be carried out bilaterally. There are, to our knowledge, no studies showing inconsistent results.
Regarding the prognosis for the contralateral hip after VOPF, the conclusions of earlier studies are inconclusive. Some authors consider that only the displaced hip should be operated on [1–3], while others recommend bilateral osteotomy in all cases [4–6].
Carr and Gage [1] analysed 36 unilaterally operated children after an average of 4.8 years (minimum 1 year). Children operated on with unilateral VOPF had a 0.9 % deterioration of MP in the contralateral hip, whereas those operated on with unilateral soft-tissue release had a 12.8 % deterioration of MP in the contralateral hip.
Gordon et al. [2] examined 48 patients 5 (2–9) years after unilateral VOPF and soft-tissue release. The condition in the contralateral hip did not worsen, regardless of age and ability to walk. The authors conclude that skeletal surgery should not be an indication for operation on the contralateral hip.
Settecerri et al. [3] studied 48 children who underwent unilateral VOPF, two of whom needed VOPF in the contralateral hip within 5 (2–15) years. The conclusion was that unilateral VOPF is effective in unilateral displacement.
Noonan et al. [4] studied 35 children who had been unilaterally operated on with a follow-up of 4.2 (1–12) years. Thirty-four children were operated on with unilateral soft-tissue release and 19 with unilateral VOPF. Fifteen children were later operated on with preventive surgery of the contralateral hip. The authors conclude that both hips should be operated on, even if only one shows displacement.
Canavese et al. [5] studied 27 children who were operated on with unilateral VOPF. Twelve needed VOPF in the contralateral hip. Their study group included also children operated with unilateral soft tissue release. The authors conclude that bilateral surgery should be considered in patients with GMFCS IV–V with unilateral dislocation, even though the contralateral hip looks normal.
After unilateral soft tissue release, the balance of strength between the adductor and abductor muscles shifts towards abduction. After unilateral surgery, this may result in a pelvic tilt with increased adduction on the contralateral side and an increased risk of contralateral displacement (Fig. 4). After unilateral VOPF, the greater trochanter is proximalized, resulting in abductor insufficiency. This does not result in increased adduction on the contralateral side (Fig. 5).
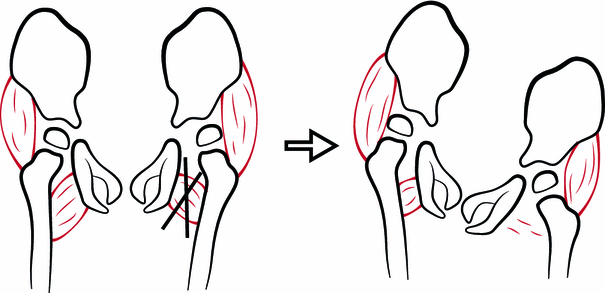
Adductor tenotomy of the left hip resulting in pelvic tilt with increased adduction and decreased femoral head coverage of the contralateral hip
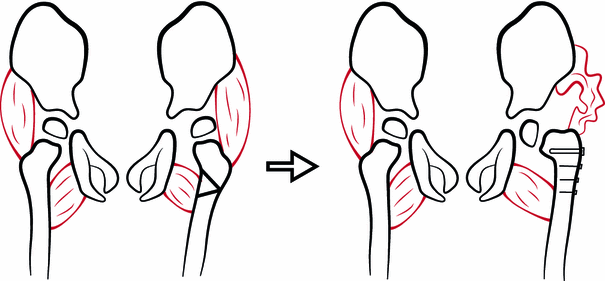
Varus osteotomy of the left hip, resulting in abductor weakness without predisposition to adduction of the contralateral hip
The different results and opinions in the literature can be explained by the fact that studies showing a high risk of contralateral displacement contain children operated on with both unilateral VOPF and unilateral soft-tissue release.
Most children with hip displacement are nonwalkers (Fig. 2). Pelvic balance and symmetric ROM is important for their sitting comfort. The difference in ROM between the operated and the contralateral hips did not change significantly in the present study. Both hips showed less mobility after 5 years, which is concordant with earlier studies of the development of ROM in children with CP [17]. Owers et al. [6] performed bilateral soft-tissue release and VOPF on 30 children. At follow-up after 3 years, 44 % of the children had a windswept deformity, compared to 50 % preoperatively. This indicates that the muscle imbalance that creates unilateral hip displacement and windswept deformity is not permanently rebalanced by bilateral surgery. Carr and Gage [1] described no tendency for windswept deformity after unilateral VOPF.
Five children (21 %) were treated with repeat VOPF of the index hip in the present study. In the study by Settecerri et al. [3], 15 % had a poor result, with an MP of >50 % of the index hip. Canavese et al. [5] reported repeat surgery, including soft tissue release, in 44 % of the index hips at follow-up. One could speculate that in some of the cases treated with unilateral VOPF, the procedure results in pelvic tilt with the operated side higher. If so, a unilateral VOPF could result in a reduced risk for contralateral displacement and an increased risk for redisplacement of the ipsilateral hip (Fig. 6).
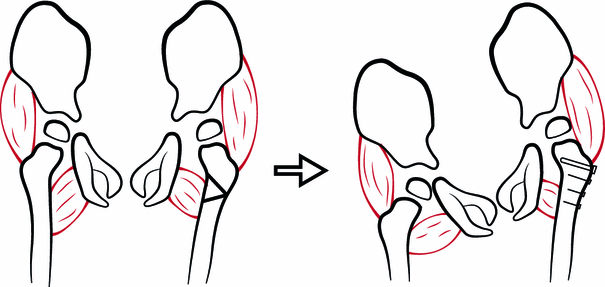
Varus osteotomy of the left hip resulting in pelvic tilt with adduction and decreased femoral head coverage of the ipsilateral hip
Unilateral VOPF results in a leg length discrepancy. However, most children are nonwalkers, and the magnitude of discrepancy should not impair their sitting ability.
We conclude that children with CP and unilateral hip displacement have a low risk of later contralateral displacement after being operated on with unilateral VOPF. This supports healthcare programmes that advocate unilateral VOPF in children with unilateral hip displacement.