
Abstract
Abstract
Background
We analyzed preoperative CT scans of hips with slipped capital femoral epiphysis (SCFE) for characteristics that could be predictive of intraoperative epiphyseal stability and developed a set of imaging criteria for stable and unstable SCFE. We then compared this grading system with the Loder classification.
Methods
We reviewed preoperative CT imaging to develop a SCFE stability classification system. Three orthopaedic surgeons used the classification system to grade stability on a series of SCFE hips. Kappa was used to evaluate intra- and interobserver reliability among the observers. A series of SCFE hips treated with open procedures in which intraoperative stability was determined under direct visualization was evaluated. Intraoperative stability was compared with stability ratings as determined by the CT classification system and the Loder classification system.
Results
Interobserver reliability among our three observers was κ = 0.823 (95% confidence interval (CI) 0.414 to 1.0; p < 0.001). Intraobserver reliability was κ = 0.901 (95% CI 0.492 to 1.31; p < 0.001). In all, 27 hips were used in the comparison of intraoperative stability with the Loder and CT classification systems. CT-predicted stability exhibited 78% concordance with intraoperative stability. The sensitivity and specificity of CT-predicted stability was 75% and 82%, respectively, versus Loder sensitivity of 69% and specificity of 91%.
Conclusion
The CT evaluation method provided is easy to use and can help to improve the accuracy in determining preoperative epiphyseal stability, which may lead to improved treatment outcomes for this population.
Level of Evidence
III
Introduction
Over the last few decades, significant improvements have been made in the operative strategies for slipped capital femoral epiphysis (SCFE), however, during the same 25 years, there has only been a modest progression in the diagnostic approach to the pathology. SCFE has historically been classified in terms of acuity, severity and stability. The stability classification system, described by Loder, helps stratify by avascular necrosis (AVN) risk, making it the most important of the three classification systems in terms of prognostic ability. 1 However, the terminology used in the classification system – stable versus unstable – has been the source of some confusion.
The terms ‘stable’ and ‘unstable’ have mechanical implications that Loder was unable to confirm intraoperatively in his landmark retrospective analysis. 1 Stability refers to whether the metaphysis can move in unison with the epiphysis (stable) or if the relationship is disrupted causing the two components to move independent of each other (unstable). In contrast, acuity is defined by duration of symptoms and severity is defined by the degree of displacement or angulation on radiographs, both easily obtained via a retrospective chart and radiograph review. Loder attempted to retrospectively evaluate the amount of reduction that occurred based on preoperative and postoperative radiographs. The radiographs were not standardized, however, and he ultimately used a patient's ability to walk as a proxy for stability. It was reasoned that subjects who were unable to bear weight on the affected extremity with or without assistive devices likely had unstable movement of the epiphysis on the metaphysis as the source of that pain. Subsequent papers have noted instances in which Loder's classification of stability did not match the intraoperative assessment of epiphyseal stability.2–4
Ziebarth et al 4 pioneered the use of intraoperative epiphyseal stability as a new benchmark, determining that the best assessment of the epiphysis was with direct visualization during surgical hip dislocation. By comparing Loder stability (as determined by weight-bearing) with actual intraoperative findings of epiphyseal stability, Ziebarth et al 4 determined that Loder's criteria had a sensitivity of only 39% and a specificity of 76%. Our own institutional experience using the Loder system preoperatively to assess epiphyseal stability based on weight-bearing has identified slips that were classified as stable and yet were then observed to demonstrate epiphyseal instability intraoperatively. Moreover, the opposite has also been observed, wherein patients that presented to the emergency department (ED) unable, or unwilling, to bear weight, have shown no movement of the epiphysis on the metaphysis during arthrotomy.
To this end, we analyzed preoperative CT scans of hips with SCFE for characteristics that could be predictive of intraoperative epiphyseal stability. We developed a set of imaging criteria for stable and unstable SCFE and asked orthopaedic surgeons in our group to grade a subset of our cohort blinded using this framework. The purpose of this study was two-fold. Our primary aim was to establish criteria of preoperative CT imaging characteristics that accurately and reliably predict SCFE intraoperative stability. Our secondary aim was to compare the accuracy of this method with historical methods, such as the Loder classification.
Materials and methods
In 2013, we began an institutional review board approved, prospective SCFE registry. All patients that underwent surgical treatment at our institution from 2013 were asked to participate in the registry. Written assent/consent has been obtained from all subjects included in the registry. In this study, we retrospectively evaluated the records of all hips that were treated with an open surgical procedure between 2013 and 2018. After exclusion criterion were applied (Fig. 1) we were left with a final cohort of 27 hips.
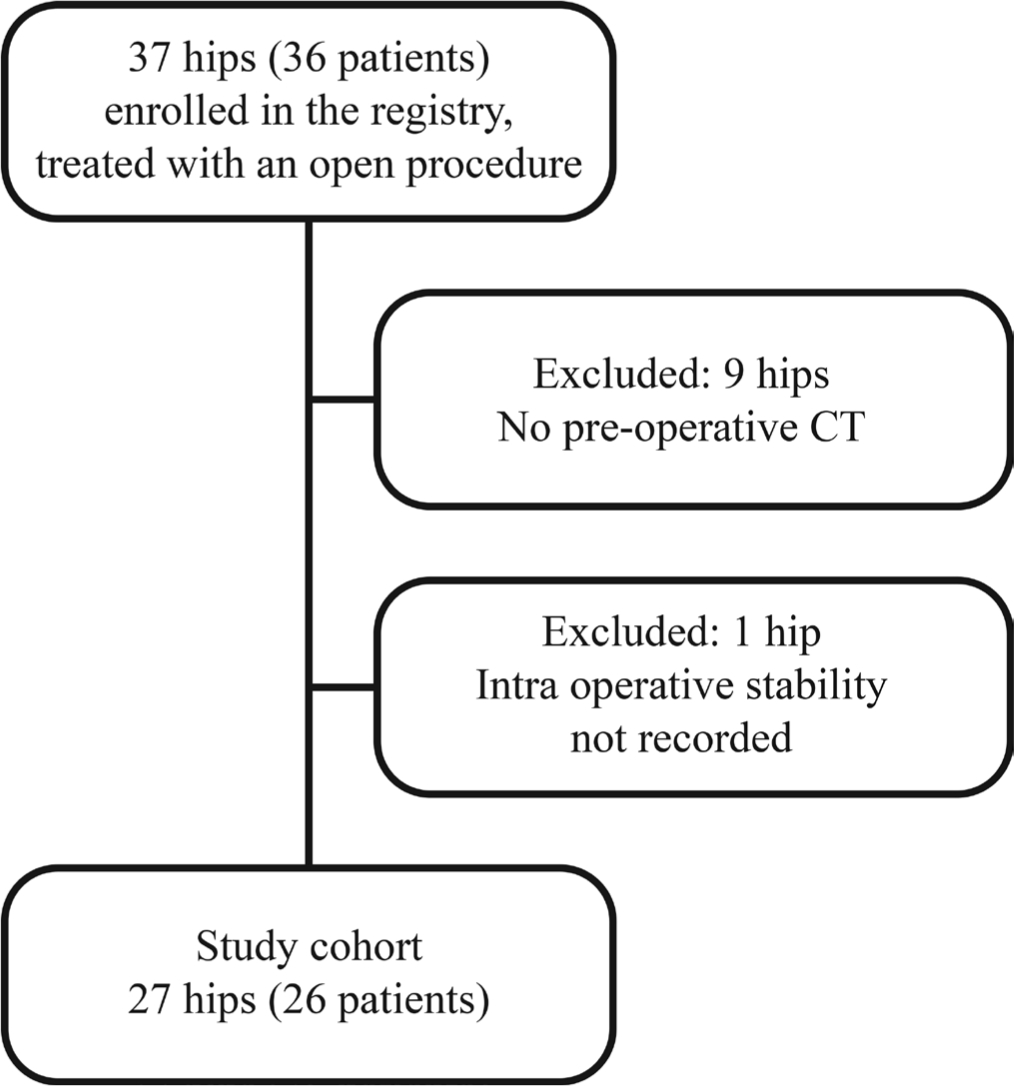
Flow diagram illustrating exclusion criteria.
The following surgical procedures were performed to treat patients in this cohort and are described below: Modified Dunn (n = 20), Parsch Method of open reduction internal fixation (n = 3) and open surgical dislocation with primary osteochondroplasty (n = 4). The Modified Dunn procedure involves surgical hip dislocation, capital realignment and epiphyseal fixation to achieve appropriate correction of the proximal femoral deformity while protecting femoral head blood supply. 2 This procedure aims to minimize complications such as secondary osteoarthritis and femoroacetabular impingement, enables intraoperative monitoring of blood supply to the femoral head, however, is a technically more challenging procedure than in situ fixation. The Parsch Method of open reduction internal fixation involves an open capsulotomy, haematoma decompression, and gentle, finger-aided reduction of the epiphysis. 5 We utilize the distal portion of the Smith-Peterson approach to perform an anterior hip capsulotomy that allows for direct visualization of the head-neck junction. Then a separate lateral incision is utilized to place the screws.
We retrospectively reviewed data from our prospective registry including age, sex, laterality of slip, dates of CT and operation, surgical method used, acuity, severity, Loder classification at time of initial presentation, intraoperative assessment of stability and surgeon performing the procedure. This prospectively collected data was verified by a retrospective chart review. Acuity was determined by duration of symptoms relative to three weeks. 6 Acute cases are those with symptom duration less than three weeks, chronic cases exhibit symptom duration greater than three weeks and acute on chronic cases are those with existing symptoms where a sudden change or worsening of symptoms occurs. We utilized intraoperative stability as the benchmark by which we compared the CT findings as defined above. Intraoperative stability was assessed via direct visualization of the epiphyseal-metaphyseal junction. A hip was determined to be unstable if the anterior periosteum was torn and the epiphysis was mobile relative to the metaphysis. 7
We reviewed preoperative CT imaging of hips in axial, coronal, sagittal and oblique views from 48 hips treated with a variety of treatment methods, not hips treated exclusively with open procedures. During this initial review, we defined our terminology and set criteria for stable versus unstable SCFE patterns on CT, as noted above. We then revisited the imaging for each hip using our new terminology, stating whether there was presence of a fracture line (Fig. 2), callus (Fig. 3), spot-welding (Fig. 4) and/or a wedge sign (Fig. 5) (see definitions in Table 1). Ultimately, we classified a slip as unstable if a fracture line was present on all slices of any view of the preoperative CT scan. We classified a slip as stable if a fracture line was absent. Any callus, spot-welding or other soft-tissue details on imaging were considered to be supportive of a stable SCFE but were not considered pathognomonic. If a fracture line ran continuously through some callus or spot-welding, this was classified as an unstable SCFE (Fig. 6).
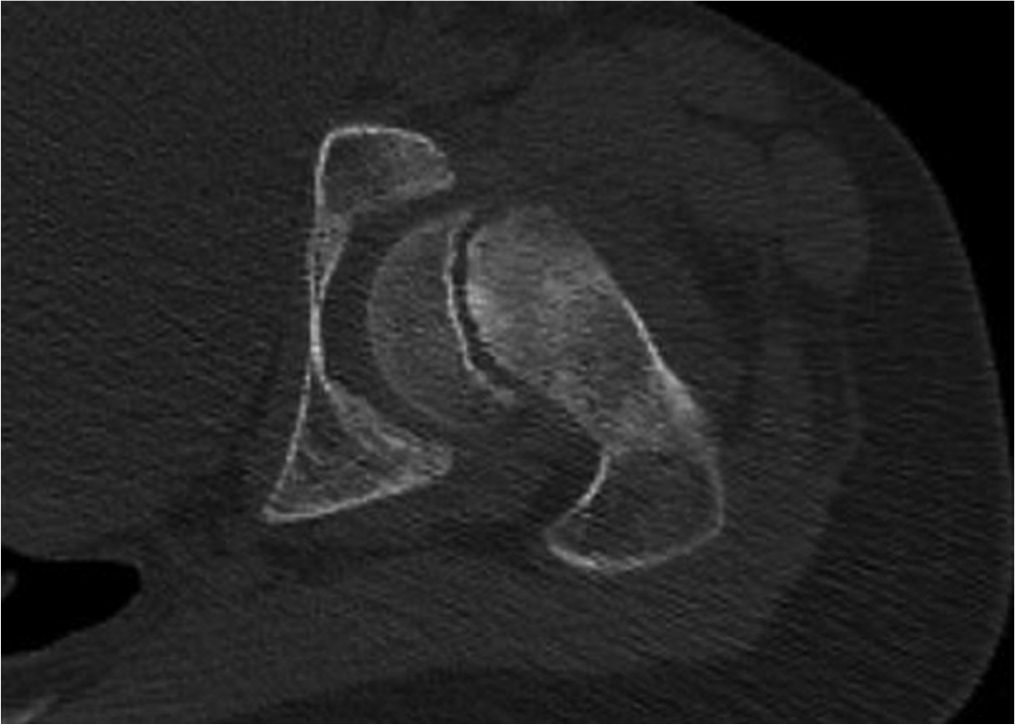
A clearly visible fracture line through the physis. ©SD PedsOrtho.
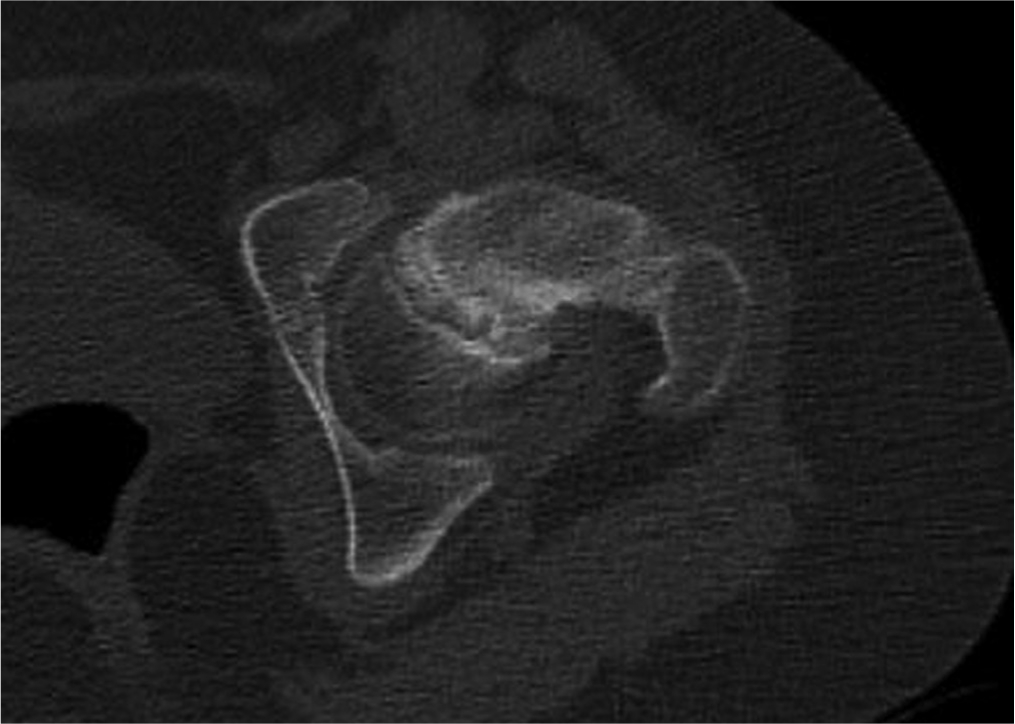
A thickened, cloudy appearing physis is indicative of callus formation following slipped capital femoral epiphysis. ©SD PedsOrtho.
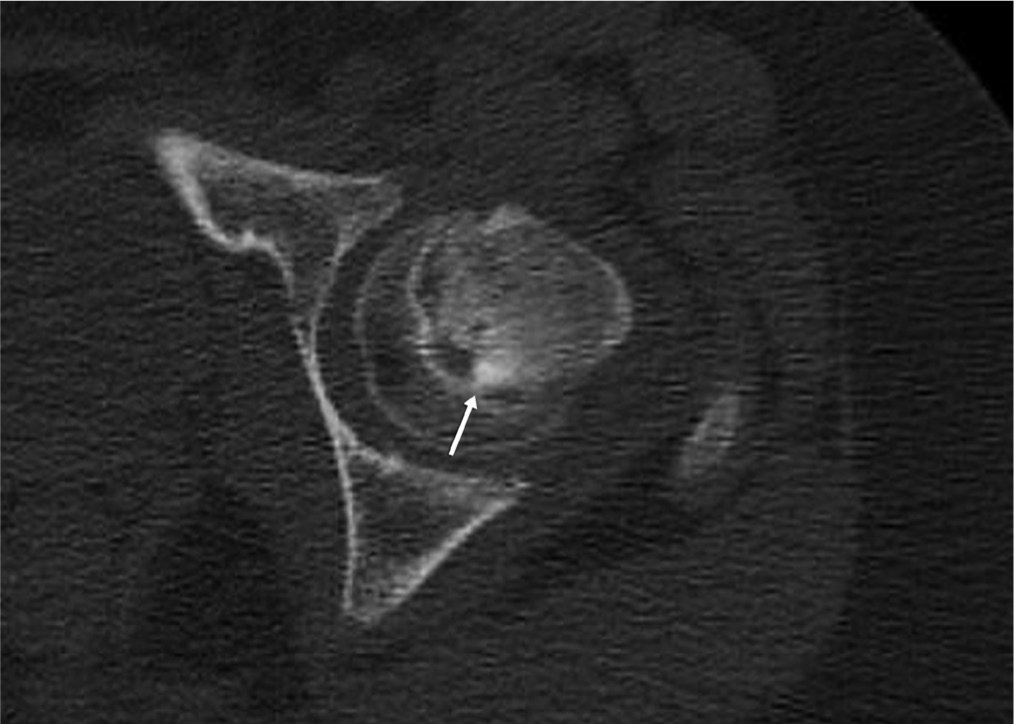
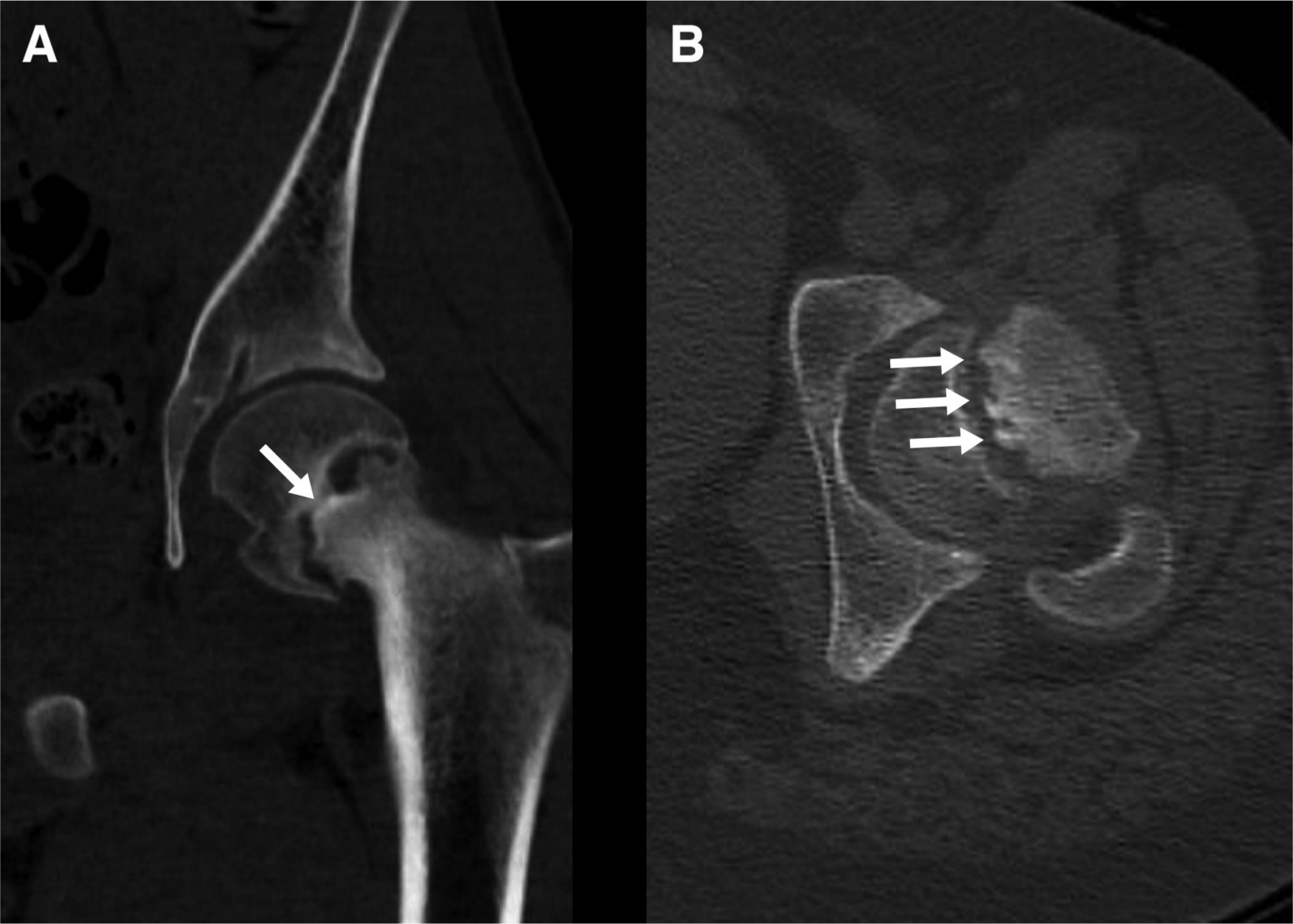
The arrow points to a focal area of healing across the physis, which we refer to as ‘spot-welding’. ©SD PedsOrtho.
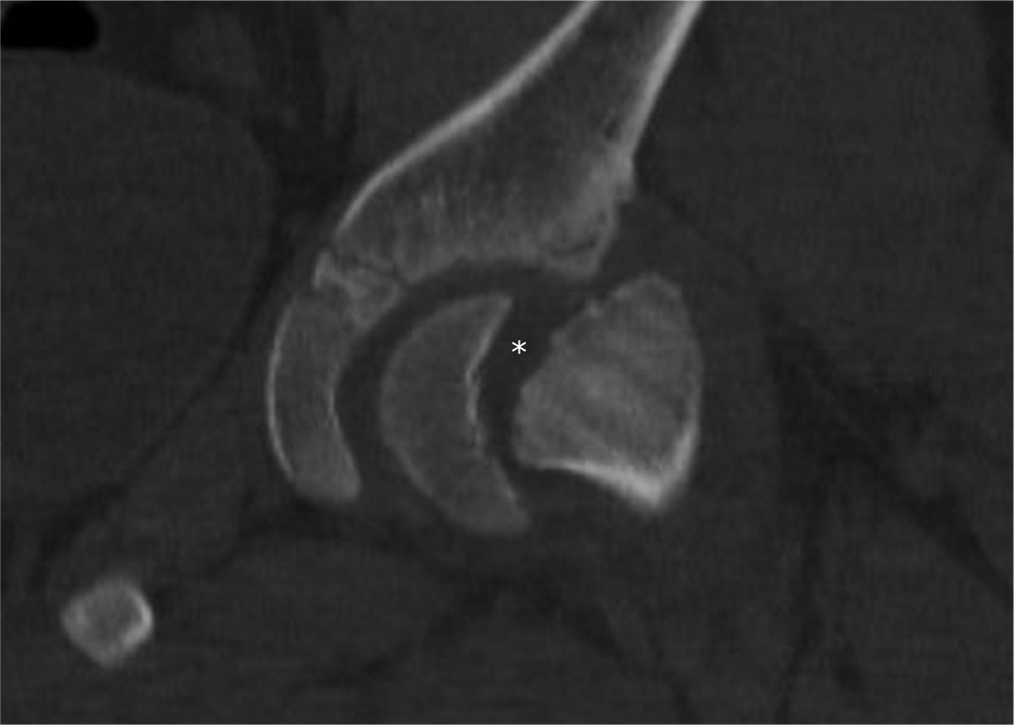
The wedge sign, seen here in the coronal plane, is the triangular lucency between the epiphysis and metaphysis, tapering inferiorly, as noted by the asterisk. ©SD PedsOrtho.
Descriptive terms and criteria of radiographic findings
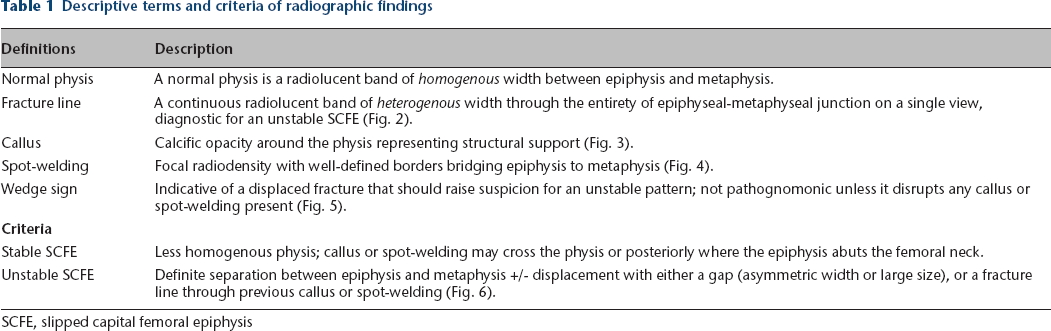
SCFE, slipped capital femoral epiphysis
Using sample images, we created a teaching module (supplementary material) to train physicians on how to predict stability via CT imaging; we provided a guide with example images, definitions and criteria for stable and unstable SCFE. We also used two example cases (one stable and one unstable), to scroll through multiple views on CT, discussing how to use the characteristics to predict epiphyseal stability.
We then provided a list of 25 CT scans to three paediatric orthopaedic surgeons in our department for grading purposes who had not been previously exposed to the imaging. This list was composed of 13 stable and 12 unstable slips, selected at random (taking care to exclude the two cases used in the training module). The similar distribution of unstable to stable slips is a result of our inclusion criteria. We only included subjects treated with an open procedure who had a preoperative CT scan. At this institution, CT scans and open procedures are performed at a higher rate in unstable slips. Our institutional rate of unstable slips is approximately 15%. The surgeons were blinded, provided only with the medical record number, CT date and laterality of SCFE. They were tasked with grading each case as stable or unstable using our criteria for the purpose of reliability. One grader repeated this list blinded for intrarater reliability.
Statistical analysis
All statistical analyses were performed with SPSS version 25 (IBM, Armonk, New York). The Shapiro-Wilk test of normality and Levene's test of homogeneity of variances was performed on all continuous data. Normally distributed data were evaluated using analysis of variance; non-normally distributed data were evaluated using Mann-Whitney U. The kappa coefficient was used to determine intra- and interobserver reliability, and to evaluate categorical data. Sensitivity and specificity were calculated from 2 × 2 tables. Statistical significance was set as p < 0.05.
Results
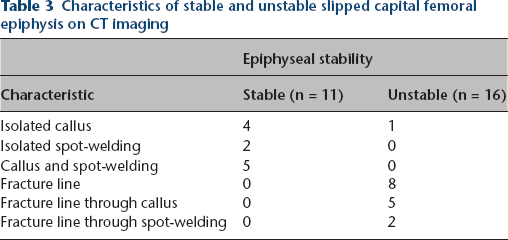
Demographic information is presented in Table 2. In all, 11 hips were determined to be intraoperatively stable and 16 hips were determined to be intraoperatively unstable. Stable slips did not exhibit a fracture line and often demonstrated callus or spot-welding from metaphysis to epiphysis (Table 3). A total of 15 unstable hips exhibited fracture line, seven of which were found in conjunction with callus or spot-welding. Six out of seven of these compound images with both fracture line and callus or spot-welding were acute on chronic slips. Of the eight unstable hips with isolated fracture lines, six had the presence of a wedge sign on coronal view.
Demographics by stability
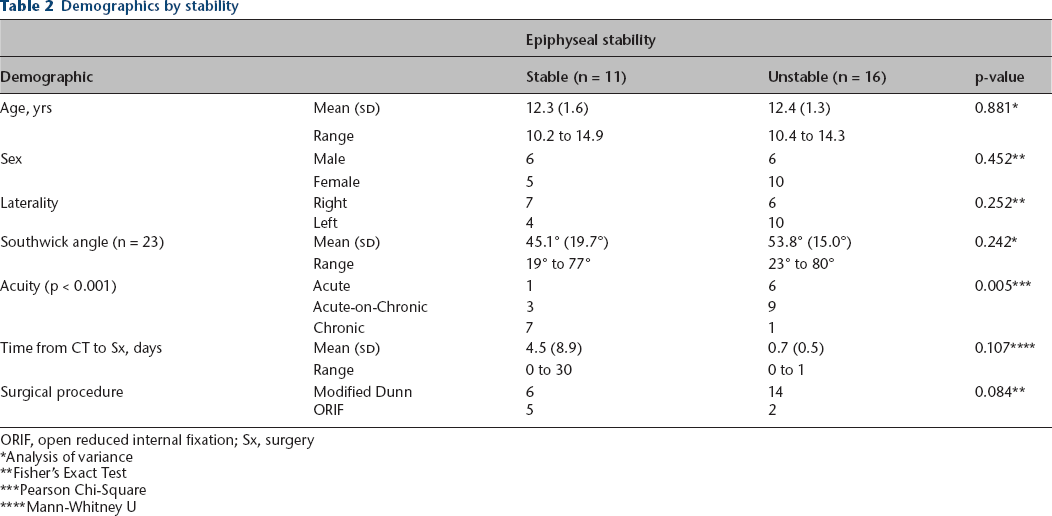
ORIF, open reduced internal fixation; Sx, surgery
Analysis of variance
Fisher's Exact Test
Pearson Chi-Square
Mann-Whitney U
Characteristics of stable and unstable slipped capital femoral epiphysis on CT imaging
With respect to CT grading conducted by three independent orthopaedic surgeons within our institution, interobserver reliability among our three observers was κ = 0.823 (95% confidence interval (CI) 0.414 to 1.0; p < 0.001). Intraobserver reliability measured by one observer over a month apart was κ = 0.901 (95% CI 0.492 to 1.31; p < 0.001). CT-predicted stability exhibited 78% concordance with intraoperative stability. The sensitivity and specificity of CT-predicted stability was 75% and 82%, respectively, versus Loder sensitivity of 69% and specificity of 91%.
Additional analysis was performed in which our CT classification was combined with Loder's classification. Subjects that were classified as unstable using either of the two classification systems were deemed unstable, all other subjects were deemed stable. This was compared with the intraoperative assessment of stability. This changed the sensitivity and specificity to 88% and 73%, respectively. The positive predictive values using the Loder classification alone, CT-predicted stability alone or a combination of the two evaluations were 92%, 86% and 82%, respectively. However, the negative predictive value improved with the combination of the Loder classification and CT-predicted stability findings compared with the Loder classification alone or the CT-predicted stability alone, becoming 80% compared with 67% and 69%, respectively.
Discussion
The primary goal of SCFE treatment is to stop slip progression, with the secondary goal of restoring proximal femoral anatomy. Our SCFE treatment patterns have evolved during the enrolment period of our SCFE registry. Early on, we performed the Modified Dunn for stable and unstable SCFE. Over time, we found that the rate of AVN was unacceptable in patients with stable SCFE that were treated with the Modified Dunn and have changed our treatment algorithm accordingly. 8 Currently, the Modified Dunn procedure is only used in patients with unstable, acute-on-chronic, moderate to severe slips. Stable, mild slips are treated with in situ screw fixation. Stable, moderate to severe slips are treated with in situ screw fixation followed by osteochondroplasty or proximal femoral osteotomy in symptomatic patients based on the magnitude of deformity. Finally, unstable, acute, moderate to severe slips are treated with the Parsch Method.
The overall incidence of SCFE is increasing, with 10% to 35% of slips classified as unstable using Loder's classification.9,10 Determining a reliable and accurate classification system for predicting intraoperative stability of SCFE helps inform surgical decision-making, including choice of procedure. An incorrect choice of procedure in either direction can pose additional risk to the patient. An unrecognized unstable slip may be scheduled on a less urgent basis than a recognized unstable slip which may risk further displacement of the femoral epiphysis and possible disruption of the retinacular vessels to the femoral head. In addition, intraoperative positioning of an unstable slip must be performed cautiously. If the surgeon does not recognize that the hip is unstable the femoral head may slip further due to unintentional movements of the leg while the patient is under anaesthesia. These issues can lead to AVN and may account for a portion of the reported AVN rate in so-called stable slips. Stable slips treated with more invasive procedures such as the Modified Dunn may have a higher incidence of AVN rates than stable slips treated with in situ pinning, which has virtually no risk for AVN.11–13 As we continue to determine optimal treatment strategies for each case, imaging modalities such as CT can provide a wealth of information to better characterize the injury pattern.
Loder et al 1 presented a clinical classification system useful in differentiating risk of osteonecrosis, not necessarily for defining and predicting physeal stability. Subjects were labeled as stable or unstable on the basis of weight-bearing ability, not observation of physeal stability. The use of intraoperative fluoroscopy and the development of open procedures such as the Modified Dunn enhance our visualization of SCFE pathology, specifically whether the epiphysis is structurally linked to the metaphysis. Pre- and perioperative imaging paired with direct intraoperative visualization of the epiphyseal-metaphyseal junction will contribute to a more comprehensive definition of an unstable slip and may eventually lead to a change in terminology. Perhaps it is more appropriate to refer to hips with and without the ability to bear weight, as ‘Loder (-) negative’ and ‘Loder (+) positive’ hips, rather than the historical ‘stable’ and ‘unstable’, respectively, when using the Loder classification system for AVN prediction.
We observed a Loder classification sensitivity and specificity of 69% and 91% respectively, this is improved compared with the findings of Ziebarth et al 4 who reported a sensitivity of 39% and specificity of 76% when comparing the Loder classification with stability determined under direct visualization. The combination of inability to bear weight and the presence of a clear fracture line were both observed to be strong data points for determining an unstable SCFE in our study cohort. Preoperative CT-based criteria resulted in an accurate and reliable prediction of intraoperative epiphyseal stability in SCFE patients. The concordance between CT stability and intraoperative stability of 78% suggests moderate to high accuracy for identifying epiphyseal stability. The kappa for inter- and intraobserver reliability of 0.823 and 0.901, respectively, suggests an acceptable level of agreement and reliability. The specificity of 82% for CT grading alludes to the notion that a clear fracture line, particularly in the absence of callus, is helpful for accurately identifying an unstable SCFE that could be falsely identified as being stable by the Loder classification.
There are some limitations to this study. The benchmark for the purpose of this study – intraoperative determination of epiphyseal stability – has some inherent degree of subjectivity because it is based on the surgeon's best clinical judgment. However, intraoperative epiphyseal stability for all subjects in this cohort was determined under direct visualization and in this field of research there is no current benchmark for determining SCFE stability, which further underscores the need for imaging studies to better characterize the nature of an unstable versus a stable SCFE. This data was collected prospectively with the question of intraoperative stability posed at the time of the procedure. Any indeterminate cases were excluded, establishing what we believe to be a more appropriate study cohort.
In addition to the limitations of this study, there are also risks associated with radiation exposure due to the radiographic evaluation methods used in this study. CT and traditional radiographs are not the only tools available when evaluating physeal stability. Kallio et al, 14 Parsch et al 5 and Loder 15 all indicate that the presence of an effusion upon ultrasound evaluation is indicative of an unstable slip. Effusion may also be recognized with MRI, which would reduce exposure to radiation.
Due to the higher than expected observed sensitivity and specificity of the Loder classification, as well as the additional stability information provided by the CT evaluation system we have provided here, we have changed our preoperative planning algorithm. Prior to this study, patients being evaluated for SCFE were assessed with an anteroposterior and frog pelvis radiograph or cross table lateral based on the patient's symptoms. We continue to document weight-bearing and ambulation status and order routine anteroposterior and frog lateral pelvis radiographs for all suspected SCFE patients and now use the following algorithm after radiograph and ambulation status has been reviewed: patients with mild slips on plain radiographs that can bear weight on their affected limb (Loder negative) are admitted and scheduled for in situ pinning. Patients unable to bear weight (Loder positive) or with severely displaced slips are admitted and an urgent CT is obtained in the ED. Subjects found to have a stable physis based on the CT findings outlined in this study are treated with in situ pinning on a non-urgent basis. Subjects with CTs that indicate physeal instability are treated urgently with more invasive procedures such as the Parsch Method or the Modified Dunn. We are unable to obtain ultrasound or MRI for these patients in our ED due to personnel and resource constraints. An MRI may postpone surgical stabilization by one to two days at our institution and we do not always have ultrasound technicians available in the ED. As such, these modalities have not been widely adopted at our institution.
Stability classification impacts surgical decision making differently today than when it was first defined several decades ago. The CT evaluation method provided is a simple, fast and accurate tool to implement in clinical practice for diagnostic purposes. The specificity of the test combined with the straightforward learning module make it relatively easy for surgeons to incorporate into their practice. While the Loder classification system was a very important step towards improving the predictability of SCFE treatment, we believe that selective preoperative CT imaging, in conjunction with the Loder classification system is another step towards improving patient care. We stand to improve patient care by better characterizing this injury pattern, using tests with greater sensitivity and specificity to stratify treatment and by establishing new standards for future investigation.
Footnotes
Acknowledgements
This study was supported by the Division of Orthopedics, Rady Children's Hospital, San Diego.
ATP reports holding stock or stock options in Imagen and paid consultancy for OrthoPediatrics, outside the submitted work.
VVU reports being a paid presenter or speaker for BroadWater: DePuy, a Johnson & Johnson Company, Nuvasive and OrthoPediatrics; research support from EOS Imaging and Pacira; paid consultancy for Globus Medical and OrthoPediatrics; and holding stock or stock options in Imagen.
MFC, CRL, JDB and PH have nothing to disclose.
CRL: Study design, Manuscript preparation, Data interpretation.
JDB: Study design, Data analysis, Data interpretation, Manuscript preparation.
PH: Data collection, Manuscript preparation.
EWE: Data collection, Data interpretation, Manuscript preparation.
ATP: Data collection, Data interpretation, Manuscript preparation.
VVU: Study design, Manuscript preparation, Data interpretation