
Abstract
Purpose:
Our study aimed to present health-related quality of life (HRQL) after combined bone reconstruction in nonambulatory patients with cerebral palsy (CP) after at least a 2-year follow-up and to assess its impact on HRQL using the Caregiver Priorities and Child Health Index of Life with Disabilities questionnaire (CPCHILD) as the primary outcome measure.
Methods:
In this prospective study, we analyzed 31 nonambulatory patients with spastic or mixed CP (GMFCS levels IV–V) who underwent hip reconstructive surgery between 2015 and 2021. The surgical procedures included one-sided varus derotation osteotomy of the femur with Dega transiliac osteotomy and, on the opposite side, varus derotation osteotomy (VDRO) of the femur with shortening and, as needed, Dega pelvic osteotomy.
Results:
The study demonstrated significant improvement in the hip joint motion range, as assessed by the Thomas test, in hip abduction and rotational movements of the hip, as well as reduction of spasticity. The procedures also resulted in significant radiographic improvement of the femoral head coverage. The assessment of symptoms and problems associated with the hip revealed a positive influence of the surgery on pain, contractures, toileting/perineal hygiene, dressing, seating, transferring, and position changes. The mean improvement at a follow-up visit was significant in all domains of the CPCHILD, except for communication and social interaction.
Conclusion:
Hip reconstruction with VDRO and Dega pelvic osteotomy can enhance the HRQL of children with CP. These surgical interventions can help to achieve the correct hip position and to reduce pain, which positively affects the patient QL, although proactive treatment results in less invasive procedures.
Level of Evidence:
IV case series.
Introduction
Hip displacement is the second most common orthopedic manifestation, after equinus of the ankle in children with cerebral palsy (CP). The prevalence of hip displacement, defined as migration percentage (MP) >30%, is 35% for the whole CP population, rising to 90% for children at Gross Motor Function Classification System (GMFCS) Level V.1 –3 Hip displacement is directly related to GMFCS Level but not motor type.1,4 Typically, it is associated with increased spasticity and shortening of the psoas and hip adductor muscles accompanied by weak hip abductors and extensors.5,6 Disturbed muscle balance forces disturb the growth of the proximal end of the femur and lead to acetabular dysplasia, 7 increased femoral anteversion, and coxa valga antetorsa.8,9 Progressive hip displacement may further result in hip dislocation, which can cause chronic pain and reduce the range of hip motion. The natural history of spastic hip disease (SHD) shows that 50% of dislocated hip joints are painful.10 –12 Hip surveillance aims to monitor hip development, offer management options to slow or reverse hip displacement, and provide the best opportunity for good hip health at skeletal maturity.12,13
The perception of well-being and the ability to participate in specific life roles are essential aspects of health-related quality of life (HRQL). 14 Motor impairment, especially in children with CP, can limit their participation in various activities and negatively affect HRQL. 15 The Caregiver Priorities and Child Health Index of Life with Disabilities (CPCHILD) questionnaire was developed and validated to assess HRQL in severely impaired children with CP, including ratings of daily activities, mobility, comfort, communication, social interaction, and overall health status. 16
Orthopedic surgeons should regard hip reconstruction procedures, such as varus derotational osteotomy (VDRO) with or without pelvic osteotomy, as surgical procedures with well-described follow-up.17 –22 Previous research assessed the success of treatment mainly based on hip X-rays but without indicating the actual HRQL-related benefits of the procedures.17 –19
This study aims to present HRQL after bone reconstruction in nonambulatory CP patients with SHD (GMFCS levels IV–V, with spastic or mixed type of CP), after at least a 2-year follow-up and to assess the impact of the surgery on HRQL using the CPCHILD questionnaire as the primary outcome measure.
Materials and methods
It was a prospective observational study of 31 patients with spastic or mixed CP, who were nonambulatory and were admitted to our hospital for hip reconstructive surgery between 2015 and 2021. The surgeries performed were one-sided VDRO with Dega pelvic osteotomy, and on the opposite side VDRO with shortening and, as needed, Dega pelvic osteotomy. Soft-tissue release was performed based on clinical examination as simultaneous surgery if needed (in case of abductor contracture or windswept pelvis) before the hip reconstructive surgery. It concerned the iliopsoas, adductors, and hamstring muscles. Immobilization in an abductor orthosis (A-frame) was applied for both lower limbs for 4 weeks. The patients were mobilized by sitting with the orthosis on the day after the surgery. Then, after X-ray hip evaluation within 5 weeks postoperatively, rehabilitation focused on the hip joint was implemented (exercises increasing range of motion (ROM) and, if possible, strengthening the gluteal and quadriceps muscles of the thigh). Plate removal in our treatment protocol was performed 12 months after primary surgery.
The Institutional Review Board approved the study and informed written consent was obtained from the parents or primary caregivers due to the patient’s communication status and cognitive disability to self-report. The included patients met the following criteria: GMFCS IV–V, Reimers migration (MP) ≥50%, 23 using a wheelchair as the primary means of transportation, admitted to the hospital for hip reconstructive surgery and prophylactic surgery on the contralateral side, and at least 2-year follow-up. Exclusion criteria included previous hip joint surgery or receiving botulinum toxin within the last 3 months.
We assessed the patient’s demographics, comorbidities, motor abilities and physical condition, radiographic measurements, and HRQL using the CPCHILD questionnaire. The physical examination was performed with a goniometer to accurately evaluate the passive ROM in the hip and knee joints. We also assessed clinically the presence of scoliosis. Spasticity was evaluated using the Modified Ashworth Scale 24 in the iliopsoas, hip adductors, rectus femoris, and hamstring. X-ray was taken according to the guidelines of the American Academy for Cerebral Palsy and Developmental Medicine (AACPDM),25,26 and the X-ray measurements included MP. We did not routinely perform an X-ray of the scoliosis as it was not part of our study protocol.
The CPCHILD questionnaire was used to measure HRQL. It is a caregiver proxy, a disease-specific instrument designed for children with severe (GMFCS levels IV and V) CP. This psychometrically valid measure consists of 7 domains, with 37 items across the first 6 domains. The items are rated on a 6-point ordinal scale, with 0 being the worst and 100 being the best. The seventh domain rates the importance of the items to the child’s QL. 14 In addition, the Polish version of the questionnaire has been validated for children aged 2 years and older. 27
All surgeries were performed by orthopedic surgeons specializing in treating neuromuscular and orthopedic disorders. The surgical indications for hip reconstruction included hip MP greater than 50% in one or both hips, evidence of progressive lateral hip subluxation or dislocation, a windswept pelvis or rotational asymmetry affecting sitting or personal care, or pain. All the patients had prophylactic surgery of the contralateral hip because unilateral hip surgery alters the forces maintaining the pelvic alignment and may destabilize the contralateral hip. Additional hip arthrography was performed to confirm the need for Dega pelvic osteotomy and range of shortening during VDRO.
The caregivers completed an informed consent form, a demographic worksheet, and the CPCHILD questionnaire at the preoperative visit. At 6, 12, and 24 months postoperatively, the caregivers completed the CPCHILD questionnaire again, and the hip joint X-ray was obtained.
The calculations were performed using Statistica software by TIBCO (TIBCO Software Inc., Palo Alto, CA, USA) and PQStat (PQStat Software, Poznań/Plewiska, Poland). A significance level of α = 0.05 was adopted. The results were considered significant when p < α. The normality of the variable distribution was verified using the Shapiro–Wilk test. To examine changes over time, the Student’s t-test for paired samples was employed for normal distribution, and the Wilcoxon test was used in all other cases. For categorical variables, the McNemar test (for dichotomous variables) or the Bowker–McNamara test was applied (for more than two categories).
Results
In this study, we evaluated a group of 31 nonambulatory patients consisting of 15 girls and 16 boys with spastic quadriplegia. Nine patients were at GMFCS IV functional level, while the rest were at level V. The patient age at the surgery ranged from 4 to 17 years, and their mean age was 9 years and 4 months. We performed 62 hip reconstructive surgeries. Four patients did not have the Dega osteotomy on the other side, and this decision was based on hip arthrography. During the 2-year follow-up, none of the patients underwent surgery due to scoliosis. The results below contain summary clinical data on the operated hip joints. Table 1 presents the demographic and clinical characteristics of the patients.
Demographic and clinical characteristics of patients (N = 31).
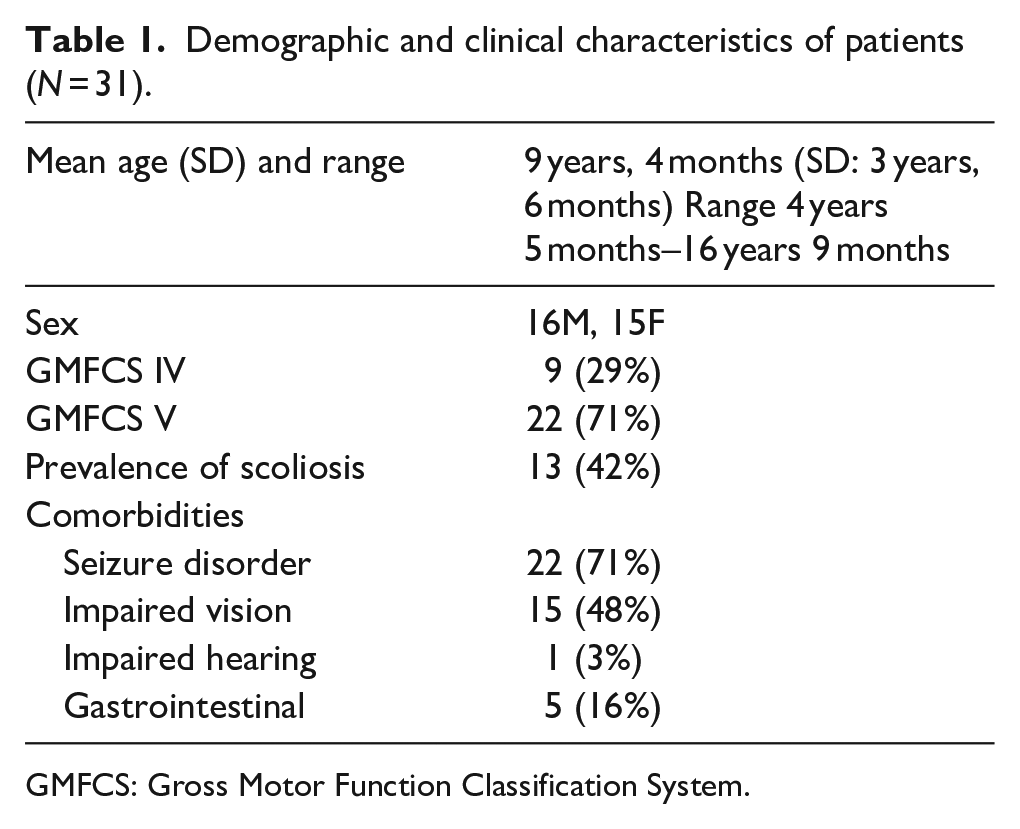
GMFCS: Gross Motor Function Classification System.
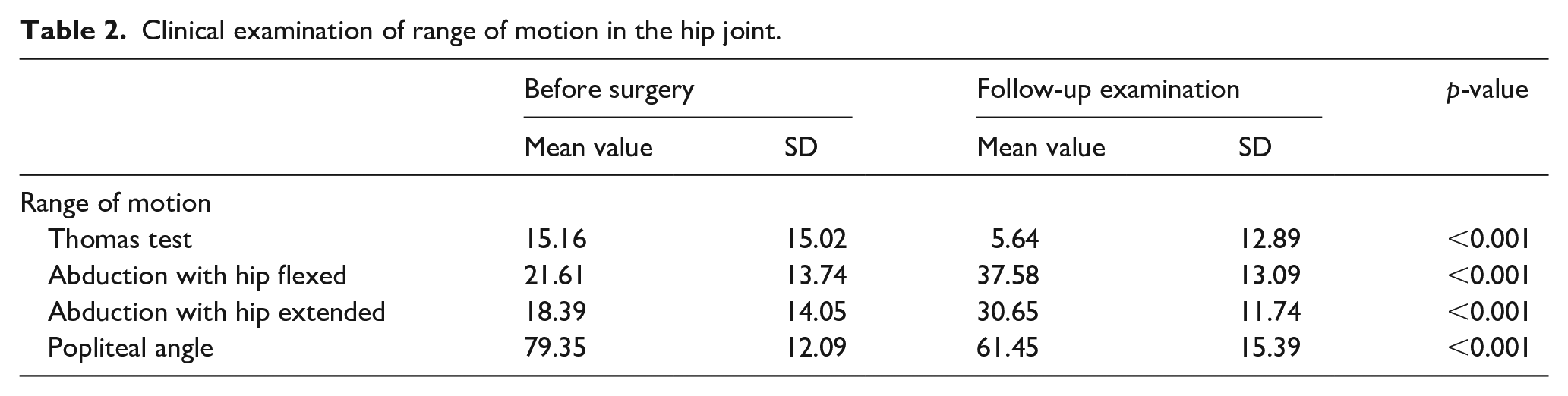
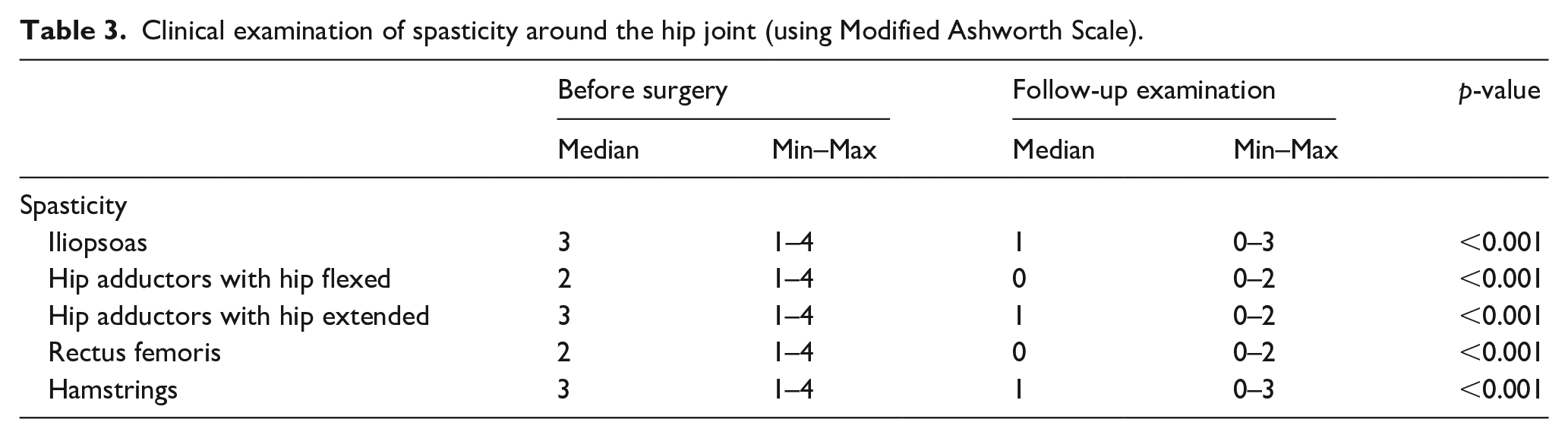
A clinical examination on the follow-up visit confirmed significant improvements in the hip joint ROM (the Thomas test, hip abduction, and popliteal angle) and reduction of spasticity. The clinical examinations are listed in Tables 2 and 3. We achieved significant improvement in the femoral head coverage, as measured by a reduction of MP from a mean of 69.5% (SD, 35.6%) to 11.7% (SD, 16.1%) (p < 0.01). In our cohort, 16 patients had windswept hips at the baseline, and 13 patients had windswept hips at the last follow-up visit. As mentioned before, soft-tissue release was performed as simultaneous surgery in the case of the windswept pelvis before the hip reconstructive surgery.
Clinical examination of range of motion in the hip joint.
Clinical examination of spasticity around the hip joint (using Modified Ashworth Scale).
The assessment of symptoms and problems associated with the hip revealed positive effects of the surgery on pain, contractures, and specific caregiving difficulties (toileting/perineal hygiene, dressing, seating, transferring, and position changes). The caregivers were interviewed regarding these issues during the clinic assessment before the surgery and at the follow-up visit (Table 4).
Symptoms and problems associated with the hip (using CPCHILD questionnaire).
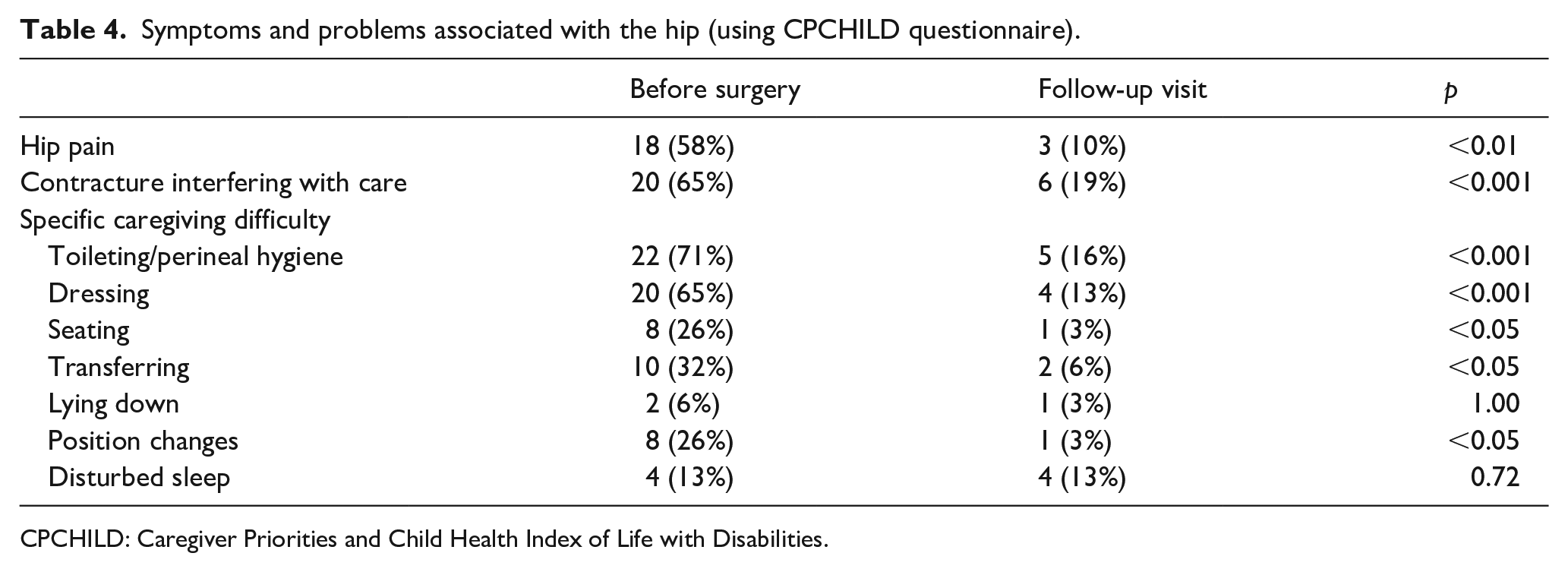
CPCHILD: Caregiver Priorities and Child Health Index of Life with Disabilities.
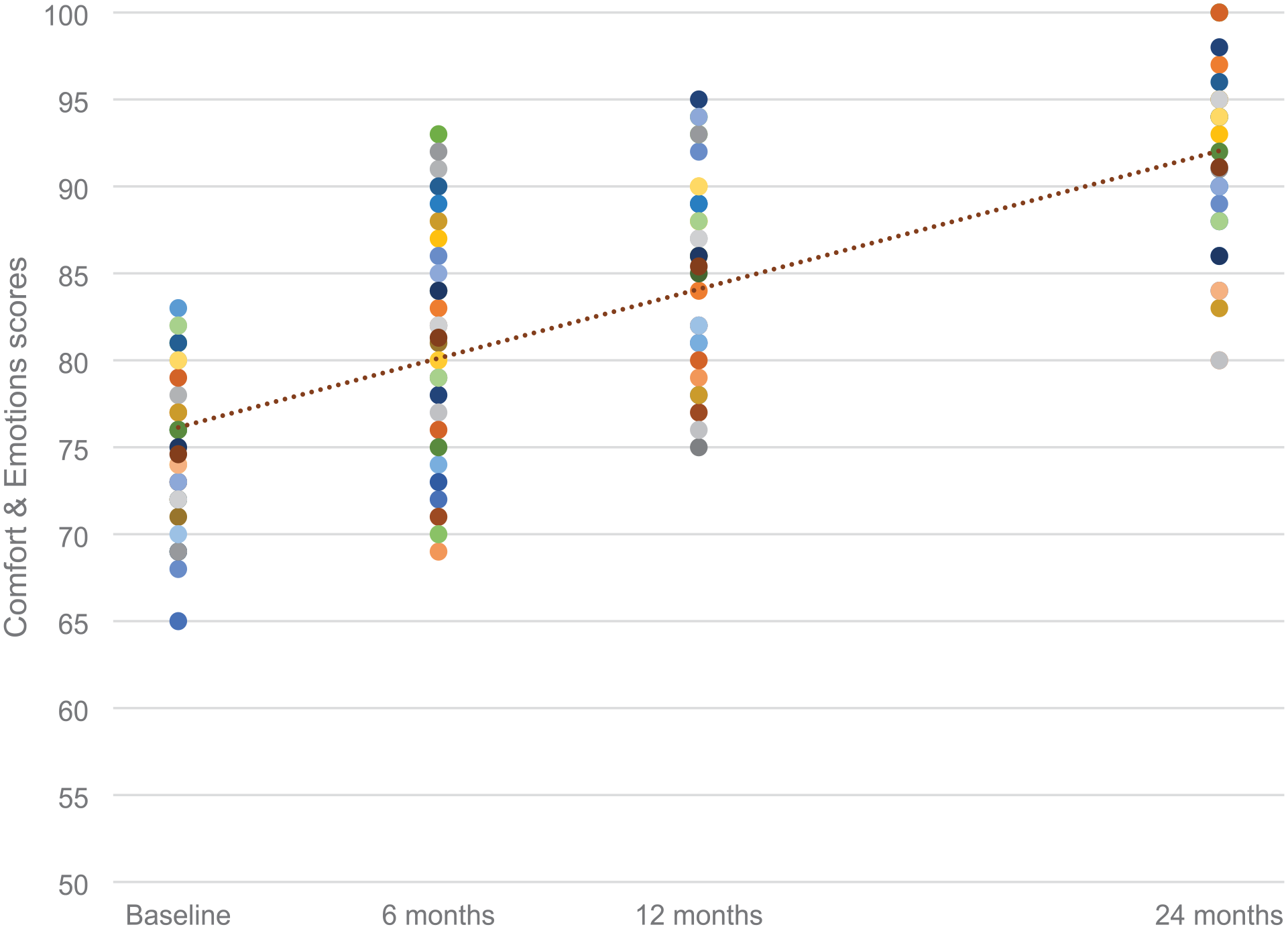
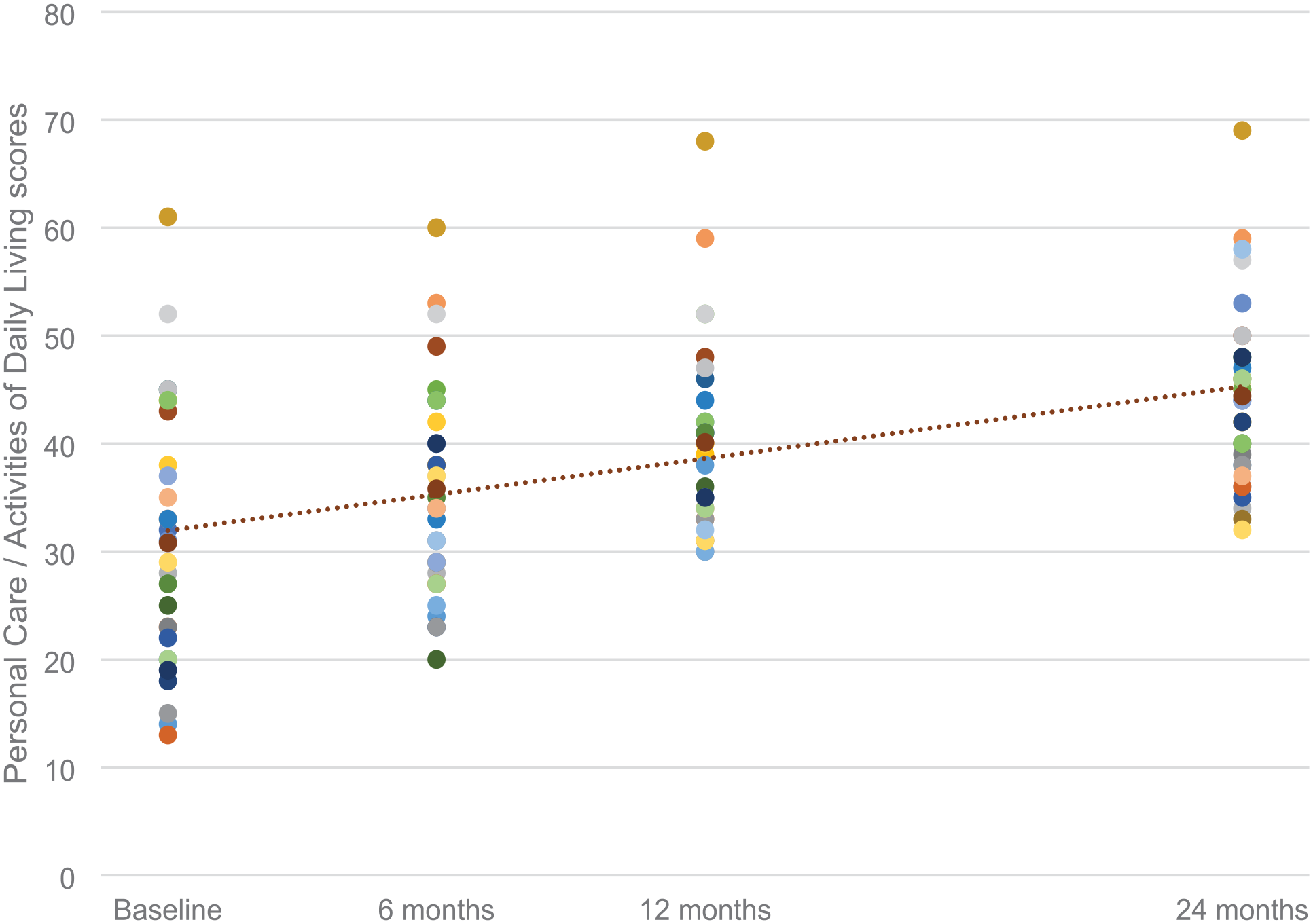
The patient’s caregivers reported satisfaction with the surgical treatment outcomes by filling out the CPCHILD questionnaire. Statistical analysis of the questionnaires revealed several interesting relationships. The mean standardized CPCHILD total score was 55.63 (SD, 14.84), ranging from 13.93 to 82.82. The mean CPCHILD score for the entire group increased significantly from baseline to 24 months postoperatively (p < 0.01) independently of sex (p = 0.62) and GMFCS (p = 0.53). Figure 1 shows CPCHILD score changes at the follow-up visits. The mean improvement at the follow-up visit was 9.3 points (95% CI, 3.8–14.7). Significant amelioration was noted from baseline to the follow-up visit in all domains of the CPCHILD questionnaire except for communication and social interaction. Mean improvements were the most significant for personal care and activities of daily living. Figure 2 presents changes in the CPCHILD questionnaire domains and total scores before the surgery and at the follow-up visits. Seizure disorders and impaired vision did not affect changes in the CPCHILD questionnaire domains and total scores (p > 0.05). There were no statistically significant differences in baseline and follow-up CPCHILD total scores between patients with or without scoliosis (p > 0.05). Figures 3 and 4 present personal care/activities of daily living and comfort & emotions scores distribution and general improvement throughout treatment in these parts of the CPCHILD questionnaire. The trend line shows the average for each questionnaire item.
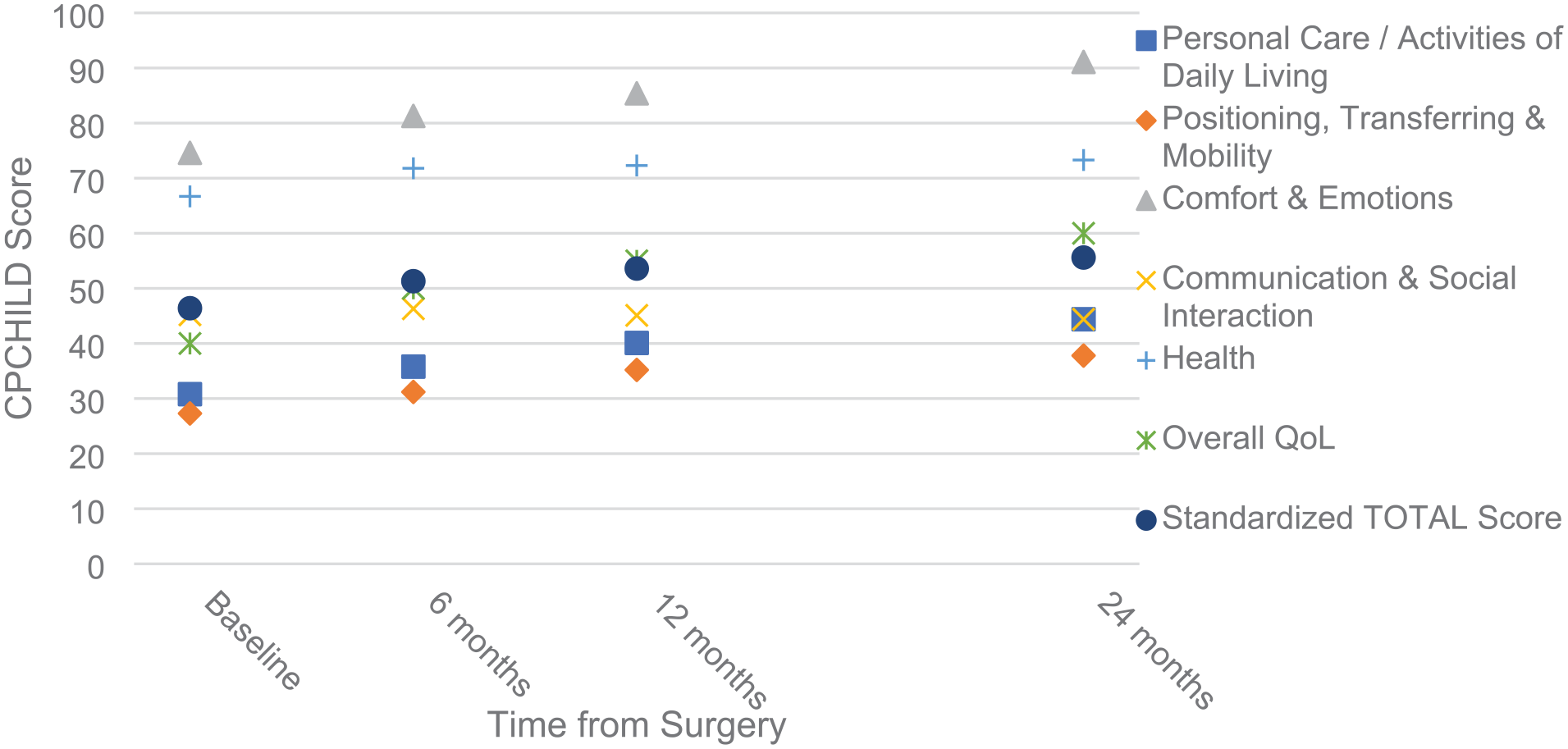
Change in CPCHILD total and domain scores over time.
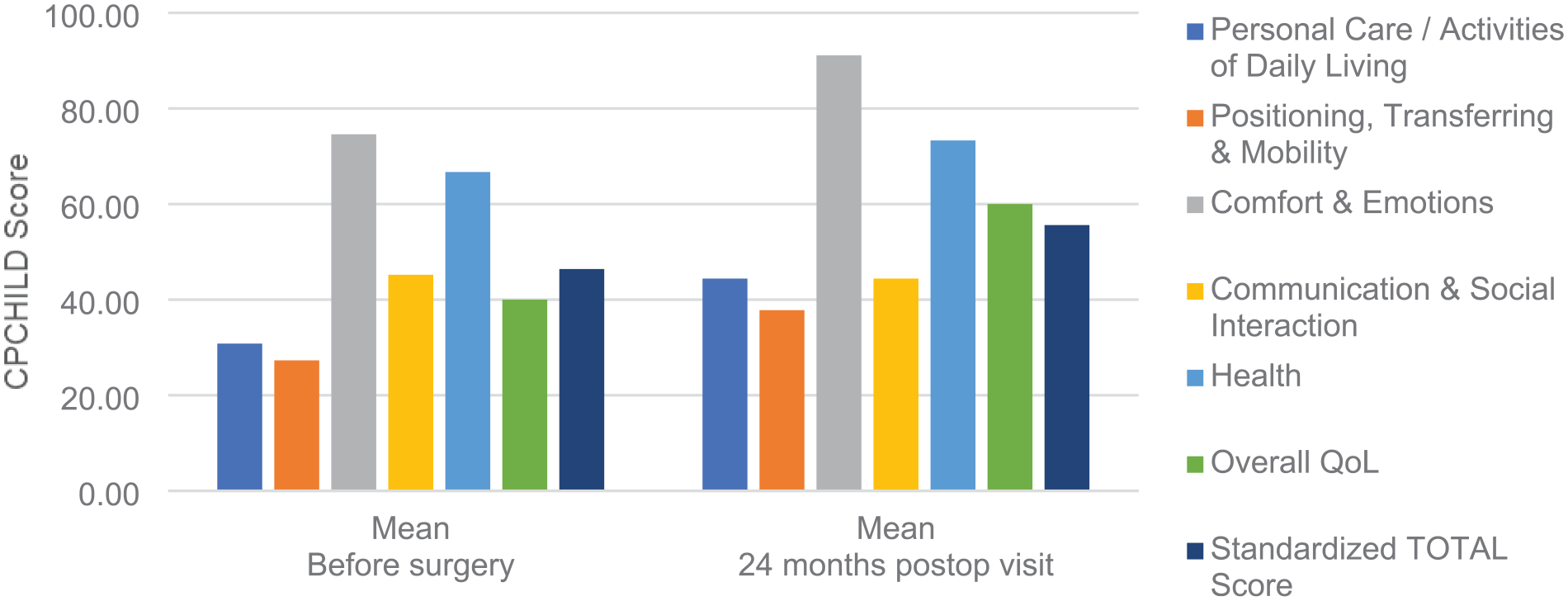
Comparison of CPCHILD domains and total scores before surgery and 2 years after surgery.
Personal care/activities of daily living scores throughout treatment.
Comfort & emotions scores throughout treatment.
Discussion
HRQL is an essential aspect of life that contributes to the perception of well-being and the ability to participate in life roles. 14 Pain and motor impairments influence HRQL in patients with CP and hip displacement.15,28 The CPCHILD questionnaire has been developed and validated for CP children severely impaired according to the GMFCS to evaluate their HRQL. 16 It comprises seven sections, including daily life activities, transfer and mobility, comfort, communication, and social interaction, as well as general health status and overall QL.
As reported by Jung et al., 29 hip lateralization is associated with lower HRQL. That study indicated a positive correlation between higher MP and lower CPCHILD scores. This association remained significant even after adjusting for GMFCS. The association between hip displacement and HRQL was mainly affected by the subdomains of communication and social interaction, and overall health status. It should be noted that the health status subdomain addresses hospital admissions and drug intake, rather than actual comorbidities, such as seizure disorders and impaired vision. Communication and social interaction refer to verbal communication and a child’s ability to participate in social interaction. As social interaction in children relates to individual mobility, this association seems reliable. 30 In addition, the hip status of children with CP has been linked to the rating of general health by the CPCHILD questionnaire. Caregivers reported greater hip mobility and personal care scores, which correlated with the comfort and health of the children. 30
Elema et al. 28 claimed that pain and hospital admissions before the assessment are the most critical factors associated with poorer HRQL scores. Neurogenic dislocation of the hip joint resulting from SHD causes pain and development of neurogenic scoliosis, significantly impeding patient care and increasing the intake of analgesics and the number of hospital admissions. Many authors consider these complications the most significant indications guiding their therapeutic decisions.31 –34 Hip displacement was associated with lower CPCHILD scores, especially on comfort, emotions, and health. 35
An inherent issue of SHD is the frequency of pain. According to the literature, in patients with CP, it ranges from 25% to 77%. The risk of pain occurrence is the most critical factor affecting the decisions concerning surgery.35,36 Pain is associated with poor sleep and lower involvement in the activities of daily living, and it is a predictor of restricted social participation and lower QL later in life.37,38 In this article, we assessed chronic secondary musculoskeletal pain according to Cerebral Palsy Pain Classification (CPPC) 36 by analyzing results from the CPCHILD questionnaire sections: “Symptoms and problems associated with the hip” and “Comfort & emotions.”
Moreover, Krebs et al. 39 showed that the most remarkable improvement following surgical treatment is observed in patients experiencing pain. Historically, surgical outcome assessment has focused on objectively documenting the correction of structural deformity and improving physical activity. More recently, the patient point of view has been recognized as fundamental to monitoring the quality of surgical outcomes.
The modern concept of SHD treatment is based on the proactive approach presented by many authors,8,17,31 who indicate the need for surgery before a complete dislocation occurs. Proactive treatment results in less invasive procedures, and there is strong evidence that the benefits outweigh the harms in the population of children with CP. The need to operate on the contralateral hip by performing VDRO is widely emphasized in the literature as the main element preventing further hip dislocation and pelvic obliquity.40,41
Our study has several important strengths, including its focus on patients with severe CP, homogeneity of the group, its uniform approach to reconstructive surgery and postoperative care, and the use of a standardized and well-validated instrument for evaluating HRQL in children with CP. 16 This questionnaire objectively measures HRQL as a crucial aspect of the treatment outcomes.
Difazio et al. also assessed the HRQL in patients after a reconstructive hip surgery but their study group was less homogeneous due to the extent of the surgical procedures.42,43
The limitations of our study include its single-center nature and a lack of a control group of non-operated patients. However, untreated hip dislocation-associated problems in patients with CP were described by Knapp and Samilson et al.31,44 According to our institutional standards, all eligible patients were offered surgery.
Our study demonstrated that hip reconstruction with VDRO and Dega pelvic osteotomy improves the HRQL of children with CP (GMFCS levels IV–V, spastic or mixed type of CP). HRQL is significantly lowered in children with hip dislocation, mainly due to functional limitations and pain.35,39 In this situation, surgical treatment of the hip improves the structural damage and QL. In the authors’ opinion, the decrease in popliteal angle and rectus spasticity is due to the shortening of the femoral bone during osteotomy and correction of pelvis position after surgery. Our study suggests that healthcare providers can use these findings to inform patient education, set realistic expectations, and increase family participation in surgical decision-making. Geyer et al. 45 identified three preoperative caregiver expectations, which include improved functionality, comfort, maintaining health, and averting crisis. Orthopedic surgeons are now required to demonstrate functional improvements following their surgical interventions, especially in this era of healthcare reforms. However, reconstructive hip surgery in nonambulatory children with CP can be a costly and emotionally challenging decision for their families. Our results show that reconstructive hip surgery improves HRQL in these patients, which can guide healthcare professionals in their decision-making process.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521241300880 – Supplemental material for Health-related quality of life after Dega pelvic osteotomy and varus derotation osteotomy due to spastic hip disease in children with cerebral palsy
Supplemental material, sj-pdf-1-cho-10.1177_18632521241300880 for Health-related quality of life after Dega pelvic osteotomy and varus derotation osteotomy due to spastic hip disease in children with cerebral palsy by Maciej Kasprzyk, Aleksander Koch and Marek Jóźwiak in Journal of Children’s Orthopaedics
Footnotes
Author contributions
Maciej Kasprzyk was responsible for conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, visualization, writing – original draft. Aleksander Koch was responsible for conceptualization, investigation, methodology, resources, visualization, writing – review & editing. Marek Jóźwiak was responsible for conceptualization, funding acquisition, investigation, project administration, supervision, validation, writing – review & editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The Medical Ethics Committee of the Poznan University of Medical Sciences approved this research (UMP 266/15).
Informed consent
All patients and legally authorized representatives of the patients provided informed written consent prior to the analysis.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.