
Abstract
Purpose:
The acetabulum interacts with the femoral head in daily activities and may exhibit structural changes in the presence of hip disorders. This study aims to redefine hip disorders in children with cerebral palsy by structural characteristics of the acetabulum in relation to the degree of the migration percentage.
Methods:
The clinical and radiographic data of 70 patients (36 males, 34 females; mean age 8.2 years) with spastic cerebral palsy were retrospectively analyzed. The acetabular structure was measured by the acetabular index on reconstructed three-dimensional computerized tomography for precision of measurement. Any significant change in acetabular index measured on the reconstructive computerized tomography related to every 10% increment of migration percentage was regarded as clinically significant in hip disorders.
Results:
The acetabular index measured on the reconstructive computerized tomography showed an increasing trend with the increment of migration percentage. The most significant acetabular index measured on the reconstructive computerized tomography change occurred between the 20%–29% and 30%–39% migration percentage groups (p < 0.001), suggesting that a migration percentage of 30% is the starting point of hip disorder. A significant increase in the posterolateral acetabular index measured on the reconstructive computerized tomography occurred in migration percentages >50%, indicating posterolateral acetabular dysplasia. Hips with migration percentages from 80% to 100% had consistent acetabular indexes measured on the reconstructive computerized tomography values, suggesting complete dislocation and no more contact and interaction between the femoral head and acetabular fossa.
Conclusion:
Structural characteristics in the acetabulum reflect hip dysfunction and potentially classify hip disorders. Results suggest the migration percentage 30% as a starting point of hip disorder and 80% as a turning point of hip dislocation in children with cerebral palsy.
Level of evidence:
level IV, diagnostic study.
Keywords
Introduction
Hip displacement is a common musculoskeletal disorder that may result in pain and diminished function in patients with cerebral palsy (CP). Surveillance programs for hip displacement have been recommended to address the disorder at an early stage.1 –3 The Reimers’ migration percentage (MP) 4 is the most common surveillance tool. However, definition of hip disorders in patients with CP is variable. Reimers 4 classified hip subluxation as MP at 33% or more and hip dislocation as MP at 100%. Miller and Bagg 5 classified hip conditions as normal (MP <30%), subluxated (MP 30%–59%), severely subluxated (MP 60%–89%), and dislocated (MP ≥90%). Graham et al. 6 classified the hips at risk as MP >10% but <40%. With these different points of view, it is necessary that the definition of hip disorders requires anatomical validation.
Hip development is modeled by the contact force between the acetabulum and the femoral head.7 –9 The structural characteristics in the acetabulum may be representative of the cumulated effects of hip motion in daily activities and potentially indicate disorders in hip development. As the Graf 10 method in infant hip ultrasounds uses the alpha angle of the acetabular roof to classify hip dysplasia, static measurements of structural characteristics in the acetabular fossa may be a reliable indicator for hip disorders in children with CP. Besides, measurement of the acetabulum in classifying hip disorders avoids bias from leg malposition due to inconsistency of position while taking radiographic image in children with CP owing to irritability and spasticity.
The technique of three-dimensional (3D) reconstruction of computerized tomography (CT) images allows orthopedic doctors to realign the pelvis and properly measure the detailed morphology of the acetabulum.11 –14 This study aims to explore structural characteristics of the acetabulum in relation to degree of the MP and to redefine hip disorders with reference to acetabular dysplasia.
Methods
Study design
This was a retrospective analysis of the radiographic data of patients with spastic CP. The study was approved by the Institutional Review Board. The relationship between acetabular dysplasia measured by the acetabular index (AI) on 3D-CT and hip displacement measured by the MP on anteroposterior pelvis plain radiography was analyzed.
Participants
Data of spastic CP children with plain radiographs and CT of the pelvis before undergoing orthopedic surgery for hip displacement at a tertiary medical center from 2004 to 2019 were reviewed. The inclusion criteria were individuals with: (1) a diagnosis of spastic CP; (2) gross motor function classification system (GMFCS) levels II to V; and (3) age between 4 and 13 years to ensure adequate ossification of the acetabulum with open triradiate cartilage.
Radiographic measurements
The MP was measured on the plain anteroposterior radiographs of the pelvis. The MP represented the portion of the ossified femoral epiphysis that had migrated laterally beyond Perkin’s line divided by the width of the femoral epiphysis.15 –17 The Perkin’s line was defined by the most lateral part of the acetabular sourcil.
The AI on anteroposterior pelvic radiographs is a well-established and reliable measurement of acetabular development in children. 18 To resolve the confounding effects from malpositioning of the pelvis, the 3D-CT model of the pelvis was reconstructed from 0.5 mm slice thickness images. The pelvis was realigned on the frontal and horizontal planes by the Hilgenreiner’s line between two inferior pores of the bilateral ilea (Figure 1(a) and (b)). 14 On the sagittal plane, the pelvis was realigned by a vertical position of the triradiate cartilage between the ischium and pubis (Figure 1(c)). Thereafter, the pelvis was rotated along the Hilgenreiner’s line, from 60° anteriorly to 60° posteriorly, so as to acquire acetabular sectional planes in nine directions: anterior 60° (A60), anterior 45° (A45), anterior 30° (A30), anterior 15° (A15), neutral 0° (0), posterior 15° (P15), posterior 30° (P30), posterior 45° (P45), and posterior 60° (P60) (Figure 2). By doing so, the geometry of the acetabular roof could be defined in these directional planes using acetabular indexes measured on the reconstructive computerized tomography (CT-AIs) (Figure 3).
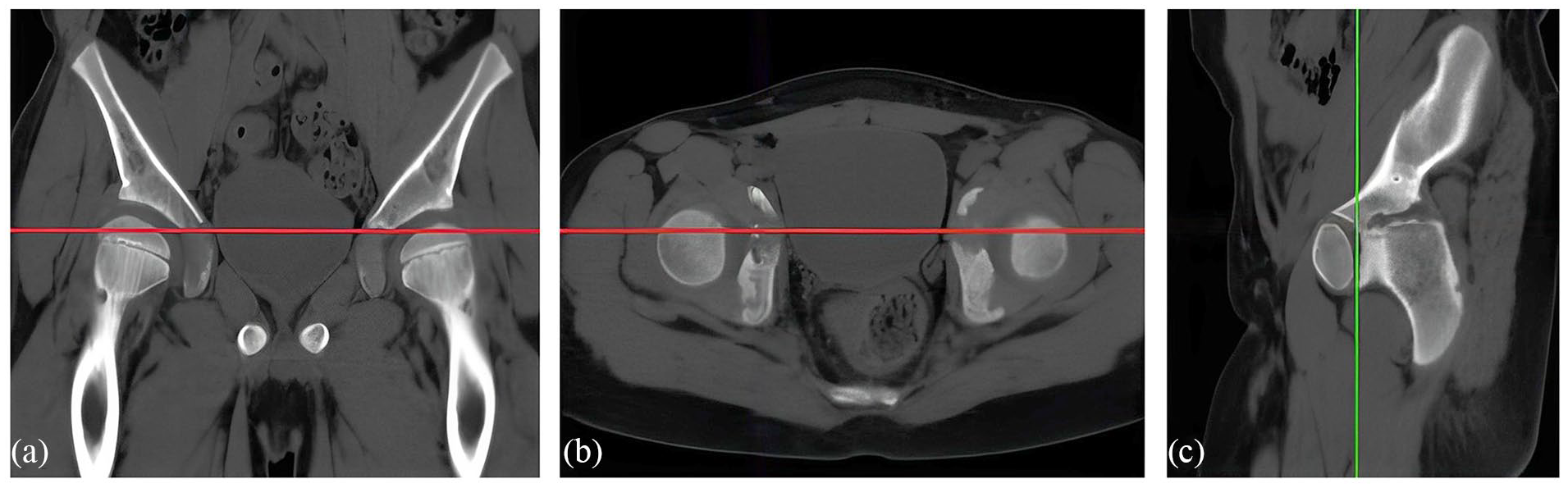
The pelvis is realigned by the Hilgenreiner line (red line) on the coronal plane (a) and the horizontal plane (b). On the sagittal plane (c), the inclination of the pelvis is calibrated by the inferior limb of the triradiate cartilage (green line).
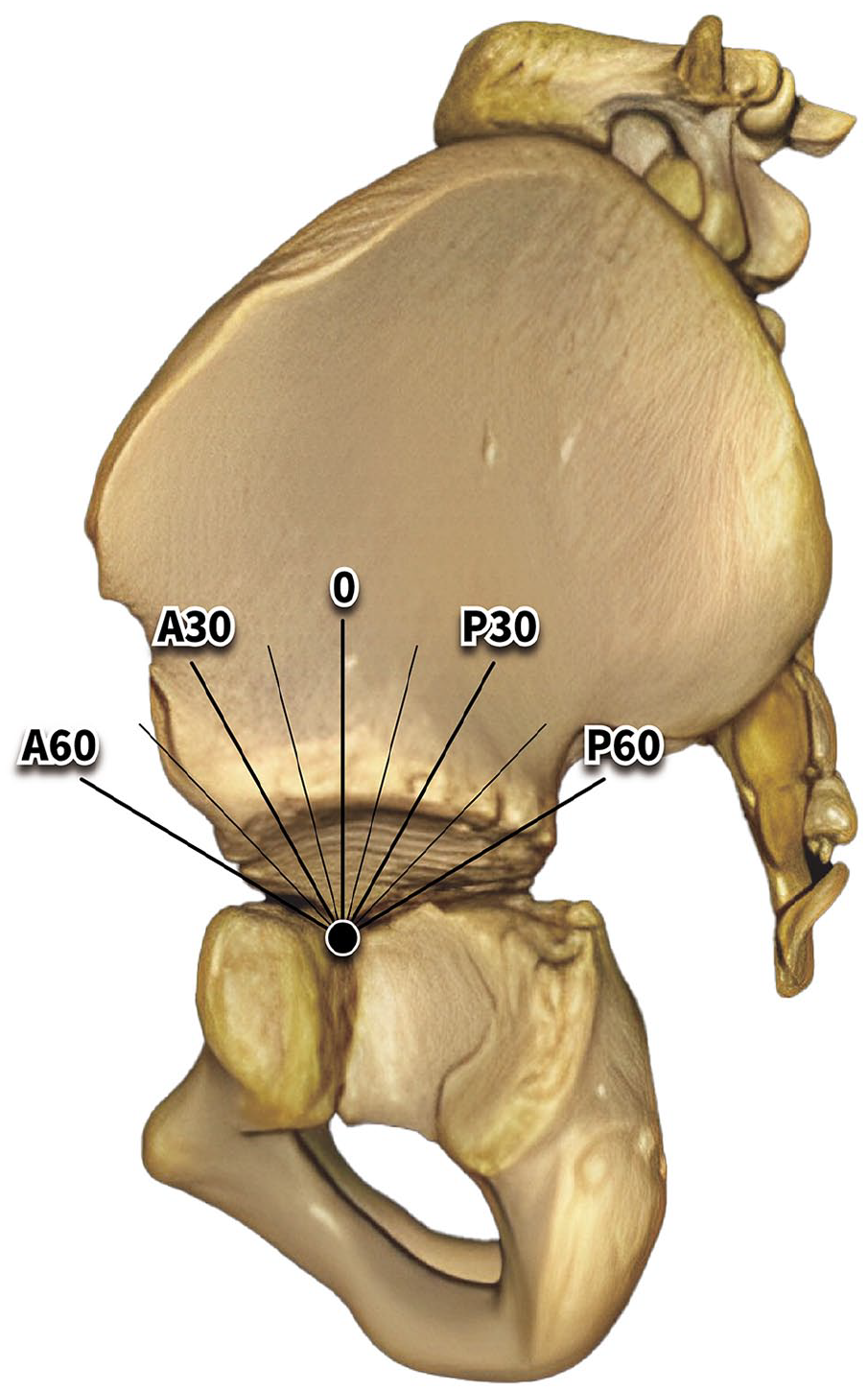
Nine sectional planes from anterior 60 degrees (A60) to posterior 60 degrees (P60) to assess the acetabular index on different directions. The 0 plane is aligned with the inferior limb of the triradiate cartilage.
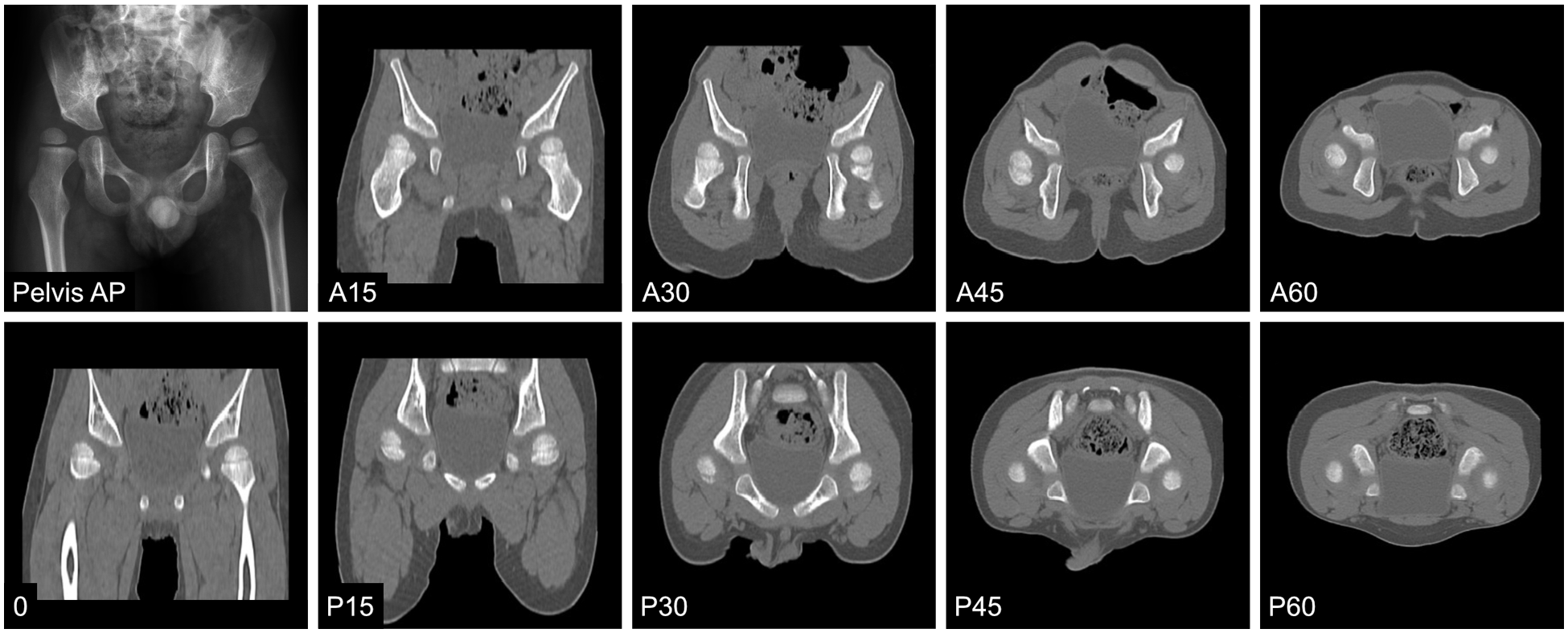
A 4.2-year-old boy with right hip displacement and a migration percentage of 76%. Right acetabular dysplasia at superior-lateral and posterosuperior aspects was revealed by reconstructed computerized tomography.
The reliability of this method has been validated using 16 hip images from eight children with CP. 14 Measurements of the CT-AIs on each plane were taken by two orthopedic doctors independently. The measurement had an excellent intra-rater reliability score (correlation coefficient = 0.924) and a good inter-rater reliability score (correlation coefficient = 0.887).
Data processing
To show the acetabular dysplasia in relation to the different degrees of MP, hips were divided into eight MP ranges: 0%–19%, 20%–29%, 30%–39%, 40%–49%, 50%–59%, 60%–79%, 80%–99%, and ≥100%. The mean values of the CT-AI in each directional planes were stratified to different MP groups. Since CT scans were not performed on patients without hip displacement, the data of MPs <30% (in the 0%–19% and 20%–29% groups) were acquired from the non-displaced hip of included patients with unilateral hip displacement. For comparison with the hips in typically developing children, CT scan images from eight age-matched children (male, n = 4; female, n = 4; mean age = 7.6 years; range: 6.2–9.6 years) without a history of any hip disorder were retrieved from the radiology department database as normal controls.
Statistical analysis
The Shapiro–Wilk test was used to check the normality of the MP and CT-AI data in each group. Then, an independent t-test or Mann–Whitney U test was used to assess differences of the CT-AI in two adjacent MP groups. Significant morphological changes between two adjacent MP groups indicate apparent events happened in the acetabular fossa, such as hip displacement and hip dislocation. A paired t-test or Wilcoxon rank sum test was used to compare the AI on pelvis radiography to the CT-AIs in the nine directions from the same individual to determine pelvic orientation. The hip CT-AIs with MPs <30% in children with CP were compared with those of typically developed children using the independent t-test to determine whether acetabular dysplasia exists in non-displaced hips. Statistical significance was set at p < 0.05. All analyses were performed using SPSS software version 20.0 (IBM Inc., Armonk, NY, USA).
Results
Data from 70 children with spastic CP (male, n = 36; female, n = 34; mean age 8.2 years; range: 4.2–13.9 years) who underwent pelvis CT as a part of preoperative evaluation from 2004 to 2019 were included in this study. Among the 70 children, 23 had bilateral displaced hips, and 47 had unilateral displaced hips. The number of children in each GMFCS level was 10, 12, 13, and 35 in levels II, III, IV, and V, respectively. Two children with hemiplegia were classified as GMFCS level II, and 68 had diplegia or quadriplegia. Sixty-four children exhibited the typical spastic type, while six children had a combination of spasticity and dyskinesia. Specifically, two children had dystonia, and four children had athetoid movements.
Among 140 hip MPs from the 70 patients, 11 were <20%, 36 were between 20% and 29%, 22 were between 30% and 39%, 16 were between 40% and 49%, 16 were between 50% and 59%, 19 were between 60% and 79%, 13 were between 80% and 99%, and 7 were ≥100%. When CT-AIs in all nine directions were stratified by MPs, the CT-AIs showed progressive acetabular dysplasia with increases in MP (Table 1). All the data were normally distributed. The CT-AI values on the A15 plane and 0 plane were comparable with the AI measured on anteroposterior radiograph of the pelvis (paired t-test, p > 0.05). The acetabular roof shown on supine anteroposterior radiograph of the pelvis was close to the area between the A15 and 0 planes relative to the inferior limb of the triradiate cartilage.
The mean values and (standard deviation) of acetabular index on the nine directional planes in hips with different migration percentages.
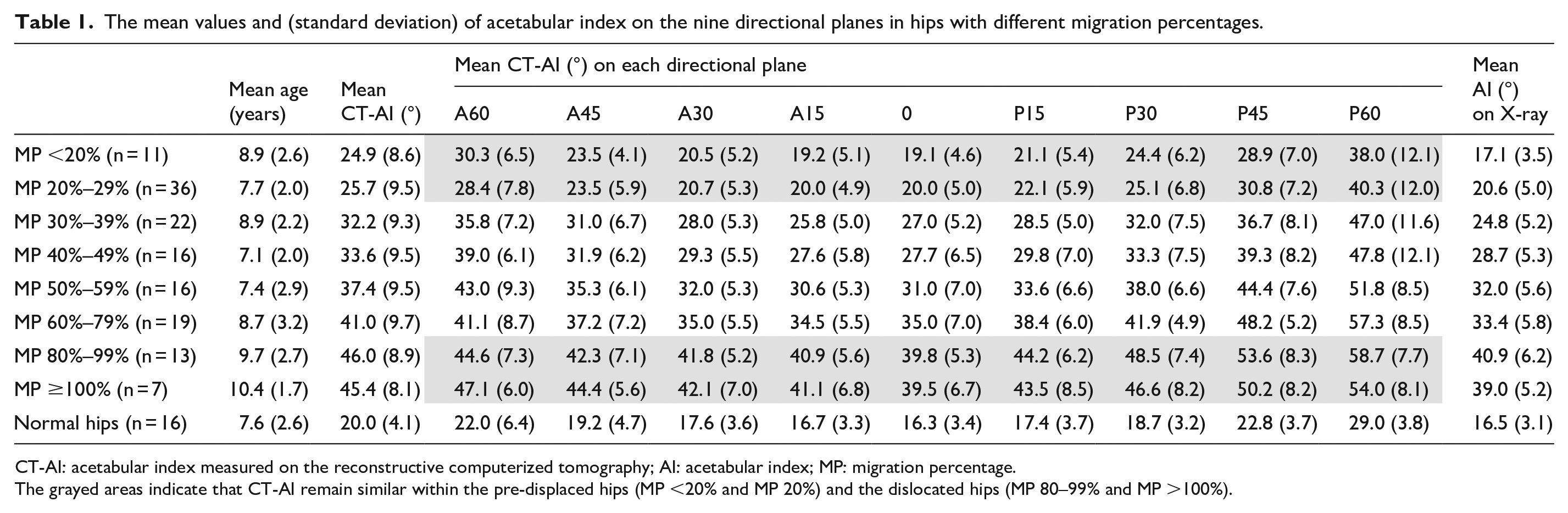
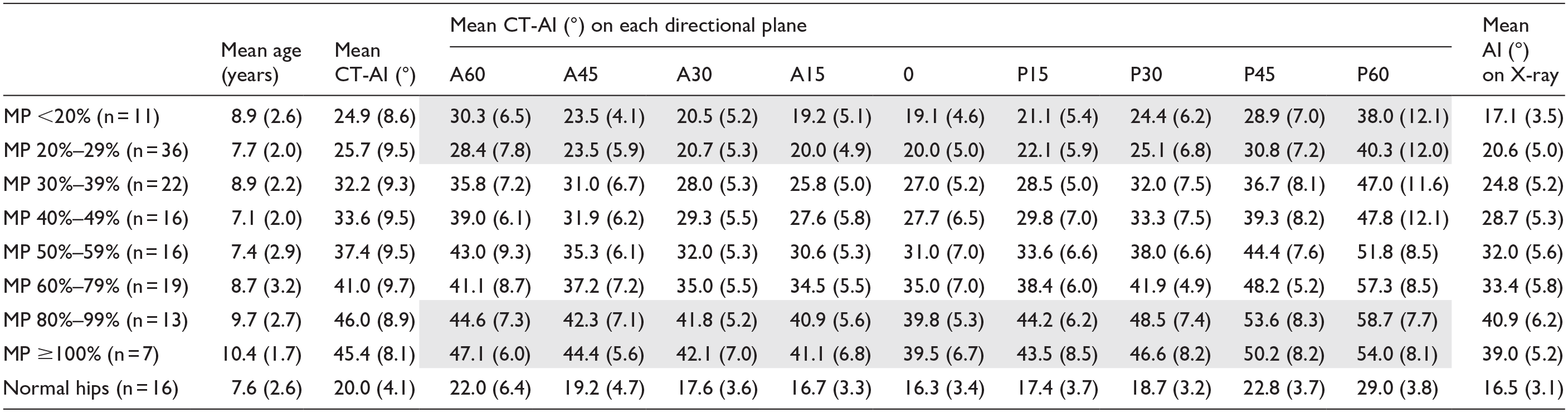
CT-AI: acetabular index measured on the reconstructive computerized tomography; AI: acetabular index; MP: migration percentage.
The grayed areas indicate that CT-AI remain similar within the pre-displaced hips (MP <20% and MP 20%) and the dislocated hips (MP 80–99% and MP >100%).
Acetabular dysplasia in different hip displacement levels
A global dysplasia involving the nine directions was noted in children with CP. Even in hips with an MP <20%, the CT-AIs of children with CP were significantly greater than those of typically developed children (independent t-test, p < 0.001; Table 1). The difference in CT-AIs between two adjacent MP groups is shown in Table 2 to demonstrate the morphological changes related to MP increment. The most significant change occurred between the hips with an MP 20%–29% and the hips with an MP 30%–39% (independent t-test, p < 0.001), indicating a significant structural alternation of the acetabulum when the MP progresses from <30% to >30%. A progressive worsening of acetabular dysplasia was evident from MPs of 40%–80%, especially in the posterolateral aspects of the hips with an MP >50% (Table 2).
The difference of computed tomography acetabular index (CT-AI) between two adjacent groups of hips stratified by migration percentage.
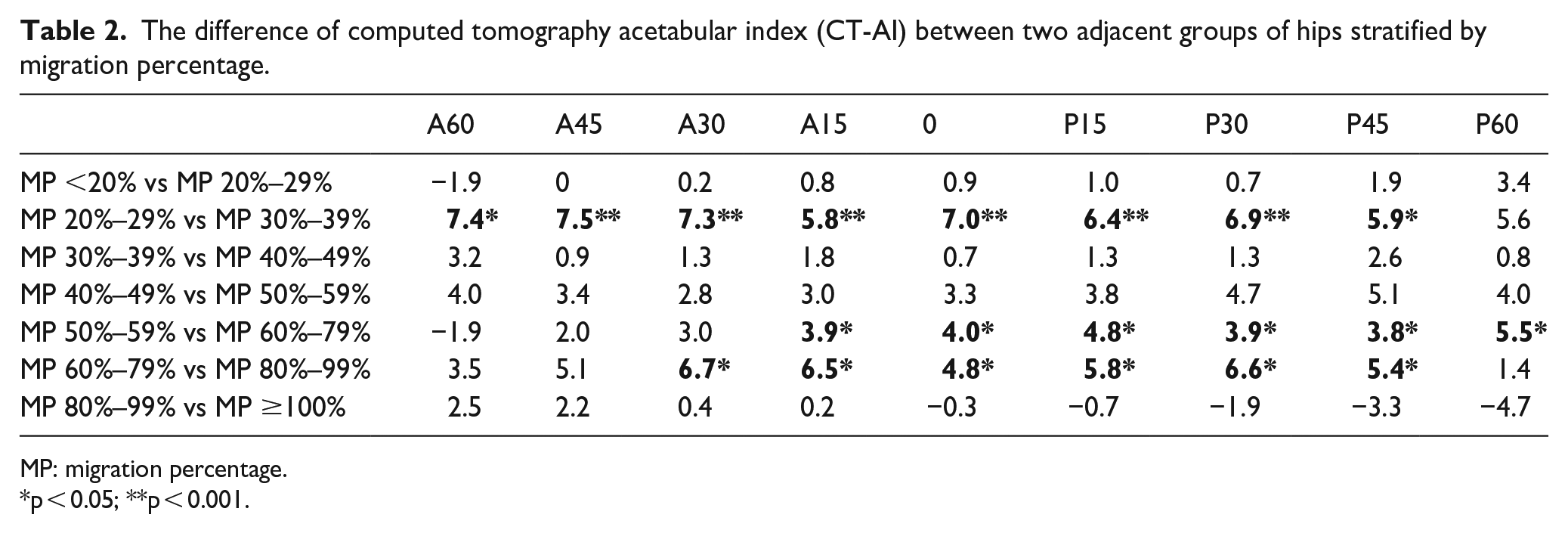
MP: migration percentage.
p < 0.05; **p < 0.001.
Definition of hip disorders by acetabular dysplasia
Two MP categories had consistent CT-AIs, the MP ≤29% and those with an MP ≥80% (grayed areas in Table 1). Consistent CT-AIs in hips with MPs <20% and 20%–29% suggest a stationary pre-displaced condition. Similarly, constant CT-AIs in hips with MPs >80% (MP groups: 80%–99% and ≥100%) suggest the femoral head may have dislocated outside the fossa, thus having no more effects on the acetabular structure.
Discussion
The structural characteristics of the acetabular fossa may record how the femur interacts with the pelvis and reveal pathogenetic processes of spastic hip displacement. The acetabular dysplasia revealed by 3D-CT in this study supports the definition of hip displacement as an MP >30% and dislocation as an MP >80%. The observed progressive acetabular dysplasia related to increasing hip displacement confirms the need for hip surveillance and treatments to prevent advanced acetabular dysplasia in CP children.
Definition of hip displacement
Surveillance studies on spastic hip displacement have mainly been conducted according to Reimers’ MP.19 –21 Reimers 4 classified hip subluxation as an MP of 33% or more. Sharrard et al. 22 proposed the concept of “hip at risk” for hips with an MP of 33%–40%, and hips with an MP of ≥40% had a greater risk of progression. In this study, data were stratified by 10% increments of MP, and the significant increase in acetabular dysplasia between MP of <30% and ≥30% supports the use of MP 30% as a turning point for detecting hip disorders in children with CP. The results were comparable to Reimer’s definition of 33% as hip subluxation. Regarding the risks of progression in hip displacement, our data were in line with findings from Sharrard’s study that showed that a significant and continuous increase in CT-AIs occurs when the MP is between 40% and 80%.
Definition of hip dislocation
Reimers 4 classified hip dislocation as an MP of 100%, whereas Miller and Bagg 5 classified hip dislocation as an MP ≥90%. This study showed a continuous and remarkable increase of CT-AIs from MP 30%–80%, and the increase of CT-AIs was no longer significant after MP >80%. These findings suggest that the acetabulum continues changing the shape when the femoral head gradually displaces. When MP goes beyond 80%, the femoral head may be situated lateral to the edge of the acetabulum and no longer in contact with the acetabular fossa. Therefore, the progressive worsening of acetabular dysplasia stops after MP >80% in our observation. Currently, there is no clinical evidence to support whether hips with MP >80% have a greater risk of unreducible hips following femoral osteotomy or re-dislocation without acetabuloplasty. This study identified a tiered progression of acetabular dysplasia that suggests stages in the course of hip subluxation to dislocation.
Acetabular dysplasia at MP <30% and >30%
The consistent CT-AI values in MP <20% and 20%–29% supported the hips with an MP <30% as a non-displacement or pre-displacement state. The CT-AIs of the hips with an MP <20% in children with CP were still significantly greater than that in typically developing children. The neurologic disorder and motor dysfunction have affected acetabular development before hip displacement occurs. The hips with acetabular dysplasia are not totally normal and require continuous surveillance for the risks of displacement later.
The study revealed that acetabular dysplasia in hips with MP >30% was significantly worse than in hips with MP <30%. These findings support the importance of surveillance to maintain MP below 30%, which may involve interventions to improve hip joint range of motion and motor functions. Surgical treatments are recommended for hips with MP exceeding 30% to prevent further deterioration of acetabular dysplasia.
Limitations
This study has several limitations. First, the inferior pole of the iliac bone is an anatomical landmark for measuring the Hilgenreiner’s line but not the global center of the acetabular fossa. The Hilgenreiner’s line is anterosuperior to the center of the acetabular fossa (Figure 2). The CT-AIs in the anterior aspect (A60, A45) and posterior aspect (P60, P45) were originally greater than the CT-AIs in the superior aspect (A15, 0, P15). Therefore, to interpret acetabular dysplasia accurately, it is important to compare the data with that of normal hips to determine the location and degree of dysplasia for planning acetabuloplasty. Second, this study compares the progression of MP and CT-AI; however, it does not include motor function-level data and involvement of limbs that play an important role in spastic hip disorders. The distribution of patients among the GMFCS levels was skewed because the CT data were obtained from surgically treated patients. Third, age is an important factor in acetabular development. This study did not stratify age groups for collecting more cases to improve the statistical power. Besides, the CT data used in this study were obtained from patients who underwent hip surgery, resulting in a higher mean age at which hip displacement typically occurs. Fourth, a limitation of cross-sectional studies is the inability to obtain follow-up data to analyze the threshold value of CT-AI in defining rapid MP progression. 23
Conclusion
The acetabular dysplasia supported MP >30% as the definition of hip displacement and MP >80% as hip dislocation in children with CP. The neurogenic acetabular dysplasia in the hips with MP <30% suggests a state that requires continuous surveillance for the risks of displacement later. Treatments for hip with an MP >30% are recommended to prevent advanced acetabular dysplasia that is related to increasing femoral head displacement.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521231185294 – Supplemental material for Definition of hip displacement and dislocation by acetabular dysplasia in children with cerebral palsy
Supplemental material, sj-pdf-1-cho-10.1177_18632521231185294 for Definition of hip displacement and dislocation by acetabular dysplasia in children with cerebral palsy by Nai Kuang Wang, Shih Hsien Shen, Brian Po Jung Chen, Chia Hsieh Chang and Ken N Kuo in Journal of Children’s Orthopaedics
Footnotes
Authors’ Note
This study is conducted in the Department of Pediatric Orthopedics, Bone and Joint Research Center, Chang Gung Memorial Hospital, Taoyuan, Taiwan.
Author contributions
N.K.W. contributed to the conceptualization, data curation, formal analysis, and writing—original draft. S.H.S. contributed to the conceptualization, data curation, supervision, writing— original draft. B.P.J.C. contributed to the formal analysis, writing—original draft, writing—review and editing. C.H.C. contributed to the conceptualization, methodology, formal analysis, supervision, writing—original draft, writing—review and editing. K.N.K. contributed to the conceptualization, methodology, formal analysis, supervision, and writing—review and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical standard
The approval for this study was given by the Institutional Review Board of Chang Gung Medical Foundation (CGMF IRB no.: 99-0627B).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Patient consent was not required due to the retrospective nature of the research.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.