
Abstract
Introduction:
Preventative foot self-care is vital for avoiding diabetic foot ulcer episodes and lowering the risk of amputations. Yet, it demands high levels of health literacy and cognitive function.
Objective:
To investigate health literacy and cognitive function in persons presenting with a diabetic foot ulcer.
Methods:
Participants with type 2 diabetes were recruited from the tertiary foot clinic at Steno Diabetes Center North Denmark. The European Health Literacy Survey Questionnaire and Addenbrooke’s Cognitive Examination were applied. A semi-structured interview guide was developed to evaluate foot self-care knowledge, attitude, and practice. The qualitative data were analyzed with a deductive approach based on a qualitative thematic analysis model. Subsequently, an integrated analysis of the quantitative and qualitative results was conducted.
Results:
The participants (n = 12) had a mean age of 62.6 ± 8.4 years, and 11 were males. The mean diabetes duration was 15.9 ± 8.9 years. Eight participants had a recurrent diabetic foot ulcer. The health literacy level was sufficient in nine participants, and cognitive function was normal in five participants. Three different profiles related to foot self-care (proactive, active, or passive, respectively) were constructed by the final integrated analysis: a proactive profile refers to taking preventative action in concordance with knowledge and attitude, an active profile to taking action in response to a situation, but challenged by conflicting levels of knowledge and attitude, and a passive profile to not taking action.
Conclusion:
The study suggests that people presenting with a diabetic foot ulcer have different foot self-care profiles based on person-specific health literacy, cognitive function, and knowledge, attitude, and practice element characteristics, highlighting the need for individualized education and intervention strategy instead of a one-size-fits-all approach.
Introduction
Diabetes mellitus (DM) is a global health concern, and current estimates report 66 million people with DM in Europe. 1 A major devastating complication of DM is a diabetic foot ulcer (DFU), which may lead to lower limb amputations. 2
Prospective studies have documented that people with a previous DFU are at higher risk of recurrent DFU episodes. 3 DFU recurrence rates are as high as 40% in the first year after healing of a DFU episode. 4 The primary reason for the common recurrence of DFU is that the precipitating factors causing the DFU in the first place, such as peripheral neuropathy, foot deformity, elevated plantar pressures, and poor blood circulation, persist beyond the first DFU episode.5–7 Therefore, preventative foot self-care initiatives are important to prevent primary and subsequent DFU episodes and the risk of lower extremity amputations. 8
However, before foot self-care can become efficient, a person at risk of getting a DFU must comply with the provided information and instructions concerning personal health self-care and DM specifically. Personal responsibility in a DFU self-care context is essential in the preventive strategy. Still, it can sometimes be problematic for people with DM due to inadequate health literacy. In people with long-term DM, the cognitive domains of attention, memory, and information processing speed are most affected.9,10 This may potentially affect the health literacy of people with DM. Health literacy is complex since it depends upon overall literacy levels and is associated with cognitive development.11,12 Previous work within health literacy has shown that people have different approaches to their health, whether proactive, active, or passive.11,12
A Danish study found that individuals with long-term DM find it challenging to understand health information and engage with healthcare professionals. 13 Other studies indicate that the general knowledge about DFU and associated risk factors in general is low among people with DM.14,15 Furthermore, long-term DM is associated with cognitive decline and a higher risk of dementia. 16 Hence, it remains unknown whether difficulties with health literacy and potentially declined cognitive function affect the capability to recall and comply with the foot self-care recommendations among people with a history of DFU or the risk of developing DFU later in life. A combined assessment of the health literacy, cognitive function, KAP (knowledge, attitude, and practice) factors, 17 and exploration of everyday life experiences of persons with DFU may provide insights into needs, barriers, and issues related to foot self-care.
The aim of the present study was to investigate health literacy and cognitive function in Danish people with active DFU in relation to foot self-care KAP.
Methods
Participants
Study participants were recruited from October 1, 2021 until February 7, 2022 from the tertiary Diabetes Foot Clinic (DFC) at Steno Diabetes Center North Denmark, Aalborg University Hospital, Denmark, for the present mixed-method study. Study inclusion criteria were a diagnosis of type 2 DM, age between 18 and 75 years, a referral to the DFC, and adequate Danish language level, whereas exclusion criteria were a history of neurological or neuropsychiatric disorder or previous or current alcohol and/or drug abuse. We excluded individuals with Charcot to maintain a more homogenous study group and excluded those with psychiatric diagnoses as well as individuals diagnosed with subtle dementia or other neurological disorders, based on information obtained from clinical records, to ensure data integrity and isolate the effects of factors related to DFU. The treating nurse invited eligible face-to-face subjects to participate in the study following their outpatient visit to the DFC. The study consisted of one session in which the participants were interviewed and completed different questionnaires. The staff at the DFC was instructed to maintain their normal instruction regarding foot self-care advice during the project period to minimize any unintended impact on the study. The staff’s normal instruction included footwear, hygiene, and visual inspection of the feet, although there may be some variability in the instructions.
Clinical records, questionnaires, and cognitive function test
Data on age, body-mass-index, DM duration, and complications were obtained from the medical records. The participants were asked to rank how challenging they found it to see, hear, read, and write on a scale from 1 to 4 (1 = very good, 2 = good, 3 = difficult, 4 = very difficult). The participants completed the Danish short version of the European Health Literacy Survey Questionnaire (HLS-EU-Q16) (16 items). 18 Scoring for the HLS-EU-Q16 varies between 0 and 16, by which three levels of health literacy are established, either as inadequate (0–8), problematic (9–12), or sufficient (13–16). The participants also filled out the Danish version of major depression index (MDI) (12 items), 19 where a score below 20 indicates no depression, 20–25 mild depression, 25–29 moderate, and above 29 severe depression. 19
The Danish version of Addenbrooke’s Cognitive Examination III (ACE-III) was used to test the participant’s cognitive function (19 items). 20 ACE-III is a screening test comprising attention, memory, fluency, language, and visuospatial domains. It is useful in screening for cognitive impairment, especially in detecting dementia, 20 with diabetes both with and without peripheral neuropathy.21,22 The highest ACE-III score that can be achieved is 100. A total ACE-III score of 88–100 is considered normal, 83–87 is inconclusive, and below 83 is reduced with respect to cognitive function.
Interview
The first and third authors constructed a semi-structured interview guide and discussed it with diabetes physicians, nurses, and research staff. The interview guide contained explorative questions, allowing the participants to elaborate and exemplify their statements. The guide to KAP surveys inspired the structure of the interview guide (Table 1) to get insight into three themes: knowledge, attitude, and practice. 23 The interview guide was subsequently pilot-tested on two individuals with diabetes, and concurrently, the interviewer (first author) was supervised by an experienced qualitative researcher (third author). The interviews were conducted by the first author (male), who held a PhD in biomedical engineering and was employed as a researcher during the study period. The interviewer introduced himself as an engineer with a keen interest in understanding the real-world challenges faced by individuals with DFUs, aiming to gather insights for inspiring new technological solutions. The interviewer had never met the participant prior to the interview. The interviewer and participant were alone during the interviews. To create a relaxed and open atmosphere during the interview, the interviewer wore clothing from his private wardrobe and appeared as a private person rather than a healthcare professional.
The interview guide used in the present study.
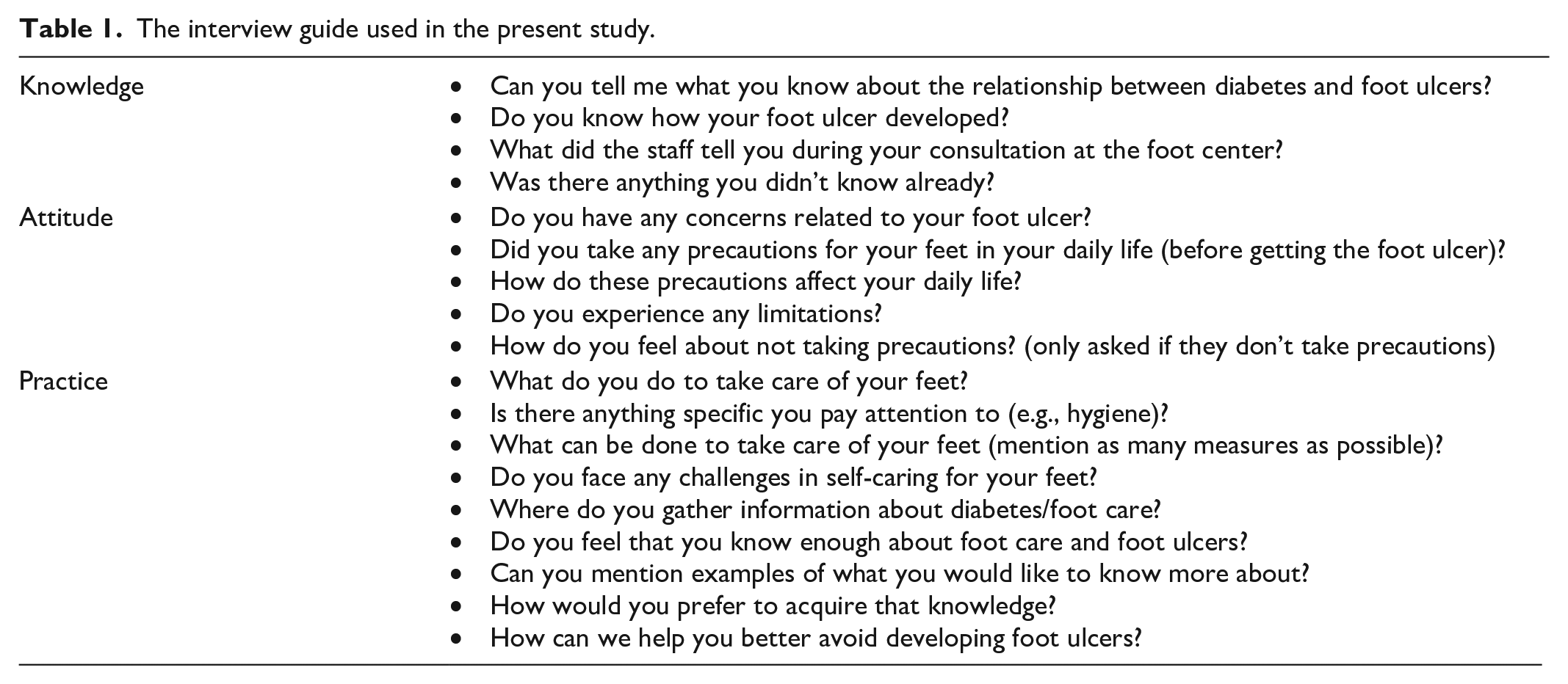
The median duration of the interviews was 11:54 min (range 5:21–16:00 min), recorded using a Dictaphone (Olympus, Shinjuku City, Japan), manually transcribed and anonymized, and given an ID number. All interviews were conducted in Danish. The interviews were later transcribed verbatim by first and second author and subsequently read and discussed among three of the authors. This allowed co-authors not involved in the data-collection to audit the transcripts. 24 Quotations in Danish were translated into English by a person with a BA degree in Business English and discussed among first, second, and third authors.
Ethics
The participants were given written and oral study information, and written informed consent was obtained. This study was conducted following the Declaration of Helsinki and approved by the North Denmark Region Committee on Health Research Ethics (N-20210048).
Statistical analysis
The demographic and clinical data, including ACE-III, MDI, and HLS-EU-16 scores, were analyzed using descriptive statistics. The qualitative data were analyzed thematically, using a stepwise approach inspired by Braun and Clarke. 25 The data analysis was iterative, shifting between familiarization with data and line-by-line coding, followed by developing and reviewing categories and themes. The second author undertook the initial coding and continuously discussed and revised it in collaboration with the first and the third author. A code tree was structured deductively, inspired by the KAP factors. Subthemes were constructed and named inductively to answer the research questions. See Table 3 for an illustration of the qualitative data analysis process.
Subsequently, an integrated analysis of the results from the quantitative and qualitative strands 26 was conducted inspired by a joint display technique used within mixed methods research in order to blend and synthesize two or more types of data together. 25 We used the Pillar Integration Process (PIP) to create an integrated analysis of quantitative and qualitative results and provide a visual presentation of the results for the same cases in parallel. 26 In the present study, foot self-care profiles were created through integrated analysis between the quantitative results shaped by cognitive function scores and health literacy and the qualitative findings from the interview. Table 4 illustrates the analysis process and procedure for conceptualizing foot self-care profiles in the center of the table.
The qualitative material was analyzed using the NVivo software 14 (QSR International, Doncaster, Australia). 27
Results
Participant characteristics
Figure 1 shows the inclusion flowchart of the study participants. During the project inclusion period, 87 subjects were referred to the DFC, and 12 were included in the study. Demographic, clinical, and functional characteristics are presented in Table 2. Eleven of the participants were males. The median age was 62.5 years (49–75), and median Body Mass Index was 27.7 (26.9–48.8). The participants had been diagnosed with DM in a median period of 18.5 years (range: 0–28). In four of the participants, the current DFU was registered as the first episode. Eleven of the participants had been diagnosed with neuropathy, and three had also been diagnosed with retinopathy. Four of the participants were still working, and the remaining eight retired. Five participants were single, four were married/de facto, and three were divorced.
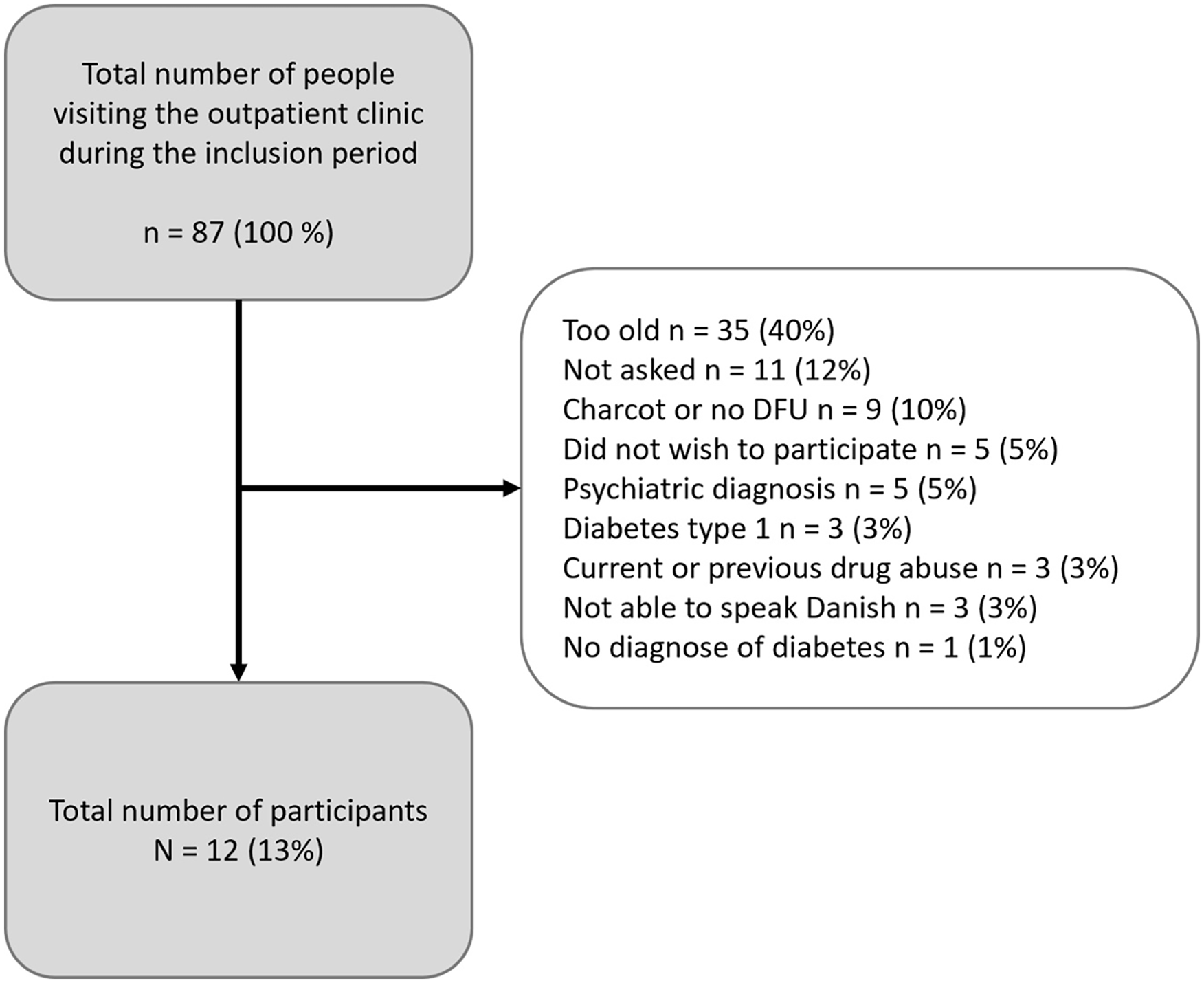
Flowchart of study participant inclusion.
Demographic, clinical and functional characteristics of the 12 study participants.

ACE-III: Addenbrooke’s Cognitive Examination; BMI: Body Mass Index; DFU: diabetic foot ulcer; HLS-EU-Q16: European Health Literacy Survey Questionnaire; MDI: Major Depression Inventory.
Health literacy, cognitive function and state of depression
Nine participants were observed with a health literacy level categorized as sufficient, problematic in two participants, and insufficient in one participant (Table 2). Five participants were observed with a normal cognitive score, three with an inconclusive score, and four with a reduced score (Table 2). Fluency and memory were the two most common domains by which the participants with cognitive deficits were observed. Figure 2 shows an overview of which domains the participants had the most errors in percentage. In one participant, the MDI score was 37, indicating severe depression; in two participants, MDI scores were 21 and 23, indicating mild depression. The remaining study participants were detected with MDI scores within normal range.

A univariate scatter plot of correct answers for the cognitive domains in the study participants tested with the Addenbrooke Cognitive Examination III. The blue dots represent each participant, and the horizontal black lines represent the mean score.
Qualitative findings
According to KAP three themes were developed through the thematic analysis: Knowledge about DFU, Attitude toward DFU, and Practice related to foot self-care actions. These themes describe the participants’ understanding, considerations, and concerns about their DFU and foot self-care practices. Table 3 provides an overview of the themes and sub-themes, illustrated by quotations.
Themes, subthemes, and data extracts form the interviews from the interviews exploring foot self-care in people with diabetic foot ulcers.

ACE: Addenbrooke’s Cognitive Examination; DFU: Diabetes foot ulcer; HLS: Health Literacy Survey.
Theme 1 (Knowledge about DFU) reflects the participants’ understanding of DM and DFU and their need for information about these conditions. Some participants demonstrated a comprehensive understanding of the connection between DM and the risk of developing DFU, while others expressed a need for more information from healthcare professionals.
Theme 2 (Attitude toward DFU) reflects the participants’ perceptions of DM and DFU, their concerns about their quality of life, encounters with the healthcare system, self-image, and opinions of others.
Theme 3 (Practice related to foot self-care actions) reflects how participants applied their knowledge and attitude toward foot self-care actions. It illustrates how their attitude may influence the levels of prevention and their actions regarding DFU and foot self-care. While some participants took a proactive role toward prevention, others appeared more passive or distant to their foot self-care actions.
Foot self-care profiles
Based upon Nutbeams and Kickbusch’s descriptions of health literacy levels11,12 three foot self-care profiles (proactive, active, and passive, respectively) were constructed through the PIP analysis. The profiles are presented in Table 4, where different columns illustrate the stepwise process of the PIP.
An integrated analysis of quantitative results and qualitative findings describing different health literacy related roles concerning foot self-care practices.

ACE-III: Addenbrooke’s Cognitive Examination III; DFU: diabetes foot ulcer; HLS: Health Literacy Survey.
The proactive profile (takes a proactive role concerning their health)
Persons with this profile can critically analyze health information and adjust their foot self-care practice. As it appears in Table 4, the participant actively prevented the incident of DFU because he had knowledge that influenced his practice. Thereby, his actions related to the prevention of DFU. For example, he ensured not to step on anything and checked his feet before putting on shoes.
The active profile (takes action in response to a situation)
Persons with this profile, independently of the ACE-III and HLS score, all seemed to be challenged by either knowledge or attitude, which might impact their practice toward foot self-care. According to Table 4, the participant had knowledge that might help him actively prevent DFU. He actively prevented an incident of DFU but did not give his feet any extra attention. This statement could indicate that his knowledge regarding DFU risk was limited or that his actions toward foot self-care were influenced negatively by his attitude.
The passive profile (takes no action)
Persons with this profile take a passive role concerning their health and make certain reservations or, at worst, neglect the information regarding the need for foot self-care. As it appears in Table 4, the participant acted passively regarding preventing DFU. Due to restricted knowledge or a reserved attitude about DM, he may not have paid any attention to the need for foot self-care.
Discussion
The present study included twelve persons with active DFU, focusing on the assessment of their KAP toward DFU. The study also investigated health literacy and cognitive function.
Nine of the participants had a sufficient HLS score, and only five of the participants had a normal cognitive score. Memory and fluency were the two most common cognitive domains challenging the participants. Deficits in these two domains align with previous studies on cognitive assessment among people with long-term DM.9,10,28–33 Nevertheless, the relationship between DFU risk and cognitive function remains debated. Prior research has indicated that cognitive impairment does not appear to be more prevalent in patients with diabetes and DFU compared to those without DFU,34–36 whereas others have observed a difference. 37 This contradiction may stem from the complex interplay of diverse cultural, educational, and social factors. To improve health literacy, it is important to consider the diversity of individuals and how these factors can impact their understanding and navigation of the healthcare system.11,12,38,39 Nevertheless, this could indicate that factors other than cognitive function, such as socio-economic disadvantage, health system inequity, and complexity of treatment regimens rather than impaired cognition, might significantly drive the risk of DFU. 40
Along those lines, the present study supports that other factors might also be important for people’s compliance with foot self-care recommendations than cognitive function alone. 40 The interviews with the participants revealed that they had varying levels of knowledge about DFU and its relation to DM. Some participants were unaware of the connection between DM and DFU, while others could explain the relationship in detail. The interviews also revealed that in some healthcare profiles, the participants had sufficient knowledge, but despite that, the participants’ attitudes caused them not to apply their knowledge in the context of foot self-care practice. However, previous studies from other countries indicate that people with DFU have a proactive attitude but lack knowledge.38,39
Initially, there did not seem to be a clear pattern between the participants’ ACE-III, HLS scores, and answers from the interview in the present study. However, when we systematically integrated the different data sources using PIP,28 three healthcare profiles emerged among the participants in the present study (proactive, active, and passive, respectively).
The proactive foot self-care profile group constitutes competencies in interacting with the health system. 11 They recognize the importance of maintaining healthy feet and avoiding DFU.41–44 Individuals with this profile proactively seek health information, and their actions demonstrate a commitment to aspiring for good health and an awareness of beneficial behaviors.41,44–46 They exhibit a willingness to seek medical assistance, engage in healthy practices, and actively inquire during medical consultations, making them distinguishable from the other profiles.11,12,41,44,46 The profile also seems characterized by having a normal cognitive function.
The active foot self-care profile is more diverse and conflicting regarding the KAP factors. It occurs that healthcare practice in persons with this profile is somehow limited due to an attitude with personal constraints and lack of responsiveness by which not even appropriation of more knowledge will not necessarily contribute to a positive change in practice. Previous studies have identified that some individuals feel little need to take preventive actions.45–48 They appear knowledgeable about how to handle their health situation, but their attitude can cause them not to apply their knowledge, and they are also reluctant to make an extra effort for their health. 11 This may also suggest that simply providing these individuals with more knowledge or information may not necessarily result in positive changes in their health behavior or practices. Therefore, healthcare providers may need to employ more tailored and personalized approaches to identify, engage, and motivate these individuals to help them care for their feet.44,46–49 In future studies, it would be valuable to delve into subgrouping within the active profile, given its diversity.
The passive profile seems to be the most problematic of the three-foot self-care profiles. Persons with this profile appear to be characterized by diminished cognitive function. Their health self-care attitude may negatively affect their receptiveness to additional information.11,12 This type of profile lacks basic knowledge, which has also been identified among some individuals in previous studies.14,15,46,49 Prior research has also revealed that certain individuals disregarded foot self-care recommendations because they had difficulties accepting their diabetes.41,45,50 This inclination is similarly observed among the participants in the current study. In previous studies, getting a DFU has been described as a wake-up call. 41 Several participants from this profile also acknowledge this, indicating they begin comprehending the severity. However, despite this realization, they appeared reluctant to shift to a proactive approach. Healthcare providers may need to use more empathetic and non-judgmental communication styles when conveying information to individuals with this profile, avoiding admonitory tones that may further discourage engagement with their self-care practices.
According to Nutbeam, progression between levels of health literacy is dependent on cognitive development and exposure to different information and is influenced by personal and social skills and self-efficacy concerning defined issues. 11 We found that people with DFU represent a heterogeneous group regarding cognitive function, health literacy capacities, and roles. We also found that knowledge and attitude influenced how the individual coped with and acted concerning their foot self-care. Therefore, to individually target the care for people with DFU, clinicians should consider focusing on all KAP factors, resources, and barriers to health literacy to support the individual in taking a proactive role regarding their foot self-care.
Several participants with active and passive profiles, respectively, contradicted their answers from the HLS-Q16 questionnaire during the interviews. For instance, although some participants answered in the HLS-EU-16 survey that they found it easy to ask their doctor questions if they did not understand something, they revealed that they did not do so during the interview. Instead, some participants reported that they often simply accepted not understanding the instructions or rationale behind them from healthcare professionals. Despite most participants exhibiting sufficient health literacy, some reported experiencing condescension by healthcare professionals in other departments, potentially contributing to their negative attitudes toward healthcare interactions. Still, they, in general, felt well-received in the DFC.
Strength and limitations
Although there are interesting findings, the study has some limitations. Firstly, the study had a small sample size, and due to the inclusion criteria, a larger proportion of eligible patients in the DFC could not be included (Figure 1). Additionally, no prior sample size calculation was conducted. Thus, only 12 participants were included in the analysis. However, these criteria were necessary in order to answer the hypothesis and limit confounding factors. Secondly, the study’s participant composition featured only one female, resulting in limited gender diversity within the sample. Consequently, the potential influence of gender on the study’s outcomes and observations has not been explored. However, this reflects the everyday diversity in the outpatient clinic and furthermore that men are more vulnerable to DFU than women. 51 Thirdly, ACE is a general test, and the transferability, for example, remembering an address compared to remembering and complying with healthcare information, may not be one-to-one. However, it could potentially be valuable if a specific tool for screening cognition and other relevant factors for DFU self-care were developed in the future. One participant was identified as experiencing severe depression, according to the MDI, which may have influenced their responses. Notably, depression was not an exclusion criterion in this study. However, it prompts consideration for future research to assess whether depression should be considered as an exclusion criterion. This study excluded many potential participants based on age, as age has been associated with cognitive decline. Nevertheless, given the significant proportion of individuals excluded, future research in this field should also consider enrolling older participants.
The strength of the study is that, firstly, the ability to examine the KAP factors and cognitive function in detail is described through several data sources. Secondly, the interview guide was structured with open-ended questions in accordance with KAP guidelines, thereby minimizing the likelihood of participants guessing the correct answer rather than genuinely knowing it, which is a risk associated with questionnaires featuring multiple-choice answers. 23 The present study used quantitative and qualitative data collection and analysis strategies for a complementary strategy. 24 Furthermore, the reporting and visualization of the integrated analysis of the quantitative and qualitative results using the PIP analysis technique provided transparency and maximized visual and methodological synthesis opportunities to increase the dependability and rigor of conceptualizing foot self-care profiles. 26 We used quotations from all participants in Tables 3 and 4 to make it possible for the reader to follow the audit trail and increase the transparency allowing the reader to judge the trustworthiness of the process and credibility of the findings. Despite the relatively small number of participants, all participants contributed to the construct of both themes and conceptual foot self-care practices. However, based on the current data material, we cannot assess whether further theoretical saturation could be reached if we had conducted more interviews, which can be considered a limitation of this study. Finally, the creditability of the findings was enhanced by involving first, second, and third authors in all steps of the analysis, which increased the analysis’s comprehensiveness and transparency. 24
Based on the findings of this study, it is clear that there is a need for a more individualized approach to foot self-care education among people with DFU. The heterogeneity among patients with DFU in terms of cognitive function and health literacy suggests that a one-size-fits-all approach may not be effective. Healthcare professionals need to identify the foot self-care profile of each patient and tailor their education and support accordingly. Further research is necessary to investigate strategies for personalized targeting, education, and attitude improvement toward foot self-care in individuals, with an emphasis on a larger study sample than the present study.
Conclusion
The present study highlights the heterogeneity among people with DFU regarding health literacy and cognitive function, suggesting that there is not necessarily a clear-cut picture of reduced functionalities in this population. However, it is noteworthy that only 5 out of the 12 participants were observed with normal cognitive function. The study identified three different foot self-care profiles within a population of people with DFU. Some participants appear to have a more proactive approach toward foot self-care based on adequate knowledge translating into a synergistic attitude. Other participants appear to take an active role but do not seem to consider their needs for foot self-care. In contrast, other participants seem to lack knowledge about DFU or have a passive attitude toward diabetic foot self-care practice.
Supplemental Material
sj-docx-1-smo-10.1177_20503121241258841 – Supplemental material for Health literacy and cognitive function in people with diabetic foot ulcer with focus on knowledge, attitude, and practice in relation to foot self-care
Supplemental material, sj-docx-1-smo-10.1177_20503121241258841 for Health literacy and cognitive function in people with diabetic foot ulcer with focus on knowledge, attitude, and practice in relation to foot self-care by Morten Bilde Simonsen, Sofie Ladekarl Christiansen, Mona Kyndi Pedersen, Johan Røikjer, Suganthiya Santhiapillai Croosu, Peter Derek Christian Leutscher and Niels Ejskjaer in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121241258841 – Supplemental material for Health literacy and cognitive function in people with diabetic foot ulcer with focus on knowledge, attitude, and practice in relation to foot self-care
Supplemental material, sj-docx-2-smo-10.1177_20503121241258841 for Health literacy and cognitive function in people with diabetic foot ulcer with focus on knowledge, attitude, and practice in relation to foot self-care by Morten Bilde Simonsen, Sofie Ladekarl Christiansen, Mona Kyndi Pedersen, Johan Røikjer, Suganthiya Santhiapillai Croosu, Peter Derek Christian Leutscher and Niels Ejskjaer in SAGE Open Medicine
Supplemental Material
sj-docx-3-smo-10.1177_20503121241258841 – Supplemental material for Health literacy and cognitive function in people with diabetic foot ulcer with focus on knowledge, attitude, and practice in relation to foot self-care
Supplemental material, sj-docx-3-smo-10.1177_20503121241258841 for Health literacy and cognitive function in people with diabetic foot ulcer with focus on knowledge, attitude, and practice in relation to foot self-care by Morten Bilde Simonsen, Sofie Ladekarl Christiansen, Mona Kyndi Pedersen, Johan Røikjer, Suganthiya Santhiapillai Croosu, Peter Derek Christian Leutscher and Niels Ejskjaer in SAGE Open Medicine
Footnotes
Acknowledgements
Thank you for the assistance from Lise Hammershøj, RN, foot ulcer specialist, and the other staff at the Diabetes Foot Center at Aalborg University Hospital. Thank you to Lotte Moss Kvist, BA Business English, for feedback on and assistance in translating the qualitative quotations from Danish to English. Also, thank you to all the persons with diabetes for sharing their thoughts, feelings, and personal stories in the interviews.
Author contributions
M.B.S, S.L.C., M.K.P., J.R., S.S.C., P.D.C.L., N.J. contributed to Conception and design of the study; M.B.S. contributed to Data Collection; M.B.S., S.L.C., M.K.P. contributed to Data analysis; M.B.S., S.L.C., M.K.P. contributed to Drafting; M.B.S., S.L.C., M.K.P., J.R., S.S.C., P.D.C.L., N.J. contributed to Revising; M.K.P., P.D.C.L., N.J. contributed to Supervision; M.B.S., P.D.C.L., N.J. contributed to Funding.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by Marie Pedersen and Louise Heibergs Fond.
Ethics approval
This study was conducted following the Declaration of Helsinki and approved by the local committee on health research ethics (N-20210048).
Consent statement
The participants were given written and oral study information, and written informed consent was obtained.
Trial registration
Not applicable.
Data availability statement
Data is available upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.