
Abstract
Abstract
Purpose
Perthes’ disease (PD) results from loss of blood supply to the hip and can progress to femoral head deformity. MRI in the early course of the disease can provide data on the initial extent of infarct. Vascularity of the femoral head is assessed by gadolinium-enhanced MRI (contrast MRI), which may be improved by the digital subtraction technique (subtraction MRI). We hypothesized that gadolinium-enhanced MRI without subtraction was comparable with subtraction MRI in depicting the femoral head perfusion.
Methods
In all, 34 patients (34 hips) with unilateral PD had gadolinium-enhanced MRI as part of a prospectively randomized study. Nine patients had three MRIs, 15 had two and ten had a single MRI. Measurement of perfusion of the femoral head (MRI perfusion index) was obtained using digital image analysis on all the MRIs, including both before and after subtraction. A paired sample t-test was performed to compare the measurements.
Results
The mean age of the patients was 8.9 years (sd 1.6). At the time of diagnosis, the subtraction MRI did not elicit a statistically significant difference in MRI perfusion index measurements when compared with the contrast MRI (p = 0.19). The same findings were found when including all patients at various stages of the disease (p = 0.30). Qualitatively, although some subtraction MRI images showed superior delineation of epiphysis, there are no significant differences throughout the whole series.
Conclusion
Although the current literature supports the increasing role of the subtraction MRI for PD management, our study proposed that the contrast MRI without subtraction technique appears adequate in assessing femoral head perfusion.
Level of Evidence
Level I - Diagnostic study
Introduction
Perthes’ disease (PD) is one of the most common hip disorders in children and adolescents. PD results from idiopathic avascular necrosis of the femoral head and presents with insidious onset of pain and limp. While the underlying cause is unknown, the pathogenesis of the disease has been well documented.1–3 Using plain radiographs, PD has been classified into four stages: initial, fragmentation, reossification and healed. MRI has the advantage over the radiograph in detecting any physeal or metaphyseal changes as well as extension of osteonecrosis early in the disease4,5 and has become standard practice in many centres.
Contrast-enhanced MRI using gadolinium can further delineate the extent of the avascular necrosis, especially in the early stages of disease when plain radiographs can appear normal. At this stage, dynamic multiphasic imaging provides accurate assessment of the proximal epiphyseal perfusion. Hypoperfusion is one of the earliest changes that can be detected in PD, which can be further evaluated with delayed (two to five minutes) T1 weighted fat suppressed imaging after contrast administration. 6 On top of this, digital subtraction technique has been reported to increase the sensitivity of detecting even subtle alterations in perfusion. 7
In some institutions, digital subtraction technique (known as subtraction MRI) has become the recommended clinical practice and the basis of studies related to femoral head vascularity in PD.8–11 These studies have utilized the Perfusion Index 8 as a method to evaluate the vascularity of the femoral head in PD. This is particularly useful in the early stage of PD and has been reported to be a reliable prognosticator. 8 It has been shown to correlate well with greater deformity changes shown by the Deformity Index 12 on plain radiographs at two years, which itself has been proven to correspond with the Stulberg 13 outcome. Further, MRI has been used to assess the rate and pattern of revascularization in active PD. 9
We performed subtraction MRI in 34 children with PD as part of a prospective, randomized and multicentre clinical trial of bisphosphonate treatment. MRI was performed as an exploratory investigation to assess the vascularity pattern of the femoral head throughout the course of the disease and compare it with standard contrast-enhanced MRI. This has also enabled us to see the effect of bisphosphonate on femoral head revascularization.
Materials and methods
This study was a part of a multicentre trial of bisphosphonate (zoledronic acid) treatment in children with early stage (lateral pillar A or B) and unilateral PD involving five tertiary referral children's hospitals. 14 Following ethics committee approval, 84 children (mean age 7.8 years, sd 1.5) were enrolled from 2010 to 2016. Subjects were randomized into either ‘treatment’ (bisphosphonates + standard care) and ‘control’ (standard care) arms of the study. Standard care involved an initial six- to 12-months non-weight-bearing period. Any supplemental management either surgical or non-surgical was at the discretion of the treating orthopaedic surgeon. Pelvic MRI was performed within six months of the diagnosis in both treatment and control subjects.
For this aspect of the study we evaluated the subtraction MRI of 40 participants who were enrolled at the coordinating centre of the trial. MRIs were performed at screening, 12 and 24 months of the study. Not all subjects had an MRI at each time point (Table 1). A total of 34 (28 boys, six girls) of these had both contrast and subtraction images (included in each MRI examination) suitable for evaluation at least at one of these time points (Table 1). Six participants had MRIs excluded due to either non-satisfactory quality of the image or performance of just a non-contrast MRI.
Summary of the epidemiological data for the subtraction MRI cohort

In all, 30 subjects had completed the trial, 17 in the treatment group and 13 controls. The mean perfusion index was compared between the two groups at 12th and 24th month to assess if bisphosphonate treatment impacted femoral head revascularization and perfusion measurements. From the 30 patients, we were able to compare 23 images from the12th month visit and another 22 from the 24th month. The remaining images were either not available or of poor quality and were not used for comparison.
Image acquisition
MRI imaging was performed using two different systems; the 1.5T Ingenia (Philips, Eindhoven, The Netherlands) with anterior and posterior array and the 3T Verio (Siemens, Erlangen, Germany) with the 32-channel body coil. The same machine was used to acquire serial measurements on any individual subject. The following sequences were obtained before administration of contrast: coronal T1-weighted, coronal and axial Proton density fat saturation. Pre-contrast images of coronal and sagittal oblique T1-weighted fat saturation (T1FS) were also obtained. Approximately two minutes after the injection of Gadolinium (0.1 mmol/kg), post-contrast images on coronal and sagittal oblique T1FS sequences were then obtained. The subtraction images were generated by subtracting the initial pre-contrast T1FS images from the corresponding post-contrast T1FS. A slice thickness of 3 mm was employed.
Image analysis
Perfusion index was used to compare the images of the subtraction MRI with the contrast-enhanced MRI. Using digital image analysis software Mimics Research 19.0 (Materialise, Leuven, Belgium), coronal images of T1FS both pre- and post-contrast, as well as subtraction were evaluated. Following the methods of Du et al, 8 the total area of the femoral head and the total area of perfusion within the head were determined. Each area of interest was quantified by outlining it with the measuring tool on the software in the units of mm2, on five serial images around the centre of the femoral head (Fig. 1). Perfusion index was obtained by dividing the sum of the area of perfusion (measured separately on both subtraction MRI and contrast MRI), with the sum of the area of the femoral head on T1FS pre-contrast images. The range of indexes were from 0 (not perfused) to 1 (totally perfused). All images were evaluated by a single observer (KJ), blinded to the patient's clinical details and treatment arms.
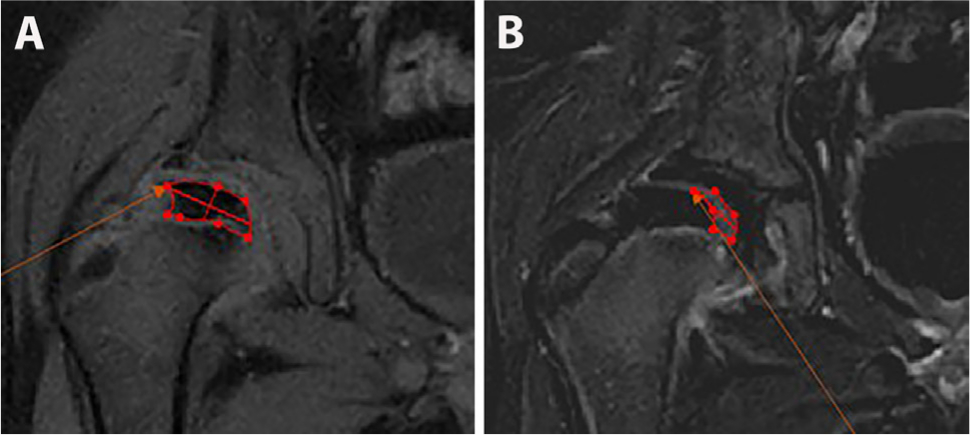
Methods of measuring area of interest on contrast-enhanced MRI. MRI obtained at the initial stage, a week after diagnosis at the age of 6.7 years. The patient was subsequently treated with bisphosphonate and was non-weight-bearing. Coronal T1-weighted fat saturation images are shown: (
Statistical analysis
The perfusion index of the subtraction MRI images was compared with the post-contrast MRI images for each patient. Paired t-student test was used. Independent student t-test was utilized to compare the perfusion index between the treatment and control group from the trial.
Results
MRIs of the 34 subjects at various stages of the disease; either during screening, 12- or 24-months of follow-up were available. The mean age at diagnosis of PD was 7.7 years (sd 1.4) and the mean duration between the diagnosis and the first MRI was 1.4 months (sd 1.7). The mean duration between the diagnosis and the third MRI was 25.5 months (sd 2.0). Out of the 34 patients, nine had three MRIs, 15 patients had two MRIs and ten had a single MRI. A total of 67 MRIs (at various PD stages) were used for the comparison study. When divided into waldenström 1 stages of disease classification, there were 18 MRIs in the initial stage, ten in the fragmentation stage, 30 in the reossification stage and nine in the healed stage.
Because the subtraction MRI was able to eliminate the background noise, there is an obvious difference between the subtraction and the contrast MRI images. This made distinguishing between the techniques very easy and meant it was not possible to blind the assessor to the technique used (Fig. 2).
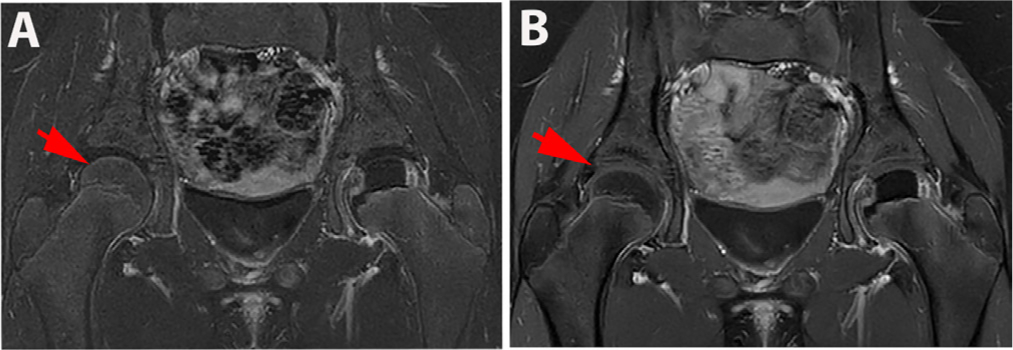
Different effects on normal femoral head. MRI obtained at the initial stage for a patient diagnosed at the age 8.1 years, who was treated with bisphosphonate and was non-weight-bearing. Coronal T1-weighted fat saturation images are shown, for subtraction (a) and post-contrast image (b), respectively: (
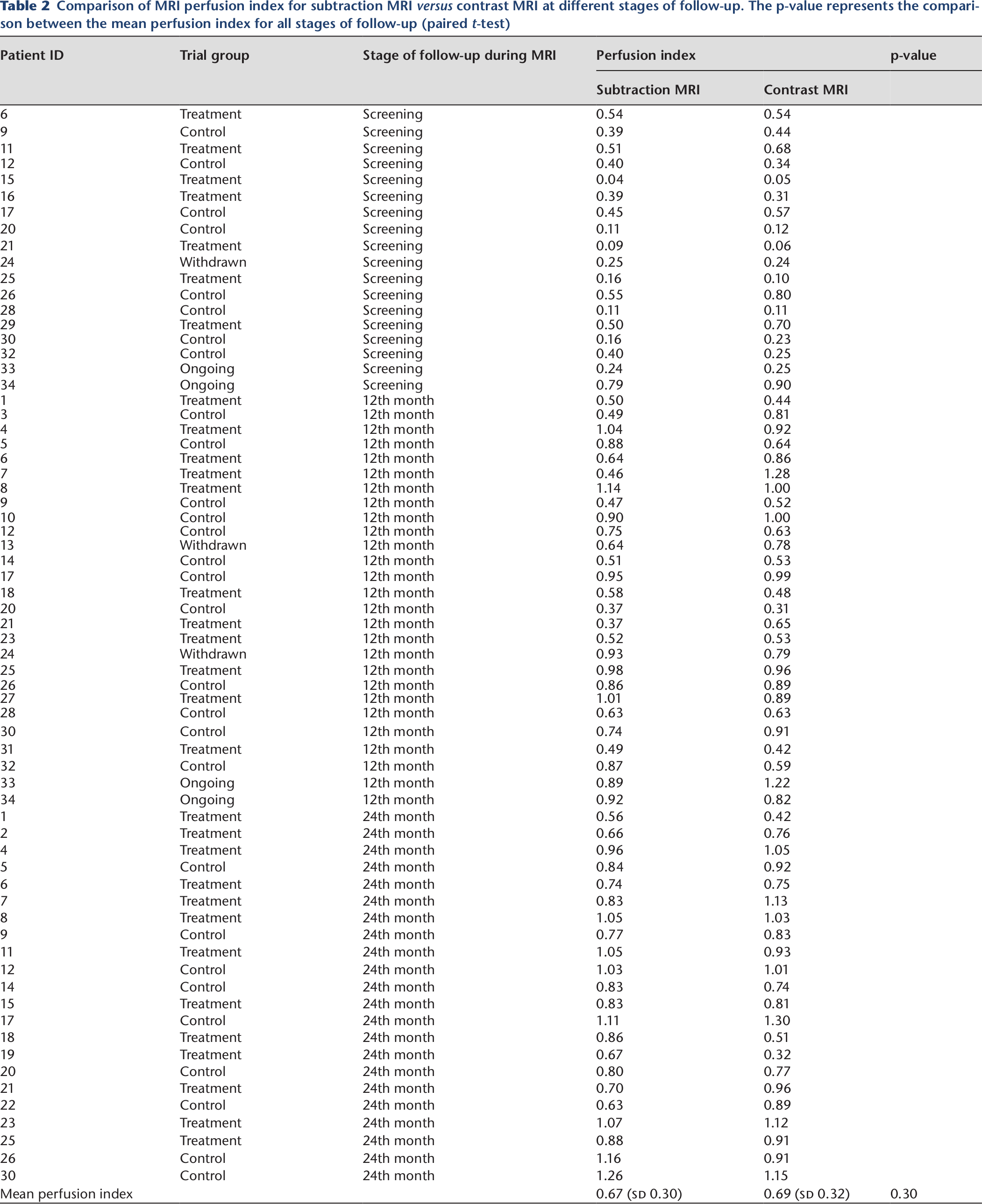
For all 67 MRIs the mean perfusion index for the subtraction MRI was 0.67 (sd 0.30) and 0.69 (sd 0.32) for the contrast MRI images (p = 0.30) (Table 2). As expected, the perfusion of the femoral head improved with time. However, as the method of measuring perfusion index is based on the area of necrosis, the measurements became harder and less accurate as perfusion increased in the later stages of PD and led to some of the perfusion indexes measuring >1.0.
Comparison of MRI perfusion index for subtraction MRI versus contrast MRI at different stages of follow-up. The p-value represents the comparison between the mean perfusion index for all stages of follow-up (paired t-test)
In all, 18 subjects had an MRI during screening, with a mean perfusion index of 0.34 (sd 0.20) for the subtraction MRI and 0.37 (sd 0.27) for the contrast MRI (p = 0.19). Figure 3 shows an example where subtraction MRI images were able to distinguish the area of necrosis better than the contrast MRI.
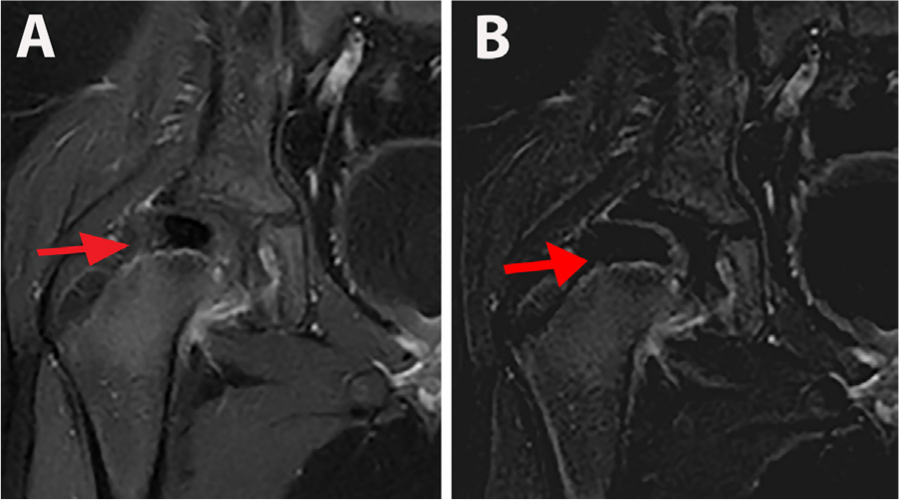
Example of the advantage of the subtraction MRI. MRI obtained at the initial stage following diagnosis at 9.8 years old. Subsequent treatment involved bisphosphonate and was non-weight-bearing. Coronal T1-weighted fat saturation images are shown, for post-contrast (a) and subtraction (b) images, respectively: (
Perfusion index comparison between subtraction MRI and contrast MRI according to the Waldenström disease stages revealed no difference: initial stage, 0.34 (sd 0.20) versus 0.37 (sd 0.27) (p = 0.19), fragmentation stage, 0.63 (sd 0.22) versus 0.74 (sd 0.26) (p = 0.25), reossification stage, 0.82 (sd 0.23) versus 0.81 (sd 0.26) (p = 0.76) and healed stage, 0.86 (sd 0.17) versus 0.85 (sd 0.22) (p = 0.89).
Treatment with zoledronate did not influence perfusion index. In the 30 subjects who completed the study, the mean perfusion index at 12 months was 0.70 (sd 0.20) for both groups (p = 0.99) and at 24 months the index was 0.94 (sd 0.21) for control and 0.84 (sd 0.16) for the treatment group (p = 0.24)
Discussion
The Herring classification, 15 which is based on the height of the lateral third of the femoral head or ‘Lateral Pillar’ on anteroposterior pelvic radiograph, has influenced the principle of managing PD since it was introduced in 1992. However, because it can only be used during the fragmentation stage, concerns exist that ‘waiting’ until this stage before deciding on a specific management plan may be detrimental to the overall outcome. MRI provides the opportunity for early detection of PD and the delineation of the extent of avascular necrosis and may prove beneficial in guiding management prior to the fragmentation phase.
Over the last decade, research into the clinical applicability of MRI during initial stage PD has intensified. Earlier studies with non-contrast MRI showed physeal and metaphyseal changes as well as hip effusions, which radiographs were not able to detect.16,17 Further, contrast MRI allowed for the accurate visualization of the necrotic phase of PD. 18 Contrast-enhanced MRI with digital subtraction provided even more information on the femoral head vascularity, which has been shown to help in both diagnosis and prognostication.6,8,19 Although contentious, there is a body of literature supporting early containment surgery for children with PD.19–22 MRI has, therefore, been proposed as the optimal method to detect early PD and guide decision-making for containment surgery. 11 Serial perfusion MRI has also been used to localize areas of avascular necrosis and thus guide multiple epiphyseal drilling as well as assess revascularization.23,24
In the current study, digital subtraction technique (referred as subtraction MRI) was used, which has been reported to enhance the clarity of the images. Most MRI studies of PD in recent times have used this method to predict Lateral Pillar involvement, 11 to assess the significance of hip synovitis 25 and also hip revascularization patterns with serial MRI. 9 While the need for the subtraction MRI in the clinical setting has been questioned, 26 some institutions have adopted early subtraction MRI and it was recently recommended in the clinical practice guidelines of American College of Radiology. 5 Until this technique is more widely utilized generalizability of results is limited.
However, it also has its own disadvantages. Although subtraction MRI only adds a few extra minutes to be performed following contrast MRI sequence, it needs strict adherence to a specific protocol. As such, it requires trained radiology staff to ensure correct images are obtained and post-acquisition analysis including matching the exact pre- and post-contrast images to generate the subtracted image that can also be hampered by patient movement. As a result, we noted a number of images which were not suitable for our study. These issues have not been highlighted by any of the previous studies utilizing subtraction MRI. Therefore, the utility of contrast MRI without the subtraction technique is rarely discussed.
In the current study, half of the cohort (18/34) had subtraction MRIs performed in the initial stage of PD, the optimal time to evaluate perfusion status. We found that the post-contrast images (contrast MRI) were comparable with the subtracted images (subtraction MRI) for delineating area of avascular necrosis. The findings between contrast and subtraction MRI were comparable for all stages of PD. These data suggest that the contrast MRI is adequate to assess perfusion of the femoral head at all stages of PD.
Despite our main findings showing there were no differences between the two MRI techniques, it should be acknowledged that the subtraction MRI did provide higher quality MRI images. One such example is shown in Figure 3 where the area of necrosis at the lateral pillar was more apparent after subtraction MRI. Early enhancement of the lateral pillar on contrast-enhanced MRI has been described as a good prognosticative indicator as it represents an uncomplicated revascularization of the femoral head.27,28 On the contrary, slower healing is related to the absence of lateral pillar enhancement. This is a similar description to Conway 29 using pinhole scintigraphy on PD patients, who proposed two revascularization pathways: pathway A was associated with a good prognosis due to activity at the lateral column, while pathway B included a base filling pattern by new vessels and was associated with a poor prognosis due to slower revascularization. 29 Kim et al 9 proposed that assessment of the lateral pillar on the subtraction MRI could be used to decide the period of non-weight-bearing for PD patients. The authors suggested that only when healing occurs over the lateral pillar region and the signal intensity normalizes indicating reossification that a patient would be allowed to weight bear. One could argue, however, that the duration that it would take for lateral pillar reossification would be lengthy, by which time a radiograph would be a sensitive enough investigation. Although we found that subtraction MRI did provide additional information on vascularization in one of our cohort, this was not consistent across all subjects.
This study was not powered specifically to compare two MRI techniques but rather the MRIs were performed as an exploratory variable. It is, therefore, possible that the small sample size was inadequate to detect a difference between the two techniques. We also used two different MRI systems with different magnetic strengths (1.5T and 3T) for the study. Although each subject was consistently examined with the same MRI system, the impact of these cofounders on the MRI evaluation could not be known. Further, unlike previous perfusion MRI studies,8,9,11 we did not perform an interobserver reliability study to compare the results as we felt a single observer is adequate to perform the MRI comparison. The strength of this study is that it had involved data collected from a prospective, randomized control trial. Comparison of the perfusion index between the two treatment groups revealed no difference, suggesting that bisphosphonate treatment did not influence revascularization in this study. Other aspects that we will look into at the end of the trial are the prognosticative value of an early MRI perfusion index and also the perfusion patterns in different treatment groups at various stages.
In conclusion, subtraction MRI did not add extra information for most patients compared with contrast MRI for assessing perfusion of the femoral head in PD. This may provide a simpler pathway for the evaluation of bone perfusion in children. In recent years subtraction MRI has become more popular in the management of PD. The subtraction MRI is being used increasingly as an investigative tool, with current evidence suggesting it may have a role for detection of early or occult PD and for follow-up after multiple epiphyseal drilling. However, our study suggests that contrast MRI would be sufficient for the physician's decision-making involving the management for the majority of patients with PD. Therefore, we could not recommend the subtraction MRI as a routine clinical investigation.
Footnotes
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
CFM: conception and study design.
DGL: conception and study design.
TW: data collection and interpretation.
EO: data collection and interpretation.
All authors were responsible for drafting the manuscript and have read and approved the final manuscript.