
Abstract
Abstract
Purpose
The aims of present study are to clarify the follow questions: 1) what constitutes paediatric chondrosarcoma?; 2) what are the effects of the demographic and tumour characteristics on survival in patients with paediatric chondrosarcoma?; 3) which prognostic factors of paediatric chondrosarcoma differ from those of the adult population, which have been reported previously?
Methods
Paediatric patients who were diagnosed with chondrosarcoma were searched for using the case listing session protocol of the National Cancer Institute's Surveillance, Epidemiology, and End Results 18 databases (1973 to 2014). The extracted demographic information includes: age, race, gender, year of diagnosis, tumour sites, tumour histological subtype, grade, stage and treatment.
Results
A total of 247 paediatric chondrosarcoma patients were extracted and included in our present study. We find that the paediatric patients have significantly better survival rates than the adult patients. The year of diagnosis, tumour sites, tumour histological subtype, grade, stage and surgery received are independent prognostic factors for the survival rate of paediatric chondrosarcoma patients, but race, gender and age are not.
Conclusion
The paediatric chondrosarcoma patients have better survival rates than the adults. Paediatric patients with a diagnosis at an early age, tumour site at the vertebral column and pelvis/sacrococcyx, myxoid variants, high grade, distant stage and who did not have surgery have a poorer prognosis than patients with a diagnosis at a later age, tumour site at limbs, head and base, chondrosarcoma not otherwise specified, lower grade, localized stage and who received surgery.
Level of Evidence
II -Prognostic Study
Introduction
Chondrosarcoma is a slow-growing malignant tumour that is comprised of transformed cells that produce a cartilaginous matrix.1,2 It is the second-most common type of bone tumour and has a high rate of recurrence and risk of death.3–6 The incidence of paediatric chondrosarcoma is very rare and comprises < 10% of total chondrosarcoma cases. 7 Paediatric chondrosarcoma has mostly been reported as a case series8,9 or as a case report.10–17
The Surveillance, Epidemiology, and End Results (SEER) database represents approximately 28% of the US population, and this registry is the largest source of information on cancer incidence and survival data in United States. Since it provides data on patient demographics and survival formation, it is a very useful resource for studying cancer.18,19 In the present study, we use the SEER database to study chondrosarcoma in the 0-18-year-old population and in particular to investigate the associations between prognostic factors and survival outcomes.
Our questions include the following: 1) what constitutes paediatric chondrosarcoma?; 2) what is the effect of demographics and tumour characteristics on survival in paediatric chondrosarcoma?; 3) what are the prognostic factors of paediatric chondrosarcoma that differ from those of the adult population, which have been reported previously?
Methods and materials
This is a retrospective study of the National Cancer Institute's SEER 18 databases (1973 to 2014). 20 We submitted a data agreement form to the SEER administration and the agreement was accepted. The database uses publicly available information without personal identifiers; therefore, no additional Institutional Review Board approval is required in this study.
Our study is compliant with the checklist of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement21,22 (Supplemental Material).
Patients with ages from 0 to 18 years that were diagnosed with chondrosarcoma (including histological Type International Classification of Diseases (ICD)-O-323: “9220: Chondrosarcoma not otherwise specified’,’ “9221: Juxtacortical chondrosarcoma’,’ “9230: Chondroblastoma, malignant”, “9231: Myxoid chondrosarcoma”, “9240: Mesenchymal chondrosarcoma”, “9242: Clear cell chondrosarcoma” and “9243: Dedifferentiated chondrosarcoma”) were searched using the case-listing session protocol of the National Cancer Institute's SEER 18 databases. 24
The demographic information includes the patients’ age, gender, race, year of diagnosis, tumour sites, tumour histological subtypes (chondrosarcoma not otherwise specified (chondrosarcoma NOS), juxtacortical chondrosarcoma, chondroblastoma malignant, myxoid chondrosarcoma, mesenchymal chondrosarcoma, clear cell chondrosarcoma and dedifferentiated chondrosarcoma), grade, stage (localized, regional and distant) and treatment (surgery or non-surgery).
Statistical analysis
We first attempted to convert the patient ages to categorical variables of 0 to four, five to nine, ten to 14 and 15 to 18 years old, but the category of 0 to four only included five cases; therefore, we combined the 0 to four and five to nine categories into one category of 0 to nine years old. The year of diagnosis was converted into categorical variables of 2004 to 2014, 1994 to 2003, 1984 to 1993 and 1973 to 1983. Tumour sites are also categorized into the following five locations: vertebral column, pelvis/sacrococcyx, limbs, other bones (such as skull, rib, sternum, clavicle and mandible) and extraskeletal sites (outside of the bone). The tumour grades were also reclassified into two grades (low grade: ICD-O-3 Grades 1 and 2; high grade: ICDO-3 Grades 3 and 4).5,25,26
Survival curves were generated using the Kaplan-Meier method and log rank test. Both bivariable and multivariable Cox proportional hazard regression models were used to calculate the hazard ratios (HRs) with 95% confidence intervals (CIs) for chondrosarcoma cancer-specific survival (CCSS) and overall survival (OS).
Results
A total of 247 paediatric chondrosarcoma patients were extracted and included in our present study; 166/247 (67.21%) were male and 81/247 (32.79%) were female. Furthermore, 190/247 (76.92%) cases were white. Chondrosarcoma (NOS) is the most common histological subtype (approximately 61.13%). Additionally, most patients undergo surgery (86.23%); only 13.77% patients did not undergo surgery. The constituents and characteristics of the included patients are summarized in Table 1.
Characteristics of the paediatric chondrosarcoma patients from the Surveillance, Epidemiology, and End Results 18 Registries Research Database, 1973 to 2014
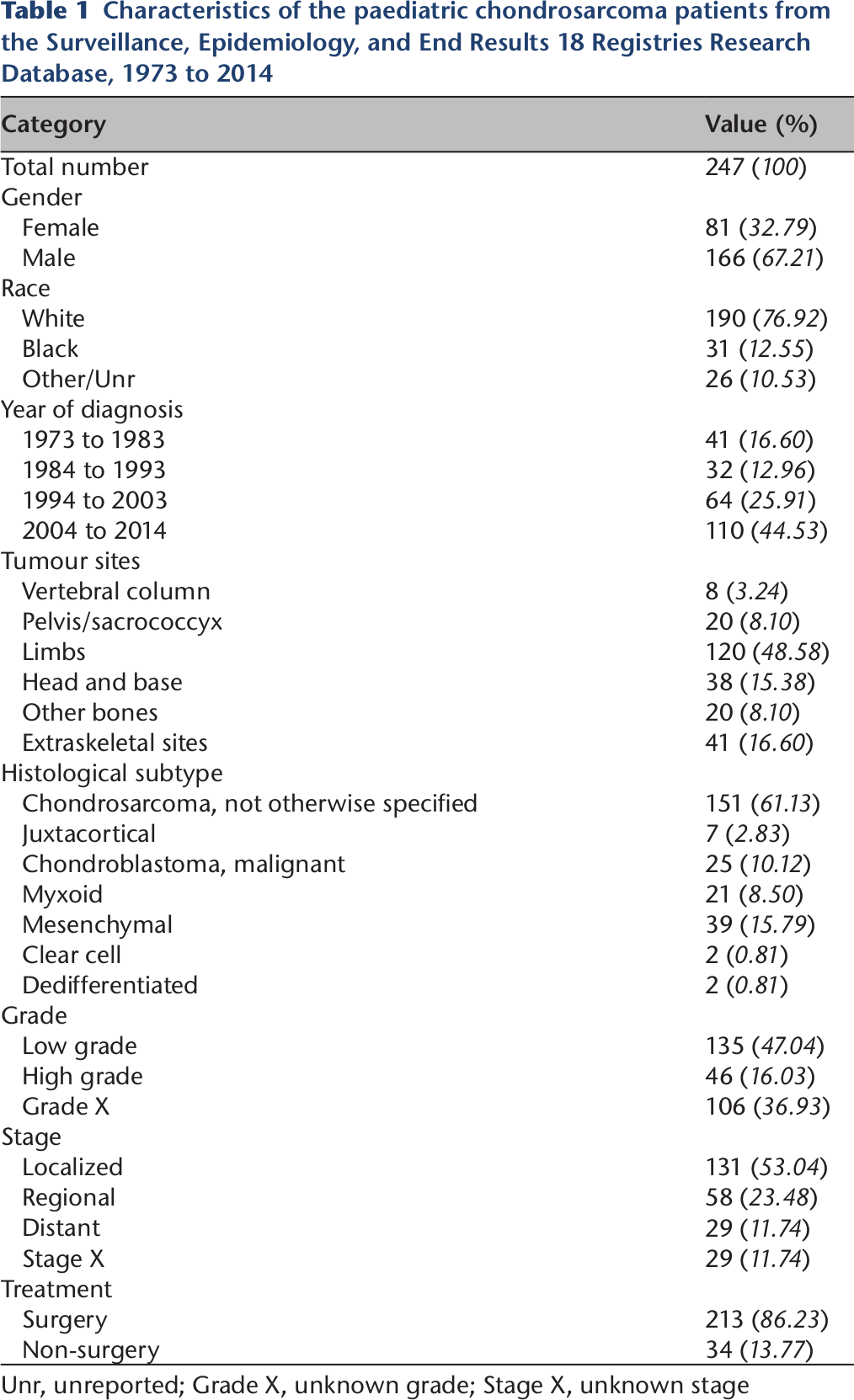
Unr, unreported; Grade X, unknown grade; Stage X, unknown stage
Paediatric versus adult patients
The paediatric patients had significantly better survival rates than the adult patients (Fig. 1). The bivariable and multivariable Cox proportional hazard regression models of CCSS and OS patients also showed the same results. When the age > 18 years category was used as a reference, the HRs (95% CI) of death caused by chondrosarcoma cancer in the 0 to 18 age category were 0.540 (0.378 to 0.772, p = 0.001) in the bivariable analysis and 0.449 (0.311 to 0.647, p < 0.001) in the multivariable analysis (Table 2). The HRs (95% CI) of death caused by all reasons in the 0 to 18 age category were 0.379 (0.285 to 0.503, p < 0.001) in the bivariable analysis and 0.345 (0.259 to 0.461, p < 0.001) in the multivariable analysis, respectively (Table 3).
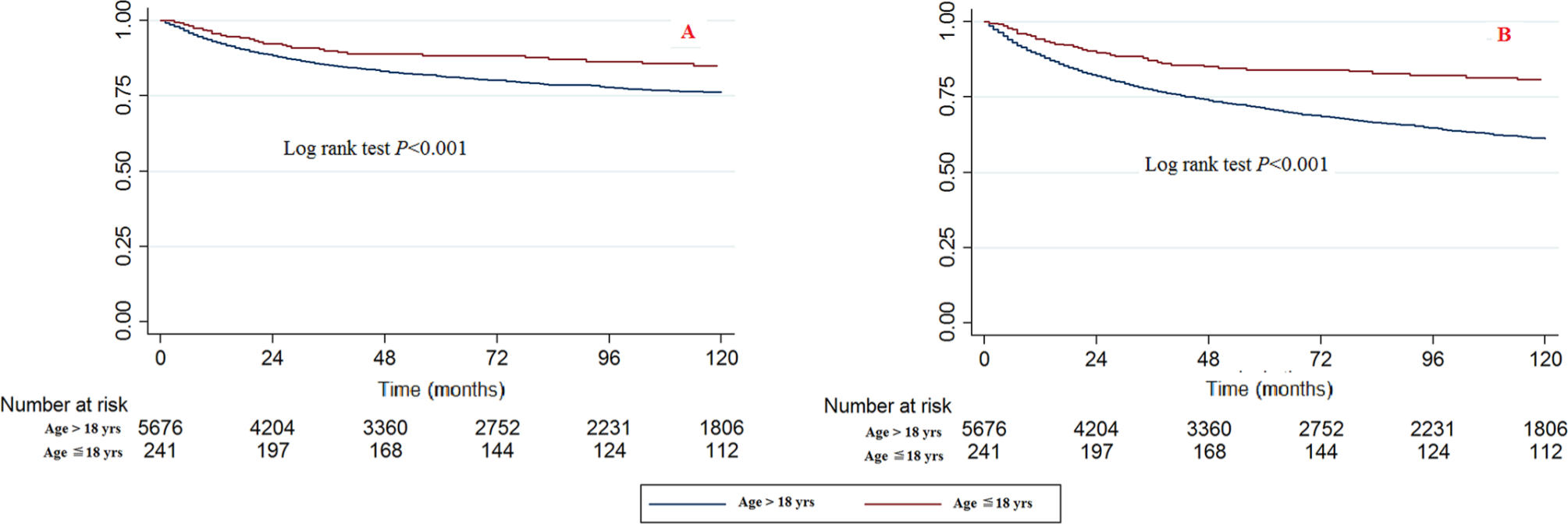
Kaplan-Meier survival curves illustrating the chondrosarcoma cancer-specific survival (
Bivariable and multivariable Cox analyses of chondrosarcoma cancer-specific survival
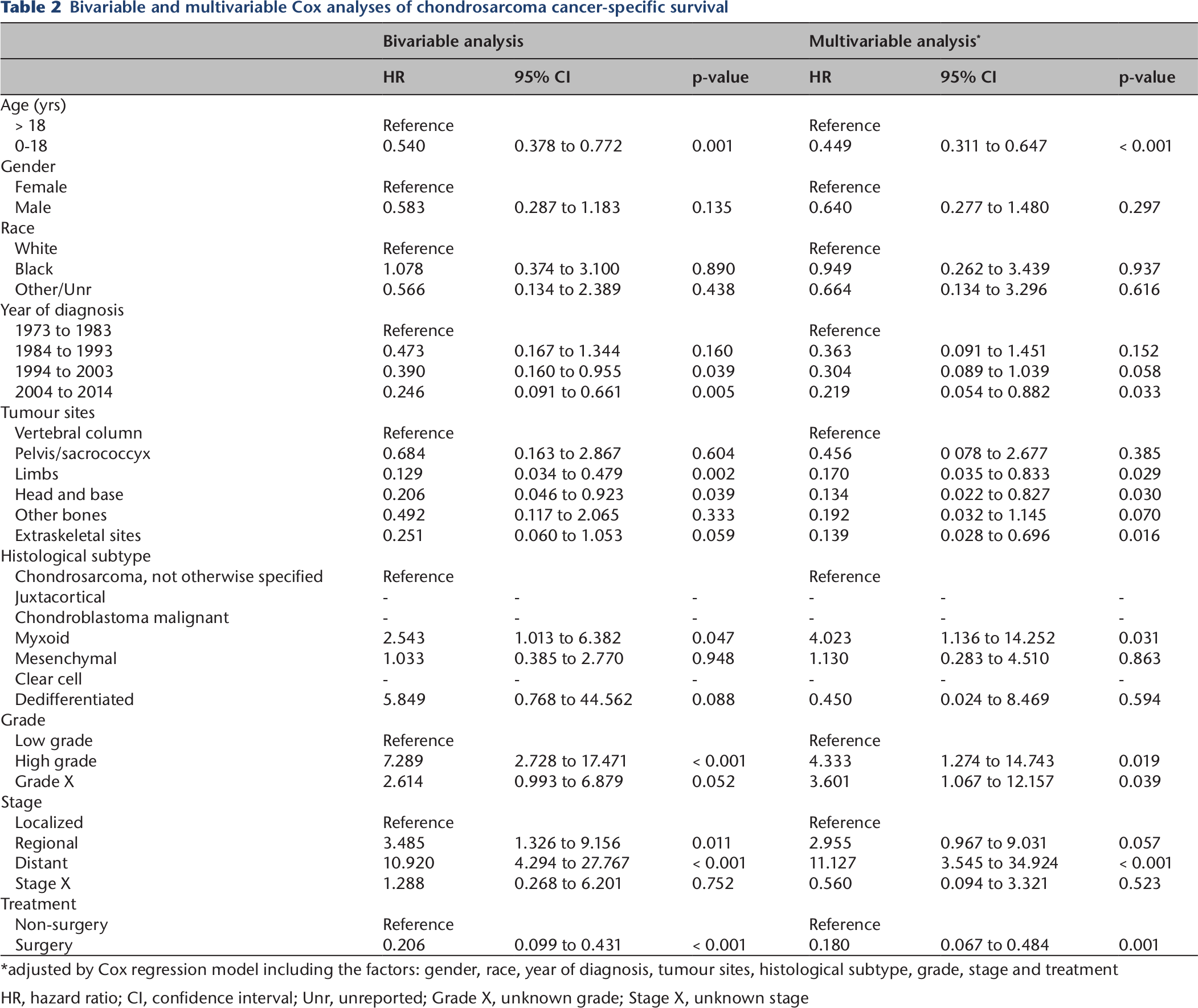
adjusted by Cox regression model including the factors: gender, race, year of diagnosis, tumour sites, histological subtype, grade, stage and treatment
HR, hazard ratio; CI, confidence interval; Unr, unreported; Grade X, unknown grade; Stage X, unknown stage
Bivariable and multivariable Cox analyses of chondrosarcoma overall survival
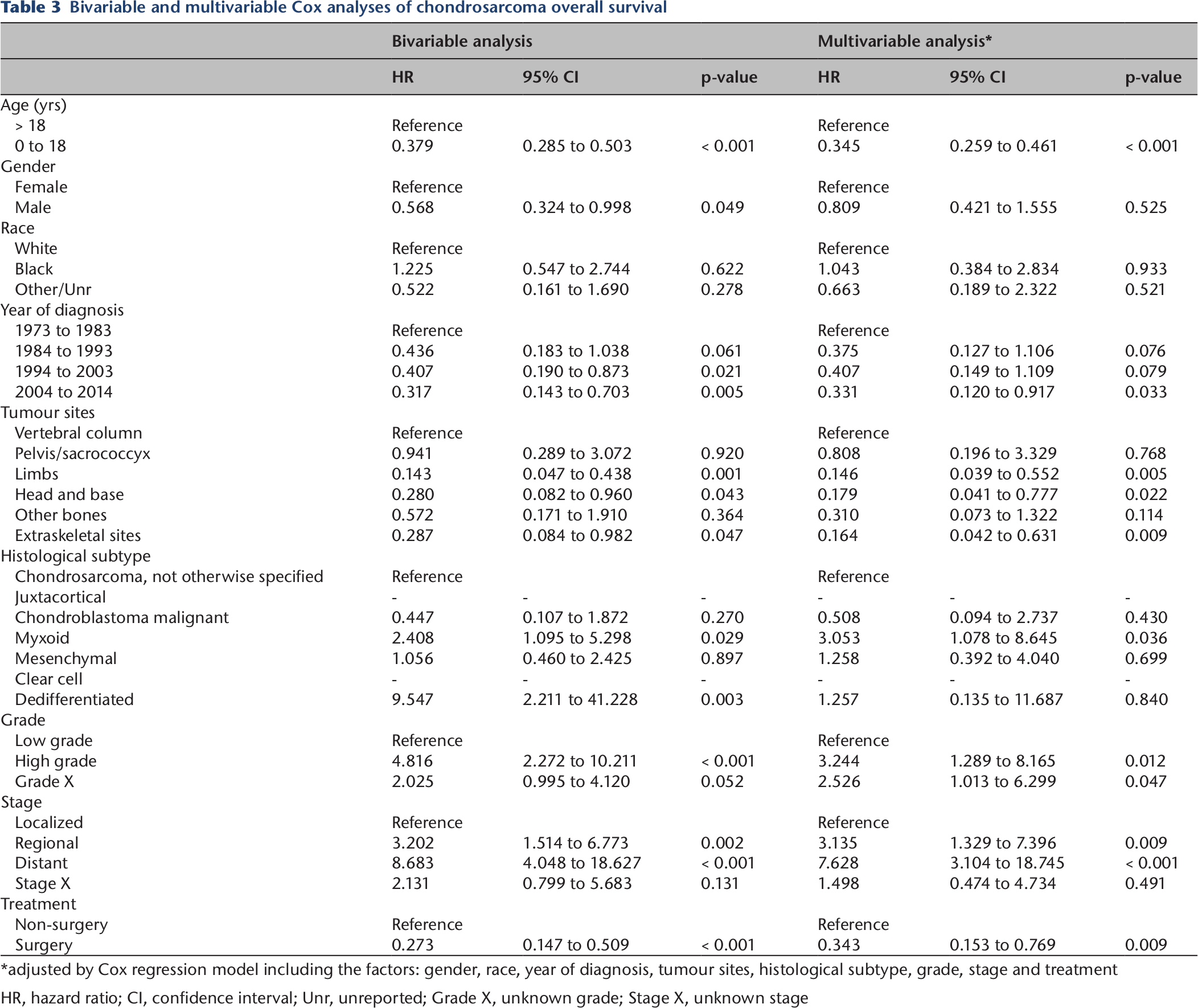
adjusted by Cox regression model including the factors: gender, race, year of diagnosis, tumour sites, histological subtype, grade, stage and treatment
HR, hazard ratio; CI, confidence interval; Unr, unreported; Grade X, unknown grade; Stage X, unknown stage
Gender
No significant differences were observed between the male and female paediatric CCSS population when using the Kaplan-Meier method or the log rank test, but the log rank test for OS showed that p = 0.046 (Supplemental Fig. 1). The bivariable Cox proportional hazard regression models for CCSS found p = 0.049 between male and female. No significant differences were found with the multivariable Cox proportional hazard regression models of CCSS or the bivariable and multivariable Cox proportional hazard regression models of OS (Table 2 and Table 3).
Race
No significant differences were observed among races for CCSS and OS when using the Kaplan-Meier method and log rank test (Supplemental Fig. 2). The bivariable and multivariable Cox proportional hazard regression models for CCSS and OS also found no significant differences among races (Table 2 and Table 3).
Year of diagnosis
Significant differences were observed among the year of diagnosis categories for CCSS and OS when using the Kaplan-Meier method and log rank test (Fig. 2). The 2004 to 2014 category had the best survival and the 1973 to 1983 category had the worst survival.
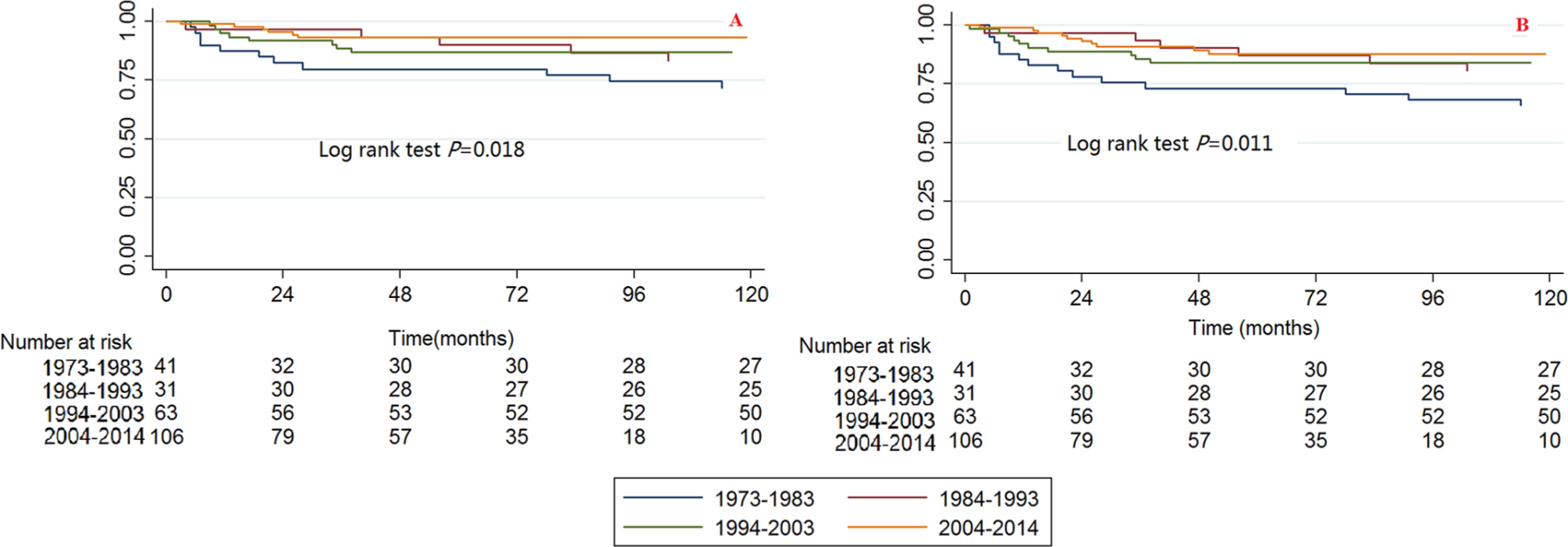
Kaplan-Meier survival curves illustrating the chondrosarcoma cancer-specific survival (
The bivariable and multivariable Cox proportional hazard regression models for CCSS and OS found that the survival trends have improved throughout the years. When the 1973 to 1983 category was used as a reference, the HRs (95% CI) of death caused by chondrosarcoma cancer in the 1984 to 1993, 1994 to 2003 and 2004 to 2014 categories were 0.473 (0.167 to 1.344, p = 0.160), 0.390 (0.159 to 0.955, p = 0.039) and 0. 246 (0.091 to 0.661, p = 0.005), respectively, for the bivariable analysis, and they were 0.363 (0.091 to 1.451, p = 0.152), 0.304 (0.089 to 1.039, p = 0.058) and 0.219 (0.054 to 0.882, p = 0.033), respectively, for the multivariable analysis (Table 2). The HRs (95% CI) of death caused by all reasons in the 1984 to 1993, 1994 to 2003 and 2004 to 2014 categories were 0.436 (0.183 to 1.038, p = 0.061), 0.407 (0.190 to 0.873, p = 0.021) and 0.317 (0.143 to 0.703, p = 0.005), respectively, for the bivariable analysis, and they were 0.375 (0.127 to 1.106, p = 0.076), 0.407 (0.149 to 1.109, p = 0.079) and 0.331 (0.120 to 0.917, p = 0.033), respectively, for the multivariable analysis (Table 3).
Tumour sites
Significant differences were observed among different tumour sites for CCSS and OS when using the Kaplan-Meier method and log rank test (Fig. 3). The tumour sites at the vertebral column and the pelvis/sacrococcyx had poorer survival rates, while those at the limbs, head and base had better survival rates.
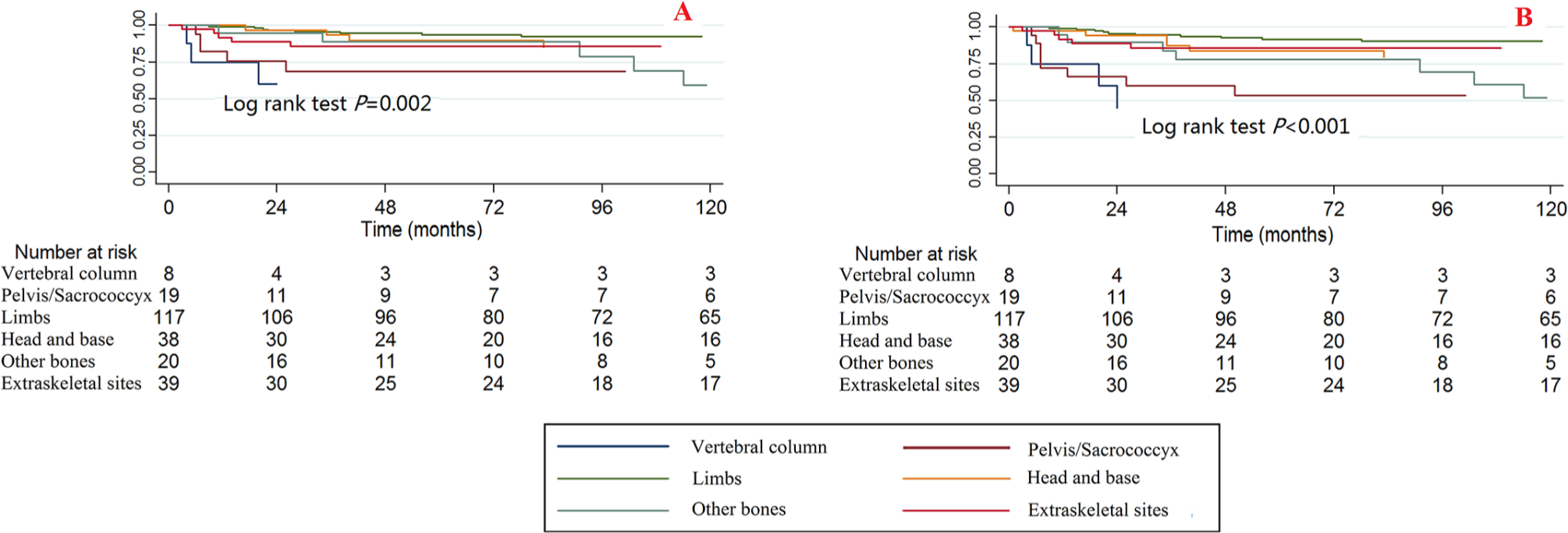
Kaplan-Meier survival curves illustrating the chondrosarcoma cancer-specific survival (
The bivariable and multivariable Cox proportional hazard regression models for CCSS and OS found no significant differences in survival for patients with tumour sites at the vertebral column and pelvis/sacrococcyx, while the multivariable Cox proportional hazard regression models for OS found that patients with tumour sites at the limbs, head and base had significantly lower death risks than those with tumour sites at the vertebral column (Tables 2 and 3).
Histological subtypes
Since some of the histological subtypes had very small simple sizes, the HRs of some of the histological subtypes cannot be calculated (Tables 2 and 3). Therefore, we provide the summarized information of the histological subtypes. The number of patients with each histological subtype in each age category is summarized in Figure 4a and the surgical ratio of each histological subtype is summarized in Figure 4b. The Kaplan-Meier curve and log rank test was also performed; the log rank P value for CCSS is 0.035 and for OS is 0.001 (Fig. 5).
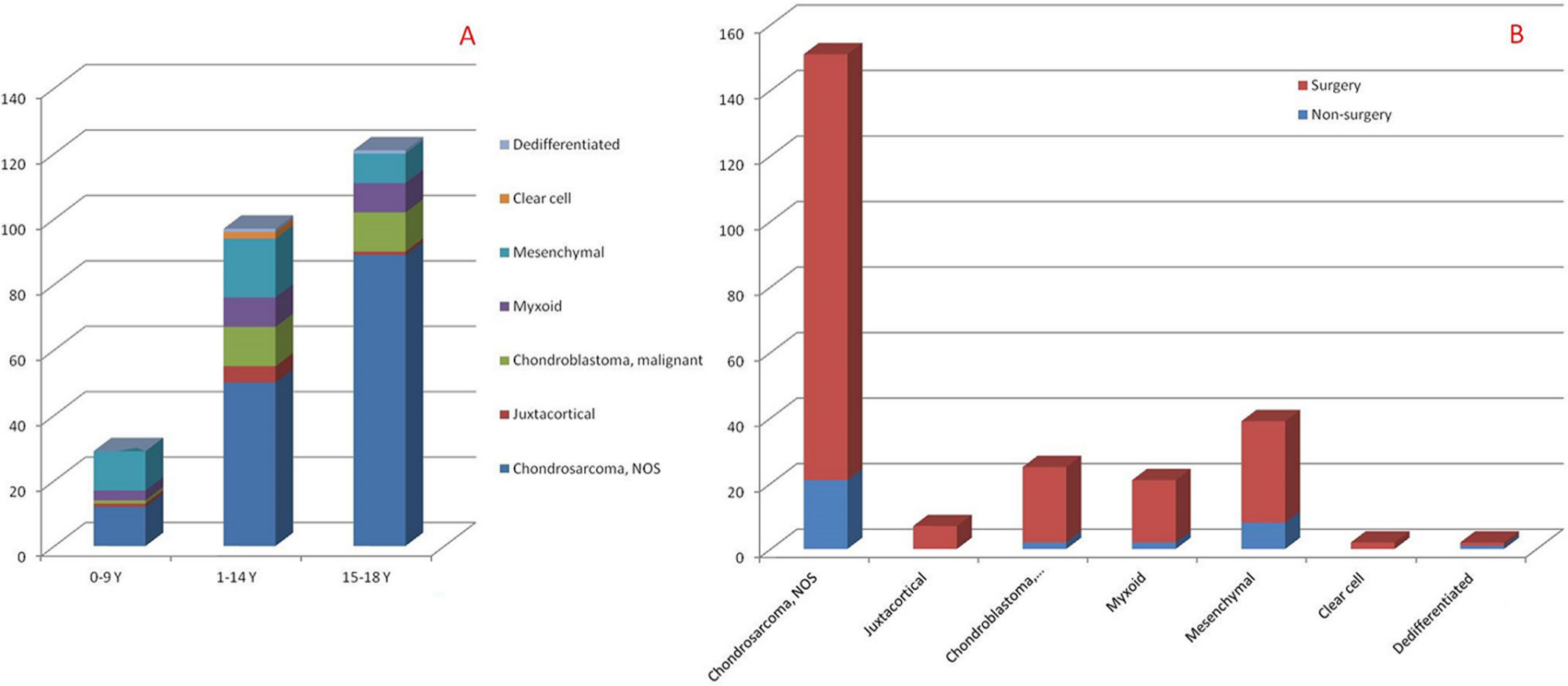
The summarized number of histological subtypes in each age categories and the surgical ratio of each histological subtype (NOS, not otherwise specified).
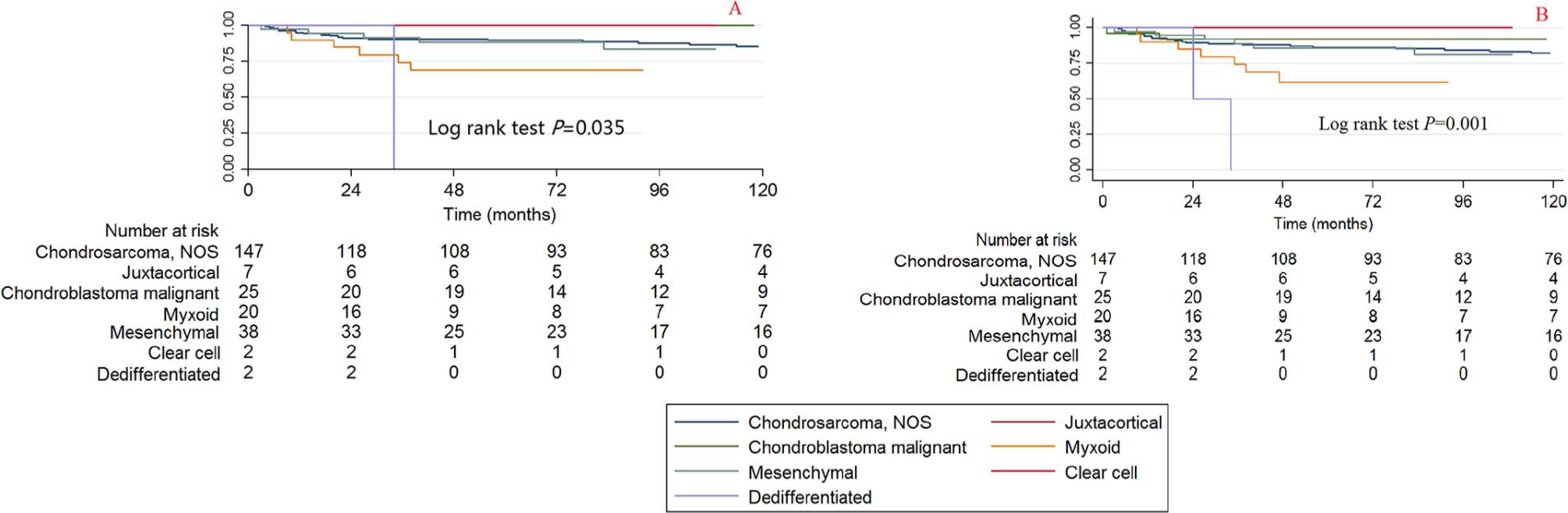
Kaplan-Meier survival curves illustrating the chondrosarcoma cancer-specific survival (
The bivariable and multivariable Cox proportional hazard regression models for CCSS and OS found that the histological subtype of myxoid has the poorest survival rate (Tables 2 and 3) and the bivariable HRs (95% CI) of all reasons causing death in patients with the dedifferentiated histological subtype is 9.547 (2.211 to 41.228, p = 0.003). No significant difference was observed for the other histological subtypes.
Grade
A significant difference was observed among the grades of CCSS and OS when using the Kaplan-Meier method and log rank test (Fig. 6). The high-grade tumours were associated with poorer survival compared with the low-grade tumours.
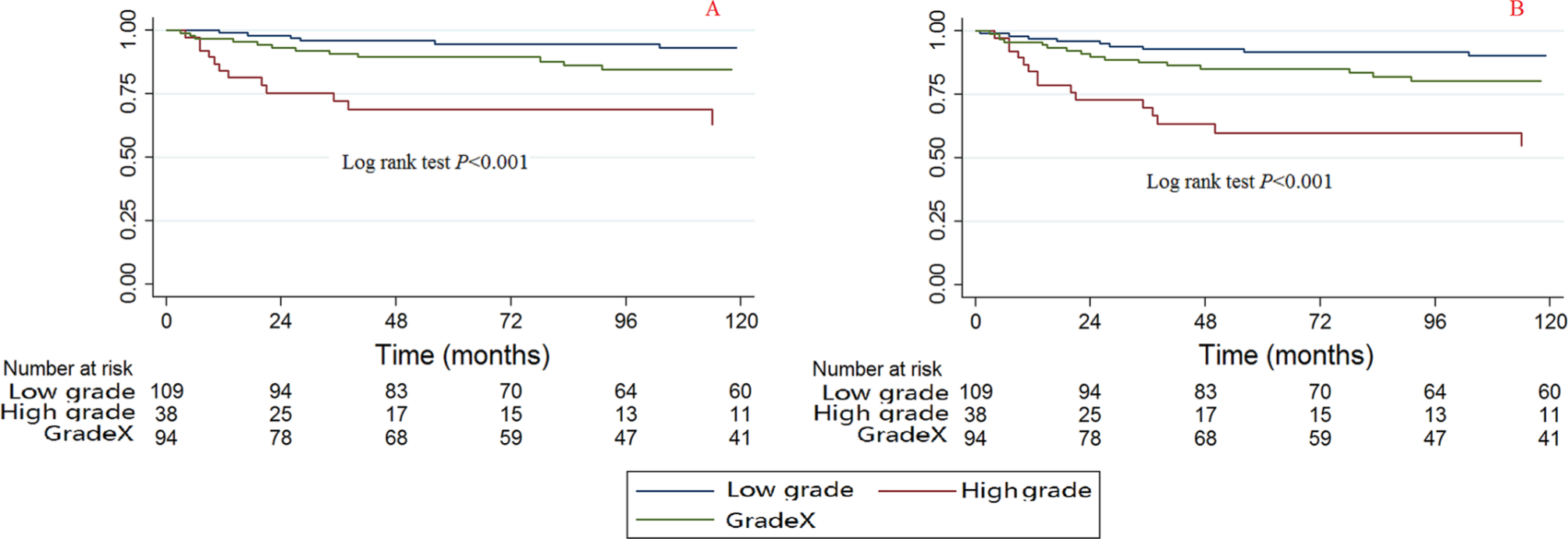
Kaplan-Meier survival curves illustrating the chondrosarcoma cancer-specific survival (
The bivariable and multivariable Cox proportional hazard regression models for CCSS and OS found that patients with high-grade tumours also have poorer survival (Tables 2 and 3); the HRs (95% CI) for bivariable CCSS, multivariable CCSS, bivariable OS and multivariable OS are 7.289 (2.728 to 17.471, p < 0.001), 4.333 (1.274 to 14.743, p = 0.019), 4.816 (2.272 to 10.211, p < 0.001) and 3.244 (1.289 to 8.165, p = 0.012), respectively.
Stage
A significant difference was observed among stages in CCSS and OS when using the Kaplan-Meier method and the log rank test (Fig. 7). Patients with a localized stage tumour had the best survival and those with a distant category had the worst survival.
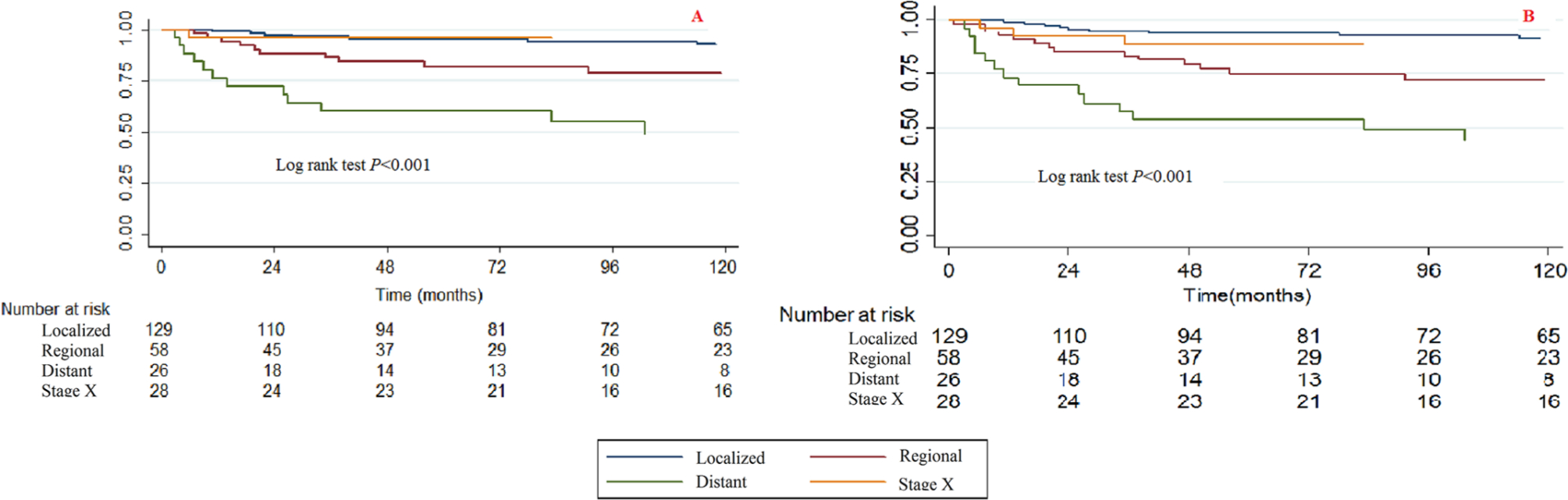
Kaplan-Meier survival curves illustrating the chondrosarcoma cancer-specific survival (
The bivariable and multivariable Cox proportional hazard regression models for CCSS and OS found that patients with higher stage tumours have poorer survival rates. When we used the localized stage as a reference, the regional stage HRs (95% CI) for bivariable CCSS, multivariable CCSS, bivariable OS and multivariable OS were 3.485 (1.326 to 9.156, p = 0.011), 2.955 (0.967 to 9.031, p = 0.057), 3.202 (1.514 to 6.773, p = 0.002) and 3.135 (1.329 to 7.396, p = 0.009), respectively. The distant stage HRs (95% CI) of bivariable CCSS, multivariable CCSS, bivariable OS and multivariable OS were 10.920 (4.294 to 27.767, p < 0.001), 11.127 (3.545 to 34.924, p < 0.001), 8.683 (4.048 to 18.627, p < 0.001) and 7.628 (3.104 to 18.745, p < 0.001), respectively.
Treatment
Significant differences were observed between surgery and non-surgery patients when using the Kaplan-Meier method and log rank test (Fig. 8). Patients who had received surgery had better survival rates than those without surgery.
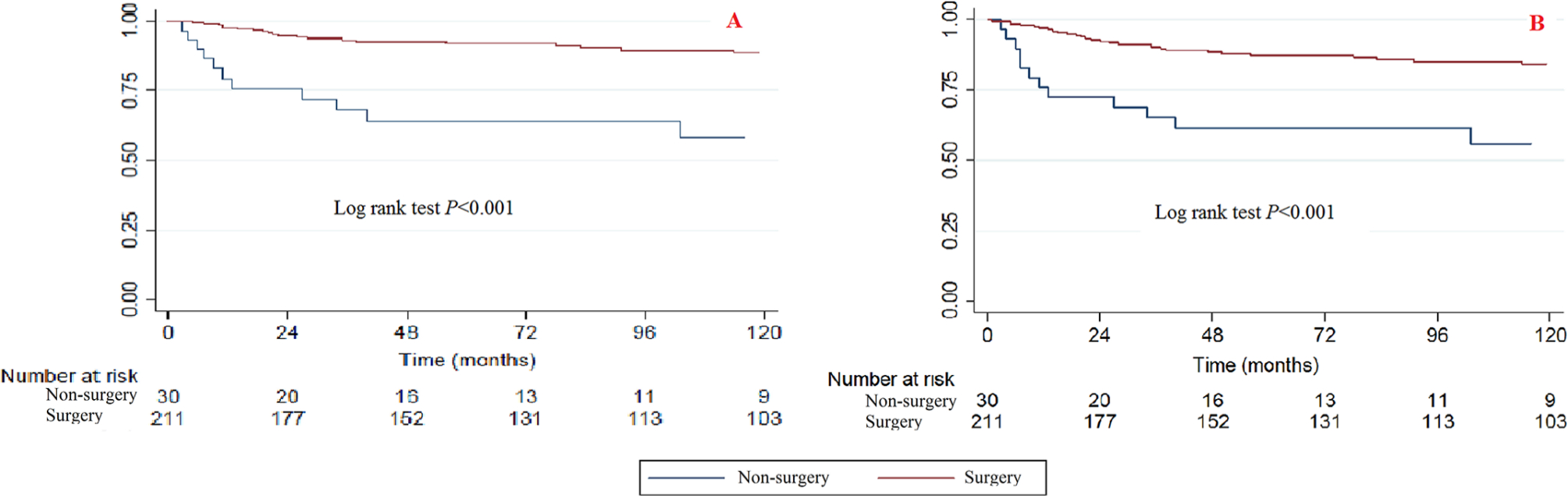
Kaplan-Meier survival curves illustrating the chondrosarcoma cancer-specific survival (
The bivariable and multivariable Cox proportional hazard regression models of CCSS and OS found that surgery can also improve the survival rate (Tables 2 and 3). When the non-surgery category was used as a reference, the surgery HRs (95% CI) for bivariable CCSS, multivariable CCSS, bivariable OS and multivariable OS were 0.206 (0.099 to 0.4311, p < 0.001), 0.180 (0.067 to 0.484, p = 0.001), 0.273 (0.147 to 0.509, p < 0.001) and 0.343 (0.153 to 0.769, p = 0.009), respectively.
Sub-analysis of the chondrosarcoma NOS subtype
There were 151 cases of patients with the chondrosarcoma NOS subtype, and the sub-analysis found that most of the results of the analysis of this chondrosarcoma NOS subtype (Supplemental Tables 1 and 2) were similar to the results of total chondrosarcoma (Tables 2 and 3); however, some of the multivariable analyses of “treatment” and “year of diagnosis” still did not show a significant difference.
Discussion
Chondrosarcoma is a rare histological entity arising both in the bones and in the soft tissues of the paediatric population.27,28 Bishop et al 9 retrospectively reviewed 12 paediatric chondrosarcoma patients (aged from 1.3 to 19.7 years) that were diagnosed at their medical centre from 01 January 1990 to 30 May 2014. With a median follow-up of 4.8 years, they found that the five-year disease-free survival and OS rates were 68.2% and 88.9%, respectively. Dantonello et al 29 reported that in 15 chondrosarcoma patients with a median age of 16.6 years (1 to 25), the median follow-up at 9.6 years found that the ten-year event-free and OS rates were 53% and 67%, respectively. Most of the other studies on paediatric chondrosarcoma are case reports.11–17 The limited number of patients means that the prognostic factors and survival outcomes cannot be measured.
Giuffrida et al 5 reported that stage was an independent prognostic factor for survival outcomes of adult patients with chondrosarcoma. In our present study, we also found that the year of diagnosis is an independent prognostic factor: the survival rate increases with the years, the 2004 to 2014 category had the best survival and the 1973 to 1983 category had the worst survival. Several reasons may contribute to this outcome, including the advancement of therapeutic techniques (surgical strategy, adjuvant treatments of radiotherapy and chemotherapy and comprehensive care) that have been developed from 1973 to the present, 30 and it is possible that the time of follow-up also influences the results.
Additionally, we found that patients with tumours in the vertebral column and pelvis/sacrococcyx had poorer survival outcomes than those with tumours located in the limbs and other bones. We propose that it is more difficult to surgically remove tumours at the spine and pelvis, which may decrease the survival rates in these regions. 3 Recently, particle beam therapy has been developed and used for pelvic chondrosarcoma, and it may be an acceptable alternative treatment, 31 especially for patients with non-resectable or incompletely resected tumours. 32
There are seven histological subtypes of chondrosarcoma, including chondrosarcoma (NOS), juxtacortical, chondroblastoma malignant, myxoid chondrosarcoma and mesenchymal chondrosarcoma. Some subtypes of chondrosarcoma may respond to the different adjuvant treatments (for example, mesenchymal chondrosarcoma is sensitive to chemotherapy), but the SEER database of 1973 to 2014 did not provide any information about adjuvant treatments; therefore, we cannot provide information on whether adjuvant treatments may improve the survival rates of patients with chondrosarcoma. Since the chondrosarcoma (NOS) subtype consisted of 151 cases, we conducted a sub-analysis of chondrosarcoma (NOS) patients. While most results from this subtype were similar to the results of total chondrosarcoma, some multivariable analyses of ‘treatment’ and ‘year of diagnosis’ still did not show any significant differences, so it may be that the sample size of 151 cases is still not large enough for the analysis of seven variables. Some other histological subtypes also have very small sample sizes in our study (the juxtacortical, chondroblastoma, malignant, myxoid, mesenchymal, clear cell and dedifferentiated subtypes only had seven, 25, 21, 39, two and two cases, respectively); therefore, the HRs of some histological subtypes cannot be calculated.
The different histological subtypes may have variable biological and clinical behaviours. We found that patients with the myxoid chondrosarcoma histological subtype have poorer survival than those with the chondrosarcoma (NOS) subtype. Bumpass et al 33 conducted a review of the literature in 2011 and found from the follow-up data of 26 patients (after a mean period of 49 months) that the rate of local recurrence was 42% and that of metastases was 31%. Mesenchymal chondrosarcoma is similar to Ewing's tumour, 34 and it has historically been considered to be associated with a poor prognosis; however, recent modern therapies have significantly improved patient survival.29,35
The grade in the SEER database is in accordance with the ICD-O-3 edition, which included four grades: well-differentiated (Grade I), moderately differentiated (Grade II), poorly-differentiated (Grade III) and undifferentiated (anaplastic, Grade IV). Referring to Giuffrida et al 5 and Chen et al, 25 we reclassified tumours into two grades (low grade: ICD-O-3 Grades I and II and high grade: ICDO-3 Grades III and III) in the present study. The high-grade patients had poorer outcomes than the low-grade patients, and the results are consistent with those of the adults.5,26
Surgical resection is the mainstream therapeutic method for chondrosarcoma, and in non-paediatric populations, surgery can significantly improve the survival rate for chondrosarcoma. 3 The paediatric outcomes of our present study are consistent with the non-paediatric ones; both suggest a survival benefit from surgery.
The strengths of our present study are as follows: 1) this is the largest paediatric chondrosarcoma study that includes both the demographic and survival information;36,37 2) we performed analyses of both CCSS and OS as well as bivariable analyses and multivariable analyses, and most of the outcomes of the prognostic factors consistently show significant differences at all of these four analyses; and 3) the multivariable Cox hazard regression model includes age at diagnosis, race, gender, year of diagnosis, tumour sites, histological subtypes, grade stages and treatments.
There are some limitations to our present study. This is a retrospective study, and the SEER database has its natural drawbacks in that it does not contain some of the detailed information on patient comorbidities and adjuvant treatments, it does not include surgical information of intralesional, marginal and wide margin tumours and a central pathology review is not available. The study is an observational study, but it is not a clinical controlled study, so it may have some cofounders that cannot be included; the present update of the SEER database did not have information on radiotherapy, although patients with the chondrosarcoma NOS histological subtype are resistant to radiation.3,38 The mesenchymal chondrosarcoma and chondrosarcoma tumours located at the base of the skull may show favourable results after radiotherapy,39,40 but this cannot be proven by an analysis from the present SEER database.
Conclusion
Paediatric chondrosarcoma patients have better survival rates than the adults. The year of diagnosis, tumour sites, tumour histological subtype, grade, stage and whether patients received surgery are independent prognostic factors for the survival rates of paediatric chondrosarcoma patients. Patients with diagnoses at a younger age, tumour site at the vertebral column and pelvis/sacrococcyx, myxoid variants, high grade, distant stage, and who did not receive surgery have poorer prognoses than those who were diagnosed at an older age or who had tumour site at the limbs, head and base, chondrosarcoma not otherwise specified, localized stage and who had received surgery.
Footnotes
This article does not contain any studies with human participants or animals performed by any of the authors.
AMW, GL, JWZ, CHC, and DC developed and tested the data collection forms.
AMW, GL, SRS, YSW, NFT and ZKL acquired the data.
AMW, GL, ZGQ, JGZ, BW, and WLF conducted the analysis and interpreted the data.
AMW, GL and HX drafted the manuscript.
All authors critically revised the manuscript.